Embed Size (px)
Citation preview

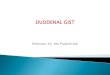
SCHEMATIC DIAGRAM
Predisposing Factors Precipitating Factors
GeneticsAge (50-69 years old) – 58 years old
mutation in exon 11 of the c-KIT (tyrosine kinase)
Overexpression and autophospholyzation of c-KIT
increased proliferation of insterstitial cells of Cajal(tumorigenesis)
GIST – Gastrointestinal Stromal Tumor
continued growth of GIST generates increasing pressure to surrounding tissue
weakening of the surrounding tissues’ blood vessels
rupture / damage of blood vessels
UPPER GI BLEEDING
StomachThe stomach is a J-shaped enlargement of the GI tract directly inferior to the diaphragm in the epigastric, umbilical, and left hypochondriac regions of the abdomen. The stomach connects the esophagus to the duodenum, the first part of the small intestine. Because a meal can be eaten much more quickly than the intestines can digest and absorb it, one of the functions of the stomach is to serve as a mixing chamber and holding reservoir. At appropriate intervals after food is ingested, the stomach forces a small quantity of material into the first portion of the small intestine. The position and size of the stomach vary continually; the diaphragm pushes it inferiorly with each inhalation and pulls it superiorly with each exhalation. Empty, it is about the size of a large sausage, but it is the most distensible part of the GI tract and can accommodate a large quantity of food. In the stomach, the digestion of starch continues, digestion of proteins and triglycerides begins, the semisolid bolus is converted into a liquid, and certain substances are absorbed.
black tarry stooldecreased Hct, HgbDOBsyncope
satiety / feeling of fullnessdyspepsiaperforation
bloody vomiting
abdominal discomfortnauseavomitingloss of appetite

AnatomyThe stomach has four main regions: the cardia, fundus, body and pylorus. The cardia surrounds the superior opening of the stomach. The rounded portion superior to and to the left of the cardia is the fundus.
Inferior to the fundus is the large central portion of the stomach called the body. The region of the stomach that connects to the duodenum is the pylorus; it has two parts, the pyloric antrum, which connects to the body of the stomach, and the pyloric canal which leads into the duodenum.
When the stomach is empty, the mucosa lies in large folds called ruggae that can be seen with the unaided eye. The pylorus communicates with the duodenum of the small intestine via a sphincter called the pyloric sphincter. The concave medial border of the stomach is called the lesser curvature, and the convex lateral border
is called the greater curvature.
HistologyThe stomach wall is composed of the same four basic layers as the rest of the GI tract, with certain modifications. The surface of the mucosa is a layer of simple columnar epithelial cells called surface mucous cells. The mucosa contains a lamina propria (areolar connective tissue) and a muscularis mucosae (smooth muscle).
Epithelial cells extend down into the lamina propria, where they form columns of secretory cells called gastric glands that line many narrow channels called gastric pits. Secretions from several gastric glands flow into each gastric pit and then into the lumen of the stomach. The gastric
glands contain three types of exocrine gland cells that secrete their products into the stomach lumen: mucous neck cells, chief cells and parietal cells. Both surface mucous cells and mucous neck cells secrete mucus. Parietal cells produce intrinsic factor (needed for absorption of Vitamin B12) and hydrochloric acid. The chief cells secrete pepsinogen and gastric lipase,
The secretion of the mucous parietal, and chief cells from gastric juice, which totals 2000-3000ml (roughly 2-3qt.) per day. In addiction gastric glands include a type of enteroendocrine cell, the G cell, which is located mainly in the pyloric antrum and secretes hormone gastrin into the bloodstream.
Three additional layers lie deep to the mucosa. The submucosa of the stomach is composed of areolar
connective tissue. The muscalaris has three layers of smooth muscle (rather than the two found in the small and large intestines): an outer longitudinal later, a middle circular layer and an inner oblique layer. The oblique layer is limited primarily to the body of the stomach. The serosa is composed of simple squamous epithelium (mesothelium) and areolar connective tissue; the portion of the serosa covering the stomach is part of the visceral peritoneum. At the lesser curvature if the stomach the visceral peritoneum extends upward to the liver as the lesser omentum. At the greater curvature of the stomach, the visceral peritoneum continues downward as the greater omentum drapes over the intestines.
Gastrointestinal Stromal TumorMesenchymal tumors of the gastrointestinal (GI) tract comprise a widely diverse group of neoplasms, completely separate from carcinomas or neuroendocrine tumors. This diverse grouping of tumors includes histopathological subtypes (e.g leiomyosarcoma, leiomyoma, neurofibroma, schwannoma, desmoid fibromatosis, benign and malignant vascular tumors, glomus tumor and other rare subtypes of sarcoma) that can also occur outside the GI tract; importantly thought the most common subtype of mesenchymal tumor of this origin system is the subtype known as gastrointestinal stromal tumor (GIST) that occurs exclusively within the abdomen, retropretineum and pelvis.

GISTs can occur at any age, although they are more common in adults with a peak incidence in the fifth and sixth decades of life. Although numbers vary from study to study it appears that males and females are affected equally. Although it is not possible to know the exact incidence of GISTs in the population these tumors are not common.
GISTs occur along the entire length of the GI tract but with different frequencies at different anatomical locations. Importantly GISTs from different GI sites of origin also exhibit different incidences of the underlying type of molecular mechanism: In other words the specific activating pathway (usually through a specific activating mutation in a signaling kinase such as the KIT pronco-oncogene) appears to correlate with the site of origin of the primary GIST.
Most small GIST lesions are asymptomatic. When large lesions are present, or if the tumor is highly infiltrative into vascular and neural structure initial symptoms may include abdominal fullness, pain nausea, dyspepsia, acute abdominal crisis with perforation, or evidence of GI bleeding. such as melena, hematemesis and anemia. (Kelsen, 2002) Gastrointestinal Stromal Tumors, or GISTs, are a relatively uncommon type of cancer that occurs in the gastrointestinal (GI) tract. GISTs are believed to start in special cells found in the wall of the GI tract, called the interstitial cells of Cajal (ICCs), or in very early cells that can develop into ICCs. ICCs are part of the autonomic nervous system, which sends signals to the GI tract. Some have called these cells the "pacemakers" of the gastrointestinal tract. The nerve signals they send cause muscles of the digestive organs to contract, which helps to move food and liquid through the GI tract. (Novartis Oncology,2009)
Although these tumors can start anywhere in the GI tract, they occur most often in the stomach (50% to 70%) or the small intestine (20% to 30%). The rest are found in the esophagus, large intestine (colon and rectum), and anus.
Interstitial Cells of Cajal
ICC serve a pacemaker cells to control autonomic function of the GI tract muscles. (Kelsen, 2002)
The Interstitial cell of Cajal (ICC) is a type of cell found in the gastrointestinal tract. It serves as a pacemaker that triggers gut contraction. Many types of smooth muscle tissues have now been shown to contain ICC, but with few exceptions the function of these cells is not known and is currently an area of active research. (Wikipedia, 2009)
Upper Gastrointestinal Bleeding
GI bleeding can originate anywhere from the mouth to the anus and can be overt or occult. The manifestations depend on the location and rate of bleeding.
Hematemesis is vomiting of red blood and indicates upper GI bleeding, usually from an arterial source or varix. Coffee-ground emesis is vomiting of dark brown, granular material that resembles coffee grounds. It results from upper GI bleeding that has slowed or stopped, with conversion of red Hb to brown hematin by gastric acid.
Hematochezia is the passage of gross blood from the rectum and
usually indicates lower GI bleeding but may result from vigorous upper GI bleeding with rapid transit of blood through the intestines.Melena is black, tarry stool and typically indicates upper GI bleeding, but bleeding from a source in the small bowel or right colon may also be the cause. About 100 to 200 mL of blood in the upper GI tract is required to cause melena, which may persist for several days after
Common Causes of GI BleedingUpper GI tract
Duodenal ulcer (20–30%)
Gastric or duodenal erosions (20–30%)
Varices (15–20%)
Gastric ulcer (10–20%)
Mallory-Weiss tear (5–10%)
Erosive esophagitis (5–10%)
Angioma (5–10%)
Arteriovenous malformation (< 5%)
Gastrointestinal stromal tumorsLower GI tract (percentages vary with the age group sampled)
Anal fissures
Angiodysplasia (vascular ectasia)
Colitis: radiation, ischemic, infectious
Colonic carcinoma
Colonic polyps
Diverticular disease
Inflammatory bowel disease: ulcerative proctitis/colitis, Crohn's disease
Internal hemorrhoidsSmall-bowel lesions (rare)
Angiomas
Arteriovenous malformations
Meckel's diverticulum
Tumors

bleeding has ceased. Black stool that does not contain occult blood may result from ingestion of iron, bismuth, or various foods and should not be mistaken for melena.
Chronic occult bleeding can occur from anywhere in the GI tract and is detectable by chemical testing of a stool specimen. Acute, severe bleeding also can occur from anywhere in the GI tract. Patients may present with signs of shock. Those with underlying ischemic heart disease may develop angina or MI because of hypoperfusion.
GI bleeding may precipitate hepatic encephalopathy (see Approach to the Patient With Liver Disease: Portal-Systemic Encephalopathy) or hepatorenal syndrome (kidney failure secondary to liver failure—see Approach to the Patient With Liver Disease: Renal and Electrolyte Abnormalities). Review of symptoms should include presence of abdominal discomfort, weight loss, easy bleeding or bruising, previous colonoscopy results, and symptoms of anemia (eg, weakness, easy fatigability, dizziness).
Physical examination: General examination focuses on vital signs and other indicators of shock or hypovolemia (eg, tachycardia, tachypnea, pallor, diaphoresis, oliguria, confusion) and anemia (eg, pallor, diaphoresis). Patients with lesser degrees of bleeding may simply have mild tachycardia (heart rate > 100). Orthostatic changes in pulse (a change of > 10 beats/min) or BP (a drop of ≥ 10 mm Hg) often develop after acute loss of ≥ 2 units of blood. However, orthostatic measurements are unwise in patients with severe bleeding (possibly causing syncope) and generally lack sensitivity and specificity as a measure of intravascular volume, especially in elderly patients.
External stigmata of bleeding disorders (eg, petechiae, ecchymoses) are sought, as are signs of chronic liver disease (eg, spider angiomas, ascites, palmar erythema) and portal hypertension (eg, splenomegaly, dilated abdominal wall veins).
A digital rectal examination is necessary to search for stool color, masses, and fissures. Anoscopy is done to diagnose hemorrhoids. Chemical testing of a stool specimen for occult blood completes the examination if gross blood is not present.
Red flags: Several findings suggest hypovolemia or hemorrhagic shock.
Syncope
Hypotension
Pallor
Diaphoresis
Tachycardia
Medical Management
Airway: A major cause of morbidity and mortality in patients with active upper GI bleeding is aspiration of blood with subsequent respiratory compromise. To prevent these problems, endotracheal intubation should be considered in patients who have inadequate gag reflexes or are obtunded or unconscious—particularly if they will be undergoing upper endoscopy.
Fluid resuscitation: IV fluids are initiated as for any patient with hypovolemia or hemorrhagic shock\: healthy adults are given normal saline IV in 500- to 1000-mL aliquots until signs of hypovolemia remit—up to a maximum of 2 L (for children, 20 mL/kg, that may be repeated once). Patients requiring further resuscitation should receive transfusion with packed RBCs. Transfusions continue until intravascular volume is restored and then are given as needed to replace ongoing blood loss. Transfusions in older patients or those with coronary artery disease may be stopped when Hct is stable at 30 unless the patient is symptomatic. Younger patients or those with chronic bleeding are usually not transfused unless Hct is < 23 or they have symptoms such as dyspnea or coronary ischemia.
Platelet count should be monitored closely; platelet transfusion may be required with severe bleeding. Patients who are taking antiplatelet drugs (eg, clopidogrel) have platelet dysfunction, often resulting in increased bleeding. Platelet transfusion should be considered when patients taking these drugs have severe ongoing bleeding, although a residual circulating drug (particularly clopidogrel) may inactivate transfused platelets. Fresh frozen plasma should be transfused after every 4 units of packed RBCs.
Nursing Management

Preoperative care and teachings which would include removing jewelry, nail polish, make-up, bowel preparation, supportive care, vital signs monitoring and administration of preoperative medications.
Insert a nasogastric tube if ordered pre-operatively. Although it is often inserted in the surgical site just prior to surgery, the nasogastric tube may be placed preoperatively to remove secretions and empty stomach contents.
Postoperative care that would include: assessment of gastric drainage (initial drainage is bright red, clear or greenish yellow in 2-3 days), maintain intravenous fluid while nasogastric suction is in place, monitor bowel sounds and abdominal distention (bowel sounds: indicating resumption of peristalsis, distention: third-spacing, obstruction, infection), resume oral food and fluids as ordered, encourage ambulation (to stimulate peristalsis).
Client with Gastrostomy or Jejunostomy Tube1. Assess tube placement by aspirating stomach contents2. Inspect the skin surrounding the insertion site for healing, redness, swelling, and the presence of any drainage.3. Assess the abdomen for distention, bowel sounds and tenderness.4. Until stoma is well healed, use sterile technique for dressing changes and site care.5. Cleansing surgical site with saline or soap and water, patting it dry with a 4X4 gauze and allow air to dry6. Irrigate the tube with 30-50ml of water, and clean the tube inside and out.7. Provide mouth care or remind client to do so.
Surgical ManagementWhen gastric cancer is identified prior to the development of metastasis, surgical removal of part or all of the stomach and regional lymph nodes is the treatment of choice. Partial gastrectomy involves removal of a portion of the stomach usually the distal half to two-thirds. In partial gastrectomy the surgeon constructs an anastamosis from the reaminder of the stomach directly to the duodenum or to the proximal jejunum. The gastroduodenostomy, or Billroth I, and the gastrojejunostomy, or BillRoth II, are commonly usued partial gastrectomy procedures. A total gastrectomy, removal of the entire stomach, may be done for diffuse cancer that is spread throughout the gastric mucosa but limited to the stomach. In a total gastrectomy, the surgeon constructs an anastamosis from the esophagus to to the duodenum or jejunum. Total gastrectomy with esophageal jejunostomy.
Sources:Kelsen, D., et.al. (2002) Principles and Practice of Gastrointestinal Oncology 2nd Edition pp.693-699Porth, C. (2005) Pathophysiology Concepts of Altered Health Status 7th Edition pp. 886-887 Tortora, G., Derrickson, B. (2006) Principles of Anatomy and Physiology 11th Edition pp. 911-913Lemone P., Burke, K. (2004) Medical Surgical Nursing Critical Thinking in Client Care 3 rd Edition Volume 1 pp.556-571Porter, R. (2004-2008) Merck Manual Online Edition: http://www.merck.com/mmpe/sec02/ch010/ch010a.html