Embed Size (px)
Citation preview

Noodzaak snelle beoordeling en gezamenlijke zorg
Elisabeth Brouwer internist reumatoloog UMCG
Giant Cell (Reuscel) arteritis en PMR

Research and Focus 2017
Dept. Rheumatology and Clinical Immunology
LifeLines,
Healthy Ageing,
Autoimmunity
RA
RARA
Amyloidosis
SpA
Care and Research
International
Regional
Autoantibodies

UMC Groningen Research Focus

Age-associated Changes in Immune
Function and Tissue
http://www.metrolic.com/fountain-of-youth-discovered-scientists-reverse-ageing-process-in-mice-149820/

Indeling Presentatie
• Grote Vaten Vasculitis/GCA
• Diagnostiek
• Behandeling
• PMR
• Diagnostiek
• Behandeling
• Zorgpad GCA/PMR
• Vragen


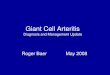
C-GCA, LV-GCA and PMR
Disease spectrum
Adapted from Dejaco et al. Rheumatology 2016

GCA and PMR:
Frequently occuring diseases
RAPMR♀
♂
Crowson et al. A&R 2011
GCA

Kliniek GCA/PMR
C(craniele)-GCA
– Hoofdpijn (a. temporalis)
– Visusstoornis/verlies (a. oftalmica)
– Kaakclaudicatie (a. facialis)
– Scalp necrosis (a. occipitalis en a. temporalis)
– TIA/CVA (a. carotis, a. vertebralis)
LV (Large Vessel)-GCA
– Malaise , koorts, afvallen
– Arm (a. axillaris, a. subclavia)/been (a. iliaca, a. femoralis) claudicatie
– PMR
– Aneurysma aortae
– PMR klachten

Hoe stel je de Diagnose?
• RCA patiënten dienen te voldoen aan de ACR classificatie criteria;
• Leeftijd > 50 jaar
• Nieuwe of andere hoofdpijn
• Gevoeligheid, verminderde pulsaties of verdikte temporaal arterie
• BSE > 50 mm / uur
• Biopsie; mononucleaire granulomateuze arteritis temporalis
Hunder GC et al . Arthritis Rheum 1990

Klacht Sens• Hoofdpijn 76%• Afvallen 43%• Koorts 42%• Moeheid 39%• Anorexie 35%• Polymyalgia 34%• Kaakclaudicatio 34%• Visusdaling (unilat) 24%• Visusdaling 9%
– (bilat) 15%• Diplopie
Smetana GW et al. JAMA 2002
Verschijnsel Sens• AT verdikking 47%• Geen pulsaties AT 45%• Schedelpijn 31%
Lab. Afwijking Sens• ↑ BSE 96%• Anemie 44%

• Sensitiviteit bepaald
door
– segmentale karakter
van de aandoening
– grootte biopsie > 2-3
cm
• Tweede biopsie
(contralat): ca. 5% meer
opbrengstNiederkohr RD Ophthalmology 2005Boyev LR et al Am J Ophthalmol 1999
Gouden Standaard biopsie Temporaal
arterie

Inflamed and occluded artery
Aneurysm
Normal artery
Leading to
ischemia
Risk of rupture
Outcome; stenosis C-GCA and
aneurysms LV-GCA


Ulcera hoofdhuid

Chewing gum test for jaw claudication in GCA
• Chew gum at the rate of of one chew per second
• Pain after 2-3 minutes of chewing
• Disappearence in rest
• Reproducible
Hung Kuo et al Sydney Australia NEJM May 5, 2016

Aanvullende Diagnostiek/ Imaging

Examination of the Temporal Arteries
The patient
should be supine
Start with longitudinal
scan
in front of the left ear
Use colour Doppler
mode
Bruyn GA & Schmidt WA. Introductory guide to musculoskeletal ultrasound for therheumatologist, 2006, Houten, NL: http://ultrasoundfortherheumatologist.com

Ultrasound: Findings in GCA
normal longitudinal
„halo“ longitudinal
normal transverse
„halo“ transverse
Wolfgang SchmidtTABUL

Ultrasound: Findings in GCA
The wall swelling („halo“) in temporal arteritis is hypoechic, not anechoic!
The artery lumen is anechoic
Wolfgang SchmidtTABUL

Arteriosclerosis is hyperechoic
Ultrasound: Findings in GCA
Wolfgang SchmidtTABUL

Axillary Artery Ultrasound
Schmidt WA, et al. Rheumatology 2008;47:96-101
Start with axillary longitudinalstandard scan for shoulder
Move probe about 1 cm mediallyin most patients
In this patient the axillary arterylocalises adjacent to theaxillary recess
Patient withLarge-vessel GCA

Ultrasound:
Sensitivity / Specificity
Sensitivity Specificity
72 % 55 % 99,5 %94 %
75 % 66 % 96 % 95 %
88 % 87 % 96 % 96 %
1 StudyN=751TA:101
23 StudiesN=2036TA:476
Largest series: Schmidt WA, et al. Ann Int Med 2003;138:609Meta-analysis: Karassa FB, et al. Ann Int Med 2005;142:359-69
Stenosis
Occlusion
Halo
All
together

FDG/PET/CT

FDG/PET/CT

FDG/PET/CT

PET/CT
• Betrouwbaarheid afhankelijk techniek en beoordeellaar
• Betrouwbaarheid afhankelijk medicatie
• First impression
• Aorta to Liver SUV
• Pattern of Uptake
Lensen et al Biomed Res Int 2015
Stellingwerf et al Clinical Nuclear Medicine 2015

CTA en MRA

MRA 3 Tesla T1Fat suppressed
Veldhoen Eur Rad 2014

MRA 1.5 Tesla T1Fat suppressed
Veldhoen Eur Rad 2014

Behandeling
• Inductie therapie:
• Start Prednisolon 40-60 mg/dag.
• Indien oogheelkundige betrokkenheid: opname voor 3 maal 1000 mg Methylprednisolon (Solu-medrol) i.v.
• Afbouwschema:
• Indien klinische en biochemische remissie na 3-4 weken bereikt is, start afbouwschema:
• met 10 mg/2 weken tot 20 mg/dag
• daarna met 2,5 mg/4 weken (mits remissie is bereikt) tot 10 mg/dag
• daarna met 1 mg/4 weken (mits remissie is bereikt) tot 0 (zie voorbeeld PMR).

Co-mediactie
• Omeprazol 20mg
• Alendroninezuur 70 mg/week
• Calcichew D3 500mg/ Vit2 dd
• Zo nodig paracetamol 3 dd 1 gram
• Naproxen max 2 dd 500 mg
• Carbasalaat calcium = ter discussie

Monitoren
• Ziekte activiteit GCA; symptomen systemische dan wel craniele GCA + een verhoogde BSE dan wel crp
• Schade GCA; Screen in hoog risico groep op AA dmv X-Thorax AP en Lateraal (TTE op indicatie) en echo abdomen ieder 2 jaar
• Bijwerkingen; Maag, BDM en Vit D

Risico Aneurysma / Stenose Aorta
• Oudere leeftijd hoger risico
• BSE niet heel hoog
• Wel hoge FDG PET uptake
• Geen dyslipidemie
• Voorafgaand CVA
• HLA DRB1*04, meer inflammatie

Recidief/ relapse
• Definitie: terugkeer symptomatologie in
combinatie met oplopen BSE en CRP;
• Verhoog prednisolon dosis met ten minste 10
mg per dag, indien dosis ten tijde van recidief
nog boven de 15 mg is.
• Start Methotrexaat als adjuvante behandeling
Jover et al Ann Int med 2001, Hoffman AR 2002, Spiera, Mahr AR 2007

Risk of Relapse
Large-vessel giant cell arteritis: a cohort studyFrancesco Muratore, Tanaz A. Kermani, Cynthia S. Crowson,Abigail B. GreenCarlo Salvarani1, Eric L. Matteson andKenneth J. Warrington. Rheumatology 2014

Duration of Steroid Treatment
Large-vessel giant cell arteritis: a cohort studyFrancesco Muratore, Tanaz A. Kermani, Cynthia S. Crowson,Abigail B. GreenCarlo Salvarani1, Eric L. Matteson andKenneth J. Warrington. Rheumatology 2014

Mahr et al. AR 2007
Methotrexate is effective in GCA

CS and TS- DMARDS
CS-DMARDS
Not effective
• Hydroxychloroquine (1 RCT) (moderate quality of evidence)
• Cyclosporine (2 RCTs) (moderate quality of evidence)
Effective
• Azathioprine (moderate quality of evidence),
• leflunomide, mycophenolatemofetil, cyclophosphamide and dapsone (low quality of evidence)
TS-DMARDS
• Baricitinib (selective and reversible inhibitor of JAK1 and JAK2 suppressive effect on both the Th17 (IL-6, IL-23) and Th1 (IL-12, IFN-γ) pathways. ClinicalTrials.gov NCT03026504; Baricitinib in Relapsing Giant Cell Arteritis (GCA): A
Phase II, Single-institution, Open-label Pilot Study Matthew J Koster
Buttgereit JAMA June 14, 2016 Volume 315, Number 22, Misra Autoimmunity Reviews
16(2017); 179-191, Smolen ARD 2013

TNF blockade
• Infliximab 1 RCT not effective (Hoffmann 2007 )
• Etanercept 1 RCT not effective (Martinez 2008)
• Adalimumab 1 RCT not effective (Seror 2014)
IL-1 blockade
• Anakinra human interleukin -1-receptor
antagonist (r-metHuIL-1ra) (Ly JBS 2013)
• Gevokizumab monoclonal antibody
targeting interleukin-1-beta (IL-1β) (no results)
Smolen ARD 2013

Breakthrough targeting IL-6
Masahiko Mihara et al. Clin. Sci. 2012;122:143-159
©2012 by Portland Press Ltd

Tocilizumab= anti-Interleukine 6 receptor Mab


Sustained Remission: Primary and
Key Secondary End Points (cont)
14 17,6
56 53,1
0
20
40
60
80
100
n = 50 51 100 49Pat
ien
ts in
Su
stai
ned
Rem
issi
on
, %
p < 0.0001
p < 0.0001
p < 0.0001
p = 0.0002
• Superior efficacy of TCZ + 26-week prednisone versus
26-week and 52-week prednisone alone
PBO + 26 PBO + 52 TCZ QW TCZ Q2W
44
https://www.rocherheumatology.com/1/212/GIACTAOral_Stone

Indeling
• Grote Vaten Vasculitis/GCA
• Diagnostiek
• Behandeling
• PMR
• Diagnostiek
• Behandeling
• Zorgpad GCA/PMR
• Vragen

Polymyalgia Rheumatica
• Inflammatoire ziekte: pijn en ochtendstijfheid
in schoudergordel, heupgordel en nek
• Leeftijd > 50,
• 30-50% van patiënten overlap met GCA
• Vaak (sterk) verhoogde BSE en CRP


Diagnose
• Geen gouden standaard
• Geen ziekte specifieke biomarker
• Pijn en stijfheid komen bij veel reumatische
ziekten voor RA / OA
• Heterogeniteit in het ziekteverloop
• Respons op glucocorticoiden vaak langzaam
• Meerdere Classificatie Criteria




PMR and imaging
• Many different imaging abnormalities have been described in PMR Camelllino and Cimmino 2012
• Shoulder ultrasound has been suggested to be especially useful Sakellariou et al., 2013
• Unlike RA, capsular/extracapsular inflammation > synovial inflammation in PMR Marzo et al 1997,
McGonagle et al., 2001, Cimmino et al., 2013
• Imaging could identify the anatomical structure involved (e.g. synovitis versus bursitis) with greater precision, improving diagnostic accuracy


Classificatie EULAR/ACR 2012



Behandeling PMR
• Anno 2017 prednisolon monotherapie?

A multicenter randomized placebo controlled
treatment study of leflunomide in
polymyalgia rheumatica
Maria Sandovici MDPhD
Suzanne Arends PhD
Liesbeth Brouwer MDPhD

Background
• PMR is the most common inflammatory musculoskeletal
disease in adults >50 years old
• Glucocorticoids are the mainstay of treatment
• Unmet need for alternative/adjuvant treatments
– 50% of patients relapse or have difficulties to reduce glucocorticoids
– Glucocorticoids have short-term and long-term side-effects/toxicity
• Low dose Methotrexate low-moderate GC-sparing effect
– 2 blinded RCTs and 4 open label studies

Why leflunomide
• Leflunomide has shown effectiveness in 2 case
series
Dasgupta et al. 2012, Diamantopoulos et al 2013
• Effective, inexpensive and safe DMARD
• Inhibits
– the dendritic cell maturation and their T cell stimulatory
capacity
– production of IL-17, TNF-α, IL-2, IL-6,IL-12

A randomized, double-blind, placebo controlled study
� Prednisolone tapering:
week 1-4 prednisolone 15 mg once daily
week 5-8 prednisolone 12.5 mg once daily
week 9-12 prednisolone 10 mg once daily
week 13-16 prednisolone 7.5 mg once daily
week 17-20 prednisolone 5 mg once daily
week 21-24 prednisolone 2.5 mg once daily
week 25-26 prednisolone 2.5 mg every other day
week 27 no steroids
� Leflunomide/Placebo:
Week 1-2: 20 mg every other day
From week 3 on till 24 months: 20 mg once
daily
� Intolerance /side effects
� Methotrexate 10-15 mg/week
On Physicians decision as rescue therapy

Criteria for response, relapse or recurrence of PMR
Consensus criteria for PMR
Response will be assessed by
(1) > 70% patient global improvement,
(2) > 70% reduction in morning stiffness
(3) Normal CRP (<5) and / or ESR (< 30)
Relapse
Signs of active PMR (aching and stiffness at shoulder, hip girdle, or both)
Increased ESR (>30 mm/h) and/or CRP (>5 mg/L).
Recurrence if it was observed after steroid withdrawal.
Criteria for remission
No signs of active PMR (aching and stiffness at shoulder, hip girdle, or
both) and a normal ESR and/or CRP

Participating Centers
• University Medical Centre Groningen, the Netherlands
• ZGT (Zorg Groep Twente), Almelo, the Netherlands
• Southend University Hospital, Westcliff-on-sea, UK
• Chapel Allerton Hospital, Leeds Teaching Hospitals NHS Trust, Leeds, UK
• Medical University Graz, Austria
• Clinic for Rheumatology and Clinical Immunology, Charite, Berlin, Germany?
• Aarhus University Hospital Nørrebrogade, Aarhus, Denmark
• Esbjerg /Kristiansand

Costs
• Monitoring in the Netherlands€ 21.000,-.
• Monitoring European Centers € 43.000,-.
• Building CRF
• Costs production capsulated leflunomide
• Costs for running the study/ performing US/
biobanking
• Costs partly provided by daily clinical practice

Preparation Medical Ethical Proposal, optimization TRIAL design by Trial methodologist
Development CRF, install data safety monitoring board
Preparation leflunomide and placebo tablets
Training CRF, S(AE) reporting, biobanking and ultrasound
Randomization inception cohort UMCG/ ZGTRaise international funding
Set up participating European centers Optimize eCRF / protocol/ include feedback patients
Randomization validation cohort
Assessments 2 weeks, 1, 3, 6 and 9, 12, 18 and 24 months
Relapse visits
Monitoring
24 months end of study
Data cleaning and analysis

Indeling
• Grote Vaten Vasculitis/GCA
• Diagnostiek
• Behandeling
• PMR
• Diagnostiek
• Behandeling
• Zorgpad GCA/PMR
• Vragen

NHG richtlijn M92 februari 2010
Polymyalgia Rheumatica en Arteriitis Temporalis
• VERWIJZING OF CONSULTATIE
• Verwijs bij:
• acute visusdaling, (geheel of gedeeltelijk) gezichtsveldverlies of dubbelzien met spoed naar de oogarts;
• vermoeden van arteriitis temporalis naar een reumatoloog/internist binnen 24 uur;
• ernstige bijwerkingen van of contra-indicaties voor langdurig gebruik van glucocorticoïden naar de reumatoloog/internist voor een eventuele behandeling met methotrexaat.

Acute zorg bij uitval
• De diagnostiek dient zo georganiseerd te zijn dat er zo min mogelijk tijdverlies plaatsvindt. Het dient adequaat en tijdefficiënt plaats te vinden. Met ander woorden bij voorkeur georganiseerd op 1 dagdeel
• Echo/doppler en of Pet/CT• Arteria Temporalis biopt• Bij visus klachten spoedconsult OHK• Bij Amaurosis fugax spoedconsult neuroloog• Bij aortitis ook infecties zoal lues uitsluiten en
bloedkweken doen

Problemen GCA spoed
• Multi-disciplinaire Structuur CSO Onvoldoende Afgestemd
– Reumatologie / Systeemziekten/ Interne geneeskunde– Oogheelkunde– Neurologie – Vaatlaboratorium– Neurochirurgie– Nucleaire geneeskunde)
• Verwijzingsstructuur / Afsprakenstructuur
Belangrijk onderscheid spoed vs niet spoed

Patil ClinExpRheum 2014

Chronische zorg
• De diagnostiek dient zo georganiseerd te zijn dat er zo min mogelijk tijdverlies plaatsvindt. Het dient adequaat en tijdefficiënt plaats te vinden. Met ander woorden bij voorkeur georganiseerd op 1 dagdeel
• Echo/doppler en/of PET/CT• Arteria Temporalis biopt• Bij Aortitis ook infecties zoal lues uitsluiten
en bloedkweken doen

72
Afspraak 1
– Bloedonderzoek (GCA screenings protocol)
– US vaten
– Bij visusklachten OHK
Afspraak 2
– Bioptafname (neurochirurgie) indien cranieleGCA.
– PET/CT indien systemische RCA
2 -3 dagen
Afspraak 3
– Uitslag biopsie en PET/CT
– Start steroiden 40-60 mg per dag in combinatie met gastro- en bot-protectie
Afspraak 3 / 4
– Afspraak systeemziekten en OHK indien noodzaak OHK follow up.
– Inkaart brengen risico op comorbiditeit; Osteoporose (BDM), Tensie, HbA1C, Infecties
Vervolgtraject:
– Geen GCA� afronding GCA traject
– Indien GCA � tight control vanwege hoge dosis
glucorticoiden en hoge kans op bijwerkingen
Zorgpad Verdenking GCA

Zorgpad Diagnostiek GCA Multidisciplinair/ Landelijk
-Verwijzing verdenking GCA en PMR:
- Screening brief door arts vasculitis expertisecentrum
- Med secr Reumatologie en Klinische Immunologie maakt afspraak op korte termijn
Afspraak 1
– Bloedonderzoek Hb,BSE en CRP
– C(raniele) GCA US vaatlab/biopsie
– LV(Large Vessel ) GCA PET/CT
– C-GCA en LV-GCA samen US vaatlab/ biopsie/ PET/CT
Klachten van de VISUS of TIA/CVA verdacht voor RCA; spoedconsult OHK/neurologie

Samenvattend GCA
• Patienten hoeven niet altijd hoofdpijn te hebben
• Wel acute fase , verhoogde BSE echter in 3% van de patienten niet verhoogd
• OHK betrokkenheid 30%, kan nog ontstaan na start steroiden
• Biopt is nog steeds gouden standaard, maar kan negatief zijn

Samenvatting GCA/ PMR
• GCA veelvoorkomende aandoening overlap met PMR
• Bij zowel GCA als PMR geen ACPA
• Alle grote vaten kunnen meedoen
• Behandeling prednisolon
• DMARD’s in opkomst

UMCG poli GCA en PMR
• Snelle Service
• Diagnostiek oa Echo, biopt, PET/low dose CT
• Start behandeling na diagnostiek
• Onderzoek gericht op verbetering diagnostiek en behandeling.
• Contact:
[email protected] 77053 [email protected] [email protected] volgt

Bedankt voor uw aandacht
• Grote Vaten Vasculitis/GCA
• Diagnostiek
• Behandeling
• PMR
• Diagnostiek
• Behandeling
• Zorgpad GCA/PMR
• Vragen

• Dept. of Pathology
– Arjan Diepstra
– Erlin Haacke
• Dept. of Laboratory Medicine
– Caroline Roozendaal
– Bartjan Kroesen
• Dept. of Nephrology
– Jan Stephan Sanders
– Coen Stegeman
• Dept. of Laboratory Medicine
– Peter Heeringa
• Dept. of Rheumatology and Clinical
Immunology
– Niels van der Geest
– Yannick van Sleen
– Jacolien Graver
– Qi Wang
– Minke Huitema
– Nico Bos
– Bram Rutgers
– Maria Sandovici
– Wayel Abdulahad
– Mieke Boots
NC Smit fonds
Acknowledgements