Embed Size (px)
Citation preview

Heart, Lung and Circulation (2014) 23, e136–e138
1443-9506/04/$36.00
http://dx.doi.org/10.1016/j.hlc.2013.11.016
IMAGE
Giant Superior Vena-ca
va Aneurysm after Glenn Surgery: A New Complication ofthe Glenn ProcedureAashrayata Aryal Pandit, MDa, Jorge R. Alegria, MDa, Anil Pandit, MDa,Martina Mookadam, MDb, Farouk Mookadam, MDa*
aDivision of Cardiovascular Diseases, Mayo Clinic, ArizonabDepartment of Family Practice, Mayo Clinic, Arizona
Received 31 August 2013; received in revised form 11 November 2013; accepted 17 November 2013; online published-ahead-of-print 24 January 2014
Keywords Superior vena cava dilatation � Glenn surgery � Congenital heart disease � Shortness of breath � Right
sided aortic arch
IntroductionAneurysm of systemic veins is uncommon with only 30 cases
reported in literature [1]. Aneurysms of the inferior vena cava
have also been rarely reported [2]. The most common cause
of SVC aneurysm is congenital or surgical weakness in the
longitudinal muscles of SVC wall [3]. We present a case of a
27 year-old patient presenting with SVC aneurysm 13 years
after a Glenn surgical procedure.
Case ReportA 27 year-old male presented with chest tightness, shortness
of breath on exertion, and palpitations. He had a history of
double outlet right ventricle with transposition of the great
vessels, sub pulmonic ventricular septal defect, membranous
septal defect, superior vena cava to right pulmonic artery
anastomosis (Bidirectional Glenn), atrial septostomy, right
pulmonary arterioplasty 13 years earlier (Fig. 1). A
pacemaker was placed for high-grade AV block. He had
New York Heart Association (NYHA) class III heart failure
and was on ACE-inhibitors and beta-blockers. Chest X ray
showed an abnormal cardiac silhouette that was initially
assumed to be right-sided aortic arch (Fig. 2, Arrow,
© 2014 Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS) a
Inc. All rights reserved.
* Corresponding author. Mayo Clinic Arizona, 13400 E Shea Blvd, Scottsdale, AZ 85
Email: [email protected]
Panel A). A transthoracic echocardiography showed a left
ventricular ejection fraction of 26%, mild left ventricular
enlargement, severe decrease in right ventricular function,
multiple ventricular septal defects, left to right shunt at atrial
level, severe pulmonary valve stenosis with maximal instan-
taneous Doppler gradient of 71 mm Hg. The superior vena
cava (SVC) was dilated measuring 6 cm. Computed tomo-
graphic (CT) angiogram confirmed the findings of the TTE
demonstrating a severely dilated SVC at the site of the Glenn
anastomosis (Fig. 2 Arrows, Panel B and C). Further, Fig. 3A
demonstrates connection of superior vena cava (SVC) with
right pulmonary artery (RPA) and Fig. 3B shows aorta (Ao)
arising from single ventricle (V). The patient underwent both
right and left heart catheterisation and findings are tabulated
in Fig. 1. The patient is currently undergoing a cardiac trans-
plant evaluation.
DiscussionThe Glenn procedure involves connection of superior vena
cava to the pulmonary artery as a palliative procedure in
many congenital heart diseases, including patients with a
single ventricle as presented. The classical Glenn surgery
involves a unidirectional connection of the right pulmonary
nd the Cardiac Society of Australia and New Zealand (CSANZ). Published by Elsevier
259. Tel.: +480 301 8000; fax: +480 301 8018,

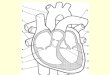
Figure 1 The diagram showing SVC aneurysm measur-ing about 6 cm with double out-let right ventricle, ven-tricular septal defect. The number represents pressurerecordings during right and left heart catheterisation.The arrows indicate course of catheters.
Figure 2 A, chest X ray showing abnormal cardiac silhouette
Computed tomographic (CT) angiogram demonstrating severely
Giant Superior Vena-cava Aneurysm e137
artery to the superior vena cava and the blood from the SVC
will flow only to right lung, because the connection of right
pulmonary artery to the main pulmonary artery is severed
and sewn. More commonly a bidirectional Glenn procedure
is performed, also known as modified Glenn procedure as
described in our case. The modified Glenn procedure
involves connecting the SVC with right pulmonary artery
and the venous blood freely flows through right and left
pulmonary artery. The usual potential complications after
this surgery are many and involve arrhythmias, protein
losing enteropathy, cyanosis, pulmonary arteriovenous mal-
formations, and hepatic dysfunction with hepatocellular car-
cinoma [4]. Moreover, aneurysm of SVC after bidirectional
Glenn is extremely rare with only one case reported in the
literature [5].
The natural history of superior vena cava aneurysms is
unknown. Review of the literature suggests that SVC aneur-
ysms can cause pulmonary embolism and thrombosis [6].
The exact pathogenesis of SVC aneurysm is not known and
possibility of deficiency of longitudinal fibers has been
reported [7]. The management of SVC aneurysms is not
clearly defined in literature particularly in patients after a
Glenn shunt.
that was initially assumed to be right-sided aortic arch. dilated SVC on Glenn connection (Arrows, Panel B and C).

Figure 3 A, computed tomographic (CT) angiogram demonstrating clear connection of superior venacava (SVC) with rightpulmonary artery (RPA). B, saggital section of CT angiogram showing origin of aorta (Ao) from the single ventricle.
e138 A.A. Pandit et al.
Conflict of InterestAuthors declare that they have no conflict of interests.
References[1] Enright TR, Kanne JP. Saccular superior vena cava aneurysm - incidental
diagnosis by MDCT. Clin Radiol 2010;65(5 May):421–2.
[2] Mookadam F, Rowley VB, Emani UR, Al-Harthi MS, Baxter CM,
Wilansky S, et al. Aneurysmal dilatation of the inferior vena cava.
Echocardiography 2011;28(8 Sep):833–42.
[3] Ream CR, Giardina A. Congenital superior vena cava aneurysm with
complications caused by infectious mononucleosis. Chest 1972;62(6 Dec):
755–7.
[4] Asrani SK, Warnes CA, Kamath PS. Hepatocellular carcinoma after the
Fontan procedure. N Engl J Med [Case Reports Letter] 2013;368(18 May 2):
1756–7.
[5] Panduranga P, Thomas E, Al-Maskari S, Al-Farqani A. Giant superior
vena caval aneurysm in a post-Glenn patient. Interact Cardiovasc Thorac
Surg 2012;14(6 Jun):878–9.
[6] Oh SG, Kim KH, Seon HJ, Yoon HJ, Ahn Y, Jeong MH, et al. Unusual
cause of acute right ventricular dysfunction: rapid progression of superior
vena cava aneurysm complicated by thrombosis and pulmonary throm-
boembolism. J Korean Med Sci 2011;26(5 May):690–3.
[7] Varma PK, Dharan BS, Ramachandran P, Neelakandhan KS. Superior
vena caval aneurysm. Interact Cardiovasc Thorac Surg 2003;2(3 Sep):
331–3.