Embed Size (px)
Citation preview

GI Lab #3- Small Intestine & Pancreas
Drs. Vanley, Wu, & Edwards
November 4, 2011

Case 1: Scenario -I
• A 44-year-old white male presented with a seven-month history of increasing diarrhea. The frequency of his bowel movements had increased to 5-7 per day, and his stools were yellow and malodorous and floated at the top of the water in the toilet. He had occasional abdominal cramping, but no tenesmus, melena, or bleeding. His appetite was good, but he had experienced gradual weight loss. His bowel movement frequency would decrease upon fasting and would increase with food intake. A family history of a brother with chronic diarrhea was elicited.

Scenario - II
• Stool tests revealed a stool output of 4128 g/d (nl 100-200 g/d) with fat excretion of 17 g/d (nl <5 g/d). Microscopic examination for ova and parasites and cultures for bacterial pathogens and acid-fast bacilli were negative. Blood testing showed mild anemia (Hct 36), hypoproteinemia (4.9 mg/dL), and hypoalbuminemia (3.4 mg/dL). Colonoscopy showed normal mucosa. Esophagogastroduodenoscopy (EGD) showed flat-appearing mucosa in the duodenum. Biopsies were performed. Serum tests for anti-endomysial and antigliadin antibodies were positive.
• The patient was discharged with appropriate dietary instructions. His diarrhea resolved, and his weight began to increase.

1 - Duodenum, normal - Low power In this duodenal biopsy specimen from a healthy person, note the appearance of the normal villi that can be best seen in
areas where the specimen is optimally oriented.

• 2 - Duodenum, normal villus - High power Although the lamina propria normally contains numerous lymphocytes, as seen here, only a few scattered lymphocytes are present within normal epithelium.

• 3 - Duodenum, celiac sprue - Low power Note the flattening of the duodenal villi. In this specimen, they are almost absent.

Question 1:
• What effect does this process have on the surface area available for absorption?

• 4 - Duodenum, celiac sprue - High power Note the numerous intraepithelial lymphocytes
Questions 2-4:
• Exposure to what dietary antigen is thought to be the cause of these changes?
• What food components contain this antigen?
• Will these histologic changes resolve with dietary modification?

• 5 - Small bowel, Whipple disease - Low power Numerous macrophages are seen throughout the lamina propria. With the routine H&E stain, the cytoplasm of these cells has a pale, foamy appearance. A PAS stain highlights the cytoplasmic inclusions, staining them a deep red. An electron micrograph reveals that these inclusions are rod-shaped bacilli. The large, round, empty spaces in the lamina propria are dilated lymphatic channels, due to lymphatic obstruction by macrophages.

• Whipple’s Disease, duodenum, PAS stain

CASE #2:
Diarrhea in an HIV+ Patient

CASE 2: SCENARIO
• A 36 -year-old HIV+ inmate presents with loose, watery stools, abdominal cramping, sweats, fevers, poor appetite (2 months) and 15 lbs weight loss. He is taking Combivir one tablet bid and Nelfinavir 1,000 mg tid, and Bactrim for secondary pneumocystis carinii pneumonia (PCP) prophylaxis. He reports good compliance with his medications, with an undetectable viral load and a CD4 count of 100 cells/mm3. He was diagnosed with HIV and PCP when he entered the U.S. from Mexico one year ago, at which time he had a CD4 count of 2 cells/mm3 and "high" HIV-1 viral load. He is an injecting drug user and has sex only with men. He reports unprotected sex with two anonymous partners two to three months ago when he traveled to Mexico.

Physical Exam
• He weighs 130 lbs and is afebrile with normal blood pressure, genital and neurologic exam. His pharynx was without thrush; there was no scleral jaundice, some temporal wasting, no rash, abdominal tenderness, organomegaly, lymphadenopathy, or peripheral edema.

Question 1:
• What is the differential diagnosis?

Differential Diagnosis• A: Opportunistic pathogens such as disseminated Mycobacterium
avium complex (MAC), PCP, and cytomegalovirus (CMV), should be considered, though PCP does not typically cause GI disease.
• Also at risk: – Entamoeba histolytica– Dientamoeba fragilis– Blastocystis hominis, – Giardia lamblia, – Campylobacter jejuni, – Shigella spp, Salmonella spp, C. difficile, – syphilis and herpes simplex virus.
• Because of recent travel to Mexico:– Escherichia coli, – Vibrio parahaemolyticus, – Yersinia spp, rotaviruses, and Norwalk-like viruses

Question 2:
• What tests should you perform/order?

Indicated tests:• A: Stool samples should be sent for WBCs, to help differentiate
inflammatory from non-inflammatory causes of diarrhea (history of watery as opposed to bloody diarrhea suggests non-inflammatory).
• Stool samples should also be sent for culture for enteric pathogens, smear for ova and parasites, Giardia antigen, Clostridium difficile toxins A and B, and acid-fast bacilli (AFB) smear and culture.
• Blood should be sent for AFB culture and routine bacterial culture.
• If there is no temporal association of the onset of diarrhea with antiretroviral therapy and the stool and blood studies are negative, the next step in the evaluation is a colonoscopy. The highest yield for colonoscopy is typically in patients with fever, weight loss, and a CD4 count of fewer than 200 cells/mm3.

Results:
• Concentrated exam of the stool showed many cysts of Giardia lamblia and Entamoeba histolytica. This diagnosis should be reported to the local public health department. Many Entamoeba coli cysts, many Endolimax nana cysts, and moderate Iodamoeba butschlii cysts were also seen. On auramine stain, moderate cryptosporidia were detected.

Giardia Lamblii Entamoeba Histolyticum
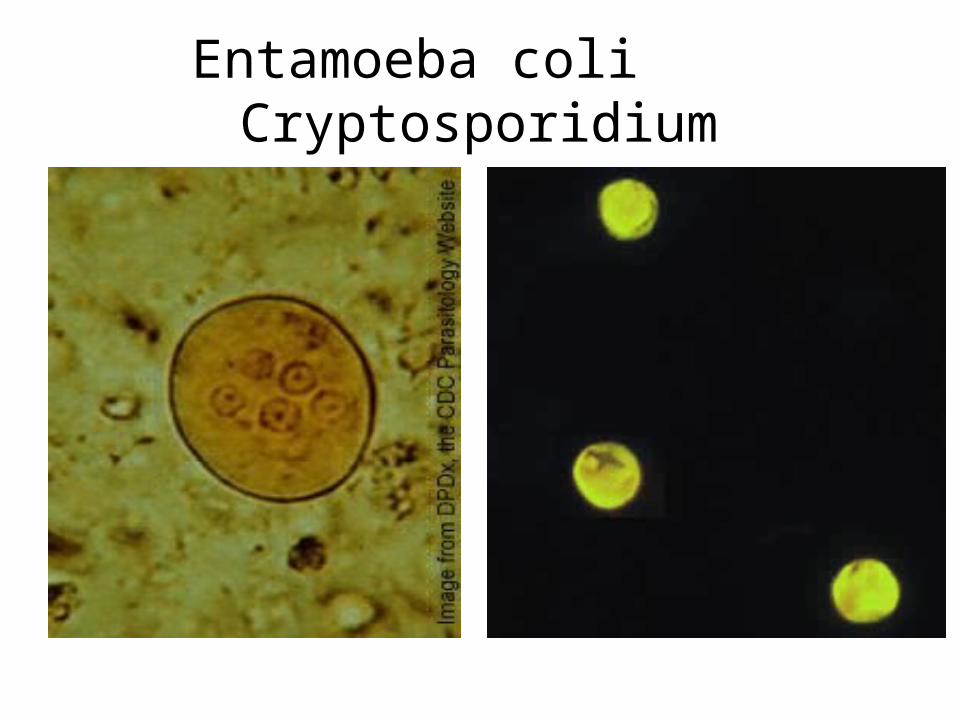
Entamoeba coli Cryptosporidium

Question 3:
• What treatment(s) should you offer this inmate? Are there drug-drug interactions to consider?

Answer• A: Endolimax nana, Entamoeba coli, and Iodamoeba butschlii are
nonpathogenic commensals and as such require no treatment.
• Giardia and Entamoeba histolytica can cause invasive disease and should generally be treated. The drug of choice for giardiasis is metronidazole 250 mg tid for seven days, which also has activity against E. histolytica.
• Unfortunately, there are no reliable therapies for Cryptosporidiosis
• Supportive care with hydration and nutrition, as well as institution of an effective antiretroviral regimen, are crucial aspects of care since improvement in the immune system often helps eradicate the infection.
• There are no known drug-drug interactions between metronidazole and the antiretrovirals he is currently taking.
Question 4:
• What infection-control measures should you recommend?

Answer
• To minimize transmission to others via fecal-oral spread, it is important to educate the inmate and staff on good hand-washing skills.
• He should be excluded from any kitchen work until his diarrhea has resolved and his stool is cleared of all organisms.
Case #3
Pancreatic Cancer

Scenario- I
• A 62-year-old man presented to his physician complaining of yellow eyes and weight loss. The patient had noted a decrease in his appetite and a decrease in his body weight of about 30 lb over the last 6 months. The patient admitted to loose bowel movements, which were greasy, clay colored, and malodorous. He had a 45 pack-year history of smoking and a history of heavy alcohol use for many years. There was no history of chemical or toxin exposure.

Scenario -2
• The physical examination revealed a thin, frail man with prominent bitemporal muscle wasting. His eyes and skin were yellow. The chest and cardiac examinations were unremarkable, except for a mild increase in the anteroposterior chest diameter and mildly decreased breath sounds. His liver percussed to 11 cm, and a firm, irregular edge was palpable below the right costal margin. No spleen was felt.

Labs:
• Hematocrit 28%• WBC 8200/µL • AST95 U/L ALT110 U/L Alk Phos 550 U/L GGT
800 U/L• Total bilirubin 5.6 mg/dL• Amylase120 U/L Lipase 58 U/L• HBsAg (-), Anti-HBc Total (-) Anti-HCV (-)• UA: pH 7.3, brown, protein (-), glucose (1+),
blood (-) bilirubin (2+) • Micro:No cells, casts, or crystals

Scenario -3• An abdominal sonogram revealed dilated common bile and
hepatic ducts, a dilated gallbladder containing sludge, and multiple masses in the liver. The pancreas was not visualized, due to overlying bowel gas. A computerized tomography scan of the abdomen confirmed the same findings, as well as a 5-cm mass in the head of the pancreas. An endoscopic retrograde cholangiopancreatogram showed a stricture of the common bile duct just above the ampulla of Vater and dilation of the common bile and hepatic ducts proximal to the stricture. A stent was placed across the stricture after brushings of the strictured distal common bile duct were taken, which later revealed malignant cells consistent with carcinoma. Blood for CA 19-9 antigen level was drawn; the result was 800 U/mL. Informed of the results, the patient declined further therapy and was offered palliative care. He expired at home several months later.

Scenario: At autopsy:
• An autopsy revealed an enlarged liver with numerous tan masses of tumor distributed throughout, some with focal areas of necrosis and hemorrhage. Scattered similar tan nodules were noted in the lungs and right adrenal gland. The common bile duct was dilated, and the distal portion showed invasion and near-total narrowing of the lumen by a poorly defined scirrhous mass in the head of the pancreas. The remainder of the pancreas was firm and fibrotic with loss of the normal lobular architecture.

• 1 - Common bile duct, stricture - ERCP image In this case, endoscopic retrograde cholangiopancreatography (ERCP) shows a stricture of the distal common bile duct. Dye passing into the common bile and hepatic ducts proximal to the stricture outlines marked dilation of the ducts, and it also passes into and outlines the main pancreatic duct.
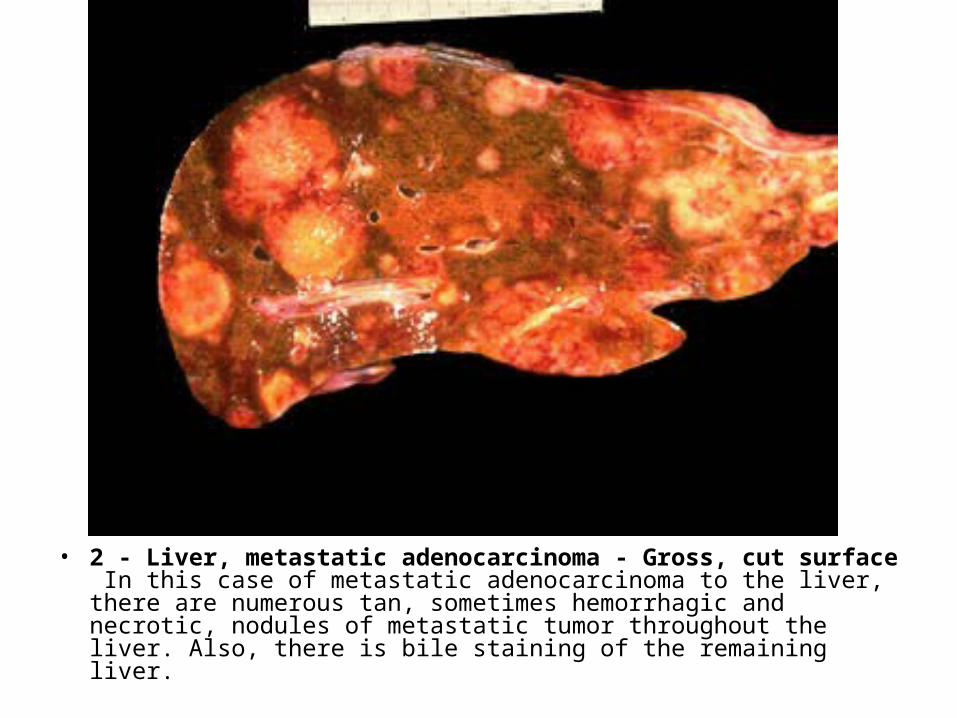
• 2 - Liver, metastatic adenocarcinoma - Gross, cut surface In this case of metastatic adenocarcinoma to the liver, there are numerous tan, sometimes hemorrhagic and necrotic, nodules of metastatic tumor throughout the liver. Also, there is bile staining of the remaining liver.

Question 1:
• By what routes do malignant tumors metastasize to the liver?

• 3 - Liver, metastatic adenocarcinoma - Low power This image shows a malignant, complex glandular nodule surrounded by fibrous tissue and normal hepatic parenchyma. This is the morphologic appearance of metastatic adenocarcinoma to the liver.

• 4 - Liver, metastatic adenocarcinoma - High power At higher magnification, the glandular nature of the metastatic infiltrate is readily apparent. Several of the malignant cells contain cytoplasmic vacuoles of mucin.

Question 2:
• From which organs do mucin-producing adenocarcinomas arise?

• 5 - Pancreas, carcinoma and chronic pancreatitis - Gross, cut surfaces This longitudinal section of the entire pancreas shows a large, gray-white tumor mass of pancreatic adenocarcinoma in the region of the head of the pancreas. The usual lobular architecture of the remainder of the pancreas is totally obscured, due to chronic pancreatitis and extensive fibrous replacement of the normal pancreatic parenchyma.

Question 3:
• Can the location of this tumor be related to the patient's signs, symptoms, and laboratory abnormalities?

Question 4:
• Did this patient have any clinical features of chronic pancreatitis? What are some other complications of chronic pancreatitis?

Question 5:
• Is the presence of pancreatitis and carcinoma in this patient coincidental or etiologically related? What are some of the causes of chronic pancreatitis?

• 6 - Pancreas, adenocarcinoma - High power Pancreatic carcinomas are usually adenocarcinomas. Several irregular malignant glands are present infiltrating desmoplastic fibrotic tissue.
Question 6:
• What are risk factors for developing pancreatic carcinoma?

• 7 - Pancreas, chronic pancreatitis - Low power There is extensive fibrous replacement and chronic inflammation in chronic pancreatitis. Note atrophy of most of the exocrine pancreatic glands and occasional preserved islets.

• 8 - Pancreas, chronic pancreatitis - Gross, cut surface In this case of chronic pancreatitis, note a couple of dilated pancreatic ducts, one of which contains a calculus in the lumen of the duct. Calculi in such cases are formed from inspissated secretions within the ducts.

• 9 - Pancreas, pseudocyst - Gross, cut surface Pancreatic pseudocysts are large cysts filled with pancreatic secretions and sometimes, as in this case, a few dark calculi as well. Pancreatic pseudocysts lack a true epithelial lining. Instead, their wall consists of a rim of fibrous tissue containing chronic inflammatory cells. They occur in the pancreas and are sometimes noted in the soft tissues just adjacent to it.

Question 7:
• What are the causes of pancreatic pseudocysts?