-
Drugs Used in GI Disorders
Drug classification; important or main drugs Important drugs
kinetics and dynamics Important SE & precaution Clinical
used
Kutcharin Phunikhom, MD Department of Pharmacology, Faculty of
Medicine, KKU
Objectives
-
Drugs used in PU /GU/ DU(include GERD)
Antidiarrheal drugs Laxative drugs Drugs used in emesis
Topic outline
-
Peptic Ulcer Disease (PUD)
Acute/chronic of gastric /duodenal ulcer Erosion of GI tract
mucosa Etiologies : -high stress(trauma,burn patients)
-drugs/irritants:NSAIDs -H. pylori -smoking -caffeine
In general
-
Enterochromaffin-like cell, parietal cell, epithelial cell
Acetylcholine, histamine, gastrin, prostaglandin Vagus nerve, post
ganglionic fiber H2-receptor, gastrin receptor, muscarinic
receptor, prostaglandin receptor Adenylate cyclase, proteinkinase,
H+/K+ ATPase HCl, mucus, HCO3-
Review: physiology of gastric secretion
-
HCI secretion by parietal cell
-
Stimulated acid secretion 1.cephalic phase: smell,taste
stimulates the vagus n. 2.gastric phase: -peptides,aa.stimulate the
G cell -stomach distension leads to gastrin release 3.intestinal
phase: aa.induce acid secretion
-
M
M
M
PG
PG
G G
H2 H H
G Blood
Vagus N
Postgang. fiber
PG
+
+
+
+ +
H+ pump H
K
-
Ca
Ca
cAMP
Mucus HCO3
Gastric Lumen
Parietal cell
Epithelial cell
ECL
Short diagram on gastric acid control
-
-Lifestyle changes
-Medications -Surgery
Treatment of PU/GU/DU
-
Classification of drugs used in PU / GU/DU
Acid inhibition Acid neutralization Protection of mucosa
Eradication of Helicobacter pylori Other
-
(I) Acid Inhibition
1) H2-receptor antagonist
Cimetidine, ranitidine, nizatidine, famotidine roxatidine,
lafutidine 80-90 % acid reduction Rapidly absorbed with 1st-pass
effect Excreted mainly in urine Adverse effect: relapse,
gynecomastia (long term use) DI: CYP450 inhibition (warfarin,
diazepam, digoxin,
propranolol, phenytoin, phenobarbital, etc)
-
M
M
M
PG
PG
G G
H2 H H
G Blood
Vagus N
Postgang. fiber
PG
+
+
+
+ +
H+ pump H
K
-
Ca
Ca
cAMP
Mucus HCO3
Gastric Lumen
Parietal cell
Epithelial cell
ECL
Short diagram on gastric acid control
-
2) Proton pump inhibitor Omeprazole, lanzoprazole, rabeprazole,
pantoprazole Rapidly absorbed, active at acidic pH (enteric
coated
capsule) Form irreversible, inactive complex with H+/K+
ATPase 95% plasma protein binding Low adverse effect DI: CYP450
inhibition
-
M
M
M
PG
PG
G G
H2 H H
G Blood
Vagus N
Postgang. fiber
PG
+
+
+
+ +
H+ pump H
K
-
Ca
Ca
cAMP
Mucus HCO3
Gastric Lumen
Parietal cell
Epithelial cell
ECL
Short diagram on gastric acid control
-
3) M-receptor antagonist
Pirenzepine, dicyclomine, telenzepine Low effect on acid
reduction Adverse effect: general M-receptor effects
(atropine-like effects) Low use now
-
M
M
M
PG
PG
G G
H2 H H
G Blood
Vagus N
Postgang. fiber
PG
+
+
+
+ +
H+ pump H
K
-
Ca
Ca
cAMP
Mucus HCO3
Gastric Lumen
Parietal cell
Epithelial cell
ECL
Short diagram on gastric acid control
-
(II) Acid Neutralization
Antacid = anti + acid = alkaline agent Needs no / low absorbed
(action mainly in lumen) Also protect mucosa (surface covering)
Al-salts, Al(OH)3 - not absorbed, slow onset,
constipation, phosphate deficiency Mg-salts, Mg(OH)2 - low
absorbed, rapid onset, diarrhea, Ca-salts, CaCO3 - varied
absorption, rapid onset,
hypercalcemia NaHCO3 - readily absorbed, CO2, systemic
alkalosis
-
(III) Protection of mucosa
Sucralfate
Sucrose octasulfate + poly Al(OH)3 Active at acidic pH,
polymerization (gel) Increase secretion of mucus, HCO3-, PG Protein
denature at ulcer site Increase healing effect Prevent absorption
of other drugs Low SE
-
Carbenoxolone Glycyrrhizic acid
derivative Increase secretion &
viscosity of mucus Inhibit pepsin activity SE: steroidal SE
(Na-
water retention, hypokalemia, hypertension)
Misoprostol PG analogue Increase secretion of
mucus & bicarbonate Inhibit acid secretion Effective for
long term
usage of NSAIDs SE: uterine stimulation
-
(IV) Eradication of H.pylori
Triple therapy:- PPI + clarithromycin + amoxycillin (or
metronidazole)
G- curved rod dyspepsia gastritis duodenal ulcer painful
stomach
Helicobacter pylori
-
Other dugs Cimethicone Motilium Magesto M.carminative
Cisapride
-
PUD complications Hemorrhage Perforation Obstruction Cancer
4-8 weeks Avoid special food: coca cola, chilly Stress
control
PU / GU/DU treatment
-
Antidiarrheal Drugs
Used when necessary Routine diarrheal treatment : Rehydration
->
antimicrobial agents -> Antidiarrheal agents (antispasmodic /
antimotility agents)
Classification : Opioids & others Opioids - opium tincture,
diphenoxylate, loperamide Others - Bismuth subsalicylate,
octreotide, adsorbent,
astringent
-
(I) Opioids Agonist at opioid receptors of GI muscle Reduce
muscle movement, but increase tone of
contraction of rectal sphincter Reduce fluid & electrolyte
secretion in GI Fast action Cause addiction (long term usage)
Careful usage in children Lomeramide (ImodiumR), diphenoxylate
(LomotilR) -
potency > opium tr.
-
(II) Other antidiarrheal
Bismuth subsalicylate: inhibit PG secretion -> inhibit
diarrhea
Octreotide: somatostatin receptor binding -> inhibit GI fluid
secretion
Adsorbent - charcoal, kaolin, chalk: trap toxin, substance into
their suface
Astringent - tea leaves: precipitate surface protein ->
reduce diarrhea
Atropine: M-receptor SE
-
Laxatives Drugs
Foods (mainly plant-based foods Bulk laxative Hydrating agents
Stimulant laxative Surfactant laxative Others
Laxative - Purgative - Cathartic
Mostly need water
-
(I) Foods Laxative
Plant-based foods Almonds, Aloe Vera, Apples, Bananas,
Blueberry,
Coconut, Coffee, Grapes, Mangos, Oranges, Papayas Preventing
constipation than treating it.
-
(II) Bulk Laxative
Dietary fiber (natural cellulose), polysaccharide, psyllium seed
(MetamucilR), Lemon basil ()
Bind to water ---> increase bulk (mass) ---> stimulate
local reflex in colon
Needs water (retain more water) Not absorbed in GI Reduces
absorption of other drugs Quite safe (except GI obstruction) Takes
days for action (12-72 hrs.)
-
(III) Hydrating agents (osmotics)
Hyperosmotic agents Sorbitol, glycerin, lactulose drawing water
into the bowel SE- withdraw water &
electrolytes into colon lumen Poorly absorbed in GI Fast action
(30 min. to 3 hrs.)
Saline laxatives Magnesium salts - Mg(OH)2,
MgSO4, sodium phosphate, sodium biphosphate
Attract and retain water in the hollow of the intestinestool
softening .increase intraluminal pressure
Poorly absorbed in GI SE- withdraw water & electrolytes
into colon lumen Fast action (30 min. to 6 hrs.)
-
(IV) Stimulant Laxative (irritants)
Diphenylmethane derivatives - bisacodyl (DulcolaxR),
phenolphthalein
Anthraquinone glycosides - senna, aloe, etc Stimulate local
reflex in colon Poorly absorbed Medium action (6-8 hr) Suppository
(1-2 hr) SE: abdominal cramp, phenolphthalein ->liver toxic
(not
in use now)
-
(V) Surfactant Laxative (stool-softeners)
Docusate, castor oil Wetting & softening agent - increase
water
permeability (fats & water to penetrate the stool) Needs
water for effect Slow action (1-3 days) Castor oil also increase
peristalsis -> fast action (1-3
hr) --> bowel evacuation before operation SE: abdominal
cramp, electrolyte imbalance (castor
oil)
-
(VI) Other Laxatives
Mineral oil - non absorbed, work as lubricant, slow action (6-8
hrs.), SE: interfere oil-soluble vitamin absorption, oil
leakage
Laxative Abuse: Weight control - loss of fluid &
electrolytes, interfere normal habit
-
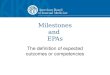
Controlling System for Emesis Vomiting
Center Sensory Aff.
CNS Pways
CTZ mood
Special sensation
Labyrinth
Motion sickness
Solitary tract nuclei
Endotoxin Drugs
Local Irritants in GI by chemical, bacteria,
virus and cytotoxic drugs
radiation
Emetic & Antiemetic Drugs
-
Stimulate vomiting center in medulla or outside (CTZ, GI)
Ipecac is used as an antidote for toxic substant ingestion
(GI)
Apomorphine (CTZ) & CuSO4 (GI) are mainly used in experiment
but not for medicated purpose
Emetic Drugs
-
Antiemetic Drugs
Block vomiting center or pathways outside medulla Mainly used in
motion sickness, pregnancy (morning
sickness), chemotherapy, food poisoning, radiation &
post-operation
Antiemesis: D2 antagonist, 5-HT antagonist, H1 antagonist, M
antagonist & miscellaneous
-
dimenhydrinate (DramamineR), diphenhydramine (BenadrylR) ->
Motion sickness
SE: Antihistamine SE
H1antagonist
M- antagonist promethazine (PhenerganR), scopolamine
(ScopodermR) -
> Motion sickness (caused by labyrynth) SE: similar to
Antihistamine SE
-
D2 antagonist Chlorpromazine (ChlorpromedR), domperidone
(MotiliumR) -> Local irritants, cytotoxic drugs, radiation
SE: BP drop , dizziness, abnormal movement in
extrapyramidal system
Ondansetron (ZofranR) -> cytotoxic drugs SE: headache,
dizziness
5HT- antagonist
-
Prokinetics Metoclopramide (PlasilR), -> general vomiting
and
morning sickness (careful use) SE: depression, dizziness,
abnormal movement in
extrapyramidal system domperidone (MotiliumR)
Dronabinol (MarinolR) -> block CTZ SE: dizziness, dry mouth,
hallucination
Misc. The end