Embed Size (px)
Citation preview

Lemone and Burke Chapters 21 - 26
GI - A & P Review� Mouth
� Pharynx
� Esophagus
� Stomach
� Small Intestines
� Large Intestines
� Liver and Gallbladder
� Pancreas
Peptic Ulcer Disease (PUD)�Objectives:� Identify different types
� Gastric Ulcer
� Duodenal Ulcer
� Stress Ulcer
� Etiology and pathophysiology
� Clinical manifestation
� Collaborative management
� Nursing diagnosis
PUD
� Breakdown mucous lining in GI tract
� Duodenal ulcers
� Gastric ulcers
PUD Etiology and Patho� Pathophysiology
� Gastric mucosa protects epithelium
� Bicarbonates
� Adequate blood supply
� Risk factors
� H. pylori infections, NSAID, Age,
� Hx of ulcers, family hx of ulcers
PUD Manifestation� Pain
� Gnawing, burning, aching
� Epigastric region – radiates to back
� Dyspepsia
� Weight loss
� Anemia

PUD Complications� Hemorrhage
� Hematemesis, blood in stool
� Fatigue, weakness, dizziness
� Orthostatic hypotension
� Hypovolemic shock
� Narrowing and obstruction (pyloric)� Epigastric fullness
� N/V - Electrolyte imbalance, metabolic alkalosis
� Perforation� Severe pain
� Rigid abdomen
� No bowel sounds
� Peritonitis
PUD Diagnosis� UGI
� EGD
� Visualize erosion
� Take biopsies
� UGI series
� Lab tests
� IgG
� Urea breath test
� Fecal test
PUD - Collaborative Management� H & P
� Medication
� PPI
� H2 receptor blocker
� Antacids
� Antibiotics
� Nutrition
� Surgery
� Tx of complications
PUD surgeries
� Pyloriplasty Billroth I
PUD – Nursing Diagnosis� Pain
� Disturbed sleep pattern
� Imbalanced nutrition < body requirement
� Fluid volume deficit
Hernias�Objectives:� Identify different types
� Hiatal
� Umbilical
� Femoral
� Ventral/incisional
� Direct/indirect inguinal
� Identify etiology and pathophysiology, clinical manifestation, and complications
� Discuss collaborative management
� Discuss nursing diagnosis and interventions

Hiatal Hernia� Stomach protrudes
through esophageal hiatus into thoracic cavity
� Usually asymptomatic
� Incidence increased w age
Sliding Hiatal Hernia� Gastroesophageal
junction and fundus of stomach slide upward into esophageal hiatus
� Symptoms:
� Dysphagia
� Chest pain
� Heartburn
� Belching
� Regurgitation
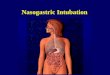
Paraesophageal Hiatal Hernia
� Fundus and possibly portions of the stomach’s greater curvature, rolls through the esophageal hiatus and into the thorax beside the esophagus
A Comparison of the normal stomach, sliding hiatal
hernia and rolling hiatal hernia
Hiatal Hernia - Diagnosis� Barium Swallow
� CXR
� Endoscopy with biopsy
� CBC
� Stool for guaiac
Hiatal Hernia - Medical Treatment� Goals
� Aimed at relieving symptoms and prevent complications
� Bleeding
� Reduce regurgitation of stomach contents into esophagus
� Medications
� Includes antacids and histamine receptor antagonists (Pepcid and Reglan)
� Neutralizes stomach acidity
� Decrease acid production

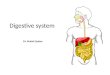
� Indirect inguinal
� Direct inguinal
� Femoral
� Umbilical
� Incisional
Types of Abdominal Hernias� Peritoneal sac w intestine or
omentum pushes down into inguinal canal
� Affect males
� May descend into the scrotum
� S/S: pain with straining
� Soft swelling increases w intra-abdominal pressure, may decrease when lying down
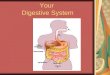
Indirect Inguinal Hernia
� In contrast, this type of hernia passes through a weak point in the abdominal wall
� Rarely enters the scrotum
� Most common in men older than 40; rare in women
� S/S: usually painless, round swelling close to pubis, which is easily reduced when supine
Direct Inguinal Hernia� Protrusion of bowel into
umbilical ring
� Most common in women
� Congenital� Infancy
� Acquired� Obesity
� Multiple pregnancies
� Ascities
� Large tumors
Umbilical Hernia
Incisional or ventral Hernias� Occur at previous surgical incision
� Results from inadequate healing of incision
� Bulge at incision
� Risk of incarceration is low
� Contributing factors:
� Poor wound closure
� Age
� Obesity
� Poor nutrition
� Protrude through the femoral ring
� More common on right side
� More common in women than men
� S/S: lump in groin; severe pain, may become strangulated
Femoral Hernia

Types of Hernias Hernia –
Collaborative Management
� Diagnosis
� H & P
� Surgical repair
� herniorrhaphy
� Nursing interventions
� H & P
� Teaching
� Post-op care
Hernia – Nursing Diagnosis� Risk of ineffective tissue perfusion - gastrointestinal
� Pain
� Knowledge deficit
Gallbladder Disorders�Objectives:� Identify etiology, pathophysiology, and clinical
manifestations of:
� Cholelithiasis
� Cholecystitis
� Discuss nursing care and interventions of these diseases
Function on Biliary System� Create, store, transport,
and release bile into the duodenum to aid in digestion
� Liver,
� Gallbladder,
� Bile ducts
Cholelithiasis� Most common problem within biliary duct
system
� Risk factors:
� Age
� Family history
� Race/ethnicity
� Obesity/hyperlipidemia
� Rapid weight loss
� Female
� Biliary stasis

Cholelithiasis - patho� Gallstones
� Abnormal bile composition
� Biliary stasis
� Increased cholesterol
� inflammation
� Manifestation
� Mild distress
� Biliary colic w obstruction
Cholecystitis� Acute or chronic disorder resulting in distention and
inflammation of gallbladder
� Most often in association with cholelithiasis (gallstones) obstructing the cystic duct
� Obstruction can lead to ischemia of gallbladder wall and mucosa
� Can lead to necrosis
� Pain
� RUQ, may radiate to back and right shoulder
� Chronic disorder results from repeated bouts of acute disease
Cholecystitis - Diagnosis� Serum alkaline phosphatase
� CBC
� Serum bilirubin
� Serum lipase and amylase if pancreas involved
� Ultrasound of right upper quadrant
� Abdominal x-ray
� HIDA SCAN
Cholecystitis – Nursing Care� H & P
� Diagnostic tests
� Pain management
� Teaching
� Nutrition
Cholecystitis - Interventions� Non surgical management
�Asymptomatic, manage conservatively
�Low fat diet
�Medication – ursodiol or chenodiol
�Acute pain - gallstones obstruct cystic or common bile duct
�Opioid analgesia (Demerol, as morphine can cause biliary spasm)
�Anti-emetics to control nausea and vomiting
�Anti-spasmodics to relax smooth muscle (Bentyl, Lomine)
�NPO, IV fluids, IV ANTIBIOTICS
�No surgery until acute infection is resolved
Cholecytitis –
Surgical Management� Laparoscopic
cholecystectomy: � Minimally invasive
� Usually home within 24 hours
� Most common complication
� Injury to bile duct
� “Free air pain” from carbon dioxide retention
� May settle on phrenic nerve and cause shoulder pain

Cholecystitis – surgical
Management (cont)
� Traditional cholecystectoy
� Removes gallbladder and stones
� 4-6 inch incision made into the abdomen
� Usually home in 1-3 days
� Back to work in 4-6 weeks
� May have t-tube placed for drainage of bile
� (If common bile duct is explored)
Cholecystectomy
Cholecystectomy:
Pre-op Nursing Diagnosis
� Alteration in bowel elimination
� Alteration in comfort
� Alteration in nutrition
� Fluid volume deficit
� Self-care deficit
� Risk for injury
� Acute pain
Cholecystectomy
Pre-op nursing interventions� Patient teaching
� Make sure there is order for consent and it is signed by patient or family (informed)
� Make patient comfortable
� Hydration
� NPO
� Lab work done and in chart
� Pre-op check list completed
Post-op nursing interventions
� Prevent pulmonary complications: CTDB, I/S� Prevent pain, PCA � Care for the incision, surgical drain � NPO - clear liquids - advances to regular as
tolerated� Monitor bowel sounds, watch for post-op ileus� Monitor urinary output� Prevent DVT’s, early ambulation is best
Cholecystectomy :
Post-op Nursing Diagnosis
� Acute pain
� Knowledge deficit
� Activity intolerance
� Ineffective breathing pattern
� Risk for infection
� Risk for injury
� Alteration in nutrition

Case Studies� 35 y/o nursing student, working PT, heart burn for
years and takes Prilosec for after dx – dudenal ulcer. Now weak, lightheaded, pale admitted for r/o UGIB
Case Studies� Juanita, 49 y/o married mother with 3 children, native
of Yucatan region of Mexico works as a checker at a local supermarket.
� Recently she started to notice a dull pain over her upper abdomen after meals – especially on Sundays when all her children come to visit with their families