-
Research Article
GITR Pathway Activation Abrogates Tumor ImmuneSuppression
through Loss of Regulatory T-cell LineageStability
David A. Schaer1, Sadna Budhu1, Cailian Liu1, Campbell Bryson2,
Nicole Malandro1,2, Adam Cohen4,Hong Zhong1, Xia Yang1, Alan N.
Houghton1, Taha Merghoub1, and Jedd D. Wolchok1,2,3
AbstractLigation of GITR (glucocorticoid-induced TNF
receptor-related gene, or TNFRSF18) by agonist antibody
has recently entered into early-phase clinical trials for the
treatment of advanced malignancies. Although theability of GITR
modulation to induce tumor regression is well documented in
preclinical studies, theunderlying mechanisms of action,
particularly its effects on CD4þFoxp3þ regulatory T cells (Treg),
have notbeen fully elucidated. We have previously shown that GITR
ligation in vivo by agonist antibody DTA-1 causesmore than 50%
reduction of intratumor Tregs with downmodulation of Foxp3
expression. Here, we show thatthe loss of Foxp3 is tumor dependent.
Adoptively transferred Foxp3þ Tregs from tumor-bearing animals
loseFoxp3 expression in the host when treated with DTA-1, whereas
Tregs from na€�ve mice maintain Foxp3expression. GITR ligation also
alters the expression of various transcription factors and
cytokines importantfor Treg function. Complete Foxp3 loss in
intratumor Tregs correlates with a dramatic decrease in
Heliosexpression and is associated with the upregulation of
transcription factors, T-Bet and Eomes. Changes inHelios correspond
with a reduction in interleukin (IL)-10 and an increase in IFN-g
expression in DTA-1–treated Tregs. Together, these data show that
GITR agonist antibody alters Treg lineage stability inducing
aninflammatory effector T-cell phenotype. The resultant loss of
lineage stability causes Tregs to lose theirintratumor
immune-suppressive function, making the tumor susceptible to
killing by tumor-specific effectorCD8þ T cells. Cancer Immunol Res;
1(5); 320–31. �2013 AACR.
IntroductionThe immune system is capable of recognizing
malignant
cells, but inmost situations, tumors develop strategies to
avoidelimination and escape immune surveillance (1). Recentadvances
in immunotherapy have succeeded in shifting thebalance from tumor
immune escape to tumor elimination.Instead of treating the tumor
directly by inhibiting cellgrowth, immunotherapeutic approaches
modulate a patient'simmune system to induce tumor regression. The
success ofthis approach is highlighted by the U.S. Food and
DrugAdministration approval of the CTLA-4–blocking antibody,
ipilimumab, the first therapy to show enhanced overall surv-ival
for patients with melanoma (2). Serving as a proof-of-principle,
CTLA-4 blockade has led to targeting of otherimmune checkpoints
(PD-1/PD-L1) alone or in combinationwith CTLA-4, with very
promising results in early-phase clin-ical trials (3–6). Although
coinhibitory receptor blockadehas shown durable clinical efficacy,
a significant number ofpatients (�50%–80%) remain refractory to
these treatmentsand some tumor types do not respond as robustly as
others(3, 7). To further potentiate antitumor immune responses
andextend clinical benefit, activating costimulatory molecules,such
as TNF receptor (TNFR) superfamily members
GITR(glucocorticoid-induced TNF receptor-related gene), OX40,and
4-1BB, represent a logical next step (8, 9).
GITR became an attractive target for cancer immunother-apy after
the agonistic anti-GITR antibodyDTA-1was shown toblock the
suppressive effects of regulatory T cells (Treg; ref.
10).Subsequently, DTA-1 was shown to enhance tumor immunityin a
concomitant immunitymodel ofmelanoma. In addition topreventing
growth of secondary tumor challenges, DTA-1treatment also caused
the regression of some of the primarytumor challenge (11). This
observation has been extended intomultiple tumor models and various
combinatorial strategieswith vaccines, adoptive T-cell transfer,
and concurrent CTLA-4blockade (12). With preclinical success of
GITR tumor immu-notherapy, it has been entered into early-phase
clinical trials
Authors' Affiliations: 1Swim Across America – Ludwig
CollaborativeLaboratory, Immunology Program, Sloan-Kettering
Institute for CancerResearch; 2Weill Cornell Medical College;
3Ludwig Center for CancerImmunotherapy at Memorial Sloan-Kettering
Cancer Center, New York,New York; and 4Perelman Center for Advanced
Medicine, University ofPennsylvania, Philadelphia, Pennsylvania
Note: Supplementary data for this article are available at
Cancer Immu-nology Research Online
(http://cancerimmunolres.aacrjournals.org/).
T. Merghoub and J.D. Wolchok have co-senior authorship in this
article.
Corresponding Author: Jedd D. Wolchok, Memorial
Sloan-KetteringCancer Center, 1275 York Avenue, New York, NY 10065.
Phone: 646-888-2315; Fax: 646-422-0453; E-mail:
[email protected]
doi: 10.1158/2326-6066.CIR-13-0086
�2013 American Association for Cancer Research.
CancerImmunology
Research
Cancer Immunol Res; 1(5) November 2013320
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
for the treatment of advanced malignancies. Despite its
ther-apeutic potential, the mechanism of action on Tregs asopposed
to effector T cells (Teff) has not been fully
elucidated.Understanding its activity on Tregs is a necessary step
toinform the effective use of GITR therapy in humans.Whether or not
GITR immunotherapy targets GITR solely
on Teffs, or on both Teffs and Tregs, has been an area
ofinvestigation. Because GITR is constitutively expressed athigh
levels on Tregs, it was assumed that DTA-1 directlyinhibited
Treg-suppressive function in vitro (10). However,GITR is also
upregulated on CD4 and CD8 Teffs followingactivation and acted as
costimulatory receptor (13). Throughthe use of GITR�/� Tregs, it
was determined that the costi-mulatory role of GITR enabled Teffs
to resist Treg suppres-sion while having no direct effect on Tregs
(14). Thus, initialreports of enhanced tumor immunity resulting
from GITRligation by agonist antibody DTA-1 were attributed to
themodulation of Teffs (15, 16). Nevertheless, we and others
haverecently shown that direct modulation of Tregs is an import-ant
consequence of DTA-1 therapy (17, 18). DTA-1 treatmentcauses more
than 50% reduction of intratumor Tregs anddown modulation of Foxp3.
In addition, the effects of DTA-1are attenuated if either Teffs or
Tregs is GITR�/� (17). Ourdata suggest that the efficacy of DTA-1
comes not only fromits effect on Teffs, but also from its
modulation of Tregs.Here, we show that GITR ligation by DTA-1
induces
intratumor Treg lineage instability. DTA-1 causes loss ofFoxp3
in a tumor-dependent manner and is preceded by theloss of the
transcription factor Helios. This results in theacquisition of a
Th1 effector-like profile and prevents Treg-mediated intratumor
suppression of the antitumor immuneresponse. Our results show that
modulation of Tregs, alongwith Teffs, is important and necessary
for the efficacy ofGITR immunotherapy.
Materials and MethodsMiceC57BL/6: CD45.1, Thy1.2þ, Thy1.1þ, and
OT-1 TCR trans-
genic mice were obtained from Jackson Laboratory. Pmel-1T-cell
receptor transgenic mice were a gift from Dr. NicohlasRestifo
[National Cancer Institute (NCI), Bethesda, MD].Foxp3-GFP knockin
mice were a gift from Dr. A. Rudensky[Memorial Sloan-Kettering
Cancer Center (MSKCC), NewYork, NY]. GITR�/� and GITRþ/þ
littermates (Sv129 �C57BL/6 background) were a gift from Dr. P.P.
Pandolfi(MSKCC) and were backcrossed more than 10 generationsand
onto Pmel-1 Thy1.1þ C57BL/6 background using aspeed congenic
system. Mice were maintained accordingto NIH Animal Care
guidelines, under a protocol (# 96-04-017) approved by the MSKCC
Institutional Animal Care andUse Committee.
Cell lines, tumor challenge, and DTA-1 therapyB16F10/LM3
(hereafter called B16) is derived from the
B16F10 line provided by I. Fidler (MD Anderson CancerCenter,
Houston, TX), and transfected with OVA to generateB16-OVA (19).
Tumor cells were cultured in RPMI-1640 medi-
um containing 7.5% FBS (for up to 2weeks after thawing).
Eachmouse received 150,000 cells in 150 mL of growth factor–reduced
Matrigel (BD Biosciences) injected subcutaneously.Four days after
tumor challenge, mice were injected intraper-itoneally with either
1 mg of affinity-purified DTA-1 or PurifiedRat immunoglobulin G
(IgG; Sigma-Aldrich) in 500 mL PBS.
Lymphocyte isolationSpleens, tumor-draining lymph nodes (TDLN),
and tumors
were excised on days indicated in the text. Tumors wereweighed,
and then tissue was homogenized through 40-mmstrainers to produce
single-cell suspensions. Red blood cellswere lysed from spleens
using an ACK lysis buffer (Lonza).Cells were washed with media, and
tissue cell counts werecalculated using Guava cell counter
(Millipore). Cells werethen either sorted for Tregs, stained
immediately by fluores-cence-activated cell sorting (FACS) or for
cytokine recall,stimulated with phorbol 12-myristate 13-acetate
(PMA) andionomycin for 4 hours, and then treated with monensin
beforeFACS staining.
Antibodies and FACS analysisAnti-GITR (DTA-1, S. Sakaguchi,
Osaka University, Osaka,
Japan) and anti-OX40 (OX86, A. Weinberg, Earle ChilesResearch
Institute, Portland, OR) were produced by theMSKCC Monoclonal
Antibody Core Facility, and anti-4-1BB(LOB12.3) was procured from
Bioxcell. Foxp3 Staining Kit(eBioscience) was used for
intracellular staining. Antibodiesto antigens listed in figures
were from BD Biosciences exceptFoxp3 (eBioscience), Helios, CD45.2
(Biolegend), and Nrp1(R&D systems). Dead cell exclusion was
done using the AquaLIVE/DEAD Fixable Dead Cell Stain Kit
(Invitrogen). Sampleswere acquired on 12-color LSRII cytometer, and
analyzed usingFlowJo (Tree Star).
Treg adoptive transfersTumor-experienced or na€�ve Foxp3-GFP
Tregs were isolated
from spleens and TDLNs of untreated Foxp3-GFPmice bearingB16
tumors 7 to 8 days after tumor challenge, or non–tumor-bearing.
CD4þ GFPþ Tregs were isolated by enriching CD4þ
cells by CD4-positive or -negative MACS microbead separa-tion
kits (Miltenyi) before sorting for GFP expression on aCytomation
MoFlo or BD FACS Aria cell sorter in the MSKCCFlow Cytometry Core
Facility. For cotransfer experiments(Fig. 1C), na€�ve Tregs were
isolated from Thy 1.1þ C57BL/6mice using MACS microbead Treg
isolation kit (Miltenyi).Tregs were then injected intravenously
(5–7 � 105cell/mousefor each Treg type being transferred) in 200 mL
of sterile PBS.
Collagen-fibrin gel-killing assayThe collagen-fibrin gel-killing
assay is described in depth by
Budhu and colleagues (20) and was adapted for ex vivo
tumors.Briefly, B16-Ova tumors isolated on day 10 or 11 after
tumorchallenge were cut into small pieces, incubated for 5
minutesin 250 mg/mL collagenase in PBS containing Ca2þMg2þ,
andhomogenized through 100-mm cell strainers to create single-cell
suspensions. Viable tumor cells and tumor-infiltratinglymphocytes
were counted by Trypan blue exclusion. A total of
GITR Induced Treg Lineage Instability
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013
321
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
A
C
Naïve
D
E
B d
donors
donor
donor
Naïve host
recipients
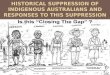
Figure 1. Foxp3 loss induced by DTA-1 is enhanced by tumor
growth and is increased in the tumor microenvironment. A, fresh
frozen sections of B16 tumorsfrom control IgG (IgG)- or
DTA-1–treated Foxp3-GFP mice at day 10 of tumor growth, labeled for
Foxp3 and DAPI described by Cohen and colleagues (17).Scale bar, 25
mm. Lack of Foxp3 staining and non-nuclear GFP label is seen in
DTA-1–treated sections. B, representative FACS plots showCD4þ
transferredTregs in spleen of recipients after gating on live,
CD45þ CD3þ, MHC-IINEG, CD11bNEG cells. (Legend continued on the
following page.)
Schaer et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology
Research322
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
104 viable tumor cells, together with all infiltrating
cells,were coembedded into collagen-fibrin gels with or without1 to
5 � 105 CD8þ T cells activated in vitro by cognatepeptide þ
interleukin (IL)-2. Duplicate gels were lysed every24 hours for 3
days, and viable remaining tumor cells werediluted and plated in
6-well plates for colony formation. Sevendays later, plates were
fixed with 3.7% formaldehyde andstained with 2% methylene blue
before counting as describedby Budhu and colleagues (20).
Rate of tumor cell killingKilling constant k is calculated as
described in ref. (20).
Briefly, k is calculated according to the following equation:bt
¼ b0e�kptþgt, where bt ¼ the concentration of B16 cells attime t;
b0 ¼ the concentration of B16 cells at time 0; k ¼ thekilling rate
constant (or killing efficiency) for CD8 T cells;p¼ the
concentration of in vitro activated CD8 T cells; g¼ thegrowth rate
constant for B16 cells.
Quantitative PCRIndividual tumors and pooled control spleenswere
collected
and stained with anti-CD45, anti-CD4, and 40,
6-diamidino-2-phenylindole (DAPI) before CD45þ CD4þ GFPþ Treg or
GFP�
Teff control, and were FACS sorted on BD FACS Aria directlyinto
Trizol reagent (Invitrogen). Total RNA was prepared andreversed
transcribed into cDNA using a High Capacity cDNAReverse
Transcription Kit (Applied Biosystems). The primer-probe sets were
from TaqMan Gene Expression Assays(Applied Biosystems).
Quantitative real-time PCR reactionswere prepared with FasStart
Universal Probemaster (Rox) mix(Roche) according to the
manufacturer's instructions anddone using the ABI 7500 Real-Time
PCR system (AppliedBiosystems). Each gene was amplified in
duplicate and repeat-ed in two separate experiments. cDNA
concentration differ-ences were normalized to
glyceraldehyde—3—phosphatedehydrogenase (GAPDH). Relative gene
expression of thetarget genes was calculated by the formula 2 – DCt
[DCt ¼Ct (target gene) – Ct (GAPDH)].
ResultsTumor growth sensitizes Tregs to DTA-1–induced
Foxp3lossWe previously showed that optimal GITR agonist
antibody
DTA-1 treatment of early established (day 4) B16 tumorscaused
intratumor Tregs to lose Foxp3 expression. By treatingtumors grown
in mice where Tregs express GFP fused inframe to Foxp3 (Foxp3-GFP),
we were able to detect remnantGFP in former Tregs, after Foxp3 had
been degraded (Fig. 1A).GFP remains, whereas Foxp3 is degraded,
because it is lesssusceptible to proteolytic degradation (Fig. 1A;
ref. 17). DTA-1–induced Foxp3 loss is not seen in peripheral
tissues, sug-
gesting that entry into the tumor microenvironment pro-motes
Treg instability and increases susceptibility to mod-ulation (17).
In addition, adoptively transferred Tregs sortedfrom spleens and
TDLNs of tumor-bearing Foxp3-GFP micelose Foxp3 expression within
48 hours of infiltrating tumorsin DTA-1–treated hosts (17). To
determine what rendersTregs susceptible to GITR modulation, we used
the adoptivetransfer system to track the highly purified
previouslyuntreated Tregs and probe the specific conditions
permittingDTA-1–induced Foxp3 loss.
Tregs have been described to contain a minor populationthat is
less stable and characterized by low CD25 expression.This
population is susceptible to Foxp3 loss after long-termtransfer (4
weeks) into Rag�/� hosts (21). It has recentlybeen shown that
stimulation with Fc-GITR-L can augmentFoxp3 loss after CD4þ T-cell
transfer into a RAG�/� model ofinflammatory bowel disease (22).
Therefore, we first askedwhether during our short-term (48 hours)
adoptive transferconditions, DTA-1 exclusively modulates only the
minorCD25 low population (which at most accounts for only�10% of
Tregs). Consistent with published reports, there isa slight loss in
the percentage of Foxp3þ Tregs in control IgG-treated mice 2 days
after transfer (�90% pretransfer to�77%after transfer, Fig. 1B). In
contrast, DTA-1 treatment induceda pronounced reduction in Foxp3þ
Tregs (�90% Foxp3þpretransfer to �10% Foxp3þ after transfer, Fig.
1B). Thistranslates to an average of a 6 (� 0.58 SEM)-fold decrease
inthe percentage of Foxp3þ transferred Tregs in DTA-1–trea-ted
hosts compared with controls. These data confirm thatDTA-1 has the
potential to modulate all Tregs and is notrestricted to the minor,
unstable CD25low Treg fraction.
Having established the effect of DTA-1 on Treg Foxp3 lossin
lymphopenic conditions, we next assessed how the pres-ence of the
tumor and/or tumor infiltration affects Tregvulnerability to DTA-1.
To accomplish this, we cotransferredcongenically marked (with CD45
and Thy1) Tregs isolatedfrom spleens and TDLNs of tumor-bearing
(CD45.2þ) orna€�ve (Thy1.1þCD45.2þ) donors into lymphoreplete
na€�veor tumor-bearing recipients (CD45.1þ) following thescheme in
Fig. 1C. Na€�ve Thy 1.1 donor Tregs transferredinto na€�ve
recipients displayed negligible loss of Foxp3 inperipheral tissues
48 hours after transfer [88% Foxp3þ,pretransfer (Fig. 1C) vs.
�86%–91% Foxp3þ, in IgG (Fig.1D)]. DTA-1 treatment induced a
maximum of 17% to 18%reduction in na€�ve Foxp3þ Tregs under these
conditions(Fig. 1D, spleen IgG vs. DTA-1). In contrast,
tumor-experi-enced CD45.2þ Tregs transferred into control
IgG-treatedhosts displayed a greater loss of Foxp3 expression
[94%Foxp3þ pretransfer (Fig. 1C) vs. �72% and �48% Foxp3þTregs in
the spleen and lymph nodes, respectively (Fig. 1D)].DTA-1 treatment
enhanced Foxp3 loss in tumor-experienced
(Continued.) C, Tregs were isolated from 25 naïve Thy1.1 CD45.2
donors and 25 tumor-bearing Foxp3-GFP CD45.2 donors, mixed 1:1, and
transferred intonaïve (D), or tumor-bearing (E) CD45.1 recipients
treated with IgG or DTA-1. Transferred Tregs were identified by
gating on live, CD45þ, CD3þ, CD4þ
cells, and then onCD45.2þ (tumor-experienced Tregs), or CD45.2þ
Thy1.1þ (naïve Tregs; D and E, left). Representative examples of
Foxp3 andCD25 stainingare shown in the spleen (D and E, middle).
Graphs show mean � SEM for percent of Foxp3þ donor Tregs recovered
in each tissue from a representativeexperiment (D and E, left).
Experiments were repeated three times with 4 to 5 per group. �, P
< 0.01; ��, P < 0.001; ���, P < 0.0001. LN, lymph
node.
GITR Induced Treg Lineage Instability
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013
323
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
Tregs, which was most evident in the lymph node, wherethere was
approximately 50% reduction in Foxp3þ Tregs inDTA-1–treated
animals, as compared with animals treatedwith control IgG (Fig.
1D). In tumor-bearing recipients, DTA-1 treatment further
potentiated the decrease in Foxp3 expres-sion in tumor-experienced
Tregs in the spleen {34% vs. 23%,IgG vs. DTA-1, P ¼ 0.025 comparing
%foxp3NEG [(Post Foxp3purity-Post Transfer Foxp3%)/Post Foxp3
purity] in Fig. 1D andE}. Na€�ve Tregs only displayed a significant
loss of Foxp3expression upon entering the tumor [(Fig. 1E) 27% drop
IgGvs. DTA-1 compared with pretransfer]. Taken together, ourdata
strongly suggest that preconditioning of Tregs in the pre-sence of
tumor or in the tumormicroenvironment before DTA-1treatment is
important to their susceptibility to Foxp3 loss.
Transferred Tregs do not display cleaved caspase-3, andequal
numbers of transferred Tregs are recovered after DTA-1 treatment
for both tumor-experienced and na€�ve Tregs(Supplementary Fig. S1A
and S1B). Foxp3 loss in tumor-experienced Tregs sorted by high CD25
expression seemedto be comparable with those sorted by Foxp3-GFP
(Supple-mentary Fig. S1C). Moreover, to address the possibility
thatFoxp3NEG Tregs result from DTA-1–induced proliferation
ofcontaminating Teffs, we monitored the proliferation oftransferred
Teff (CD4þ GFPNEG) sorted from Foxp3-GFPtumor-bearing mice.
Supplementary Figure 1D shows thatCD4þ GFPNEG Teffs (sorted from
Foxp3-GFP tumor-bearingmice) do not proliferate or accumulate after
transfer andDTA-1 treatment. In sum, these data indicate that
Foxp3NEG
Tregs come directly from the Foxp3þ Tregs, the frequency ofwhich
is not reduced as a consequence of cell death, deple-tion, or
proliferation of contaminating Teffs.
In addition, we found that the DTA-1–induced Foxp3 lossoccurs in
a dose-dependent manner (Supplementary Fig. S1E).Interestingly,
agonist antibodies to GITR-related TNFR familymembers, 4-1BB and
OX40, did not affect the frequency ofFoxp3þTregs (Supplementary
Fig. S1F). Thus, this effect seemsto be uniquely associated with
GITR stimulation.
Foxp3 loss correlates with a loss of Helios expressionThe data
above suggest that lymphopenic conditions and
the presence of tumor sensitize Tregs to the effects of DTA-1.In
addition, the data imply that DTA-1 has the ability tomodulate a
large percentage of the Treg population, whichremains viable after
loss of Foxp3. Therefore, we hypothesizedthat in the tumor therapy
setting, even the intratumor Tregsthat maintain Foxp3 expression
after DTA-1 treatment wouldbe affected by GITR stimulation. In
fact, we have previouslyshown that Foxp3 expression in the
remaining Tregs is signif-icantly lower in DTA-1– versus control
IgG-treated tumors,supporting this concept (17). To better
understand the out-come of DTA-1–induced Treg instability, we
investigatedwhether there were changes in other markers associated
withTreg stability, function, and/or ontogeny such as the
transcrip-tion factor Helios, and expression of the cell surface
VEGFcoreceptor neuropilin 1 (Nrp1). Expression of Nrp1 has
beenreported to distinguish between thymus-derived (tTreg)
andperipherally derived Tregs (pTreg) and is important for
Tregtrafficking to B16 tumors (23–25). Although the exact role
of
the Ikaros family transcription factor Helios remains
unre-solved, it has been described as amarker of Treg activation
andidentifies the most suppressive population of
tumor-infiltrat-ing Tregs (26, 27). In control animals, intratumor
Tregs areuniformly HeliosHIGH with a majority being Nrp1HIGH, at
thepeak of B16 immune infiltration compared with peripheralTregs
(spleen, 10–11 days after tumor challenge; ref. 28), sug-gesting a
highly activated tTreg phenotype (Fig. 2A; refs. 25, 27).In
contrast, DTA-1 treatment causes a clear loss of Heliosexpression
in the remaining Foxp3þ intratumorTregs (Fig. 2A).Nrp1 expression
did not seem to be as significantly affected asHelios, which may be
related to its role in Treg trafficking (24).
Using changes in Helios expression as a surrogate markerto
identify DTA-1–modulated Tregs in addition to Foxp3 loss,we
expanded our analysis to early phases of Treg tumor in-filtration
to determine the kinetics of Helios loss and its
possiblecorrelation with Treg survival and function. At day 7 of
tumorgrowth (3 days after DTA-1 treatment), there is already
asignificant increase in the HeliosLOW Treg cell population(�18%
compared with �55% in IgG vs. DTA-1 treatment,respectively, Fig.
2B, left). By day 10, there is an approximately55% to 60% loss of
Foxp3þ Tregs (Supplementary Fig. 2A), andthe remaining Foxp3þ Tregs
(�45%–50%) are HeliosLOW inDTA-1–treated tumors. Taken together,
these data suggest thatapproximately 75% to 80% of the Tregs
(compared with controlIgG) in the tumor have been modulated by
DTA-1.
HeliosLOW Tregs in DTA-1–treated tumors express moreof the
prosurvival genes BCL-2 and BCLXL than Helios
HIGH ortotal IgG Tregs (Fig. 2B). This phenotype extends to the
peakof immune infiltration at day 10, but by day 14, even thoughthe
tumors are regressing, the majority of the remainingTregs are
HeliosHIGH (Fig. 2B). Tregs with the lowest levelsof Helios at day
7 also displayed a pronounced reduction ofFoxp3 and CD25 (Fig. 2C).
Helios loss seems to parallel theextent to which free cell surface
GITR is saturated/modulatedby DTA-1, preventing further staining on
Tregs (Fig. 2D). Atday 14, the 1 mg/mouse dose of DTA-1 no longer
saturatesavailable GITR, and intratumor Tregs in DTA-1–treated
micedisplay similar Helios expression compared with IgG (day
14posttumor challenge in Fig. 2B and D). This supports
theconclusion that Tregs lose Foxp3 expression after
tumorinfiltration, with gross changes in Helios expression being
areliable marker of GITR modulation. Increased expression ofBCL-2
and BCLXL, combined with the lack of activated cas-pase-3
(Supplementary Fig. S1), shows that modulated Tregsmaintain a
prosurvival phenotype.
GITR stimulation alters Treg lineage stabilityTregs naturally
co-opt and express inflammatory T-cell
lineage transcription factors (T-bet, RORgt) to facilitate
thesuppression of the corresponding Teff program (29, 30).
WhenFoxp3 expression is ablated in Tregs, they have been shown
torevert to cells with a Teff phenotype. In addition, Helios
hasbeen shown to stabilize Treg programming and suppress
IL-2expression (31, 32). Therefore, DTA-1–treated Tregs that
havelost or are losing Foxp3 expression could acquire a
Teff-likephenotype. In contrast with the reduced expression of
Foxp3and CD25 in DTA-1–treated mice, HeliosLOW Tregs showed
Schaer et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology
Research324
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
increased protein expression of T-cell lineage
transcriptionfactors such as T-bet, RORgt, and Eomes, compared
withHeliosHIGH Tregs (Fig. 3A). Expression in HeliosLOW Tregs
wasalso higher than in Tregs in the IgG control groups at
multipletime points (day 7 for T-bet, days 7–14 for Eomes, days 10
and14 for RORgt; Fig. 3A).
To determine whether increased T-bet, RORgt, and Eomesprotein
levels in Tregs has biologic consequence, we con-ducted a cytokine
recall assay on cells isolated from tumors10 days after DTA-1
treatment. Foxp3-GFP mice were usedfor this experiment because the
staining for Foxp3 andHelios is diminished and unreliable after
PMA/ionomycin
A
B
C D
Figure 2. DTA-1–modulated Tregs show reduced Helios expression
and a prosurvival phenotype. A, representative FACS plots show the
percentage ofHeliosLOW Tregs (live, CD45þ, CD3þ, CD4þ Foxp3þ) in
pooled spleens and individual tumors of DTA-1- and IgG–treated mice
11 days after tumor challenge.B, example FACS histograms (top) show
Helios expression of IgG- (gray filled) and DTA-1–treated (black
line) tumor-infiltrating Tregs on indicated dayafter tumor
challenge. Bottom histograms show comparison of BCL-2 expression in
HeliosHIGH (dashed line) with HeliosLOW (solid black line)
DTA-1–treatedTregs. Mean � SEM for the percentage of HeliosLOW
Tregs in IgG- and DTA-1–treated tumors, mean fluorescence intensity
(MFI) of BCL-2 and BCLXLfor IgG Tregs, compared with HeliosLOW
DTA-1 Tregs at each time point is shown in the graphs. C,
representative Foxp3 and CD25 expression of IgGTregs (gray filed)
versus DTA-1–treated HeliosHIGH (dashed line) and HeliosLOW (black
solid line) Tregs, 7 days after tumor challenge. D, example
FACSplots show Foxp3 and GITR (DTA-1-PE-Cy7) staining of CD4 T
cells in IgG tumors (day 10 post tumor challenge) compared with
DTA-1–treatedtumors on days 7, 10, and 14 posttumor challenge.
Experiments were repeated three times with 4 to 5 per group, with
one representative experiment shown.�, P < 0.01; ��, P <
0.001; ���, P < 0.0001. TC, tumor challenge.
GITR Induced Treg Lineage Instability
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013
325
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
stimulation (Supplementary Fig. S2B). Using Foxp3-GFPmice also
allowed us to circumvent this technical hurdleas low levels of
Foxp3 expression correlate with loss of
Helios (Fig. 2C), allowing us to subset our analysis
toFoxp3-GFPLOW and Foxp3-GFPHIGH Tregs. GFPLOW Tregs(HeliosLOW) in
DTA-1–treated mice showed a more than
A
B C
D
,
,
,
,
,
,,
,
g
Day post TC Day post TC Day post TC
g-
g-
IFN-g
Figure 3. DTA-1–treated Tregs display a Teff-like profile. A,
Helios expression compared with T-bet, RORgt, and Eomes in Tregs
(CD45þ, CD3þ, CD4þ) fromDTA-1–treated tumors is shown in
representative plots. Graphs show the mean� SEM for mean
fluorescence intensity (MFI) of these markers for IgG
Tregs,compared with DTA-1–modulated HeliosLOW Tregs at each time
point. B, IFN-g recalls expression in GFP high (gray shaded)
compared with GFP low Tregs(black line) from day 10 IgG- and
DTA-1–treated tumors. Graph shows themean� SEM IFN-g expression in
IgG Tregs, compared with GFP lowDTA-1 Tregs.C and D, Tregs and
Teffs were sorted from individual mice as described in Materials
and Methods from indicated tissue and time points for gene
expressionanalysis. Graphs compare the level of IL-10, IFN-g (C),
Foxp3, and Helios (D) expression in IgG- compared with
DTA-1–treated tumors. Splenic Tregs andtumor Teffs are provided as
controls. Experimentswere repeated three timeswith 4 to 5per group
(A andB) and two timeswith 10per group (CandD),with
onerepresentative experiment shown. �, P < 0.01; ��, P <
0.001; ���, P < 0.0001. TC, tumor challenge; GAPDH,
glyceraldehyde-3-phosphate dehydrogenase.
Schaer et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology
Research326
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
2-fold increase in IFN-g production compared with
controlIgG-treated Tregs (Fig. 3B). Although there was no
differ-ence in the IFN-g expression between GFPHIGH and GFPLOW
cells in IgG control tumors (Fig. 3B, top), IFN-g expressionwas
restricted to GFPLOW in DTA-1–treated Tregs (Fig. 3B,bottom).
Despite increased RORgt expression in HeliosLOW
Tregs, we did not detect any significant difference betweenIgG
and DTA-1–treated Tregs in its related cytokine IL-17(data not
shown). To confirm this result and more closelymeasure the changes
in Treg lineage phenotype, we sortedFoxp3-GFP Tregs from individual
tumors and measuredthe expression of relevant Tregs and Teff genes.
Using thisapproach, we found a maximum of 4-fold upregulation
inIFN-g expression (day 7) and approximately 2-fold decreasein
IL-10 expression (day 10) in DTA-1–treated Tregs (Fig.3C). Other
markers, such as GITR, IL-2, IL-17, TNF-a, TGF-b,and SATB1, were
expressed to equivalent levels in DTA-1–treated and IgG-treated
Tregs (data not shown). AlthoughHelios protein levels after DTA-1
treatment correlated withreduced Helios gene expression, there was
no major differ-ence in Foxp3 gene expression (Fig. 3D). This would
indicatethat GITR signaling may cause a posttranscription
modifi-cation that leads to reduced Foxp3 protein
expression.Regardless of the mechanism responsible for the loss
ofFoxp3 and Helios expression, these results suggest thatDTA-1
induces Treg lineage instability and acquisition ofa Teff-like
profile.
DTA-1–induced lineage instability removes Treg-suppressive
function from the tumorTo determine whether the phenotypic changes
described
above alter Treg-suppressive function in vivo, we used an exvivo
collagen-fibrin gel matrix culture to measure CD8þ cyto-lytic
T-cell (CTL) effector function against tumor cells fromcontrol IgG-
or DTA-1–treated mice (20). Collagen-fibrin gelsmimic a
three-dimensional tissue-like environment and aremore sensitive
than packed cell-pellet assays at measuringCD8þ CTL effector
function (20). Furthermore, we have foundthat collagen-fibrin gel
cultures of explanted B16 or B16-expressing OVA (B16-OVA) tumors,
which include all infiltrat-ing cells, are resistant to killing by
a 10- to 50-fold excess ofin vitro cognate antigen-activated CD8þ
CTL, recapitulatingthe suppression that exists in vivo (Fig. 4A;
and Budhu andSchaer; unpublished data).Consistent with prior
results, control IgG-treated tumors
become resistant to killing by in vitro activated CTLs
andproliferate in the collagen gels after 24 hours, with the
numberof tumor cells increasing overtime (Fig. 4A; Budhu and
Schaer;unpublished data). In contrast, DTA-1 treatment causedtumors
to remain susceptible to ex vivo killing by activatedCTLs, and the
number of viable tumor cells continued todecrease at 48 and 72
hours (2-fold and 3-fold, respectively,vs. 0 hour; Fig. 4A).
Calculation of the killing efficiency, k (asdescribed in Materials
and Methods and in ref. 20) highlightsthe differences between
DTA-1– and control IgG-treatedtumors. Killing efficiency of CTLs in
DTA-1–treated tumorsincreases over 2-fold at 48 hours (5.3� 10�10
at 24 hours to 1.3� 10�9 at 48 hours; Fig. 4A) in contrast with
that in IgG-treated
mice, which maintains suppression. Ex vivo addition of DTA-1had
no effect on the killing of DTA-1–treated tumors,
controlIgG-treated tumors, or cultured B16 cells, and GITR�/�
CTLkilled tumor cells from DTA-1–treated tumors and culturedB16
cells at the same rate asGITRþ/þCTL (Fig. 4B, dashed linesand green
lines vs. red lines). This suggests that killing isindependent of
GITR stimulation by DTA-1 on CTL (Fig.4B). Combined, our data
support the conclusion that GITRmodulation of Tregs by DTA-1
removes their suppressiveinfluence in the tumor
microenvironment.
DiscussionThe overarching goal of cancer immunotherapy has
been
the activation of tumor-specific immunity that is able
toovercome the hurdles established by tumors to evade
immunedestruction. GITR activation seems to reach an
importantbalance by enhancing tumor immunity while inhibitingimmune
suppression in a tumor-dependent manner. Theresearch presented here
shows that in addition to its estab-lished role in modulating
Teffs, DTA-1 treatment causes Tregsto lose lineage stability,
reducing their suppressive influenceover the tumor
microenvironment.
Our data suggest that conditions present in tumor-bearingmice
and the tumor microenvironment are responsible formaking Tregs
susceptible to GITR-induced Foxp3 loss.Reduced IL-2 levels have
been shown to be important for Tregstability and homeostasis (33,
34). However, we do not believethat the lack of IL-2 accounts for
Treg instability in our systembecause transferred Tregs lose Foxp3
in the periphery evenafter transfer into lymphoreplete hosts. In
addition, equalnumbers of cotransferred tumor-experienced and
na€�veTregs are recovered from DTA-1–treated animals, despite
theloss of Foxp3 expression in tumor-experienced Tregs.
Thissuggests that DTA-1 does not simply deplete Foxp3þ Tregs(Fig.
1D and Supplementary Fig. S1B). Only upon tumorinfiltration in
DTA-1–treated animals do na€�ve donor Tregsmanifest significant
Foxp3 loss, highlighting further the role oftumor conditioning on
Tregs and even at steady state. There-fore, although the detailed
mechanism of GITR signaling-induced Foxp3 loss requires further
investigation, it is evidentthat tumor preconditioning and the
tumor microenvironmentplay amajor role in permitting
GITR-dependentmodulation ofFoxp3 expression.
The reduction of CD25 expression and the production ofIFN-g
observed in intratumor Tregs during DTA-1 therapy(Figs. 2 and 3)
are similar to what has been reported whenFoxp3 is deleted inmature
Tregs (35). There has been evidencesuggesting that inflammatory
environments cause Tregs tolose stability and convert to a
Teff-like phenotype (29); how-ever, recent research has brought
these findings into question.Results from Miyao and colleagues and
Zhou and colleaguessuggest that the conversion of Tregs into Teffs
is actually due toa transient expression of Foxp3 in non-Tregs (36,
37). It isunlikely that the DTA-1–induced Treg lineage conversion
weobserve here is an artifact of lineagemarking. The Treg
transferand gene expression analysis experiments (Figs. 1 and 3)
rely onsorting an entire Foxp3-GFP–positive Treg population and
donot use a lineage marking Cre recombinase system. In fact, we
GITR Induced Treg Lineage Instability
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013
327
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
were unable to use Foxp3-Cre mice due to the "leaky"
lineagemarking seen during backcrossing to the C57BL/6
background(data not shown). Thus, we believe the results presented
hereillustrate that DTA-1–mediated GITR stimulation
causestumor-specific reprogramming of Tregs into a Teff-like
phe-notype. As we were unable to isolate or phenotype
repolarizedFoxp3� Tregs using the Foxp3-Cre lineage marking mice,
itremains to be established whether the conversion of Tregs toa
Teff-like profile is necessary or secondary to the loss
ofFoxp3/suppressive function. Development of complex geneticmodels
would be needed to answer this question and deter-
mine whether former DTA-1–modulated Tregs work to poten-tiate
antitumor immunity after losing suppressive capacity.
How DTA-1–induced GITR signaling leads to Foxp3 degra-dation is
an important question. Expression levels of Foxp3mRNA were
comparable between control IgG- and DTA-1–treated mice, but there
is a marked reduction in Foxp3 proteinlevels (Figs. 3B and 2C).
This would suggest that downstreamsignaling fromGITR imposes
posttranscriptional or posttrans-lational control of Foxp3 protein
expression. Although down-stream signaling from GITR induced by
GITR-L was recentlyshown to alter Treg-suppressive function through
the
A
B
Figure 4. Treg lineage instability removes intratumor immune
suppression. A and B, experiment schematic: tumors were isolated
and dissociated, and10,000 live tumor cells were then embedded
along with all tumor-infiltrating cells (�3–5 times tumor cell
counts) in collagen-fibrin gel together with or withoutCTLs as
described in Materials and Methods. After 24, 48, and 72 hours,
gels were lysed and viable cells were cultured in a colony-forming
assay. Nokilling would appear with 100þ colonies, and killing would
show very few colonies. A, graphs show number of viable tumor cells
recovered at indicated timepoints for IgG (left) and DTA-1 (middle)
for total tumors alone (blue line) or with activatedOT-1 T cells
(red line). Right, rate of B16 cell killing byOT-1CTL
(killingconstant k, as calculated inMateriala andMethods), of IgG
(dark gray) andDTA-1 (white) tumors is showncomparedwith primary
tissue cultureB16cells alone(light gray). B, viable tumor cells
recovered from cultures of IgG- and DTA-1–treated total tumors
alone (blue), with GITRþ/þ Pmel-1 (red), and GITR�/� Pmel-1(green).
Dashed lines indicate cultures that included the ex vivo addition
of 10 mg/mL of DTA-1; solid ones indicate control cultures.
Experiments wererepeated three times with tumors pooled from 3 to 5
mice for each experiment. Mean and � SEM of three experiments is
shown in A; a representativeexperiment is shown in B. �, P <
0.01.
Schaer et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology
Research328
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
activation of c-jun-NH2-kinase (JNK), it is unclear whetherDTA-1
causes a similar effect (38). JNK activation after long-term GITR-L
stimulus resulted in reduced Foxp3 mRNAexpression to a level that
we did not observe with DTA-1treatment. GITR and TNFR family
members use TNFR-asso-ciated factor (TRAF) proteins to transmit
downstream signals(8, 39). Because many TRAF proteins function as
E3 ubiquitinligases, one hypothesis could be that overstimulation
of GITRby DTA-1 could cause an intersection of this cascade
withFoxp3 protein and targeting it for degradation. Because
intra-tumor Tregs express less Foxp3 mRNA than peripheral
Tregs(Fig. 3B), this may make them uniquely sensitive to
GITR-induced degradation of Foxp3.A propensity to modulate pTregs
over tTregs would be a
logical assumption considering their unstable nature
(29).However, in the case of B16 melanoma, it seems that
themajority of intratumor Tregs have a tTreg-like phenotype, ashas
been seen in 4T1 tumors, and without a minor pTregpopulation as
seen in other tumors (25). In fact, transferexperiments into Rag�/�
mice established that a majority ofTregs can be rendered
susceptible to GITR-induced loss ofFoxp3. We found a similar
result, with 75% to 80% of Tregsmodulated in the tumor
microenvironment during DTA-1therapy in wild-type mice (% of
intratumor Treg Foxp3 lossþ % Foxp3þHeliosLOW Tregs; Supplementary
Fig. S2A andS2B). This suggests that the effects of DTA-1 are not
limitedto a minor subset of Tregs, such as pTregs. Regardless,
DTA-1treatment caused Tregs to lose Helios protein and
geneexpression, corresponding with increased levels of
inflamma-tory T-cell transcription factors, T-bet, RORgt, and
Eomes.Treg expression of T-bet or RORgt is not unprecedented,
andthe expression of these transcription factors is important
forthe Treg-suppressive function (29). Surprisingly, Eomes,
tra-ditionally thought of as a CD8þ CTL transcription factor,
ishighly upregulated in the DTA-1–treated Tregs. We havereported
recently that simulation of the closely related TNFRfamily member
OX40 has the ability to induce Eomes in CD4Teffs (40). Even though
there has been evidence that Tregscould control immunity through
granzyme-dependent killingof B cells, to date no role for Eomes in
Treg function has beendescribed (41). The significance of Eomes
expression in DTA-1modulation of Tregs will require further
investigation; how-ever, it exemplifies the level to which
overstimulation ofGITR on susceptible Tregs can alter their lineage
programThe end result of Treg lineage instability caused by
GITR
immunotherapy is the removal of intratumor suppressionmediated
by Tregs, as shown by the collagen-fibrin gel killingassay (Fig.
4). Using the same approach, we recently deter-mined that
intratumor immune suppression in B16 tumorsis Treg dependent, as
specific in vivo depletion of Tregsrestores killing of explanted
tumors (Budhu and Schaer;unpublished data). Whether or not the
DTA-1 effect is dueto reduced intratumor Treg numbers, Treg lineage
instabil-ity, or a combination of both remains to be
determined.Interestingly, even though GITR treatment removes
Tregsuppression and DTA-1–treated tumors are regressingin vivo,
tumor cells cocultured with total infiltrates continueto grow ex
vivo (Fig. 4). We interpret the need for additional
input of Teffs to continue killing as evidence that for
optimalin vivo therapy, GITR's ability to enhance CD8þ T-cell
numbersand persistence also plays an important role (42).
Consequent-ly, targeting Tregs seems to be a major mechanism for
DTA-1treatment along with its intrinsic effects on CD8þ T cells.
Thisconclusion is in agreement with our prior results showing
thatboth Tregs and Teffs must express GITR for the optimal
effectsof DTA-1 (17).
Development of new immunotherapies that accelerateantitumor
immunity is important, as checkpoint blockadedoes not benefit all
patients (2, 3). Our data show that ligationof GITR can accomplish
both goals. By inducing Treg lineageinstability, DTA-1 releases an
important source of suppres-sion of tumor immunity. At the same
time, we and others haveshown that GITR ligation by DTA-1
accelerates antitumorimmunity to take advantage of the now
permissive tumormicroenvironment (12, 17). The unique ability of
GITR ligationto target both axes, modulating Tregs primarily in the
tumormicroenvironment, supports the continued clinical develop-ment
of GITR agonist agents. Accordingly, in collaborationswith GITR
Inc., we are currently investigating the agonist anti-human GITR
antibody, TRX-518, in a phase I first-in-humantrial (GITR Inc.,
Clinical trials.gov: NCT01239134). We believethat the knowledge
gained from our study in understandingGITR mechanism of action will
help facilitate the develop-ment of appropriate biomarkers and
inform rational designof future clinical trials.
Disclosure of Potential Conflicts of InterestNo potential
conflicts of interest were disclosed.
Authors' ContributionsConception and design: D.A. Schaer, C.
Liu, A.D. Cohen, A.N. Houghton,T. Merghoub, J.D. WolchokDevelopment
of methodology: D.A. Schaer, C. Liu, A.D. Cohen, T.
MerghoubAcquisition of data (provided animals, acquired and managed
patients,provided facilities, etc.): D.A. Schaer, S. Budhu, C. Liu,
C.F. Bryson, N.M.Malandro, A.D. Cohen, H. Zhong, X. Yang, T.
MerghoubAnalysis and interpretation of data (e.g., statistical
analysis, biostatistics,computational analysis): D.A. Schaer, S.
Budhu, C. Liu, C.F. Bryson, N.M.Malandro, A.D. Cohen, T. Merghoub,
J.D. WolchokWriting, review, and/or revision of the manuscript:
D.A. Schaer, S. Budhu,T. Merghoub, J.D. WolchokAdministrative,
technical, or material support (i.e., reporting or orga-nizing
data, constructing databases): C. Liu, H. ZhongStudy supervision:
A.N. Houghton, T. Merghoub, J.D. Wolchok
AcknowledgmentsThe authors thank current and former Wolchok Lab
members: Dr.
Stephanie Terzulli, Andre Burey, Judith Murphy, Kelly Crowley,
RodgerPellegrini, Drs. Arvin Yang, and Francesca Avogadri for their
support on theGITR project; Rudensky lab members: Drs. Steve
Josefowicz, Rachel Niec,Ashutosh Chaudhry, and Robert Samstein for
generous sharing of reagentsand always being available for advice
and thoughtful discussion about Treglineage stability; Dr. Joe
Ponte for valuable shared insight on the mechanismof GITR
immunotherapy; Dr. Michael Curran for assistance with experimen-tal
design; members of the MSKCC flow cytometry, and molecular
cytologycore facilities; and Dr. Roberta Zappasodi for her very
helpful comments,critical reading, and editing of this
manuscript.
Grant SupportThis work was supported by NIH grants R01CA56821,
P01CA33049, and
P01CA59350 (to A.N. Houghton and J.D. Wolchok), D.A. Schaer was
supportedby the NIH Clinical Training for Scholar Grant K12
CA120121-01, and receivedsupport from the NIH/NCI Immunology
Training Grant T32 CA09149-30and JohnD. Proctor Foundation:Margaret
A. Cunningham ImmuneMechanismsin Cancer Research Fellowship Award;
Swim Across America; the Mr. William
GITR Induced Treg Lineage Instability
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013
329
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
H.Goodwin andMrs. AliceGoodwin and theCommonwealth Cancer
Foundationfor Research and the Experimental Therapeutics Center of
MSKCC (to J.D.Wolchok).
The costs of publication of this article were defrayed in part
by thepayment of page charges. This article must therefore be
hereby marked
advertisement in accordance with 18 U.S.C. Section 1734 solely
to indicatethis fact.
Received June 26, 2013; revised August 23, 2013; accepted
September 8, 2013;published OnlineFirst September 16, 2013.
References1. Schreiber RD, Old LJ, Smyth MJ. Cancer
immunoediting: integrating
immunity's roles in cancer suppression and promotion. Science
2011;331:1565–70.
2. Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA,
HaanenJB, et al. Improved survival with ipilimumab in patients with
metastaticmelanoma. N Engl J Med 2010;363:711–23.
3. Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC,
McDer-mott DF, et al. Safety, activity, and immune correlates of
anti-PD-1antibody in cancer. N Engl J Med 2012;366:2443–54.
4. Brahmer JR, Tykodi SS, Chow LQ, HwuWJ, Topalian SL, Hwu P, et
al.Safety and activity of anti-PD-L1 antibody in patients with
advancedcancer. N Engl J Med 2012;366:2455–65.
5. HamidO, Robert C, DaudA, Hodi FS, HwuW-J, Kefford R, et al.
Safetyand tumor responses with lambrolizumab (Anti–PD-1) in
melanoma. NEngl J Med 2013;369:134–44.
6. Wolchok JD, Kluger H, Callahan MK, Postow MA, Rizvi NA,
LesokhinAM, et al. Nivolumab plus ipilimumab in advancedmelanoma. N
Engl JMed 2013;369:122–33.
7. Royal RE, Levy C, Turner K, Mathur A, Hughes M, Kammula US,
et al.Phase 2 trial of single agent Ipilimumab (anti-CTLA-4) for
locallyadvanced or metastatic pancreatic adenocarcinoma. J
Immunother2010;33:828–33.
8. Snell LM, Lin GHY, McPherson AJ, Moraes TJ, Watts TH.
T-cellintrinsic effects of GITR and 4-1BB during viral infection
and cancerimmunotherapy. Immunol Rev 2011;244:197–217.
9. Weinberg AD, Morris NP, Kovacsovics-Bankowski M, Urba WJ,
CurtiBD. Science gone translational: the OX40 agonist story.
Immunol Rev2011;244:218–31.
10. Shimizu J, Yamazaki S, Takahashi T, Ishida Y, Sakaguchi S.
Stimu-lation of CD25(þ)CD4(þ) regulatory T cells through GITR
breaksimmunological self-tolerance. Nat Immunol 2002;3:135–42.
11. TurkMJ, Guevara-Patino JA, RizzutoGA, EngelhornME, Sakaguchi
S,Houghton AN. Concomitant tumor immunity to a poorly
immunogenicmelanoma is prevented by regulatory T cells. J Exp Med
2004;200:771–82.
12. Schaer DA, Murphy JT, Wolchok JD. Modulation of GITR for
cancerimmunotherapy. Curr Opin Immunol 2012;24:217–24.
13. Kanamaru F, Youngnak P, Hashiguchi M, Nishioka T, Takahashi
T,Sakaguchi S, et al. Costimulation via glucocorticoid-induced
TNFreceptor in both conventional and CD25þ regulatory CD4þ T
cells.J Immunol 2004;172:7306–14.
14. Stephens GL, McHugh RS, Whitters MJ, Young DA, Luxenberg
D,Carreno BM, et al. Engagement of glucocorticoid-induced
TNFRfamily-related receptor on effector T cells by its ligand
mediatesresistance to suppression by CD4þCD25þ T cells. J Immunol
2004;173:5008–20.
15. Ramirez-Montagut T, Chow A, Hirschhorn-Cymerman D, Terwey
TH,Kochman AA, Lu S, et al. Glucocorticoid-induced TNF receptor
familyrelated gene activation overcomes tolerance/ignorance to
melanomadifferentiation antigens and enhances antitumor immunity. J
Immunol2006;176:6434–42.
16. Cohen AD, Diab A, Perales MA, Wolchok JD, Rizzuto G,
Merghoub T,et al. Agonist anti-GITR antibody enhances
vaccine-induced CD8(þ)T-cell responses and tumor immunity. Cancer
Res 2006;66:4904–12.
17. CohenAD, Schaer DA, LiuC, Li Y,
Hirschhorn-CymmermanD,KimSC,et al. Agonist anti-GITR monoclonal
antibody induces melanomatumor immunity in mice by altering
regulatory T cell stability andintra-tumor accumulation. PLoS ONE
2010;5:e10436.
18. Coe D, Begom S, Addey C, White M, Dyson J, Chai JG.
Depletion ofregulatory T cells by anti-GITR mAb as a novel
mechanism for cancerimmunotherapy. Cancer Immunol Immunother
2010;59:1367–77.
19. Wang S, Bartido S, Yang G, Qin J, Moroi Y, Panageas KS, et
al. A rolefor a melanosome transport signal in accessing the MHC
class IIpresentation pathway and in eliciting CD4þ T cell
responses. J Immu-nol 1999;163:5820–6.
20. Budhu S, Loike JD, Pandolfi A, Han S, Catalano G,
Constantinescu A,et al. CD8þ T cell concentration determines their
efficiency in killingcognate antigen-expressing syngeneic mammalian
cells in vitro and inmouse tissues. J Exp Med 2010;207:223–35.
21. Komatsu N,Mariotti-Ferrandiz ME,Wang Y,Malissen
B,WaldmannH,Hori S. Heterogeneity of natural Foxp3þ T cells: a
committed regu-latory T-cell lineage and an uncommitted minor
population retainingplasticity. Proc Natl Acad Sci
2009;106:1903–8.
22. Ephrem A, Epstein AL, Stephens GL, Thornton AM, Glass D,
ShevachEM. Modulation of Treg cells/Teffector function by GITR
signaling iscontext-dependent. Eur J Immunol 2013May30. [Epub
aheadof print].
23. Yadav M, Louvet C, Davini D, Gardner JM, Martinez-Llordella
M,Bailey-Bucktrout S, et al. Neuropilin-1 distinguishes natural and
induc-ible regulatory T cells among regulatory T cell subsets in
vivo. J ExpMed 2012;209:1713–22.
24. Hansen W, Hutzler M, Abel S, Alter C, Stockmann C, Kliche S,
et al.Neuropilin 1 deficiency on CD4þFoxp3þ regulatory T cells
impairsmouse melanoma growth. J Exp Med 2012;209:2001–16.
25. Weiss JM, Bilate AM, Gobert M, Ding Y, Curotto de Lafaille
MA,Parkhurst CN, et al. Neuropilin 1 is expressed on
thymus-derivednatural regulatory T cells, but not mucosa-generated
induced Foxp3þT reg cells. J Exp Med 2012;209:1723–42.
26. GottschalkRA,Corse E, Allison JP. Expression ofHelios in
peripherallyinduced Foxp3þ regulatory T cells. J Immunology
2012;188:976–80.
27. Zabransky DJ, Nirschl CJ, Durham NM, Park BV, Ceccato CM,
BrunoTC, et al. Phenotypic and functional properties of Heliosþ
regulatory Tcells. PLoS ONE 2012;7:e34547.
28. SchaerDA, Li Y,MerghoubT, RizzutoGA,ShemeshA,CohenAD, et
al.Detection of intra-tumor self antigen recognition during
melanomatumor progression in mice using advanced multimode
confocal/twophoton microscope. PLoS ONE 2011;6:e21214.
29. Hori S. Stability of regulatory T-cell lineage. Adv Immunol
2011;112:1–24.
30. Chaudhry A, Samstein RM, Treuting P, Liang Y, Pils MC,
Heinrich JM,et al. Interleukin-10 signaling in regulatory T cells
is required forsuppression of Th17 cell-mediated inflammation.
Immunity 2011;34:566–78.
31. Getnet D, Grosso JF, GoldbergMV, Harris TJ, Yen HR, Bruno
TC, et al.A role for the transcription factor Helios in human
CD4þCD25þregulatory T cells. Mol Immunol 2010;47:1595–600.
32. Baine I, Basu S, Ames R, Sellers RS, Macian F. Helios
inducesepigenetic silencing of il2 gene expression in regulatory T
cells.J Immunol 2013;190:1008–16.
33. Setoguchi R, Hori S, Takahashi T, Sakaguchi S. Homeostatic
main-tenance of natural Foxp3þ CD25þ CD4þ regulatory T cells by
inter-leukin (IL)-2 and induction of autoimmune disease by IL-2
neutraliza-tion. J Exp Med 2005;201:723–35.
34. Fontenot JD, Rasmussen JP, Gavin MA, Rudensky AY. A function
forinterleukin 2 in Foxp3-expressing regulatory T cells. Nat
Immunol2005;6:1142–51.
35. Williams LM, Rudensky AY. Maintenance of the
Foxp3-dependentdevelopmental program inmature regulatory Tcells
requires continuedexpression of Foxp3. Nat Immunol
2007;8:277–84.
36. Miyao T, Floess S, Setoguchi R, Luche H, Fehling HJ,
Waldmann H,et al. Plasticity of Foxp3(þ) T cells reflects
promiscuous Foxp3 expres-sion in conventional T cells but not
reprogrammingof regulatory Tcells.Immunity 2012;36:262–75.
Schaer et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology
Research330
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
37. Zhou X, Bailey-Bucktrout SL, Jeker LT, Penaranda C,
Martinez-Llor-della M, Ashby M, et al. Instability of the
transcription factor Foxp3leads to the generation of pathogenic
memory T cells in vivo. NatImmunol 2009;10:1000–7.
38. Joetham A, Ohnishi H, Okamoto M, Takeda K, Schedel M,
Dome-nico J, et al. Loss of T regulatory cell suppression following
sig-naling through glucocorticoid-induced tumor necrosis
receptor(GITR) is dependent on c-Jun N-terminal kinase activation.
J BiolChem 2012;287:17100–8.
39. Hacker H, Tseng PH, Karin M. Expanding TRAF function: TRAF3
as atri-faced immune regulator. Nat Rev Immunol 2011;11:457–68.
40. Hirschhorn-Cymerman D, Budhu S, Kitano S, Liu C, Zhao F,
Zhong H,et al. Induction of tumoricidal function in CD4þ T cells is
associatedwith concomitant memory and terminally differentiated
phenotype.J Exp Med 2012;209:2113–26.
41. Zhao D-M, Thornton AM, DiPaolo RJ, Shevach EM.
ActivatedCD4þCD25þ T cells selectively kill B lymphocytes. Blood
2006;107:3925–32.
42. Snell LM, McPherson AJ, Lin GH, Sakaguchi S, Pandolfi PP,
RiccardiC, et al. CD8 T cell-intrinsic GITR is required for T cell
clonal expansionand mouse survival following severe influenza
infection. J Immunol2010;185:7223–34.
GITR Induced Treg Lineage Instability
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013
331
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/
-
2013;1:320-331. Published OnlineFirst September 16, 2013.Cancer
Immunol Res David A. Schaer, Sadna Budhu, Cailian Liu, et al.
through Loss of Regulatory T-cell Lineage StabilityGITR Pathway
Activation Abrogates Tumor Immune Suppression
Updated version
10.1158/2326-6066.CIR-13-0086doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerimmunolres.aacrjournals.org/content/suppl/2013/09/17/2326-6066.CIR-13-0086.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/1/5/320.full#ref-list-1
This article cites 41 articles, 19 of which you can access for
free at:
Citing articles
http://cancerimmunolres.aacrjournals.org/content/1/5/320.full#related-urls
This article has been cited by 20 HighWire-hosted articles.
Access the articles at:
E-mail alerts related to this article or journal.Sign up to
receive free email-alerts
Subscriptions
Reprints and
[email protected]
To order reprints of this article or to subscribe to the
journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take
you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/1/5/320To
request permission to re-use all or part of this article, use this
link
on June 12, 2021. © 2013 American Association for Cancer
Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst September 16, 2013; DOI:
10.1158/2326-6066.CIR-13-0086
http://cancerimmunolres.aacrjournals.org/lookup/doi/10.1158/2326-6066.CIR-13-0086http://cancerimmunolres.aacrjournals.org/content/suppl/2013/09/17/2326-6066.CIR-13-0086.DC1http://cancerimmunolres.aacrjournals.org/content/1/5/320.full#ref-list-1http://cancerimmunolres.aacrjournals.org/content/1/5/320.full#related-urlshttp://cancerimmunolres.aacrjournals.org/cgi/alertsmailto:[email protected]://cancerimmunolres.aacrjournals.org/content/1/5/320http://cancerimmunolres.aacrjournals.org/