Embed Size (px)
Citation preview

Giant Cell Tumours of Bone
Is it benign or malignant
Henry Soeharno
Singapore General Hospital
Dept of Orthopaedic Surgery

Giant Cell Tumour of bone
First described by Cooper and Travers in 1818
5% of all primary bone tumours
20% of all benign bone tumours
Peak incidence: 3rd – 4th decade
Benign, expansile, locally aggressive, osteolytic tumour
Characterised by presence of numerous giant cells that exhibit the phenotypic features of mature osteoclasts.

Giant Cell Tumour of bone
Occasionally undergo malignant transformation
and metastasis (usually to lungs) occurs in
around 2%
PRIMARY VS SECONDARY
Primary malignant GCT – less that 1%
Secondary malignant GCT – post irradiation or
recurrence (poor prognosis)

Classification
ENNEKING
Stage % Description
I (latent) 15% •Confined totally to bone
•Asymptomatic
•Inactive on bone scan
II (active) 70% •Expanded cortex with no breakthrough
•Symptomatic if pathological fracture
•Active on bone scan
III
(aggressive)
15% •Rapidly growing mass
•Symptomatic
•Extensive activity on bone scan
Malignant rare Sarcomatous lesion contiguous with benign GCT

Classification
Grade Description
1 Intramedullary lesion confined to bone
2 Thinned, expanded cortex
3 Cortical breakout
Campanacci

Management options
SURGERY
Molecular Therapy
Embolisation
Radiation

Surgery
Intralesional ‘extended’ curettage (with or without
adjuncts such as phenol and liquid nitrogen)
Recurrence rates
Curettage alone : 50-60%
Curettage + adjuncts : 10-20%
AIM of surgery : balance between reducing incidence
of local recurrence while preserving local functional
anatomy

Role of adjuncts
High-speed burr
Phenol
Cementation with PMMA – thermal necrosis and
cytotoxic effects
Liquid nitrogen (cryotherapy)– associated with high
incidence of local wound and bone complications
AIM : to ‘extend’ the curettage or intralesional
excision by chemical or physical means

Molecular Therapy
BISPHOSPHONATES
Widely used to inhibit osteolysis in conditions such as
osteoporosis, Paget’s disease and metastatic cancer
Act by inhibiting farnesyl diphosphate synthase, an
enzyme in the mevalonate pathway
Inhibition of osteoclastic formation
Decrease osteoclast resorption
Increased osteoclast apoptosis

Tse et al , Bone 2008
Retrospective case-control study on 44 patients with appendicular GCT between 1998-2004
Intralesional curettage/wide excision followed with
cementation or biological reconstruction.
24 patients received intravenous and oral bisphosphonate peri-operatively
Average f/u was 48 months
1 of 24 pt (4.2%) developed local recurrence vs 6 of 20 in control group (30%), p=0.056

Balke et al, BMC Cancer 2010 24 cases of GCT recruited from four European centers (5
aggressive primary, 7 recurrence and 12 metastatic disease)
Indication, dose and method of administration differed between various centers
Zoledronic acid most commonly used
Follow up period 36-64 months
Results:
Most inoperable sacral/pelvic tumours did not increase in size
No further recurrence was seen in GCTs that had repeatedly recurred in bone and soft tissue
Lung metastasis did not increase in size or number during course of treatment with Bisphosphonate

Molecular and Cellular biology
of GCT Biphenotypic
Osteoclast-like giant cells – RANK
Mesenchymal neoplastic stromal cells - RANKL
Interaction between these cells lead to bone
resorption

Denosumab
Denosumab – a monoclonal antibody that binds RANKL
and directly inhibits osteoclastogenesis

Denosumab
Thomas et al , The Lancet Oncology, 2010
37 patients with recurrent or unresectable GCT enrolled
Most common sites : pelvis, lungs and lower limb
All treated with 120mg Denosumab s/c once a month
for 25 weeks
30 of 35 patients showed tumour response, defined by at
least 90% elimination of giant cells or no radiologic
progression of target lesion
In 1 patient, tumour progression recurred after
Denosumab was discontinued.

Chawla et al, Lancet Oncology 2013
International , open-label , phase 2 trial (282 patients)
3 Cohorts : 1. Unsalvageable CGTB
2. Salvageable – morbid surgery
3. Previous denosumab GCTB study transfer
Results:
Safety analysis:
1% Osteonecrosis of jaw
5% hypocalcaemia
3% hypophosphataemia
1% anaemia, back and extremity pain
96% in cohort-1 had no disease progression (13 mths)
74% in cohort-2 had no surgery and 62% patients who had surgery
underwent a less morbid procedure (9 mths)

? Secondary malignancy following Denosumab therapy

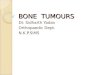
August 2010 Sept 2009
January 2013
DENOSUMAB
5/12 post Denosumab June 2014
July 2009

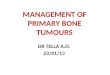
Santosh et al, 2015.
Case report on a Pseudosarcomatous Spindle cell
Proliferation with Osteoid Matrix Mimicking
Osteosarcoma in a 68 years old female with left
distal radius GCT following Denosumab therapy

Conclusion
GCTB is a benign but locally aggressive bone
tumour with a high propensity for recurrence
Goal of treatment is to achieve local control whilst
preserving function
Denosumab has shown promising results in the
management of unresectable/recurrent GCT
Concern regarding secondary malignancy
following Denosumab therapy warrants further
prospective studies

Thank you