Embed Size (px)
Citation preview

ARCH SOC ESP OFTALMOL 2007; 82: 563-566
GIANT NODULAR POSTERIOR SCLERITIS COMPATIBLEWITH OCULAR SARCOIDOSIS SIMULATING CHOROIDAL
MELANOMA
ESCLERITIS NODULAR POSTERIOR GIGANTE COMPATIBLECON SARCOIDOSIS OCULAR SIMULANDO UN MELANOMA DE
LA COROIDES
PÉREZ-CAMPAGNE E1, GUEX-CROSIER Y2, SCHALENBOURG A2, UFFER S2, ZOGRAFOS L2
Received: 31/5/06. Accepted: 25/7/07.Hôpital Ophtalmique Jules Gonin. Université de Lausanne. Lausanne (Switzerland).1 Graduate in Medicine.2 Ph.D. in Medicine. Communication presented at the LXXXII Congress of S.E.O. (La Coruña 2006).
Correspondence:Eric Pérez-CampagneHôpital Ophtalmique Jules GoninAvenue de France, 15CH-1004 LausanneSwitzerlandE-mail: [email protected]
ABSTRACT
Case report: A 30-year-old man was referred toour ocular oncology service with a diagnosis ofamelanotic choroidal melanoma of the left eye. Thefollowing tests were performed: ophthalmoscopy,fluorescein angiography, indocyanine green angio-graphy, ultrasonography, magnetic resonance ima-ging and biopsy.Discussion: The diagnosis of giant nodular poste-rior scleritis, as suggested by ultrasonography, wasconfirmed by biopsy. A comprehensive medicalevaluation was performed, but no etiology wasfound. The histology revealed a granuloma compa-tible with ocular sarcoidosis. A rapid response wasobtained by systemic steroid administration(1 mg/kg). Sarcoidosis continues to be a challengein diagnosis. It is important to distinguish nodularposterior scleritis from choroidal melanoma (ArchSoc Esp Oftalmol 2007; 82: 563-566).
Key words: Scleritis, eye neoplasms, uveal neo-plasms, choroid neoplasms, sarcoidosis, choroidalmelanoma.
SHORT COMMUNICATION
RESUMEN
Caso clínico: Un paciente de 30 años fue enviado anuestro servicio oncológico de referencia con eldiagnóstico de melanoma amelanótico de la coroi-des del ojo izquierdo. Se hicieron los siguientesexámenes: oftalmoscopía, angiografía fluoresceíni-ca, angiografía con verde de indocianina, ecografía,resonancia magnética y biopsia.Discusión: El diagnóstico de escleritis nodular pos-terior gigante basado en la ecografía se confirmómediante una biopsia. Se realizó un examen médi-co completo buscándose el posible agente causal;no se encontró la etiología. La histología reveló ungranuloma que era compatible con una sarcoidosisocular. Mediante la administración de esteroidespor vía oral (1 mg/kg), se obtuvo una evoluciónrápidamente favorable del cuadro. El diagnóstico deesta afección sigue siendo un desafío. Es importan-te diferenciar una escleritis posterior nodular de unmelanoma de la coroides.
Palabras clave: Escleritis, tumores del ojo, tumo-res de la úvea, tumores de la coroides, sarcoidosis,melanoma de la coroides.
INTRODUCTION
Giant nodular posterior scleritis is a severeinflammatory pathology involving the posteriorsclera and may cause a choroidal detachment up tothe ora serrata. This is the case in 2 to 12 percent ofscleritis cases. It affects mainly females (66-83 per-cent). It may appear as a granulomatous disease, butin most cases it is idiopathic and unilateral (1). Dueto its shape and volume, it may be mistaken for auveal tumor (2,3). The case described herein wasreferred to the ophthalmology department as a cho-roidal melanoma.
CASE REPORT
In November 2005, a 30-year-old Caucasianmale, without relevant medical history, was referredto the ophthalmology unit reporting a choroidalmelanoma in his left eye (LE).
Since August 2005, the patient had noticed in hisRE a unilateral reduction in visual acuity (VA). Hehad been complaining for a month of ocular pain inthe said eye.
The right eye’s (RE) VA was 10/10 with –0.5 Dspherical correction, while the LE was <1/10 wit-hout correction and 8/10 with an added –5.00 Dspherical correction.
The RE ophthalmologic examination showed norelevant signs.
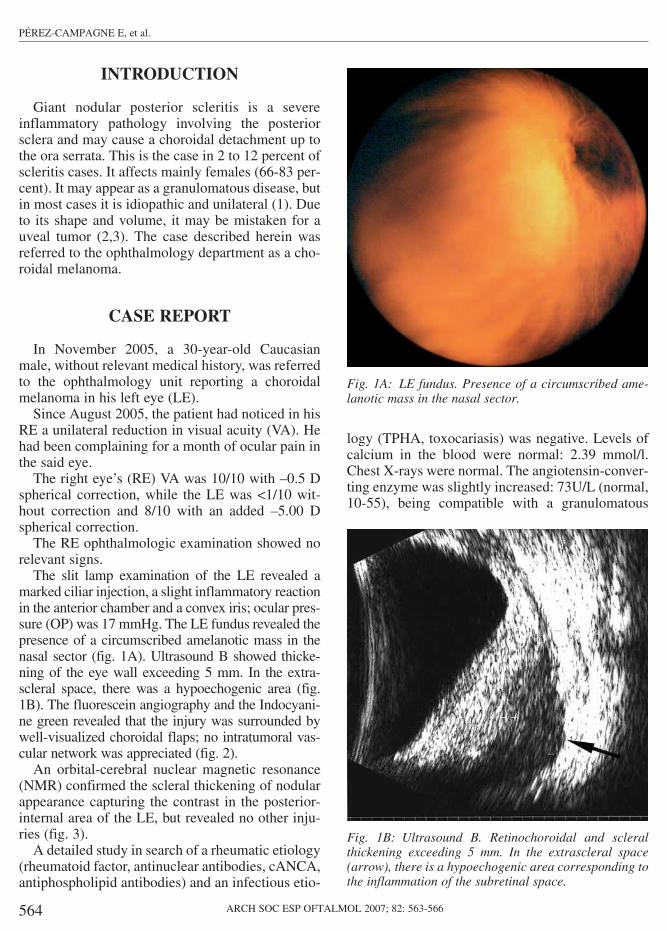
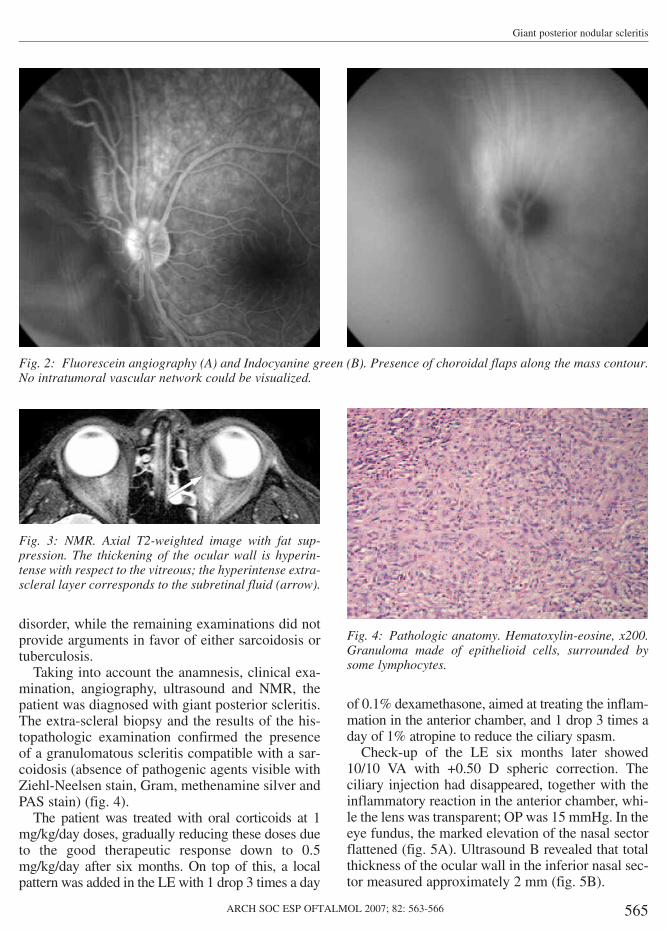
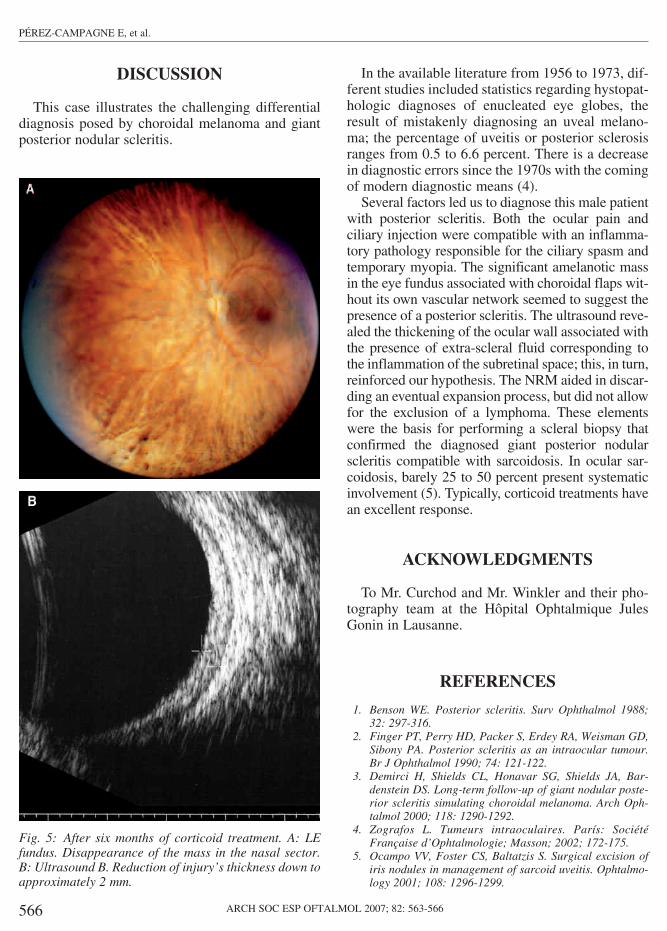
The slit lamp examination of the LE revealed amarked ciliar injection, a slight inflammatory reactionin the anterior chamber and a convex iris; ocular pres-sure (OP) was 17 mmHg. The LE fundus revealed thepresence of a circumscribed amelanotic mass in thenasal sector (fig. 1A). Ultrasound B showed thicke-ning of the eye wall exceeding 5 mm. In the extra-scleral space, there was a hypoechogenic area (fig.1B). The fluorescein angiography and the Indocyani-ne green revealed that the injury was surrounded bywell-visualized choroidal flaps; no intratumoral vas-cular network was appreciated (fig. 2).
An orbital-cerebral nuclear magnetic resonance(NMR) confirmed the scleral thickening of nodularappearance capturing the contrast in the posterior-internal area of the LE, but revealed no other inju-ries (fig. 3).
A detailed study in search of a rheumatic etiology(rheumatoid factor, antinuclear antibodies, cANCA,antiphospholipid antibodies) and an infectious etio-
logy (TPHA, toxocariasis) was negative. Levels ofcalcium in the blood were normal: 2.39 mmol/l.Chest X-rays were normal. The angiotensin-conver-ting enzyme was slightly increased: 73U/L (normal,10-55), being compatible with a granulomatous
564 ARCH SOC ESP OFTALMOL 2007; 82: 563-566
PÉREZ-CAMPAGNE E, et al.
Fig. 1A: LE fundus. Presence of a circumscribed ame-lanotic mass in the nasal sector.
Fig. 1B: Ultrasound B. Retinochoroidal and scleralthickening exceeding 5 mm. In the extrascleral space(arrow), there is a hypoechogenic area corresponding tothe inflammation of the subretinal space.
disorder, while the remaining examinations did notprovide arguments in favor of either sarcoidosis ortuberculosis.
Taking into account the anamnesis, clinical exa-mination, angiography, ultrasound and NMR, thepatient was diagnosed with giant posterior scleritis.The extra-scleral biopsy and the results of the his-topathologic examination confirmed the presenceof a granulomatous scleritis compatible with a sar-coidosis (absence of pathogenic agents visible withZiehl-Neelsen stain, Gram, methenamine silver andPAS stain) (fig. 4).
The patient was treated with oral corticoids at 1mg/kg/day doses, gradually reducing these doses dueto the good therapeutic response down to 0.5mg/kg/day after six months. On top of this, a localpattern was added in the LE with 1 drop 3 times a day
of 0.1% dexamethasone, aimed at treating the inflam-mation in the anterior chamber, and 1 drop 3 times aday of 1% atropine to reduce the ciliary spasm.
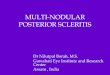
Check-up of the LE six months later showed10/10 VA with +0.50 D spheric correction. Theciliary injection had disappeared, together with theinflammatory reaction in the anterior chamber, whi-le the lens was transparent; OP was 15 mmHg. In theeye fundus, the marked elevation of the nasal sectorflattened (fig. 5A). Ultrasound B revealed that totalthickness of the ocular wall in the inferior nasal sec-tor measured approximately 2 mm (fig. 5B).
565ARCH SOC ESP OFTALMOL 2007; 82: 563-566
Giant posterior nodular scleritis
Fig. 2: Fluorescein angiography (A) and Indocyanine green (B). Presence of choroidal flaps along the mass contour.No intratumoral vascular network could be visualized.
Fig. 3: NMR. Axial T2-weighted image with fat sup-pression. The thickening of the ocular wall is hyperin-tense with respect to the vitreous; the hyperintense extra-scleral layer corresponds to the subretinal fluid (arrow).
Fig. 4: Pathologic anatomy. Hematoxylin-eosine, x200.Granuloma made of epithelioid cells, surrounded bysome lymphocytes.
DISCUSSION
This case illustrates the challenging differentialdiagnosis posed by choroidal melanoma and giantposterior nodular scleritis.
In the available literature from 1956 to 1973, dif-ferent studies included statistics regarding hystopat-hologic diagnoses of enucleated eye globes, theresult of mistakenly diagnosing an uveal melano-ma; the percentage of uveitis or posterior sclerosisranges from 0.5 to 6.6 percent. There is a decreasein diagnostic errors since the 1970s with the comingof modern diagnostic means (4).
Several factors led us to diagnose this male patientwith posterior scleritis. Both the ocular pain andciliary injection were compatible with an inflamma-tory pathology responsible for the ciliary spasm andtemporary myopia. The significant amelanotic massin the eye fundus associated with choroidal flaps wit-hout its own vascular network seemed to suggest thepresence of a posterior scleritis. The ultrasound reve-aled the thickening of the ocular wall associated withthe presence of extra-scleral fluid corresponding tothe inflammation of the subretinal space; this, in turn,reinforced our hypothesis. The NRM aided in discar-ding an eventual expansion process, but did not allowfor the exclusion of a lymphoma. These elementswere the basis for performing a scleral biopsy thatconfirmed the diagnosed giant posterior nodularscleritis compatible with sarcoidosis. In ocular sar-coidosis, barely 25 to 50 percent present systematicinvolvement (5). Typically, corticoid treatments havean excellent response.
ACKNOWLEDGMENTS
To Mr. Curchod and Mr. Winkler and their pho-tography team at the Hôpital Ophtalmique JulesGonin in Lausanne.
REFERENCES
1. Benson WE. Posterior scleritis. Surv Ophthalmol 1988;32: 297-316.
2. Finger PT, Perry HD, Packer S, Erdey RA, Weisman GD,Sibony PA. Posterior scleritis as an intraocular tumour.Br J Ophthalmol 1990; 74: 121-122.
3. Demirci H, Shields CL, Honavar SG, Shields JA, Bar-denstein DS. Long-term follow-up of giant nodular poste-rior scleritis simulating choroidal melanoma. Arch Oph-talmol 2000; 118: 1290-1292.
4. Zografos L. Tumeurs intraoculaires. París: SociétéFrançaise d’Ophtalmologie; Masson; 2002; 172-175.
5. Ocampo VV, Foster CS, Baltatzis S. Surgical excision ofiris nodules in management of sarcoid uveitis. Ophtalmo-logy 2001; 108: 1296-1299.
566 ARCH SOC ESP OFTALMOL 2007; 82: 563-566
PÉREZ-CAMPAGNE E, et al.
Fig. 5: After six months of corticoid treatment. A: LEfundus. Disappearance of the mass in the nasal sector.B: Ultrasound B. Reduction of injury’s thickness down toapproximately 2 mm.




![A case of scleritis associated rheumatoid arthritis ...syphilis, caused by nodular infectious uveitis [9, 10]. Biswas et al. reported a case of tuberculous uveitis associated with](https://img.pdfslide.us/doc/110x75/60997293e4fd5e2ef7072fd8/a-case-of-scleritis-associated-rheumatoid-arthritis-syphilis-caused-by-nodular.jpg)























