Embed Size (px)
Citation preview
Cancro del testicolo
Revisione poster
Giuseppe L. Banna
Oncologia Medica
A.O. Cannizzaro Catania
Outline
Survival and prognosis
New drugs and targetable targets
Tumor biomarkers
Survivors: toxicity and follow-up
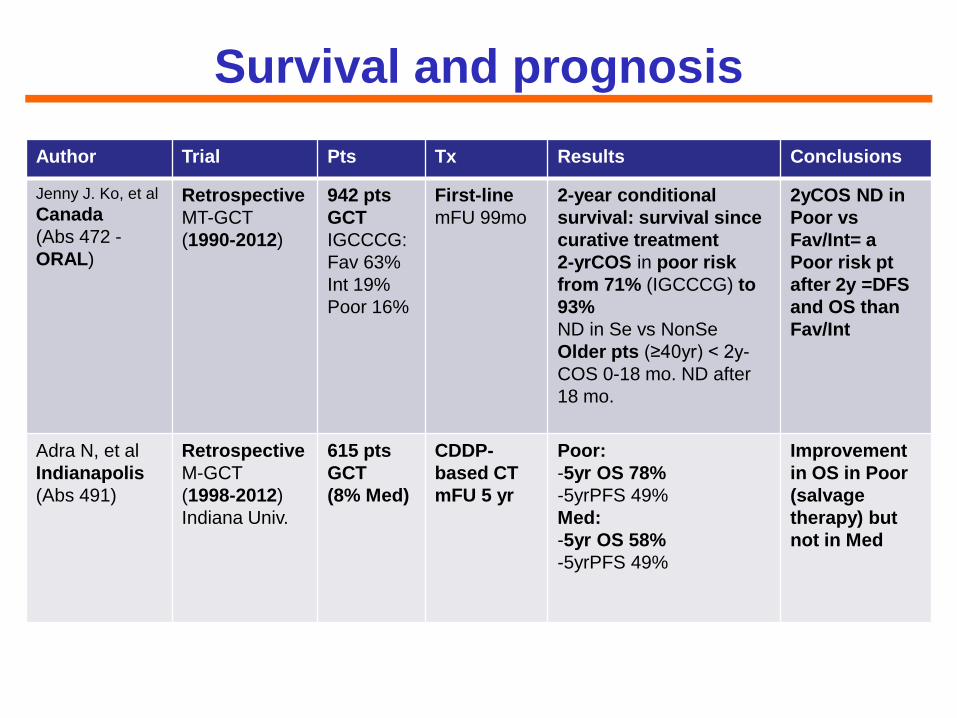
Survival and prognosis
Author Trial Pts Tx Results Conclusions
Jenny J. Ko, et al
Canada
(Abs 472 -
ORAL)
Retrospective
MT-GCT
(1990-2012)
942 pts
GCT
IGCCCG:
Fav 63%
Int 19%
Poor 16%
First-line
mFU 99mo
2-year conditional
survival: survival since
curative treatment
2-yrCOS in poor risk
from 71% (IGCCCG) to
93%
ND in Se vs NonSe
Older pts (≥40yr) < 2y-
COS 0-18 mo. ND after
18 mo.
2yCOS ND in
Poor vs
Fav/Int= a
Poor risk pt
after 2y =DFS
and OS than
Fav/Int
Adra N, et al
Indianapolis
(Abs 491)
Retrospective
M-GCT
(1998-2012)
Indiana Univ.
615 pts
GCT
(8% Med)
CDDP-
based CT
mFU 5 yr
Poor:
-5yr OS 78%
-5yrPFS 49%
Med:
-5yr OS 58%
-5yrPFS 49%
Improvement
in OS in Poor
(salvage
therapy) but
not in Med
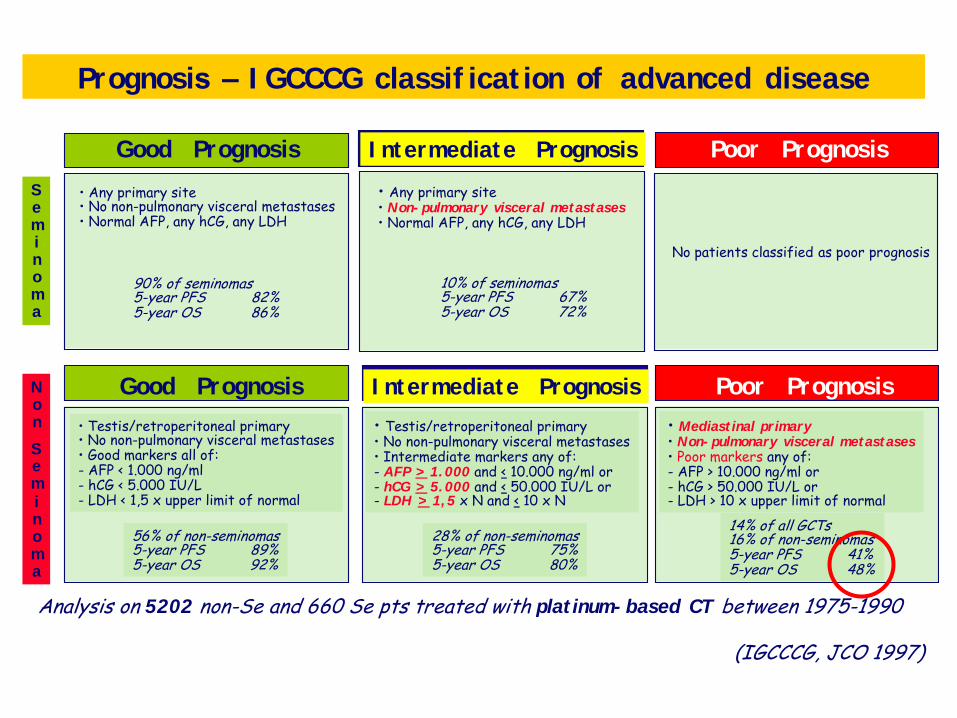
Good Prognosis
• Any primary site • No non-pulmonary visceral metastases • Normal AFP, any hCG, any LDH
90% of seminomas 5-year PFS 82% 5-year OS 86%
Poor Prognosis
No patients classified as poor prognosis
Analysis on 5202 non-Se and 660 Se pts treated with plat inum- based CT between 1975-1990
(IGCCCG, JCO 1997)
Seminoma
Non
Seminoma
• Testis/retroperitoneal primary • No non-pulmonary visceral metastases • Good markers all of: - AFP < 1.000 ng/ml - hCG < 5.000 IU/L - LDH < 1,5 x upper limit of normal
56% of non-seminomas 5-year PFS 89% 5-year OS 92%
Good Prognosis
• Testis/retroperitoneal primary • No non-pulmonary visceral metastases • Intermediate markers any of: - AFP > 1. 000 and < 10.000 ng/ml or - hCG > 5. 000 and < 50.000 IU/L or - LDH > 1, 5 x N and < 10 x N
28% of non-seminomas 5-year PFS 75% 5-year OS 80%
I ntermediate Prognosis
• Mediast inal pr imary • Non- pulmonary visceral metast ases • Poor markers any of: - AFP > 10.000 ng/ml or - hCG > 50.000 IU/L or - LDH > 10 x upper limit of normal
14% of all GCTs 16% of non-seminomas 5-year PFS 41% 5-year OS 48%
Poor Prognosis
I ntermediate Prognosis
• Any primary site • Non- pulmonary visceral metastases • Normal AFP, any hCG, any LDH
10% of seminomas 5-year PFS 67% 5-year OS 72%
Prognosis – I GCCCG classif icat ion of advanced disease
Survival and prognosis
Take-home messages
Prognosis of IGCCG poor risk pts has been
improved in the last years (IGCCG data are
1975-1990 lasted) thanks to appropriate first
line and salvage therapy
PMNSGCTs represent a current challenge
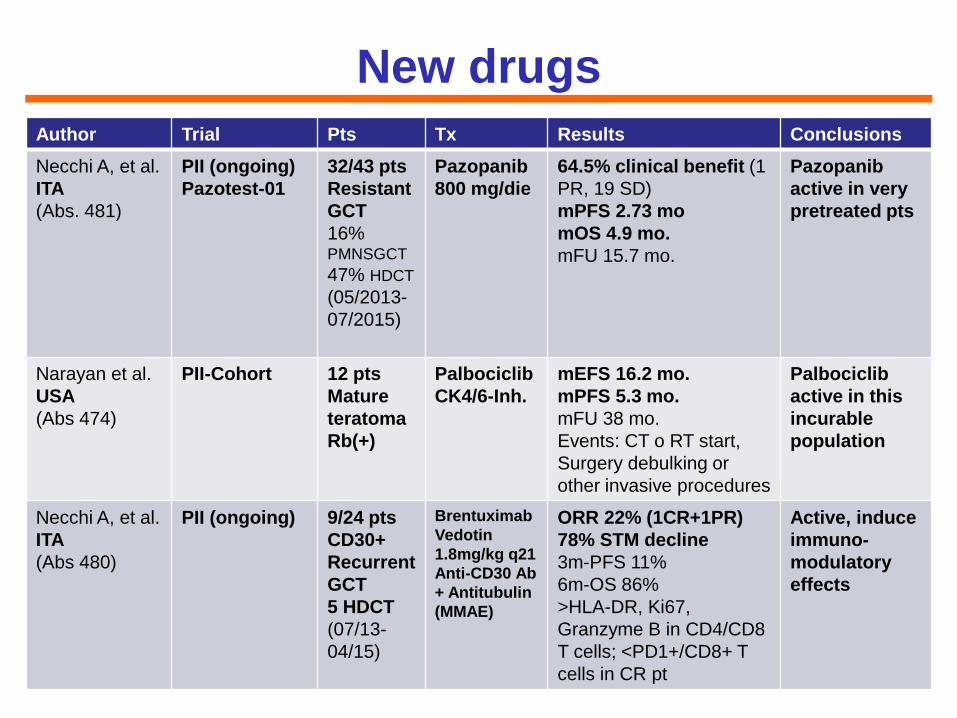
Author Trial Pts Tx Results Conclusions
Necchi A, et al.
ITA
(Abs. 481)
PII (ongoing)
Pazotest-01
32/43 pts
Resistant
GCT
16% PMNSGCT
47% HDCT
(05/2013-
07/2015)
Pazopanib
800 mg/die
64.5% clinical benefit (1
PR, 19 SD)
mPFS 2.73 mo
mOS 4.9 mo.
mFU 15.7 mo.
Pazopanib
active in very
pretreated pts
Narayan et al.
USA
(Abs 474)
PII-Cohort 12 pts
Mature
teratoma
Rb(+)
Palbociclib
CK4/6-Inh.
mEFS 16.2 mo.
mPFS 5.3 mo.
mFU 38 mo.
Events: CT o RT start,
Surgery debulking or
other invasive procedures
Palbociclib
active in this
incurable
population
Necchi A, et al.
ITA
(Abs 480)
PII (ongoing) 9/24 pts
CD30+
Recurrent
GCT
5 HDCT
(07/13-
04/15)
Brentuximab
Vedotin
1.8mg/kg q21
Anti-CD30 Ab
+ Antitubulin
(MMAE)
ORR 22% (1CR+1PR)
78% STM decline
3m-PFS 11%
6m-OS 86%
>HLA-DR, Ki67,
Granzyme B in CD4/CD8
T cells; <PD1+/CD8+ T
cells in CR pt
Active, induce
immuno-
modulatory
effects
New drugs
Targetable targets
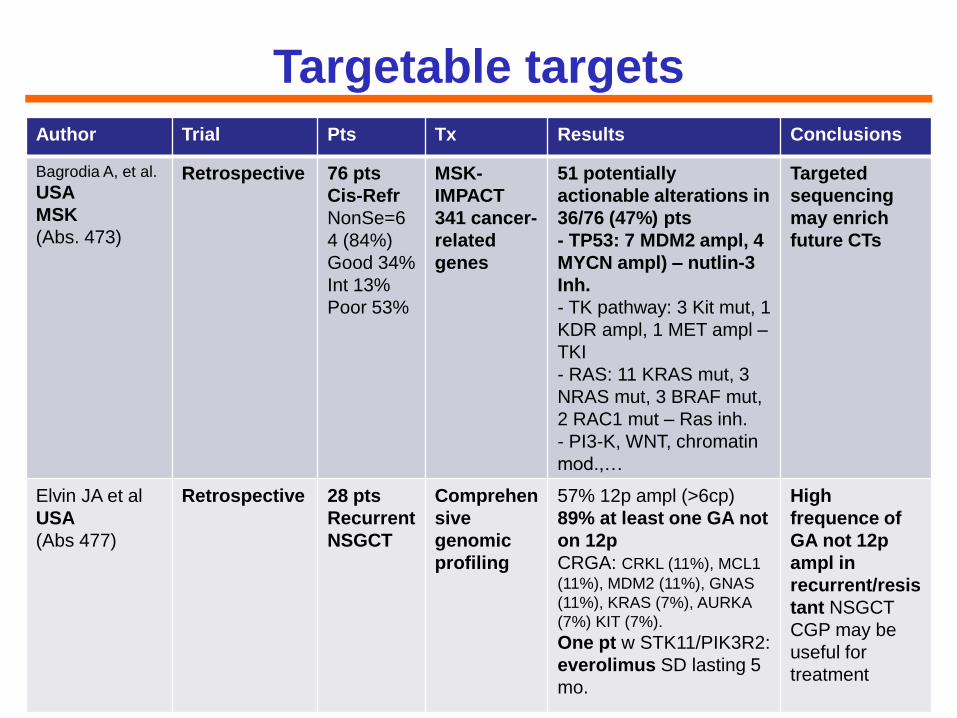
Author Trial Pts Tx Results Conclusions
Bagrodia A, et al.
USA
MSK
(Abs. 473)
Retrospective
76 pts
Cis-Refr
NonSe=6
4 (84%)
Good 34%
Int 13%
Poor 53%
MSK-
IMPACT
341 cancer-
related
genes
51 potentially
actionable alterations in
36/76 (47%) pts
- TP53: 7 MDM2 ampl, 4
MYCN ampl) – nutlin-3
Inh.
- TK pathway: 3 Kit mut, 1
KDR ampl, 1 MET ampl –
TKI
- RAS: 11 KRAS mut, 3
NRAS mut, 3 BRAF mut,
2 RAC1 mut – Ras inh.
- PI3-K, WNT, chromatin
mod.,…
Targeted
sequencing
may enrich
future CTs
Elvin JA et al
USA
(Abs 477)
Retrospective 28 pts
Recurrent
NSGCT
Comprehen
sive
genomic
profiling
57% 12p ampl (>6cp)
89% at least one GA not
on 12p
CRGA: CRKL (11%), MCL1
(11%), MDM2 (11%), GNAS
(11%), KRAS (7%), AURKA
(7%) KIT (7%).
One pt w STK11/PIK3R2:
everolimus SD lasting 5
mo.
High
frequence of
GA not 12p
ampl in
recurrent/resis
tant NSGCT
CGP may be
useful for
treatment
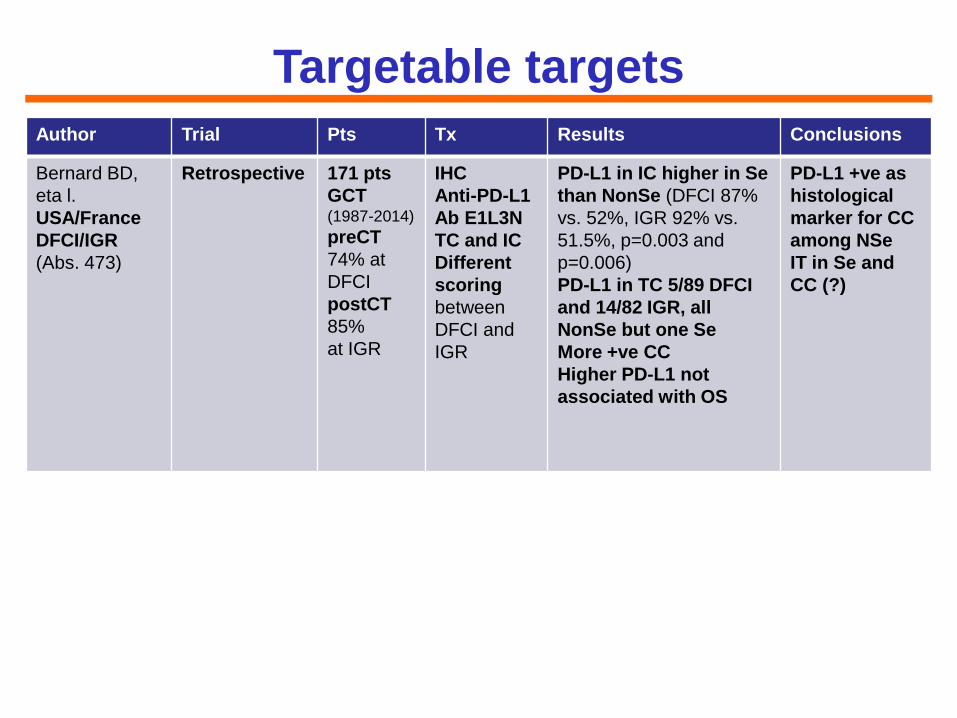
Targetable targets
Author Trial Pts Tx Results Conclusions
Bernard BD,
eta l.
USA/France
DFCI/IGR
(Abs. 473)
Retrospective
171 pts
GCT (1987-2014)
preCT
74% at
DFCI
postCT
85%
at IGR
IHC
Anti-PD-L1
Ab E1L3N
TC and IC
Different
scoring
between
DFCI and
IGR
PD-L1 in IC higher in Se
than NonSe (DFCI 87%
vs. 52%, IGR 92% vs.
51.5%, p=0.003 and
p=0.006)
PD-L1 in TC 5/89 DFCI
and 14/82 IGR, all
NonSe but one Se
More +ve CC
Higher PD-L1 not
associated with OS
PD-L1 +ve as
histological
marker for CC
among NSe
IT in Se and
CC (?)
New drugs and Targetable targets
Take-home messages
Genome sequencing for actionable targets
may be a useful option for testing new drugs in
recurrent/resistant GCTs
Pazopanib and Brentuximab Vedotin seem to
be active in heavily pretreated resistant GCT
Palbociclib active in mature teratoma
PD-L1 could be a target for Se and CC ?
Brentuximab Vedotin may act by enhancing
immune response (rationale for IT?)
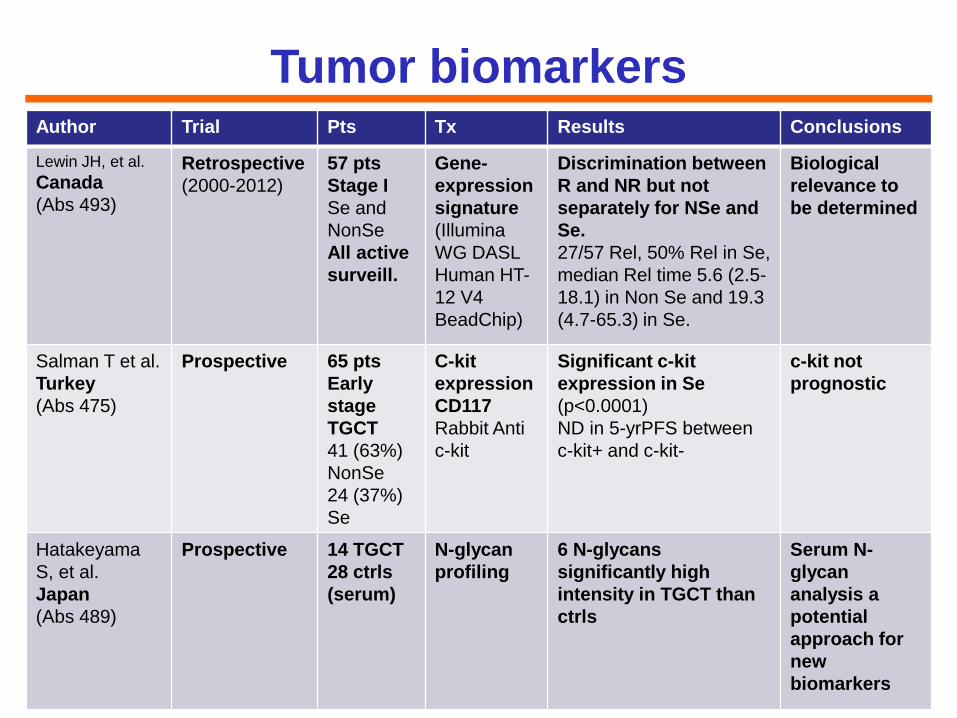
Author Trial Pts Tx Results Conclusions
Lewin JH, et al.
Canada
(Abs 493)
Retrospective
(2000-2012)
57 pts
Stage I
Se and
NonSe
All active
surveill.
Gene-
expression
signature
(Illumina
WG DASL
Human HT-
12 V4
BeadChip)
Discrimination between
R and NR but not
separately for NSe and
Se.
27/57 Rel, 50% Rel in Se,
median Rel time 5.6 (2.5-
18.1) in Non Se and 19.3
(4.7-65.3) in Se.
Biological
relevance to
be determined
Salman T et al.
Turkey
(Abs 475)
Prospective
65 pts
Early
stage
TGCT
41 (63%)
NonSe
24 (37%)
Se
C-kit
expression
CD117
Rabbit Anti
c-kit
Significant c-kit
expression in Se
(p<0.0001)
ND in 5-yrPFS between
c-kit+ and c-kit-
c-kit not
prognostic
Hatakeyama
S, et al.
Japan
(Abs 489)
Prospective 14 TGCT
28 ctrls
(serum)
N-glycan
profiling
6 N-glycans
significantly high
intensity in TGCT than
ctrls
Serum N-
glycan
analysis a
potential
approach for
new
biomarkers
Tumor biomarkers
Genomic profiling may be an useful tool when
active surveillance is the standard option for
stage I TGCT, but is not ready for prime time
cKit significantly expressed in Se than in
NonSe but not prognostic (nor targetable
with imatinib in a previous experience)
N-glycan analysis is a novel approach that
could be explored to identify new biomarkers
in TGCT
Tumor biomarkers
Take-home messages
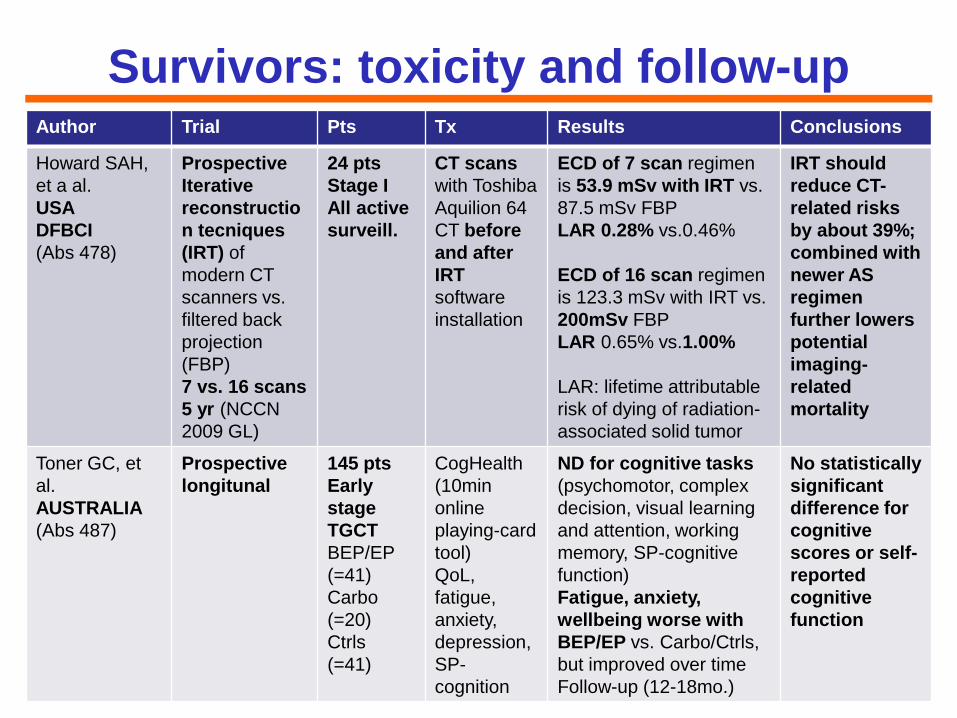
Author Trial Pts Tx Results Conclusions
Howard SAH,
et a al.
USA
DFBCI
(Abs 478)
Prospective
Iterative
reconstructio
n tecniques
(IRT) of
modern CT
scanners vs.
filtered back
projection
(FBP)
7 vs. 16 scans
5 yr (NCCN
2009 GL)
24 pts
Stage I
All active
surveill.
CT scans
with Toshiba
Aquilion 64
CT before
and after
IRT
software
installation
ECD of 7 scan regimen
is 53.9 mSv with IRT vs.
87.5 mSv FBP
LAR 0.28% vs.0.46%
ECD of 16 scan regimen
is 123.3 mSv with IRT vs.
200mSv FBP
LAR 0.65% vs.1.00%
LAR: lifetime attributable
risk of dying of radiation-
associated solid tumor
IRT should
reduce CT-
related risks
by about 39%;
combined with
newer AS
regimen
further lowers
potential
imaging-
related
mortality
Toner GC, et
al.
AUSTRALIA
(Abs 487)
Prospective
longitunal
145 pts
Early
stage
TGCT
BEP/EP
(=41)
Carbo
(=20)
Ctrls
(=41)
CogHealth
(10min
online
playing-card
tool)
QoL,
fatigue,
anxiety,
depression,
SP-
cognition
ND for cognitive tasks
(psychomotor, complex
decision, visual learning
and attention, working
memory, SP-cognitive
function)
Fatigue, anxiety,
wellbeing worse with
BEP/EP vs. Carbo/Ctrls,
but improved over time
Follow-up (12-18mo.)
No statistically
significant
difference for
cognitive
scores or self-
reported
cognitive
function
Survivors: toxicity and follow-up
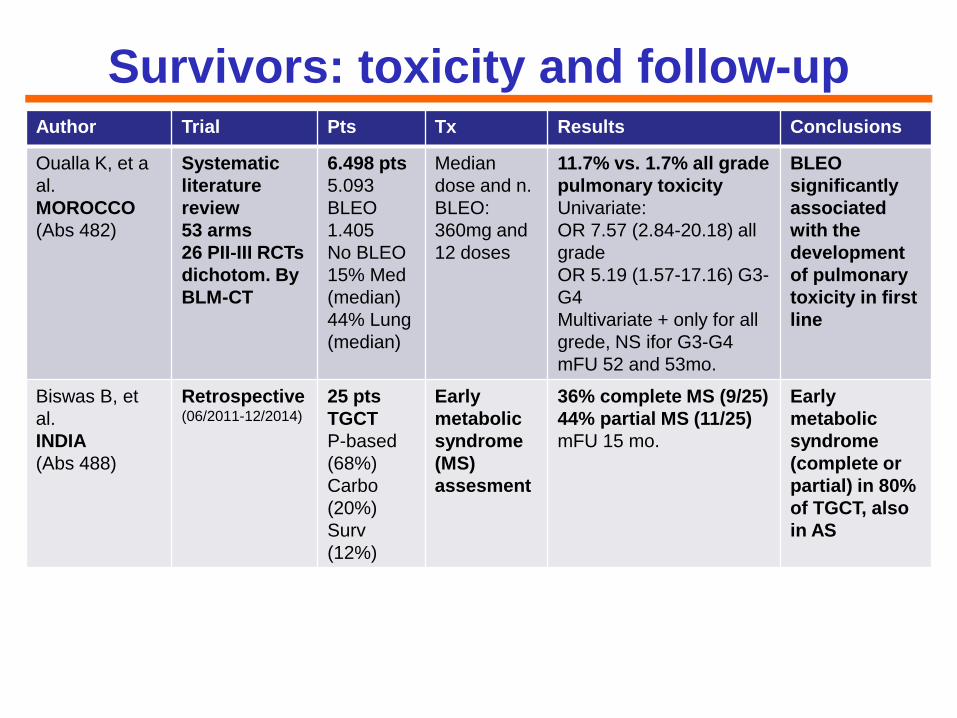
Author Trial Pts Tx Results Conclusions
Oualla K, et a
al.
MOROCCO
(Abs 482)
Systematic
literature
review
53 arms
26 PII-III RCTs
dichotom. By
BLM-CT
6.498 pts
5.093
BLEO
1.405
No BLEO
15% Med
(median)
44% Lung
(median)
Median
dose and n.
BLEO:
360mg and
12 doses
11.7% vs. 1.7% all grade
pulmonary toxicity
Univariate:
OR 7.57 (2.84-20.18) all
grade
OR 5.19 (1.57-17.16) G3-
G4
Multivariate + only for all
grede, NS ifor G3-G4
mFU 52 and 53mo.
BLEO
significantly
associated
with the
development
of pulmonary
toxicity in first
line
Biswas B, et
al.
INDIA
(Abs 488)
Retrospective (06/2011-12/2014)
25 pts
TGCT
P-based
(68%)
Carbo
(20%)
Surv
(12%)
Early
metabolic
syndrome
(MS)
assesment
36% complete MS (9/25)
44% partial MS (11/25)
mFU 15 mo.
Early
metabolic
syndrome
(complete or
partial) in 80%
of TGCT, also
in AS
Survivors: toxicity and follow-up
A 7-scan regimen for AS along with the use of
modern CT scanners (with IRT software) may
significantly reduce the already small potential mortality
of imaging associated cancers
Cognitive function of TGCT patients treated with CT
(BEP/PE or Carbo) is not impaired
Pulmonary toxicity of BLEO should be taken into
account in first-line (no BLEO containing regimens?)
Metabolic syndrome affect a significant (up to 80%)
proportion of treated and untreated TGCT pts
requiring early intervention
Survivor: toxicity and follow-up
Take-home messages
Grazie
“Meglio aggiungere vita ai giorni che
non giorni alla vita” Rita Levi Montalcini
Anno 2015
Carcinoma della
prostata
Anno 2016
Cancro del
testicolo
e Consiglio Direttivo IGG