Embed Size (px)
Citation preview

Giancarlo Agnelli
Internal Emergency and Vascular Medicine - Stroke Unit
University of Perugia, Italy
NOACs for VTE treatment in cancer patients

Anticoagulant agents in cancer patients
Clinical settings
• Prophylaxis of venous thromboembolism after cancer
surgery
• Prophylaxis of venous thromboembolism in ambulatory
cancer patients
• Treatment of venous thromboembolism

Anticoagulant agents in cancer patients
Clinical settings
• Prophylaxis of venous thromboembolism after cancer
surgery
• Prophylaxis of venous thromboembolism in ambulatory
cancer patients
• Treatment of venous thromboembolism

• The issue
• The benchmark and the current guidelines
• Evidence for NOACs
• The recently published or ongoing NOACs studies
My talk today
Treatment of VTE in patients with cancer

• The issue
• The benchmark and the current guidelines
• Evidence for NOACs
• The recently published or ongoing NOACs studies
My talk today
Treatment of VTE in patients with cancer

• 15-25% of VTE patients (5% in phase III NOACs RCTs)
• Poor clinical status
• Complexity of clinical care
• Concomitant anticancer treatments
• High risk of recurrence and treatment-related bleeding
VTE treatment in cancer patients
Peculiarities of cancer patients

Recurrent VTE and bleeding during anticoagulant treatment
1 year
0
10
20
30
Re
curr
ent V
TE
, %
Hazard ratio 3.2 (1.9 - 5.4)
Cancer 21%
No Cancer 7%
1 year
0
10
20
30
Ma
jor
Ble
edin
g, %
Cancer 12%
No Cancer 5%
Hazard ratio 2.2 (1.2 - 4.1)
Prandoni et al., Blood 2002

• The issue
• The benchmark and the current guidelines
• Evidence for NOACs
• The recently published or ongoing NOACs studies
My talk today
Treatment of VTE in patients with cancer

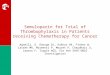
Dalteparin vs. Warfarin in Cancer patients with VTE
0
Days after randomisation
30 60 90 120 150 180 210 0
5
10
15
20
25
V
TE
re
cu
rre
nce (
%)
Risk reduction=52% p=0.0017
Dalteparin/VKA
Lee et al., N Engl J Med 2003
CLOT Study
Cancer patients with acute DVT and/or PE
n=308
n=298
OAC with VKA Dalteparin
Dalteparin Dalteparin (¾ dose)
4 wks R
Dalteparin
15.8%
8.0%

Lee et al. JAMA 2015
HR: 0.65 [95% CI 0,41-1,03; P=0.07]
10,5%
7.2%
HR: 0.89 [95% CI 0.40-1.99; P=0.77]
Recurrent venous thromboembolism Major bleeding
All-Cause Mortality
HR: 1.08 [95% CI 0.85-1.36; P=0.54]
34.7%
32.2%
The Catch study

Initial treatment LMWH is the
preferred approach
for the initial 5-10
days.
LMWH, UFH or
fondaparinux
according to
patient’s
characeristics and
clinical situation
Weight –adjusted
LMWH,
If creatinine
clearance < 25-30
ml/min either UFH
or LMWH with
antiXa monitoring
LMWH, UFH or
fondaparinux for
the first 10 days, if
severe renal failure
UFH or early VKA
LMWH for the first
3-6 months of long-
term anticoagulant
therapy (Grade 1A)
Long term
treatment
LMWH for at least 6
months; VKA are
acceptable when
LMWH are not
available,
LMWH is preferred LMWH LMWH for 3-6
months; LMWH or
VKA beyond 6
months
Cancer patients
with VTE are
recommended to
receive long-term
LMWH
monotherapy
(grade 2B)
Optimal
duration
Indefinite
anticoagulation in
patients with active
cancer
Indefinite
anticoagulation in
patients with active
cancer or
persistent risk
factors
for at least 3-6
months
Long term
treatment for
patients with active
cancer
Not specified indefinitely or until
the cancer is
resolved (Grade
1C)
VTE treatment in cancer patients

• LMWH-associated risk recurrence still significant (10%)
• No reduction in bleeding rate
• Subcutaneous injections uncomfortable and difficult to
maintain long-term (adherence or persistence to/on
treatment)
• Treatment after 6 months unclear
After the Clot & Catch studies
Remaining issues

van der Wall et al, J Thromb Haemost 2017
1.0
0.9
0.8
0.7
0.6
0.5
0 30 60 90 120 150 180
Days of trratment
LM
WH
d
isco
nti
nu
ati
on
Number of
patients
372 354 348 325 316 307 293
LMWH discontinuation in patients treated for VTE

• The issue
• The benchmark and the current guidelines
• Evidence for NOACs
• The recently published or ongoing NOACs studies
My talk today
Treatment of VTE in patients with cancer

VTE treatment & cancer patients
NOACs studies * 3-8%
Clinical practice: 18-20%
Study population likely not-representative of the full-spectrum of
patients with cancer in the NOACs studies

NOACs for VTE treatment in cancer patients
Level of Evidence
• Sub-group analyses of phase III RCT including patients
with cancer
• Meta-analyses on cancer patients included in phase III
RCT
• Phase III randomized RCT

VTE and VTE related death Major bleeding
Apixaban
Enoxaparin/ Warfarin
Apixaban
Enoxaparin/ Warfarin
Agnelli et al., J Thromb Haemost 2015
Amplify cancer sub-analysis: results by cancer status

6 studies: 1132 patients with cancer at baseline Recurrent VTE
Study or Subgroup
AMPLIFY 2013
EINSTEIN-DVT 2010
EINSTEIN-PE 2012
HOKUSAI 2013
RECOVER I & II 2013
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.36, df = 4 (P = 0.99); I² = 0%
Test for overall effect: Z = 1.62 (P = 0.10)
Events
3
4
2
4
10
23
Total
81
118
114
109
173
595
Events
5
5
3
7
12
32
Total
78
89
109
99
162
537
Weight
15.2%
17.1%
9.4%
22.0%
36.3%
100.0%
M-H, Fixed, 95% CI
0.56 [0.13, 2.43]
0.59 [0.15, 2.26]
0.63 [0.10, 3.85]
0.50 [0.14, 1.77]
0.77 [0.32, 1.83]
0.63 [0.37, 1.10]
DOA Comparator Odds Ratio Odds Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favors DOA Favors comparator
DOACs for cancer-associated VTE: meta-analysis
3.8% vs 5.9%
Vedovati et al., Chest 2015

Study or Subgroup
AMPLIFY 2013
EINSTEIN DVT & PE 2013
HOKUSAI 2013
RECOVER I & II 2013
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.40, df = 3 (P = 0.70); I² = 0%
Test for overall effect: Z = 0.81 (P = 0.42)
Events
2
6
5
6
19
Total
87
232
109
159
587
Events
4
8
3
7
22
Total
80
196
99
152
527
Weight
18.2%
37.7%
13.4%
30.7%
100.0%
M-H, Fixed, 95% CI
0.45 [0.08, 2.51]
0.62 [0.21, 1.83]
1.54 [0.36, 6.61]
0.81 [0.27, 2.47]
0.77 [0.41, 1.44]
DOA Comparator Odds Ratio Odds Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favors DOA Favors comparator
3.2% vs 4.2%
DOACs for cancer-associated VTE: meta-analysis
Vedovati et al., Chest 2015
6 studies: 1132 patients with cancer at baseline Major bleeding

• The issue
• The benchmark and the current guidelines
• Evidence for NOACs
• The recently published or ongoing NOACs studies
My talk today
Treatment of VTE in patients with cancer

Dalteparin 150 IU/kg QD
Patients with cancer and objectively confirmed VTE;
Stratified by bleeding risk and dose-adjustment;
1:1 randomization into 2 treatment groups
R A N D O M I Z E
LMWH* Edoxaban QD†
Dalteparin 200 IU/kg QD
Day 5
Day 0 Day 30 Month 12
Planned N ≈ 1000
Planned enrollment is approximately 130 study sites across 13 countries in North America, Europe,
Australia, and New Zealand
Estimated completion date: December 2017 (Final data collection date for primary outcome measure)
*At least 5 days of LMWH. The choice of the LMWH type and lead-in duration will be left to the treating physician; †Edoxaban 60 mg (30
mg QD for patients requiring dose adjustment for CrCL = 30-50 mL/min, body weight 60 kg, and/or concomitant P-gp inhibitor use);
CrCL = creatinine clearance; LMWH = low-molecular weight heparin; P-gp = P-glycoprotein; QD = once-daily; VTE = venous
thromboembolism.
Van Es et al. Thromb Haemost 2015

Raskob et al., NEJM 2017
Recurrent VTE & MB
Edoxaban: 12.8%
Dalteparin: 13.5%
HR: 0.97 (0.70-1.36)
P=0.006 for non-inferiority

Raskob et al. NEJM 2017
Recurrent VTE
Edoxaban: 7.9%
Dalteparin: 11.3%
HR: 0.71 (0.48-1.06)
Major bleeding
Edoxaban: 6.9%
Dalteparin: 4.0%
HR: 1.77 (1.77-3.04)

select-d
Rivaroxaban* Cancer patients with
symptomatic DVT and/or PE
without chemotherapy
N~530 Dalteparin#
PE index event or RVT
positive before 6
months N~300
RVT negative before 6
months N~130 No treatment
Fo
llo
w U
p
FPFV: Q4-13 LPLV: 16/17
Indication: VTEx patients with cancer
Short design: Prospective, randomized,
open-label, multicentre pilot phase III study
Rationale: To assess the efficacy and safety of rivaroxaban versus dalteparin for the treatment of VTE in patients with cancer not currently receiving chemotherapy
R
6 months
Rivaroxaban
Placebo
R
12 months
*15 mg bid for 21 days followed by 20 mg od; for patients with CrCl 30–49 ml/min dosing recommendations as in rivaroxaban SmPC; if a patient’s
platelet counts falls to <50,000/mm3, rivaroxaban should be discontinued until the platelet count recovers to above 50,000/mm3; #200 IU/kg od for the
first 30 days of treatment followed by 150 IU/kg od; if a patient’s platelet count falls to 50,000–100,000/mm3 the daily dose of dalteparin should be
reduced by 2500 IU until platelet count returns to ≥100,000/mm3; if a patient’s platelet count falls to <50,000/mm3, dalteparin should be discontinued
until the platelet count recovers to above 50,000/mm3
IIR, Investigator Initiated Research; FU, follow-up; R, randomization; RVT, residual vein thrombosis
http://www2.warwick.ac.uk/fac/med/research/hscience/ctu/trials/cancer/select-d/; EudraCT number: 2012-005589-37

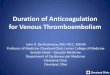
Young A et al, JCO 2018
select-d: VTE recurrence
Dalteparin
Rivaroxaban
Number at risk
Dalteparin 203 171 139 115
Rivaroxaban 203 174 149 134
40
35
30
25
20
15
10
5
0
0 1 2 3 4 5 6
Time from trial entry (months)
VT
E r
ec
urr
en
ce (
%)
Outcome at 6 months Rivaroxaban
(n=203) Dalteparin
(n=203)
Lower limb DVT/PE
recurrence,
(95% CI)
3%
(1-7)
9%
(6-15)

select-d: Major, Fatal and CRNM bleeding
*.
Young A et al, JCO 2018
Most Major Bleedings events were Gastrointestinal Bleedings*. No Central Nervous System Bleeding
was observed in rivaroxaban and dalteparin groups.

Clinical outcome studies
• Casta Diva
• Adam
• Canvas
• Caravaggio
Ongoing trials in patients with cancer and VTE

Caravaggio study design
Randomized, open-label, PROBE, non inferiority study
Symptomatic or
unsuspected
proximal lower-limb
DVT
R
Apixaban Apixaban
10 mg bid 5 mg bid
Dalteparin 200 IU/kg od Dalteparin 150 IU/kg od
30 days
observation
period
Day 1 Day 7 Day 30 6 months Symptomatic or
unsuspected PE in a
segmental or more
proximal pulmonary
artery
<72 hours*
Principal Investigator Giancarlo Agnelli
Countries Involved 11
Centers Involved ≈ 140
Sample Size 1168 patients
* Max time allowed between diagnosis and randomization

Conclusions
• Patients with CAT have a higher risk of recurrent VTE and
bleeding than the general population
• Evidence suggests that NOACs could be alternatives to
conventional therapy for VTE in cancer patients
• Edoxaban and rivaroxaban were at least as effective as
LMWH in cancer patients, but were associated with
significantly higher rates of major bleeding or CRNMB
• Ongoing studies of NOACs (vs LMWH) will provide
further information on the role of NOACs CAT patients
NOACs for VTE treatment in cancer patients