Embed Size (px)
Citation preview

Gingival Disease
Nield-Gehrig CH 10Perry CH 6

Gingival Description

6 Gingival Characteristics
Color Size Position of margin Shape of margins and papillae Texture and consistency Bleeding and/or exudate

Healthy Gingiva
Tissue fits snugly around the tooth Pointed papillae fill embrasure spaces Firm and resilient Little or no gingival crevicular fluid
(GCF)
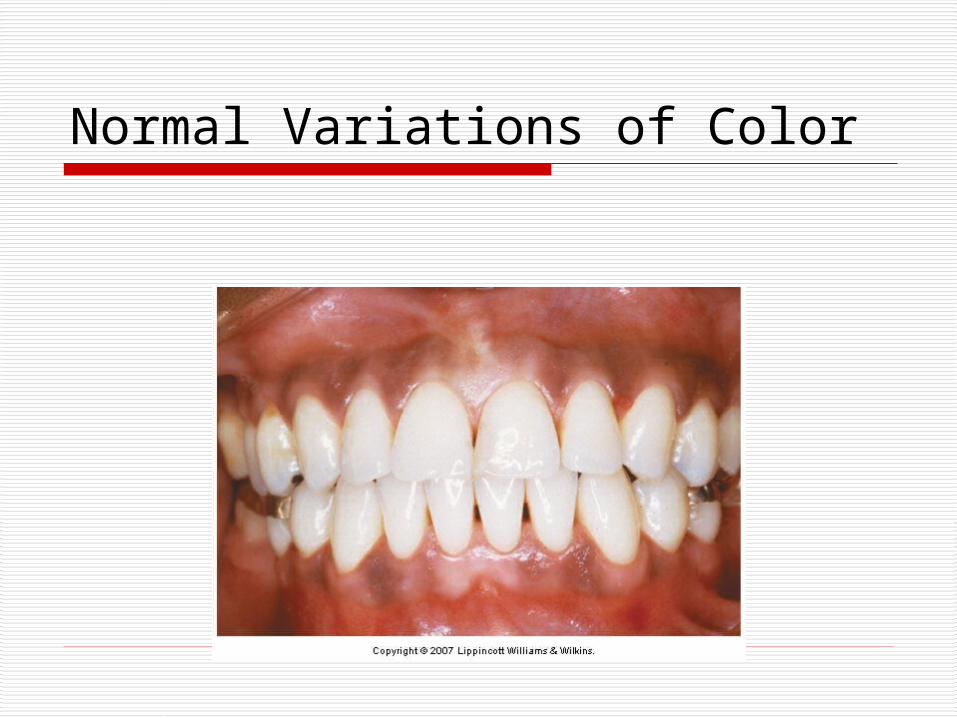
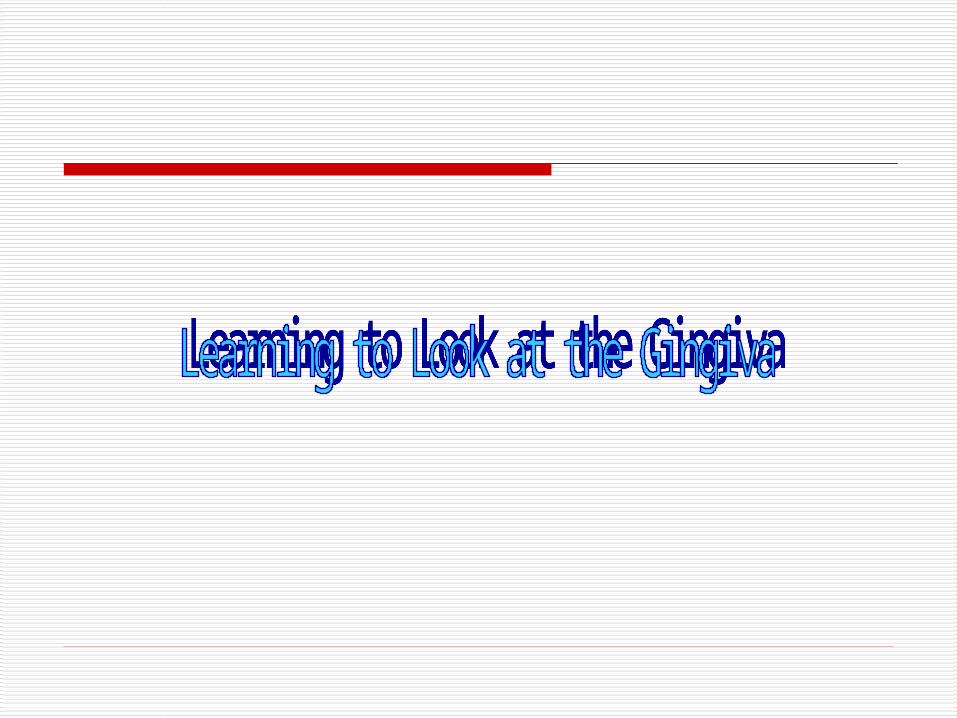
Normal Variations of Color

Gingivitis The mildest and most
common form of periodontal disese
Gingivitis – inflammation of the gingiva causing tissue to become edematous and erythematous…bleeds easily on provocation.

Tissue Color In Gingivitis
Acute inflammation = increased blood flow = RED tissue
Chronic inflammation = bluish-red or purplish – red

Changes in Disease
Gingival Bleeding on Probing The two earliest signs of ginigval
inflammation preceding established gingivitis are: 1. Increased gingival crevicular fluid
production rate GCF = inflammatory exudate Recently – development of tests for the
detection or prediction of periodontal disease using the components, origin, and function of GCF
Drugs in GCF – tetracycline and Metronidazole 2. Bleeding from the gingivl sulcus on
gentle probing

Gingival Bleeding In gingival inflammation, histopathologic alterations
that result in abnormal gingival bleeding include dilation and engorgement of the capillaries and thinning or laceration of the sulcular epithelium.
Because the capillaries are engorged and closer to the surface, and the thinned, degenerated epithelium is less protective, stimuli that are normally innocuous cause rupture of the capillaries and gingival bleeding.
The severity of the bleeding and the ease of its provocation depend on the intensity of the inflammation.
In cases of moderate or advanced periodontitis, the presence of bleeding on probing is considered a sign of active tissue destruction.

Gingival Bleeding Associated with Systemc Changes In some systemic disorders, gingival hemorrhage
occurs spontaneously or after irritation and is excessive and difficult to control. Vascular abnormalities – Vit. C deficiency or
allergy Platelet disorders – thrombocytopenic purpura Hypprothrombinemia – Vit. K deficiency Other coagulation defects – hemophilia,
leukemia, Deficient platlet thromboplastic factor (PF3)
resulting from uremia, multiple myeloma and ostrubella purpura.

Gingival Bleeding Associated with Systemc Changes Hormonal replacement therapy Oral contraceptives Pregnancy Menstral cycle Diabetes Medications:
Anticonvulsants Antihypertensive calcium channel blockers Immunosuppressant drugs aspirin

Change in Sizein disease
Tissue Size in Gingivitis
Increase in tissue fluid causes enlargement of the marginal and interproximal gingival tissues (Edema)
Change can be localized to a few areas or affect the whole mouth (generalized)

Change in Position in Margin

Change in Position of Margin

Change in Shape of Margin

Bulbous Papilla

Cratered Papilla

Missing and Blunted Papilla

Changes in the Consistency In Gingival Disease
Both chronic and acute inflammations produce changes int the normal firm and resilient consistency of the gingiva.
Chronic gingivitis = edematous – (destructive) and fibrotic –
(repairative) changes coexist The consistency of the gingiva is
determined by their relative pedominance.

Spongy Tissue

Surface Texture Changes in Disease
The surface of normal gingiva usually exhibits numerous small depressions and elevations = stippling
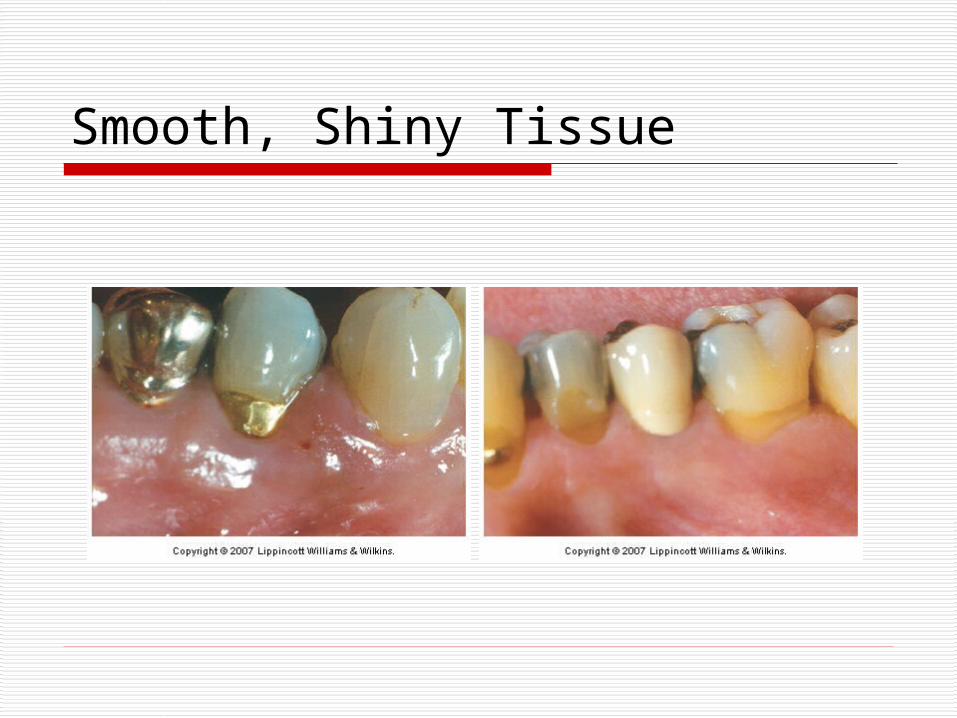
In chronic inflammation the surface is either smooth and shiny or firm and nodular This depends on whether the dominant
changes are exudative or fibrotic

Smooth, Shiny Tissue
Can be: exudative Epithelial atrophy in atrophic gingivitis Chronic desquamative gingivitis can also
have peeling of the surface
Smooth, Shiny Tissue

Changes in surface texture chronic gingivitis
Hyperkeratosis results in a leathery texture (example = chronic gingival disease in a smoker)
Fibrotic = firm nodular Drug induced gingival overgrowth
also produces a nodular surface

Nodular Tissue

Assess the Following
Color Size Position of gingival margin Shape of margins and papillae Use air and probe to determine
texture Consistency Check for bleeding

More on Size Gingival Enlargement or gingival
overgrowth are the current terms used to describe an increase in the size of the gingiva
“hypertrophic gingivitis” or “gingival hyperplasia” may have erroneous pathologic connotations
Gingival enlargement is a purely clinical term

Gingival enlargement can beclassified according to etiologic factors and pathologic changes
I. Inflammatory enlargement A. Chronic B. Acute
II. Drug-induced enlargement III. Enlagements associated with systemic
diseases or conditions IV. Neoplastic enlargement (gingival
tumors) V. False enlargement

Criteria of location Localized: limited to the gingiva adjacent
to a sengle tooth or group of teeth. Generalized: involving the gingiva
throughout the mouth Marginal: confined to the marginal gingiva Papillary: Confined to the interdental
papillae Diffuse: Involving the marginal and
attached gingivae and papillae. Discrete: An isolated sessile or
pedunculated, tumorlike enlargement.





Non-Plaque –Induced Gingival diseases
Bacterial origin – Neisseria gonorrhea – associated lesions Treponema pallidum – associated lesions Streptococcal species – associated
lesions
RARE – Non-plaque is RARE


Non-Plaque-induced gingival diseases of viral origins
RARE – Non-plaque is RARE Acute herpetic gingivostomatitis Recurrent oral herpes Varicella-zoster infections

Primary Herpetic Gingivostomatitis Caused by herpes simplex virus type 1
(HSV-1) Most often occuring in infants and children
under 6 years In most people the primary infection is
asymptomatic As part of the primary infection, the virus
ascends through sensory and autonomic nerves, where it persists as latent HSV in neuronal ganglia that innervate the site
In 1/3 of the world’s population secondary manifestations result from various stimuli


NUG
Punched-out, craterlike depressions at the crest of the interdental papillae
Gray, pseudomembranous slough Linear erythema Spontanious gingival hemorrhage Fetid odor


Gingival Diseases Modified by Malnutrition
Most clinical studies have not shown a relationship between the development of gingival diseases and malnutrition with the possible exception of severe vitamin C deficiency.


Lichen Planus
Inflammatory mucocutaneous disorder that may involve mucosal surfaces and the skin.
Current evidence suggests that lichen planus is an immunologically mediated mucocutaneous disorder in which host T lymphocytes play a central role.