Embed Size (px)
Citation preview
Gingival Status of Brazilian RenalTransplant Recipients UnderSirolimus-Based RegimensLuıs Otavio Miranda Cota,* Ana Paula Lima Oliveira,* Jose Eustaquio Costa,*Sheila Cavalca Cortelli,† and Fernando Oliveira Costa*
Background: Although the prevalence of gingival over-growth (GO) in calcineurin-inhibitor (CNI) immunosuppressiveregimens has been well documented, to the best of our knowl-edge data from sirolimus (SIR) regimens have not been de-scribed. We sought to investigate the gingival status of renaltransplant recipients under SIR-based regimens with regard tothe prevalence and potential risk variables associated with GO.
Methods: A cross-sectional study was conducted at a publichospital in Belo Horizonte, MG, Brazil. Of 886 transplant recip-ients, an eligible sample of 144 subjects was selected. Medical,pharmacologic, and periodontal variables were recorded foreach subject. GO was assessed through visual inspection andwas evaluated in relation to variables of interest by univariateand multivariate analyses.
Results: Although not clinically significant, 20.8% of thesamples had GO, with a mean GO score of 5.0% – 3.98%(range, 0% to 19%) and mean GO score per papilla of 0.378 –0.361 (range, 0.1 to 1.9); the percentage of papilla affectedby GO was 14.35% – 9.86% (range, 5% to 45%). The multivar-iate final model, excluding periodontal variables, showed thatthe concomitant use of calcium channel blockers (P = 0.033)and the interaction between time since transplant and previousCNI use (P <0.001) were associated with GO. Adding peri-odontal variables to the model improved its accuracy andretained papillary bleeding index as being strongly associatedwith GO (P <0.001).
Conclusions: GO was observed in a considerable number ofsubjects under SIR-based immunosuppressive regimens, al-though the relationship was not clinically significant. Findingspoint to the importance of cooperation between medical anddental health care personnel in the maintenance of renal trans-plant recipients under SIR-based immunosuppressive regi-mens. J Periodontol 2008;79:2060-2068.
KEY WORDS
Gingival overgrowth; renal transplantation; risk; sirolimus.
Renal transplantation has progressedover the years to become a verysuccessful and routine procedure.
It has been a key advancement in thetreatment of end-stage renal disease byimproving quality of life and patient sur-vival. Allograft and recipient survivalhave improved significantly.1,2 Calcineu-rin inhibitor (CNI) agents, primarily cy-closporin A (CsA) and, later, tacrolimus(Tcr), have become the foundations ofimmunosuppressive therapy since theearly 1980s. Despite substantial enhance-ment of short-term survival rates, thelong-term graft outcome has remainedvirtually unchanged.2,3
Therefore, the goals of immunosup-pressive therapies have changed overthe last decade. With high graft survivalrates and a low incidence of acute re-jection, strategies have shifted towardeliminating acute rejection, decreasingchronic nephropathy, improving long-term outcomes, and reducing the side ef-fects of medications.4,5 The nephrotoxicand extrarenal adverse effects of CNIagents, suchashypertensive,dyslipidemic,atherosclerotic, diabetogenic, infectious,and carcinogenic events, seem to havean important negative impact on long-term graft survival.2,6-8
Newimmunosuppressive tailoringstrat-egies that can prevent allograft losseswhile maintaining immunosuppressionefficacy and controlling adverse effectsare of great interest. Although the optimal
* Department of Periodontology, Dentistry School, Federal University of Minas Gerais, BeloHorizonte, MG, Brazil.
† Department of Dentistry, Periodontics Research Division, University of Taubate, Taubate,SP, Brazil.
doi: 10.1902/jop.2008.080194
Volume 79 • Number 11
2060

regimen has not been defined, the availability of sev-eral agents permits the regimen to be individualized.9
Several CNI minimization strategies have been re-ported, involving early complete CNI avoidance, CNItapering, or CNI withdrawal. Some of these strategiesinclude mycophenolate mofetil (MMF) or sirolimus(SIR) administration alone or in combination mainte-nance therapies.10-12
SIR is an inhibitor of the mammalian target of rapa-mycin, a molecule that is important in the regulationof cellular activation in response to growth factors. Asa result, SIR acts later in the cell cycle to inhibit the cy-tokine-stimulated proliferation of T cells, resulting ingrowth arrest late in the G phase.13
Some investigators14,15 speculated that SIR immu-nosuppressive regimens might dramatically changethe natural course of chronic allograft nephropathyand may influence long-term patient survival. Al-though some protocols seem to reduce the risk foracute rejection and chronic allograft nephropathy, ad-verse effects were reported in SIR-based maintenanceregimens,12,13 including inferior patient and allograftoutcomes,16 such as hyperlipidemia, delayed woundhealing, lymphocele, arthralgias, thrombocytopenia,and protocol deviations.12,13,17-19
Gingival overgrowth (GO) is a well-recognized andresearched oral side effect of CNI-based immunosup-pressive regimens. GO is characterized by a distur-bance in collagen metabolism leading to excessiveaccumulation of type I collagen fibers in gingival con-nective tissue with an unbalanced cytokine profile andvarious degrees of inflammation, including vascularand epithelium changes, edema, and plasma cell in-filtrate.20,21 It is a significant, disfiguring, and uncom-fortable condition for affected subjects.
The prevalence rates of this disorder vary greatlyfor CNI immunosuppressive regimens. Prevalencestudies22-25 revealed that ;25% to 81% of patientsmedicated with CsA, alone or in combination withother drugs, experienced GO. Reports23,26,27 on GOin Tcr-treated subjects suggested that prevalencerates are lower than in subjects taking CsA and thatthe GO tends to be less severe.
Prevalence data for GO in CsA and Tcr regimenshave been well documented in the dental litera-ture.22-31 However, to the best of our knowledge, dataon gingival status with SIR regimens have not beendescribed, nor have the occurrence of GO and the re-lationships between gingival status and different phar-macologic, demographic, and periodontal variables.
Therefore, the aim of the present study was to in-vestigate the gingival status of renal transplant sub-jects under SIR immunosuppressive regimens, todetermine the prevalence and severity of GO, and toinvestigate the effects of potential risk variables asso-ciated with GO in this group of subjects.
MATERIALS AND METHODS
Study Design and Sampling StrategyThe present cross-sectional study was conducted ata public hospital in Belo Horizonte, MG, Brazil. Thestudy was approved by the research ethics commit-tees of the Federal University of Minas Gerais (ETIC514/05) and Felıcio Rocho Hospital (CEP/HFR 141/05), Belo Horizonte, MG, Brazil. Participants were in-formed of the aims of the study and provided writteninformed consent prior to their participation in thestudy. Subjects’ rights were protected at all times.
An eligible sample was selected and recruitedfrom the organ transplant unit of the Felıcio RochoHospital, where they were seen on a regular basis tomonitor drug therapy and graft survival. Eight hun-dred eighty-six subjects who received solid organtransplants, including liver, kidney, and pancreastransplants, were under immunosuppressive main-tenance therapy in the hospital unit during the periodof the study. Of these subjects, 623 were renal trans-plant recipients, and 239 were under SIR-basedregimens. Data were collected through patient ques-tionnaires, medical records, and periodontal exami-nation from February to October 2007. During theperiod of data collection, patients meeting the inclu-sion criteria were randomly invited to participate inthe study. According to their accessibility and avail-ability in the post-transplant maintenance routine,subjects were selected and underwent gingival eval-uation.
Participants were all renal transplant recipients,under an SIR-based immunosuppressive therapy,‡2 months post-transplant, ‡18 years old at the timeof examination, and had a minimum of six of the 12most anterior teeth in the upper or lower dentalarches. Subjects under combined SIR/CNI therapiesand current and former smokers were excluded fromthe study. Based on these criteria, the final sampleconsisted of 144 subjects.
GO was assessed in relation to the following vari-ables: age, gender, weight, creatinine level, plaquescore,32 papillary bleeding index,33 time since trans-plant, SIR dosage, SIR serum level, prednisone andMMF dosages, previous CNI use, and concomitantcalcium channel blocker (CCB) use.
Medical and Pharmacologic VariablesMedical and pharmacologic data were obtained fromeach subject’s medical records. As part of long-termmanagement, transplant recipients were screenedregularly for whole blood and serum concentrationsof SIR. Data from the most recent assessment, usuallythe last medical examination, were recorded and usedin the analysis. Patients’ medical records were exam-ined thoroughly, and data were confirmed by the or-gan transplant medical group.
J Periodontol • November 2008 Cota, Oliveira, Costa, Cortelli, Costa
2061

Gingival AssessmentsAfter the examination of patients’ medical records,subjects were scheduled for gingival evaluation. Peri-odontal assessment through clinical attachment leveland probing depth was not performed because the de-pendent variable in this study was related to gingivalchanges. The periodontal condition of the sample wasassessed through indicators of inflammation and oralhygiene, such as the papillary bleeding index and theplaque index.27 This methodologic approach wassupported by cross-sectional studies23,24,26,27 thatdemonstrated that gingival bleeding is a good indica-tor of the role of inflammation induced by bacterialplaque in GO severity.
Gingival evaluation was performed by one trainedand calibrated periodontist who was masked to eachpatient’s identity, medical history, and immunosup-pressive regimen. Examiner calibration was done atthe beginning of the study and repeated 1 month laterto determine intraexaminer reliability. For this pur-pose, papillary bleeding index and GO scores of 10subjects were evaluated, and all unweighted kappascores were >0.92.
The level of oral hygiene score was obtained ac-cording to the plaque index.32 Measurements wereperformed on the lingual, labial, and interproximalsurfaces of the six most anterior teeth in the upperand lower arches. Scores for each site were totaled,and the mean values were attained. The papillarybleeding index was recorded in the interproximal pa-pillae of the six most anterior teeth in both arches.33
The present study assessed GO in the 12 most an-terior teeth based on previous reports25,34,35 thatdemonstrated higher occurrence rates of GO in the an-terior area. GO of upper and lower anterior teeth wasevaluated through visual inspection, as previously de-scribed.23,24 Scores between 0 and 5, depending onthe amount of horizontal and vertical enlargement,were assigned to each buccal and lingual papilla ofthe six most anterior upper and lower teeth. Basedon the number of anterior teeth available on each den-tal arch, a total of 20 papillae could be selected andexamined. The potential maximum GO score was100, and it was expressed as a percentage. Subjectswith GO scores ‡30 were classified as having clinicallysignificant overgrowth, as previously suggested.35
Statistical AnalysisAll individual patient data were collected and ana-lyzed using statistical software.‡ Samples were di-vided according to the presence (GO+) and absence(GO-) of GO, as well as the concomitant use ofCCB and the previous use of CNI. These groups werefirst described in relation to demographic, pharmaco-logic, and periodontal variables. The comparison ofvariables among the groups was performed using
the unpaired independent-sample t test and the x2 sta-tistic, as appropriate.
The effect of a range of independent variables onthe occurrence of GO was assessed using multivariatelogistic regression analysis. Two different models,excluding and including periodontal variables, werecreated. Then, all corresponding variables for eachmodel were selected to enter the multivariate regres-sion and were retained if significant P values (P <0.05)were attained. First-order interactions among timesince transplant, CCB use, and previous CNI use weretested in the models and retained if significant.
Regression coefficients, their 95% confidence inter-vals (CIs), odds ratio (OR) estimates, and P valueswere also determined. Areas under the receiver oper-ating characteristic (ROC) curves, an estimate of ac-curacy for the models, were reported.
RESULTS
Findings from the present study revealed no clinicallysignificant GO (‡30%) among subjects under SIR reg-imens. However, when scores <30% were considered,a GO prevalence of 20.8% (n = 30) was observed. Thetotal sample showed that 2.99% – 7.34% (range, 0% to45%) of papilla were affected by GO, with a mean GOscore per papilla of 0.08 – 0.22 (range, 0 to 1.9); themean GO score was 1.04% – 2.71% (range, 0% to19%). Among GO+ subjects, 18.8% (n = 27) showedGO scores from 1% to 10%, and 2.1% (n = 3) showedscores from 11% to 19%. No GO score >19% was ob-served. In addition, the mean GO score was 5.0% –3.98% (range, 0% to 19%), the mean GO score per pa-pilla was 0.378 – 0.361 (range, 0.1 to 1.9), and thepercentage of papilla affected by GO was 14.35% –9.86% (range, 5% to 45%).
Demographic, pharmacologic, and periodontalvariables in GO+ and GO- subjects are detailed inTable 1. GO+ group showed a longer time sincetransplant (P = 0.011), a greater number of subjectswith concomitant CCB use (P = 0.005), and a highernumber of subjects with previous CNI use (P = 0.005)compared to those without GO. A marginally sig-nificant association was observed between male gen-der and GO (P = 0.051). No significant differenceswere observed in relation to SIR dosage and serumconcentrations or other non-periodontal variables.With regard to periodontal variables, GO+ subjectsshowed a higher papillary bleeding index (P <0.001)and a higher percentage of papilla with bleeding uponstimulation (P <0.001) compared to GO- subjects(Table 1).
Demographic, pharmacologic, and periodontalvariables of the subjects, divided according to the
‡ Statistical Package for Social Sciences, Version 9.0 for Windows, SPSS,Chicago, IL.
Gingival Status in Sirolimus Immunosuppressive Regimens Volume 79 • Number 11
2062
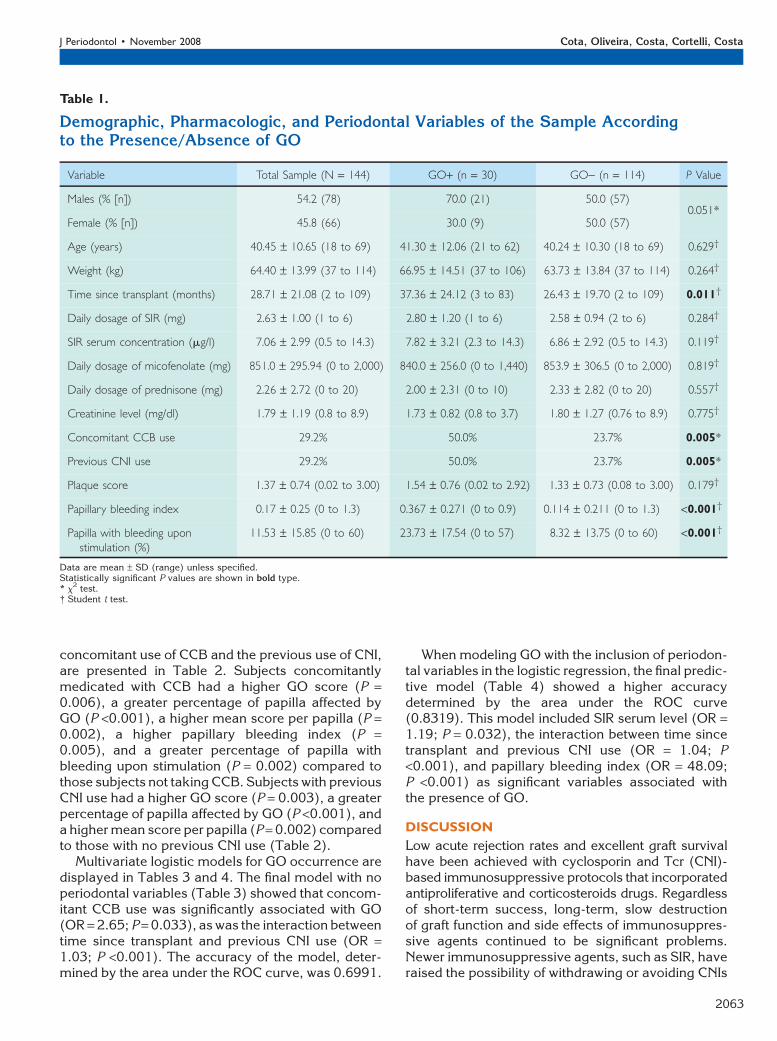
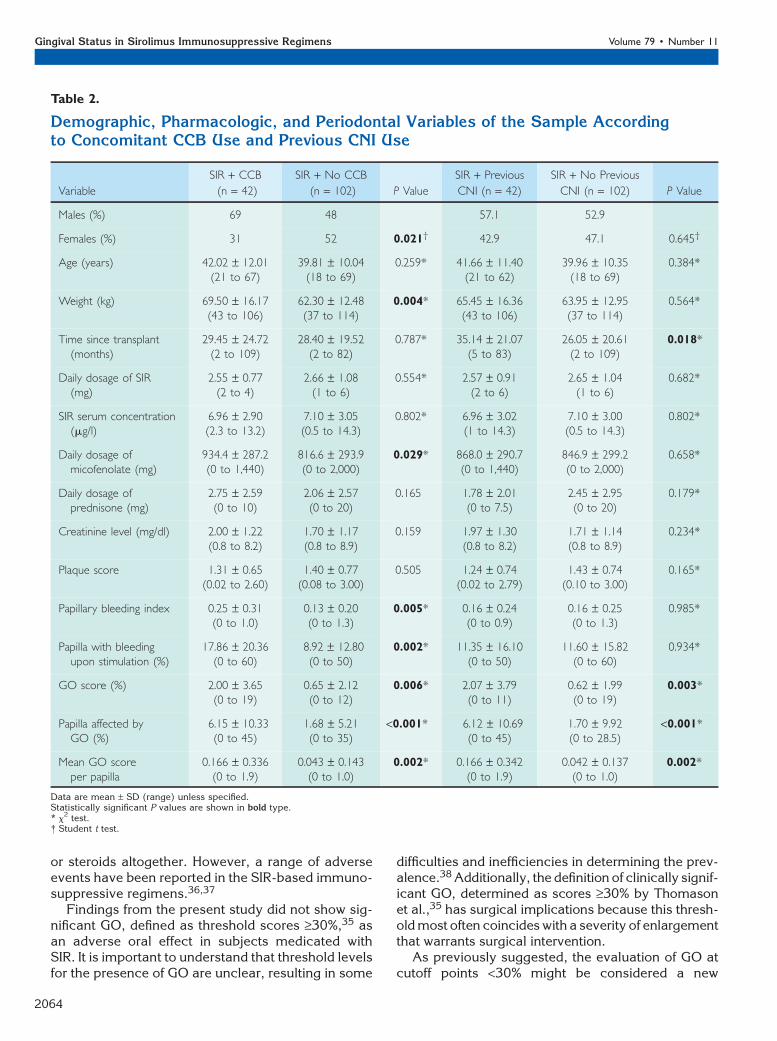
concomitant use of CCB and the previous use of CNI,are presented in Table 2. Subjects concomitantlymedicated with CCB had a higher GO score (P =0.006), a greater percentage of papilla affected byGO (P <0.001), a higher mean score per papilla (P =0.002), a higher papillary bleeding index (P =0.005), and a greater percentage of papilla withbleeding upon stimulation (P = 0.002) compared tothose subjects not taking CCB. Subjects with previousCNI use had a higher GO score (P = 0.003), a greaterpercentage of papilla affected by GO (P <0.001), anda higher mean score per papilla (P = 0.002) comparedto those with no previous CNI use (Table 2).
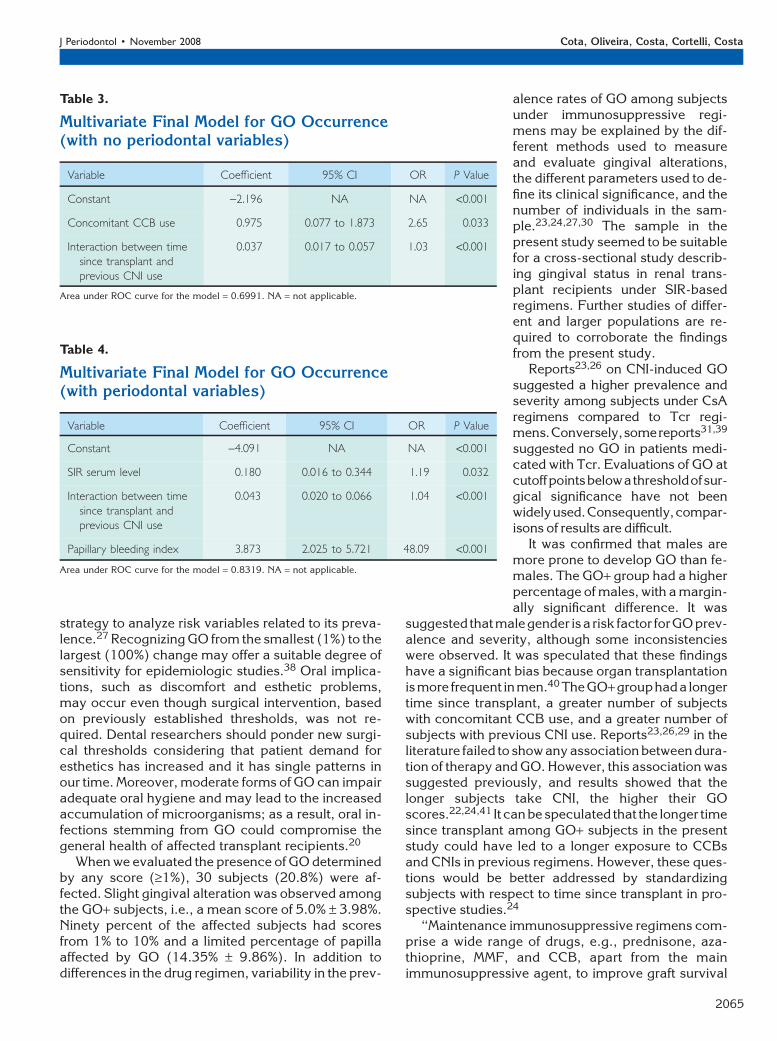
Multivariate logistic models for GO occurrence aredisplayed in Tables 3 and 4. The final model with noperiodontal variables (Table 3) showed that concom-itant CCB use was significantly associated with GO(OR = 2.65; P = 0.033), as was the interaction betweentime since transplant and previous CNI use (OR =1.03; P <0.001). The accuracy of the model, deter-mined by the area under the ROC curve, was 0.6991.
When modeling GO with the inclusion of periodon-tal variables in the logistic regression, the final predic-tive model (Table 4) showed a higher accuracydetermined by the area under the ROC curve(0.8319). This model included SIR serum level (OR =1.19; P = 0.032), the interaction between time sincetransplant and previous CNI use (OR = 1.04; P<0.001), and papillary bleeding index (OR = 48.09;P <0.001) as significant variables associated withthe presence of GO.
DISCUSSION
Low acute rejection rates and excellent graft survivalhave been achieved with cyclosporin and Tcr (CNI)-based immunosuppressive protocols that incorporatedantiproliferative and corticosteroids drugs. Regardlessof short-term success, long-term, slow destructionof graft function and side effects of immunosuppres-sive agents continued to be significant problems.Newer immunosuppressive agents, such as SIR, haveraised the possibility of withdrawing or avoiding CNIs
Table 1.
Demographic, Pharmacologic, and Periodontal Variables of the Sample Accordingto the Presence/Absence of GO
Variable Total Sample (N = 144) GO+ (n = 30) GO- (n = 114) P Value
Males (% [n]) 54.2 (78) 70.0 (21) 50.0 (57)0.051*
Female (% [n]) 45.8 (66) 30.0 (9) 50.0 (57)
Age (years) 40.45 – 10.65 (18 to 69) 41.30 – 12.06 (21 to 62) 40.24 – 10.30 (18 to 69) 0.629†
Weight (kg) 64.40 – 13.99 (37 to 114) 66.95 – 14.51 (37 to 106) 63.73 – 13.84 (37 to 114) 0.264†
Time since transplant (months) 28.71 – 21.08 (2 to 109) 37.36 – 24.12 (3 to 83) 26.43 – 19.70 (2 to 109) 0.011†
Daily dosage of SIR (mg) 2.63 – 1.00 (1 to 6) 2.80 – 1.20 (1 to 6) 2.58 – 0.94 (2 to 6) 0.284†
SIR serum concentration (mg/l) 7.06 – 2.99 (0.5 to 14.3) 7.82 – 3.21 (2.3 to 14.3) 6.86 – 2.92 (0.5 to 14.3) 0.119†
Daily dosage of micofenolate (mg) 851.0 – 295.94 (0 to 2,000) 840.0 – 256.0 (0 to 1,440) 853.9 – 306.5 (0 to 2,000) 0.819†
Daily dosage of prednisone (mg) 2.26 – 2.72 (0 to 20) 2.00 – 2.31 (0 to 10) 2.33 – 2.82 (0 to 20) 0.557†
Creatinine level (mg/dl) 1.79 – 1.19 (0.8 to 8.9) 1.73 – 0.82 (0.8 to 3.7) 1.80 – 1.27 (0.76 to 8.9) 0.775†
Concomitant CCB use 29.2% 50.0% 23.7% 0.005*
Previous CNI use 29.2% 50.0% 23.7% 0.005*
Plaque score 1.37 – 0.74 (0.02 to 3.00) 1.54 – 0.76 (0.02 to 2.92) 1.33 – 0.73 (0.08 to 3.00) 0.179†
Papillary bleeding index 0.17 – 0.25 (0 to 1.3) 0.367 – 0.271 (0 to 0.9) 0.114 – 0.211 (0 to 1.3) <0.001†
Papilla with bleeding uponstimulation (%)
11.53 – 15.85 (0 to 60) 23.73 – 17.54 (0 to 57) 8.32 – 13.75 (0 to 60) <0.001†
Data are mean – SD (range) unless specified.Statistically significant P values are shown in bold type.* x
2 test.† Student t test.
J Periodontol • November 2008 Cota, Oliveira, Costa, Cortelli, Costa
2063
or steroids altogether. However, a range of adverseevents have been reported in the SIR-based immuno-suppressive regimens.36,37
Findings from the present study did not show sig-nificant GO, defined as threshold scores ‡30%,35 asan adverse oral effect in subjects medicated withSIR. It is important to understand that threshold levelsfor the presence of GO are unclear, resulting in some
difficulties and inefficiencies in determining the prev-alence.38 Additionally, the definition of clinically signif-icant GO, determined as scores ‡30% by Thomasonet al.,35 has surgical implications because this thresh-old most often coincides with a severity of enlargementthat warrants surgical intervention.
As previously suggested, the evaluation of GO atcutoff points <30% might be considered a new
Table 2.
Demographic, Pharmacologic, and Periodontal Variables of the Sample Accordingto Concomitant CCB Use and Previous CNI Use
Variable
SIR + CCB
(n = 42)
SIR + No CCB
(n = 102) P Value
SIR + Previous
CNI (n = 42)
SIR + No Previous
CNI (n = 102) P Value
Males (%) 69 48 57.1 52.9
Females (%) 31 52 0.021† 42.9 47.1 0.645†
Age (years) 42.02 – 12.01(21 to 67)
39.81 – 10.04(18 to 69)
0.259* 41.66 – 11.40(21 to 62)
39.96 – 10.35(18 to 69)
0.384*
Weight (kg) 69.50 – 16.17(43 to 106)
62.30 – 12.48(37 to 114)
0.004* 65.45 – 16.36(43 to 106)
63.95 – 12.95(37 to 114)
0.564*
Time since transplant(months)
29.45 – 24.72(2 to 109)
28.40 – 19.52(2 to 82)
0.787* 35.14 – 21.07(5 to 83)
26.05 – 20.61(2 to 109)
0.018*
Daily dosage of SIR(mg)
2.55 – 0.77(2 to 4)
2.66 – 1.08(1 to 6)
0.554* 2.57 – 0.91(2 to 6)
2.65 – 1.04(1 to 6)
0.682*
SIR serum concentration(mg/l)
6.96 – 2.90(2.3 to 13.2)
7.10 – 3.05(0.5 to 14.3)
0.802* 6.96 – 3.02(1 to 14.3)
7.10 – 3.00(0.5 to 14.3)
0.802*
Daily dosage ofmicofenolate (mg)
934.4 – 287.2(0 to 1,440)
816.6 – 293.9(0 to 2,000)
0.029* 868.0 – 290.7(0 to 1,440)
846.9 – 299.2(0 to 2,000)
0.658*
Daily dosage ofprednisone (mg)
2.75 – 2.59(0 to 10)
2.06 – 2.57(0 to 20)
0.165 1.78 – 2.01(0 to 7.5)
2.45 – 2.95(0 to 20)
0.179*
Creatinine level (mg/dl) 2.00 – 1.22(0.8 to 8.2)
1.70 – 1.17(0.8 to 8.9)
0.159 1.97 – 1.30(0.8 to 8.2)
1.71 – 1.14(0.8 to 8.9)
0.234*
Plaque score 1.31 – 0.65(0.02 to 2.60)
1.40 – 0.77(0.08 to 3.00)
0.505 1.24 – 0.74(0.02 to 2.79)
1.43 – 0.74(0.10 to 3.00)
0.165*
Papillary bleeding index 0.25 – 0.31(0 to 1.0)
0.13 – 0.20(0 to 1.3)
0.005* 0.16 – 0.24(0 to 0.9)
0.16 – 0.25(0 to 1.3)
0.985*
Papilla with bleedingupon stimulation (%)
17.86 – 20.36(0 to 60)
8.92 – 12.80(0 to 50)
0.002* 11.35 – 16.10(0 to 50)
11.60 – 15.82(0 to 60)
0.934*
GO score (%) 2.00 – 3.65(0 to 19)
0.65 – 2.12(0 to 12)
0.006* 2.07 – 3.79(0 to 11)
0.62 – 1.99(0 to 19)
0.003*
Papilla affected byGO (%)
6.15 – 10.33(0 to 45)
1.68 – 5.21(0 to 35)
<0.001* 6.12 – 10.69(0 to 45)
1.70 – 9.92(0 to 28.5)
<0.001*
Mean GO scoreper papilla
0.166 – 0.336(0 to 1.9)
0.043 – 0.143(0 to 1.0)
0.002* 0.166 – 0.342(0 to 1.9)
0.042 – 0.137(0 to 1.0)
0.002*
Data are mean – SD (range) unless specified.Statistically significant P values are shown in bold type.* x
2 test.† Student t test.
Gingival Status in Sirolimus Immunosuppressive Regimens Volume 79 • Number 11
2064
strategy to analyze risk variables related to its preva-lence.27 Recognizing GO from the smallest (1%) to thelargest (100%) change may offer a suitable degree ofsensitivity for epidemiologic studies.38 Oral implica-tions, such as discomfort and esthetic problems,may occur even though surgical intervention, basedon previously established thresholds, was not re-quired. Dental researchers should ponder new surgi-cal thresholds considering that patient demand foresthetics has increased and it has single patterns inour time. Moreover, moderate forms of GO can impairadequate oral hygiene and may lead to the increasedaccumulation of microorganisms; as a result, oral in-fections stemming from GO could compromise thegeneral health of affected transplant recipients.20
When we evaluated the presence of GO determinedby any score (‡1%), 30 subjects (20.8%) were af-fected. Slight gingival alteration was observed amongthe GO+ subjects, i.e., a mean score of 5.0% – 3.98%.Ninety percent of the affected subjects had scoresfrom 1% to 10% and a limited percentage of papillaaffected by GO (14.35% – 9.86%). In addition todifferences in the drug regimen, variability in the prev-
alence rates of GO among subjectsunder immunosuppressive regi-mens may be explained by the dif-ferent methods used to measureand evaluate gingival alterations,the different parameters used to de-fine its clinical significance, and thenumber of individuals in the sam-ple.23,24,27,30 The sample in thepresent study seemed to be suitablefor a cross-sectional study describ-ing gingival status in renal trans-plant recipients under SIR-basedregimens. Further studies of differ-ent and larger populations are re-quired to corroborate the findingsfrom the present study.
Reports23,26 on CNI-induced GOsuggested a higher prevalence andseverity among subjects under CsAregimens compared to Tcr regi-mens.Conversely,somereports31,39
suggested no GO in patients medi-cated with Tcr. Evaluations of GO atcutoffpointsbelowathresholdofsur-gical significance have not beenwidelyused.Consequently,compar-isons of results are difficult.
It was confirmed that males aremore prone to develop GO than fe-males. The GO+ group had a higherpercentage of males, with a margin-ally significant difference. It was
suggested thatmalegender isa risk factor forGOprev-alence and severity, although some inconsistencieswere observed. It was speculated that these findingshave a significant bias because organ transplantationismore frequent inmen.40 TheGO+grouphada longertime since transplant, a greater number of subjectswith concomitant CCB use, and a greater number ofsubjects with previous CNI use. Reports23,26,29 in theliterature failed to show any association betweendura-tion of therapy and GO. However, this association wassuggested previously, and results showed that thelonger subjects take CNI, the higher their GOscores.22,24,41 It canbespeculated that the longer timesince transplant among GO+ subjects in the presentstudy could have led to a longer exposure to CCBsand CNIs in previous regimens. However, these ques-tions would be better addressed by standardizingsubjects with respect to time since transplant in pro-spective studies.24
‘‘Maintenance immunosuppressive regimens com-prise a wide range of drugs, e.g., prednisone, aza-thioprine, MMF, and CCB, apart from the mainimmunosuppressive agent, to improve graft survival
Table 3.
Multivariate Final Model for GO Occurrence(with no periodontal variables)
Variable Coefficient 95% CI OR P Value
Constant -2.196 NA NA <0.001
Concomitant CCB use 0.975 0.077 to 1.873 2.65 0.033
Interaction between timesince transplant andprevious CNI use
0.037 0.017 to 0.057 1.03 <0.001
Area under ROC curve for the model = 0.6991. NA = not applicable.
Table 4.
Multivariate Final Model for GO Occurrence(with periodontal variables)
Variable Coefficient 95% CI OR P Value
Constant -4.091 NA NA <0.001
SIR serum level 0.180 0.016 to 0.344 1.19 0.032
Interaction between timesince transplant andprevious CNI use
0.043 0.020 to 0.066 1.04 <0.001
Papillary bleeding index 3.873 2.025 to 5.721 48.09 <0.001
Area under ROC curve for the model = 0.8319. NA = not applicable.
J Periodontol • November 2008 Cota, Oliveira, Costa, Cortelli, Costa
2065

and patient systemic status.’’24 Previous re-ports23,26,40 showed that the concomitant use of someof these drugs may contribute to adverse oral sideeffects.
The effects of CCBs on GO are well documented inthe literature. It was shown that CCBs can indepen-dently induce GO, albeit at a lower prevalence ratethan CsA.42,43 CCBs were also determined to be asso-ciated with the prevalence and severity of GO underCNI-based regimens.23,26,30,40,42 Findings from thepresent study demonstrated that a greater percentageof GO+ subjects were concomitantly medicated withCCBs. In addition, patients medicated with SIR +CCB showed a greater severity of GO compared tothose with no concomitant CCB use. Speculation thatGO among subjects under SIR-based regimens can besolely attributed to CCB use during immunosuppres-sive therapy should be addressed in further studiesbecause subjects not medicated with CCB alsoshowed some level of gingival alterations.
A significant number of transplanted subjects usedCsA before changing to Tcr. Some reports26,28-30
showed that the CsA-induced GO decreased, but itwas not eliminated when the therapy was changed.In this regard, GO observed in subjects treated withTcr with previous exposure to CsA could be a resultof a residual effect of CsA. Likewise, subjects underSIR-based regimens have been previously treatedwith CsA and/or Tcr. It can also be hypothesized thatgingival alterations among subjects medicated withSIR may be a result of previous CNI exposure. Resultsshowed a greater percentage of subjects with previ-ous CNI use among GO+ subjects. In addition, pa-tients previously exposed to CNI therapies showedhigher severity of GO compared to those with no pre-vious CNI use.
It is known that GO may regress or disappear withimmunosuppressive agent substitution. However,it may take 6 to 12 months after discontinuation ofthe offending drug for GO to resolve. The time sincereplacement of CNI with SIR was 7.25 – 5.74 months(range, 2 to 20 months; data not shown). The chal-lenge of future studies is to gather information fromtransplant recipients who have been medicated withSIR, but not CNI, and have no CCB concomitant use tobetter address gingival status related solely to SIR use.
In the present study, no association between plaqueindex and GO was demonstrated, although this as-sociation was stated elsewhere.39,40 GO+ subjects un-der SIR-based regimens showed a higher papillarybleeding index and a greater percentage of papilla withbleeding upon stimulation compared to GO- subjects.The positive association between gingival inflamma-tion and GO is widely accepted.23,26,27,39-41 Neverthe-less, most evidence to support this association hasbeen derived from cross-sectional studies. As a result,
it is not clear whether inflammation is a contributoryfactor or a consequence of the gingival changes.Therefore, it is difficult to determine which side of therelationship is causal.40,41
Inthemultivariateanalysis, thefirstpredictivemodelwas created with no periodontal variables included.This model showed concomitant CCB use and the in-teraction between time since transplant and previousCNI use as significant risk variables for the presenceof GO. This interaction may reflect the longer exposureofGO+ subjects toCNIagents inprevious immunosup-pressive regimensandmay indicate that gingival alter-ationsarea residualeffectofpastCNIexposure.Addedtogether, this observed interaction and the concomi-tant CCB use might have increased the prevalenceand severity of gingival changes. It was demonstratedthat the higher GO scores were observed within regi-mens including CsA and CCBs.23,26,39 It also was sug-gested that CsA, taken at low dosages and not incombination with CCBs, may not be associated witha significant risk for GO.39
Adding periodontal variables to the logistic modelimproved its accuracy. A great risk for gingival alter-ations was determined by papillary bleeding index,reinforcing the role of inflammation in the patho-genesis of GO. The association between gingival in-flammation and GO was by far the most robust, inaccordance with a previous report.41 The interactionbetween time since transplant and CNI previous usewas maintained within the model with similar coeffi-cients and P values, adding credence to this variablein the prevalence of gingival alterations among SIR-treated subjects. SIR serum level was also retainedin the model as a significant variable. Further studiesare necessary to investigate the role of SIR dosagesand serum concentrations in gingival alterationswithin SIR-based regimens.
CONCLUSIONS
GO was observed in a considerable number of sub-jects under SIR-based immunosuppressive regimens.However, this GO was not clinically significant. In ad-dition, it was strongly associated with papillary bleed-ing index and the interaction between time sincetransplant and previous CNI use. Such findings pointtoward the importance of cooperation between med-ical and dental health care personnel in the mainte-nance of renal transplant recipients under SIR-basedimmunosuppressive regimens. Managing periodontalconditions in post-transplant subjects under immuno-suppressive regimens may improve gingival statusand quality of life.
ACKNOWLEDGMENTS
The authors thank the Transplant Unit of FelicioRocho Hospital and all study participants for their
Gingival Status in Sirolimus Immunosuppressive Regimens Volume 79 • Number 11
2066
time and involvement. This study was supported bygrants from the Coordination of Improvement of UpperLevel Personnel (CAPES), Brasılia, DF, Brazil, and theFoundation for Support of Research in Minas Gerais(FAPEMIG/#13016), Belo Horizonte, MG, Brazil. Theauthors report no conflicts of interest related to thisstudy.
REFERENCES1. Magoha GA, Ngumi ZW. Renal transplantation during
the twentieth century: A review. East Afr Med J 2001;78:317-321.
2. Magee CC, Pascual M. Update in renal transplantation.Arch Intern Med 2004;164:1373-1388.
3. Pascual M, Theruvath T, Kawai T, Tolkoff-Rubin N,Cosimi AB. Strategies to improve long term outcomesafter renal transplantation. N Engl J Med 2002;346:580-590.
4. Rajab A, Pelletier RP, Henry ML, et al. Evolution ofimmunosuppression in kidney transplantation: TheOhio State University experience. Clin Transpl 2005;111-117.
5. Callaghan CJ, Bradley JA. Current status of renaltransplantation. Methods Mol Biol 2006;333:1-28.
6. Dannovitch MD. Immunosuppressant-induced meta-bolic toxicities. Transplant Rev 2000;14:65-81.
7. Miller LW. Cardiovascular toxicities of immunosup-pressive agents. Am J Transplant 2002;2:807-808.
8. Nankivell BJ, Borrows RJ, Fung CL, O’Connell PJ,Allen RD, Chapman JR. The natural history of chronicallograft nephropathy. N Engl J Med 2003;349:2326-2333.
9. Dahm F, Weber M. Kidney transplantation: New devel-opments. Swiss Surg 2003;9:205-212.
10. Flechner SM. Minimizing calcineurin inhibitor drugsin renal transplantation. Transplant Proc 2003;35:118S-121S.
11. Bestard O, Cruzado JM, Grinyo JM. Calcineurin-in-hibitor-sparing immunosuppressive protocols. Trans-plant Proc 2005;37:3729-3732.
12. Barbari AG, Stephan AG, Masri MA. Calcineuriminhibitor-free protocols: Risks and benefits. Saudi JKidney Dis Transpl 2007;18:1-23.
13. Watson CJE. Sirolimus (Rapamycin) in clinical trans-plantation. Transplant Rev 2001;15:165-177.
14. Flechner SM, Goldfarb D, Solez K, et al. Kidneytransplantation with sirolimus and mycophenolatemofetil-based immunosuppression: 5-year results ofa randomized prospective trial compared to calci-neurin inhibitor drugs. Transplantation 2007;83:883-892.
15. Kruger B, Fischereder M, Jauch KW, et al. Five-yearfollow-up after latter conversion from calcineurim in-hibitors to sirolimus in patients with chronic renal allo-graft dysfunction. Transplant Proc 2007;39:518-521.
16. Srinivas TR, Schold JD, Guerra G, Eagan A, Bucci CM,Meier-Kriesche HU. Mycophenolate mofetil/sirolimuscompared to other common immunosuppressive reg-imens in kidney transplantation. Am J Transplant2007;7:586-594.
17. Merkel S, Mogilevskaja N, Mengel M, Haller H,Schwarz A. Side effects of sirolimus. Transplant Proc2006;38:714-715.
18. Webster AC, Lee VW, Chapman JR, Craig JC. Targetof rapamycin inhibitors (sirolimus and everolimus)
for primary immunosuppression of kidney transplantrecipients: A systematic review and meta-analysisof randomized trials. Transplantation 2006;81:1234-1248.
19. van Gelder T. The ups and downs of sirolimus inkidney transplantation, and the importance of report-ing negative findings. Neth J Med 2007;65:3-4.
20. Trackman PC, Kantarci A. Connective tissue metab-olism and gingival overgrowth. Crit Rev Oral Biol Med2004;15:165-175.
21. Kataoka M, Kido J, Shinohara Y, Nagata T. Drug-induced gingival overgrowth – A review. Biol PharmBull 2005;28:1817-1821.
22. Vescovi P, Meleti M, Manfredi M, Merigo E, Pedrazzi G.Cyclosporin-induced gingival overgrowth: A clinical-epidemiological evaluation of 121 Italian renal trans-plant recipients. J Periodontol 2005;76:1259-1264.
23. Costa FO, Ferreira SD, Cota LOM, Costa JE, AguiarMA. Prevalence, severity, and risk variables associatedwith gingival overgrowth in renal transplant subjectstreated under tacrolimus or cyclosporin regimens.J Periodontol 2006;77:969-975.
24. Costa FO, Ferreira SD, Lages EJP, Costa JE, OliveiraAMSD, Cota LOM. Demographic, pharmacologic, andperiodontal variables for gingival overgrowth in sub-jects medicated with cyclosporin in the absence ofcalcium channel blockers. J Periodontol 2007;78:254-261.
25. Afonso M, Bello VO, Shibli JA, Sposto MR. Cyclo-sporin A-induced gingival overgrowth in renal trans-plant patients. J Periodontol 2003;74:51-56.
26. Ellis JS, Seymour RA, Taylor JJ, Thomason JM.Prevalence of gingival overgrowth in transplant pa-tients immunosuppressed with tacrolimus. J ClinPeriodontol 2004;31:126-131.
27. Cezario ES, Cota LO, Ferreira SD, et al. Gingivalovergrowth in renal transplant subjects medicatedwith tacrolimus in the absence of calcium channelblockers. Transplantation 2008;85:232-236.
28. Hernandez G, Arribal L, Frias MC, et al. Conversionfrom cyclosporin A to tacrolimus as a non-surgicalalternative to reduce gingival enlargement: A prelimi-nary case series. J Periodontol 2003;74:1816-1823.
29. James JA, Boomer S, Maxwell AP, et al. Reductionin gingival overgrowth associated with conversionfrom cyclosporin A to tacrolimus. J Clin Periodontol2000;27:144-148.
30. James JA, Jamal S, Hull PA, et al. Tacrolimus is notassociated with gingival overgrowth in renal transplantpatients. J Clin Periodontol 2001;28:848-852.
31. McKaig SJ, Kelly D, Shaw L. Investigation of the effectof FK506 (tacrolimus) and cyclosporin on gingivalovergrowth following paediatric liver transplantation.Int J Paediatr Dent 2002;12:398-403.
32. Silness J, Loe H. Periodontal disease in pregnancy: II.Correlation between oral hygiene and periodontalcondition. Acta Odontol Scand 1964;22:121-135.
33. Saxer UP, Muhlemann HR. Motivation and education(in German). SSO Schweiz Monatsschr Zahnheilkd1975;85:905-919.
34. Thomason JM, Kelly PJ, Seymour RA. The distributionof gingival overgrowth in organ transplant patients.J Clin Periodontol 1996;23:367-371.
35. Thomason JM, Seymour RA, Rice N. The prevalenceand severity of cyclosporin and nifedipine-inducedgingival overgrowth. J Clin Periodontol 1993;20:37-40.
J Periodontol • November 2008 Cota, Oliveira, Costa, Cortelli, Costa
2067
36. Ekberg H, Tedesco-Silva H, Demirbas A, et al.Reduced exposure to calcineurin inhibitors in renaltransplantation. N Engl J Med 2007;357:2562-2575.
37. Saber LT, Ikeda MY, Almeida JM. Posttransplantationconversion to sirolimus-based immunosuppression: Asingle center experience. Transplant Proc 2007;39:3098-3100.
38. Ellis JS, Seymour RA, Robertson P, Butler TJ,Thomason JM. Photographic scoring of gingival over-growth. J Clin Periodontol 2001;28:81-85.
39. Greenberg KV, Armitage GC, Shiboski CH. Gingivalenlargement among renal transplant recipients in theera of new-generation immunosuppressants. J Peri-odontol 2008;79:453-460.
40. Seymour RA, Ellis JS, Thomason JM. Risk factors fordrug-induced gingival overgrowth. J Clin Periodontol2000;27:217-223.
41. Thomason JM, Seymour RA, Ellis JS. Risk factorsfor gingival overgrowth in patients medicated with
cyclosporin in the absence of calcium channelblockers. J Clin Periodontol 2005;32:273-279.
42. James JA, Marley JJ, Jamal S, et al. The calciumchannel blocker used with cyclosporin has an effect ongingival overgrowth. J Clin Periodontol 2000;27:109-115.
43. Ellis JS, Seymour RA, Steele JG, Robertson P, ButlerTJ, Thomason JM. Prevalence of gingival overgrowthinduced by calcium channel blockers: A community-based study. J Periodontol 1999;70:63-67.
Correspondence: Dr. Fernando Oliveira Costa, Depart-ment of Periodontology, Federal University of MinasGerais, Antonio Carlos Ave., 6627 – Pampulha, P.O. Box359, Belo Horizonte 31270-901, MG, Brazil. Fax: 55-31-3282-6787; e-mail: [email protected].
Submitted April 12, 2008; accepted for publication May24, 2008.
Gingival Status in Sirolimus Immunosuppressive Regimens Volume 79 • Number 11
2068