Embed Size (px)
Citation preview

2. Discussion
The CSF abnormalities of neurosyphilis develop in 10–20% of patients with untreated primary and 30–70% of pa-tients with untreated secondary syphilis. In the majority ofpatients the infection remains asymptomatic and the diag-nosis is made on the basis of positive serum serology, CSFpleocytosis, and a positive CSF-Venereal Disease ResearchLaboratory (VDRL) test. The CSF changes are clear in70% of patients at the end of the secondary stage. Individ-uals who do not clear CSF are probably at increased risk ofsymptomatic neurosyphilis. Symptomatic neurosyphilishas many forms, including aseptic meningitis, cranial nerveneuropathy, stroke secondary to vasculitis, tabes dorsalisdementia and gumma.1,2
Cerebral syphilitic gumma is a rare complication of tertiarysyphilis in immunocompetent as well as immunocompro-mised hosts,3 with only a few reported cases in the litera-ture.3–12 The majority of reported cases were in thecerebrum, with some cases in other locations, including thespinal cord,6 pituitary gland,8 brain stem10 and cerebellopon-tine angle.12 Most reported cases were either multiple4 orshowed ring enhancement suggestive of an infectious process.
In our patient the clinical presentations with increasedintracranial pressure and the radiological appearance of asingle irregularly enhancing lesion with an area of centralhypodensity and extensive surrounding oedema was highlysuggestive of a malignant brain tumour. Surgery couldhave been avoided if the diagnosis had been madepreoperatively.
Treatment of neurosyphilis including syphilitic gumma ismedical, with high-dose penicillin (18–24 · 106 units intra-venously per day, given as 3–4 · 106 units intravenouslyevery 4 hours) for 10–14 days and close radiological andserological follow up.1,4 CSF white blood cell (WBC) countshould decline at 3 months and all CSF abnormalitiesshould resolve at 2 years. If the CSF WBC count is normaland CSF-VDRL reactivity is not reactive at 3 months, nofurther testing is required. For those with persistent CSFabnormalities at 3 months after therapy (excluding elevated
protein concentration), CSF should be re-examined at 6months after therapy and every 6 months thereafter untilthe CSF WBC count and VDRL reactivity normalise. Fail-ure of the CSF WBC count to decrease at 6 months and fail-ure of CSF-VDRL reactivity to decline fourfold at 1 year isan indication for retreatment.1 Because of the rarity of thecondition, the significance of persistent abnormalities onneuroimaging is not known.
Our patient was unique because of the extensive sur-rounding oedema and the solitary nature of the lesion.
References
1. Marra CM. Neurosyphilis. In: Scheld WM, Whitely RJ, Marra CM,editors. Infections of the Central Nervous System. Philadelphia: Lip-pincott Williams and Wilkins; 2004. p. 649–57.
2. Timmermans M, Carr J. Neurosyphilis in the modern era. J Neurol
Neurosurg Psychiatry 2004;75:1727–30.3. Horowitz HW, Valsamis MP, Wicher V, et al. Brief report: cerebral
syphilitic gumma confirmed by the polymerase chain reaction in aman with human immunodeficiency virus infection. N Engl J Med
1994;33:1488–91.4. Roeske LC, Kennedy PR. Syphilitic gummas in a patient with human
immunodeficiency virus infection. N Engl J Med 1996;335:1123.5. Kaplan JG, Sterman AB, Horoupian D, et al. Luetic meningitis with
gumma: clinical, radiologic and neuropathologic features. Neurology
1981;31:464–7.6. El Quessar A, El Hassani R, Chakir N, et al. Syphilitic spinal cord
gumma. J Neuroradiol 2000;27:207–10.7. Lana-Peixoto MA, Teixeira Jr AL, Tzelikis PF, et al. Asymptomatic
intracranial gumma in a patient with syphilitic uveitis and humanimmunodeficiency virus infection. Scand J Infect Dis 2003;35:343–5.
8. Benzick AE, Withwein DP, Weinberg A, et al. Pituitary gland gummain congenital syphilis after failed maternal treatment: a case report.Pediatrics 1999;104:e4.
9. Uemura K, Yamada T, Tsukada A, et al. Cerebral gumma mimickingglioblastoma on magnetic resonance images: case report. Neurol Med
Chir (Tokyo) 1995;35:462–6.10. Herrold JM. A syphilitic cerebral gumma manifesting as brain-stem
mass that responded to corticosteroid monotherapy. Mayo Clin Proc
1994;69:960–1.11. Berger JR, Waskin H, Pall L, et al. Syphilitic cerebral gumma with
HIV infection. Neurology 1992;42:1282–7.12. Eltomey AA, Olin MS, Roberts MP. Cerebellopontine angle gumma.
Neurosurg 1984;15:252–3.
doi:10.1016/j.jocn.2006.07.023
2
310 Case Reports / Journal of Clinical Neuroscience 15 (2008) 310–313
Giant cervical pseudomeningocoele following brachial plexus trauma
Manmohan Singh *, Manish Kumar Kasliwal, Ashok Kumar Mahapatra
Department of Neurosurgery, CN Centre, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029, India
Received 15 April 2006; accepted 7 June 2006
* Corresponding author. Tel.: +91 11 26588700x4914; fax: +91 116588207.
E-mail address: [email protected] (M. Singh).

Abstract
We report an unusual case of a young man with a traumatic brachial plexus injury who presented with a large right-sided neck swell-ing 1 month after trauma. Clinical and diagnostic evaluations revealed a giant cervical pseudomeningocoele with meningitis and hydro-cephalus. Following treatment for meningitis, the patient underwent ventriculoperitoneal shunt, which produced total resolution of thepseudomeningocoele. The management is discussed.� 2007 Published by Elsevier Ltd.
Keywords: Pseudomeningocoele; Brachial plexus injury; Hydrocephalus; Meningitis; Neck swelling
Fig. 1. Large right cervical and supraclavicular tense swelling.
Case Reports / Journal of Clinical Neuroscience 15 (2008) 310–313 311
1. Introduction
Traumatic pseudomeningocoele formation followingbrachial plexus injury is common. MRI scans of the cervi-cal spine can easily detect this abnormality. However, onclinical examination, the pseudomeningocoele is never vis-ible or palpable. There is a paucity of published informa-tion on large pseudomeningocoeles that form followingbrachial plexus injury and that are evident on clinicalexamination, as described by Jakobsen et al.1 Here we de-scribe a rare patient and review the literature on thissubject.
2. Case report
A 23-year-old male with no significant medical historywas referred to our institute with a right brachial plexusinjury 7 days after a road traffic accident. The patientdid not suffer any long bone fractures or a head injury fol-lowing the accident. On examination, a deep wound wasfound on the right side of the patient’s neck, with evidenceof infection. There was right-sided complete brachialplexus injury, and the patient had no power or sensationin his right upper limb. The patient was advised to dressthe wound daily, prescribed antibiotics, and asked to un-dergo regular follow up in the outpatient department.However, the patient returned to outpatient departmentafter only 1 month, presenting with a large right cervicaland supraclavicular swelling (Fig. 1), which was very tenseon palpation. The patient complained of clear watery dis-charge from the swelling at one point, which was sugges-tive of a cerebrospinal fluid (CSF) leak. He was alsosuffering from severe headache and vomiting over the pre-vious few days. Clinical examination revealed neck stiff-ness and positive Kernig’s sign. The patient underwentan MRI of the cervical spine (Fig. 2a, b), which revealeda large right-sided pseudomeningocoele exiting from theC6 nerve root foramen and communicating with the spinalsubarachnoid space. The patient also underwent non-con-trast CT (Fig. 3) of head, which showed communicatinghydrocephalus. A lumbar CSF examination revealed 40polymorphs/mL, 24 mg/dL glucose and 80 mg/dL protein,which was suggestive of meningitis; however, a CSF cul-ture was negative. The patient was admitted to hospitaland treated with intravenous cefoperazone/sulbactam
and netilmicin in antimeningitic doses. Lumbar CSFdrainage was also carried out daily. Every time lumbarCSF drainage was carried out, the pseudomeningocoelebecame lax. The patient was kept on intravenous antibiot-ics for the next 10 days. When the CSF examination re-vealed no evidence of meningitis, the patient underwenta left ventriculoperitoneal shunt, after which the pseud-omeningocoele completely subsided (Fig. 4). The patientwas kept on intravenous antibiotics for the next 2 weeks.Two months following the ventriculoperitoneal shunt,the patient underwent brachial plexus exploration, becausethere was no evidence of improvement in his right upperlimb power. Exploration revealed dense scarring of thesupraclavicular brachial plexus at the root and trunk level.Between the scarred roots, the collapsed pseud-omeningocoele sac was found (Fig. 5), which did not poseany problems during surgical exploration. Complete exter-nal and internal neurolysis of the roots and trunks wascarried out. Neurotisation of the supraspinatus nerveand musculocutaneous nerve was carried out with theaccessory and intercostal nerves, respectively. At the time

of writing, 2 months after the neurotisation, the patient isundergoing physiotherapy.
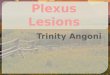
Fig. 2. T2-weighted coronal (a) and axial (b) MRI of the cervical spine showing a giant right-sided pseudomeningocele exiting from the C5-6 neuralforamen.
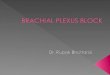
Fig. 3. Non-contrast CT scan of the head revealed hydrocephalus.
Fig. 4. The right cervical and supra-clavicular swelling completelyresolved following insertion of a ventriculoperitoneal shunt.
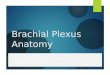
Fig. 5. Intraoperative photograph showing the pseudomeningocoele sacbetween the roots of the brachial plexus. The arrow indicates the bulgingarachnoid.
312 Case Reports / Journal of Clinical Neuroscience 15 (2008) 310–313
3. Discussion
A pseudomeningocoele is an extravasated collection ofCSF outside the dura that results from a dural tear. Itcan be congenital, iatrogenic or traumatic.2 Traumaticpseudomeningocoele in the cervical region has been de-scribed mostly in association with severe brachial plexusinjury or vertebral dislocation,3 and is generally difficultto diagnose clinically. Diagnosis often requires myelogra-phy, CT myelography or MRI to detect evidence of

a giant pseudomeningocoele after brachial plexus injuryis rare. Coexisting hydrocephalus should be ruled outin such a situation. A simple ventriculoperitoneal or lum-bar peritoneal shunt can be used to effectively managethe condition.
References
1. Jakobsen H, Roder OC, Bojsen-Moller J. Large paracervical menin-gocele due to lesion of cervical spinal nerve roots. Acta Chir Scand
1983;149:537–9.2. Couture D, Branch Jr CL. Spinal pseudomeningoceles and cerebro-
spinal fluid fistulas. Neurosurg Focus 2003;15:E6.3. Natale M, Bocchetti A, Scuotto A, et al. Post traumatic
retropharyngeal pseudomeningocele. Acta Neurochir (Wein)
2004;146:735–9.4. Walker TA, Chaloupka JC, De Lotbiniere ACI, et al. Detection
of nerve rootlet avulsion on CT myelography in patients withbirth palsy and brachial plexus injury after trauma. AJR
1996;167:1283–7.5. Samardzic M, Grujieic D, Antunovic V. Nerve transfer in brachial
plexus traction injuries. J Neurosurg 1992;76:191–7.
Case Reports / Journal of Clinical Neuroscience 15 (2008) 313–316 313
preganglionic nerve injury.3–5 A large cervical post-trau-matic pseudomeningocoele of a similar size followingbrachial plexus injury has been reported by Jakobsenet al.1 Pseudomeningocoele associated with a closed bra-chial plexus injury does not generally require treatment.However, a giant pseudomeningocoele as in the presentcase is very unusual, and can pose a difficult therapeuticchallenge. Factors predisposing a patient to developmentof such a large pseudomeningocoele should be lookedfor, such as hydrocephalus, which was present in ourcase. In this particular case, there was an infected lacer-ated wound in the neck, along with avulsed brachialplexus roots and CSF leakage, which caused CSF infec-tion and meningitis and subsequently hydrocephalus.The persistence of hydrocephalus caused the pseud-omeningocoele in the neck to increase in size. In this pa-tient a ventriculoperitoneal shunt effectively treated thecondition. Similarly, a patient with traumatic retropha-ryngeal pseudomeningocoele described by Natale et al.3
was treated with a lumbar peritoneal shunt. To conclude,
doi:10.1016/j.jocn.2006.06.025
Terson’s syndrome in spontaneous spinal subarachnoid haemorrhage
Michelle L. Baker *, Peter J. Hand, Damien Tange
Melbourne Neuroscience Centre, The Royal Melbourne Hospital, Grattan Street, Parkville, 3050, Victoria, Australia
Received 21 June 2006; accepted 1 September 2006
Abstract
This paper is a case report of Terson’s Syndrome (TS) in spontaneous spinal subarachnoid haemorrhage (SAH). A 66-year-oldwoman with acute onset of severe back pain was transferred to our institution for management of her sciatica. The presence of an intra-retinal haemorrhage alerted us to consider intracranial SAH, but investigations showed no intracranial source. Eventually, the patientwas diagnosed with a thoracic spinal SAH. The patient’s symptoms gradually improved with conservative management but within 1month she had a recurrence. A spinal and CT angiogram did not elicit the aetiology. The diagnosis of spontaneous spinal SAH canbe difficult. The recognition of TS has important prognostic implications, often heralding subarachnoid rebleeding. Fundoscopic exam-ination appears mandatory as a tool for diagnosis and regular non-invasive monitoring of patients with SAH.� 2007 Elsevier Ltd. All rights reserved.
Keywords: Terson’s syndrome; Spinal subarachnoid haemorrhage
1. Introduction
Terson’s syndrome (TS) is any type of intraocular haem-orrhage occurring as a direct consequence of intracranialor intraspinal haemorrhage (usually subarachnoid haemor-
rhage (SAH)).1 Spinal SAH is a rare entity and accountsfor less than 1% of all patients with SAH.2 We describe apatient who presented with back and neck pain, drowsinessand fever. Initially, multiple diagnoses were consideredincluding meningitis. The presence of an intraretinal haem-orrhage alerted us to consider intracranial SAH but inves-tigations showed no intracranial source. Eventually, thepatient was diagnosed with a thoracic spinal SAH. To
* Corresponding author. Tel.: +61 411 969 787.E-mail address: [email protected] (M.L. Baker).