Embed Size (px)
Citation preview
5/2/2017
1
Get Ready :Motility
speedyeyes.com
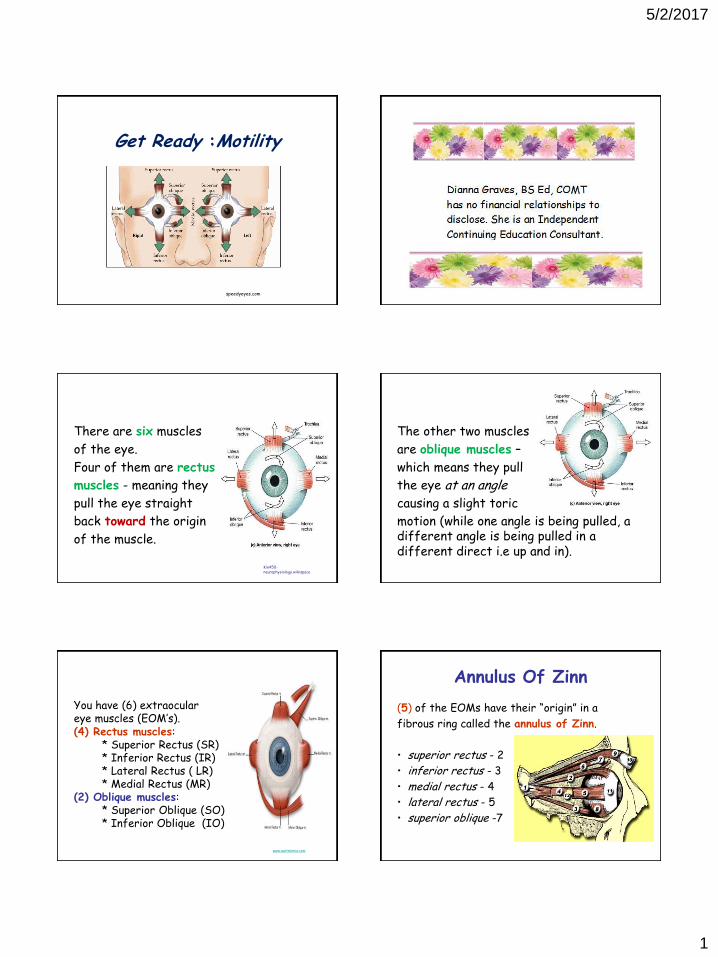
There are six muscles
of the eye.
Four of them are rectus
muscles - meaning they
pull the eye straight
back toward the origin
of the muscle.
Kin450-neurophysiology.wikispace
The other two muscles
are oblique muscles –
which means they pull
the eye at an angle
causing a slight toric
motion (while one angle is being pulled, a different angle is being pulled in a different direct i.e up and in).
You have (6) extraocular eye muscles (EOM’s). (4) Rectus muscles: * Superior Rectus (SR) * Inferior Rectus (IR) * Lateral Rectus ( LR) * Medial Rectus (MR) (2) Oblique muscles: * Superior Oblique (SO) * Inferior Oblique (IO)
www.auntminnie.com
(5) of the EOMs have their “origin” in a
fibrous ring called the annulus of Zinn.
• superior rectus - 2
• inferior rectus - 3
• medial rectus - 4
• lateral rectus - 5
• superior oblique -7
Annulus Of Zinn
5/2/2017
2
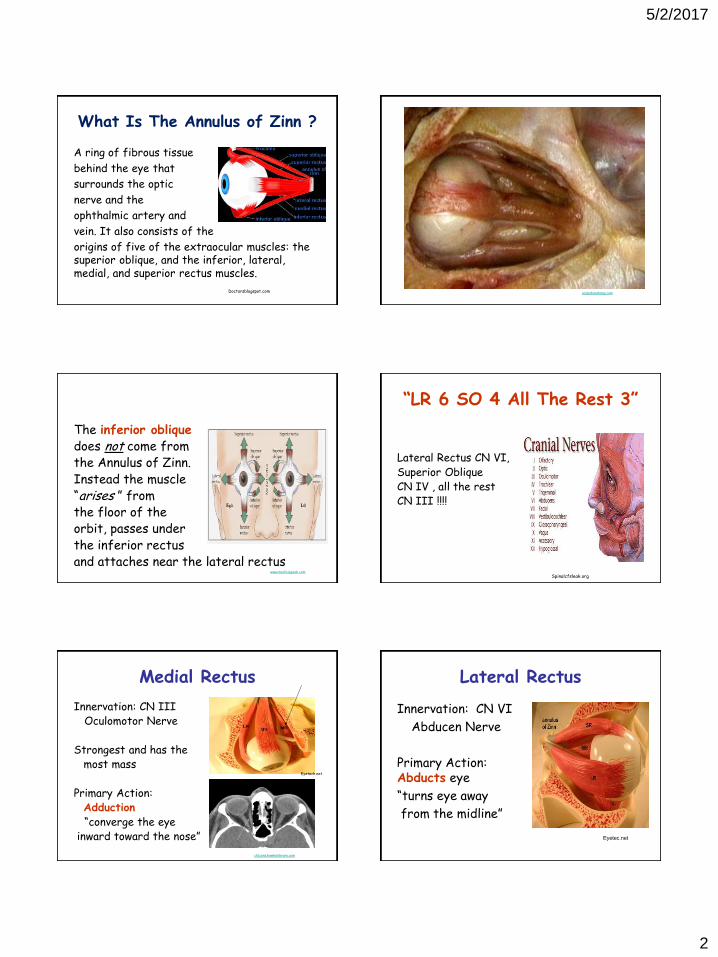
What Is The Annulus of Zinn ?
A ring of fibrous tissue
behind the eye that
surrounds the optic
nerve and the
ophthalmic artery and
vein. It also consists of the
origins of five of the extraocular muscles: the superior oblique, and the inferior, lateral, medial, and superior rectus muscles.
Doctorsblogspot.com aclandanatomy.com
The inferior oblique does not come from the Annulus of Zinn. Instead the muscle “arises ” from the floor of the orbit, passes under the inferior rectus and attaches near the lateral rectus
www.medicalgeek.com
“LR 6 SO 4 All The Rest 3”
Lateral Rectus CN VI, Superior Oblique CN IV , all the rest CN III !!!!
Spinalcfsleak.org
Medial Rectus
Innervation: CN III Oculomotor Nerve Strongest and has the most mass
Primary Action: Adduction “converge the eye inward toward the nose”
Eyetech.net
ctscans.hawkelibrary.com
Lateral Rectus
Innervation: CN VI
Abducen Nerve
Primary Action: Abducts eye
“turns eye away
from the midline”
Eyetec.net
5/2/2017
3
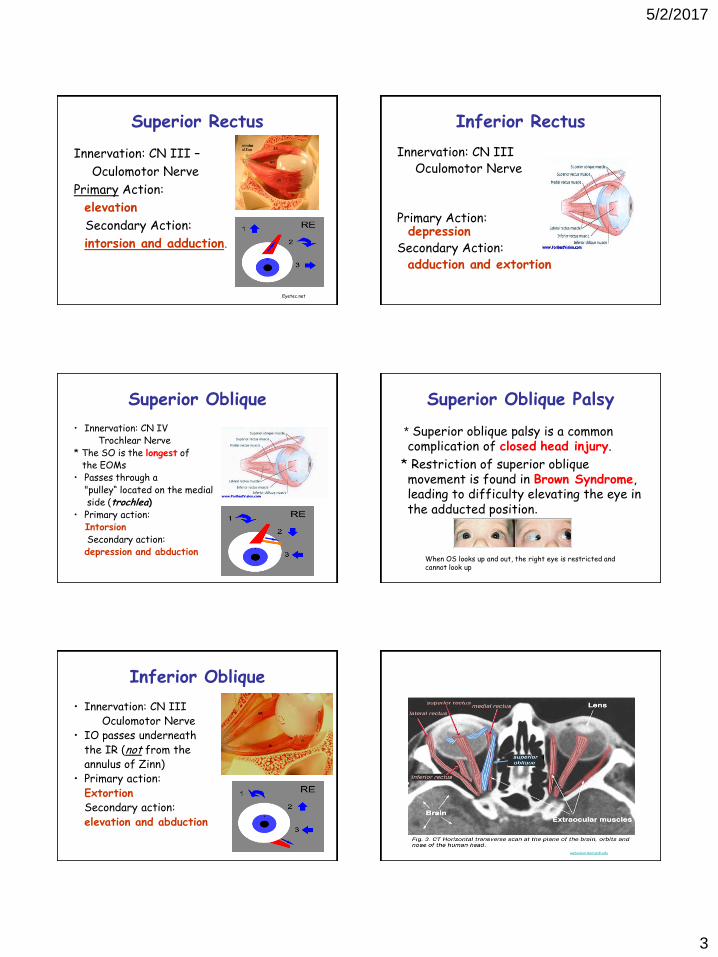
Superior Rectus
Innervation: CN III –
Oculomotor Nerve
Primary Action:
elevation
Secondary Action:
intorsion and adduction.
Eyetec.net
Inferior Rectus
Innervation: CN III Oculomotor Nerve Primary Action: depression Secondary Action: adduction and extortion
Superior Oblique
• Innervation: CN IV Trochlear Nerve * The SO is the longest of the EOMs • Passes through a "pulley“ located on the medial side (trochlea) • Primary action: Intorsion Secondary action: depression and abduction
Superior Oblique Palsy
* Superior oblique palsy is a common complication of closed head injury.
* Restriction of superior oblique movement is found in Brown Syndrome, leading to difficulty elevating the eye in the adducted position.
When OS looks up and out, the right eye is restricted and cannot look up
Inferior Oblique
• Innervation: CN III Oculomotor Nerve • IO passes underneath the IR (not from the annulus of Zinn) • Primary action: Extortion Secondary action: elevation and abduction
webvision.med.utah.edu
5/2/2017
4
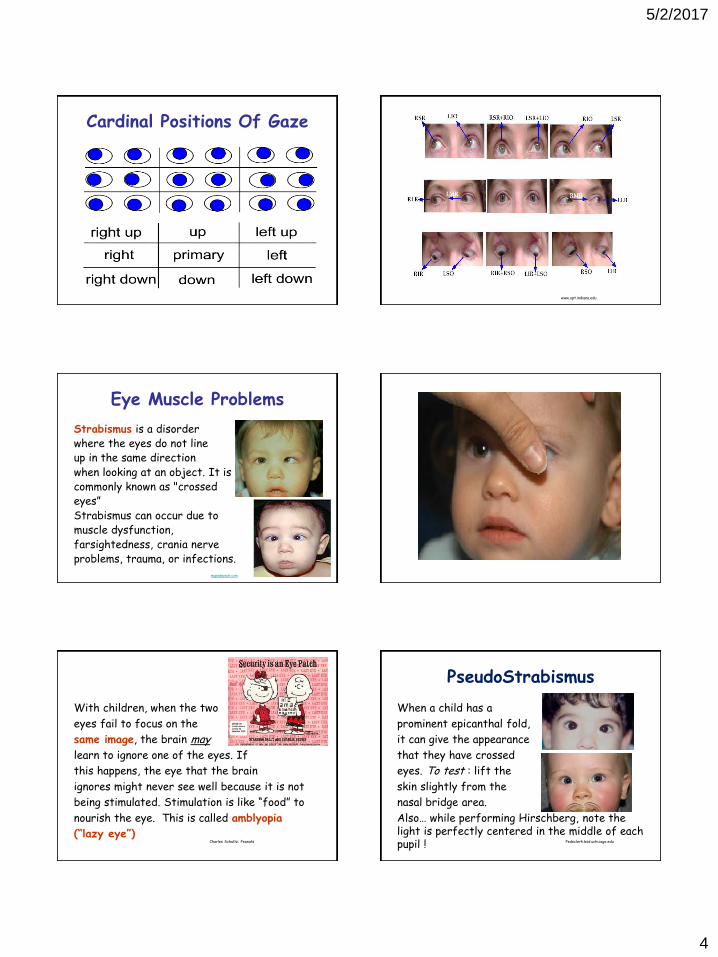
Cardinal Positions Of Gaze
www.opt.indiana.edu
Eye Muscle Problems
Strabismus is a disorder where the eyes do not line up in the same direction when looking at an object. It is commonly known as "crossed eyes” Strabismus can occur due to muscle dysfunction, farsightedness, crania nerve problems, trauma, or infections.
mypedeyedr.com
With children, when the two
eyes fail to focus on the
same image, the brain may
learn to ignore one of the eyes. If
this happens, the eye that the brain
ignores might never see well because it is not
being stimulated. Stimulation is like “food” to
nourish the eye. This is called amblyopia
(“lazy eye”) Charles Schultz: Peanuts
PseudoStrabismus
When a child has a
prominent epicanthal fold,
it can give the appearance
that they have crossed
eyes. To test : lift the
skin slightly from the
nasal bridge area.
Also… while performing Hirschberg, note the light is perfectly centered in the middle of each pupil ! Pedsclerk.bsd.uchicago.edu
5/2/2017
5
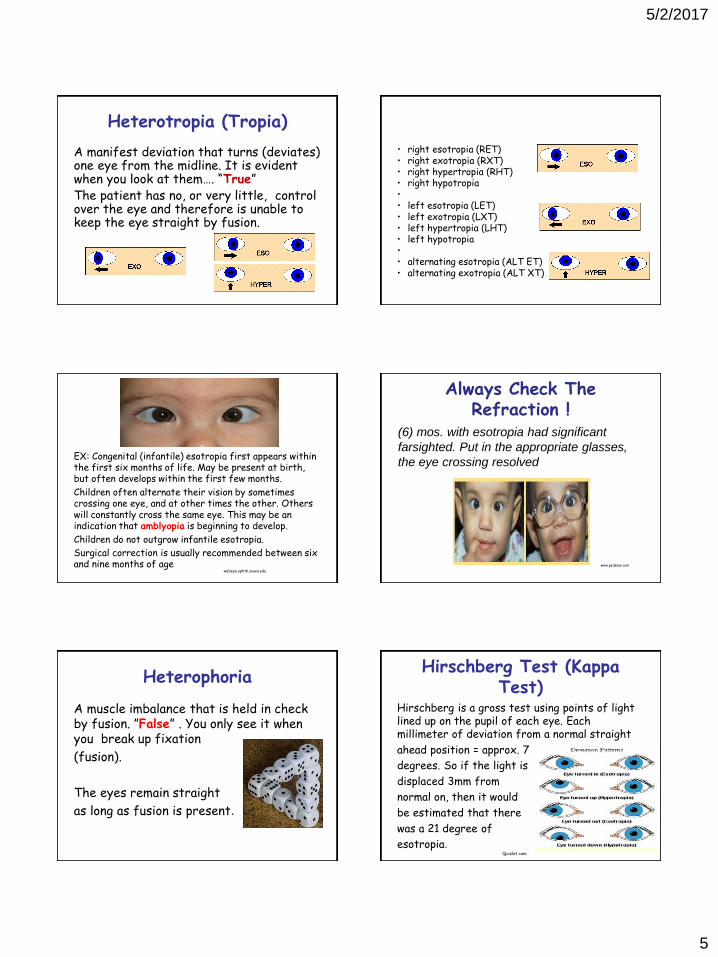
Heterotropia (Tropia)
A manifest deviation that turns (deviates) one eye from the midline. It is evident when you look at them…. “True” The patient has no, or very little, control over the eye and therefore is unable to keep the eye straight by fusion.
• right esotropia (RET) • right exotropia (RXT) • right hypertropia (RHT) • right hypotropia • • left esotropia (LET) • left exotropia (LXT) • left hypertropia (LHT) • left hypotropia • • alternating esotropia (ALT ET) • alternating exotropia (ALT XT)
EX: Congenital (infantile) esotropia first appears within the first six months of life. May be present at birth, but often develops within the first few months.
Children often alternate their vision by sometimes crossing one eye, and at other times the other. Others will constantly cross the same eye. This may be an indication that amblyopia is beginning to develop.
Children do not outgrow infantile esotropia.
Surgical correction is usually recommended between six and nine months of age
webeye.ophth.uiowa.edu
Always Check The Refraction !
(6) mos. with esotropia had significant
farsighted. Put in the appropriate glasses,
the eye crossing resolved
www.pedseye.com
Heterophoria
A muscle imbalance that is held in check by fusion. ”False” . You only see it when you break up fixation
(fusion).
The eyes remain straight
as long as fusion is present.
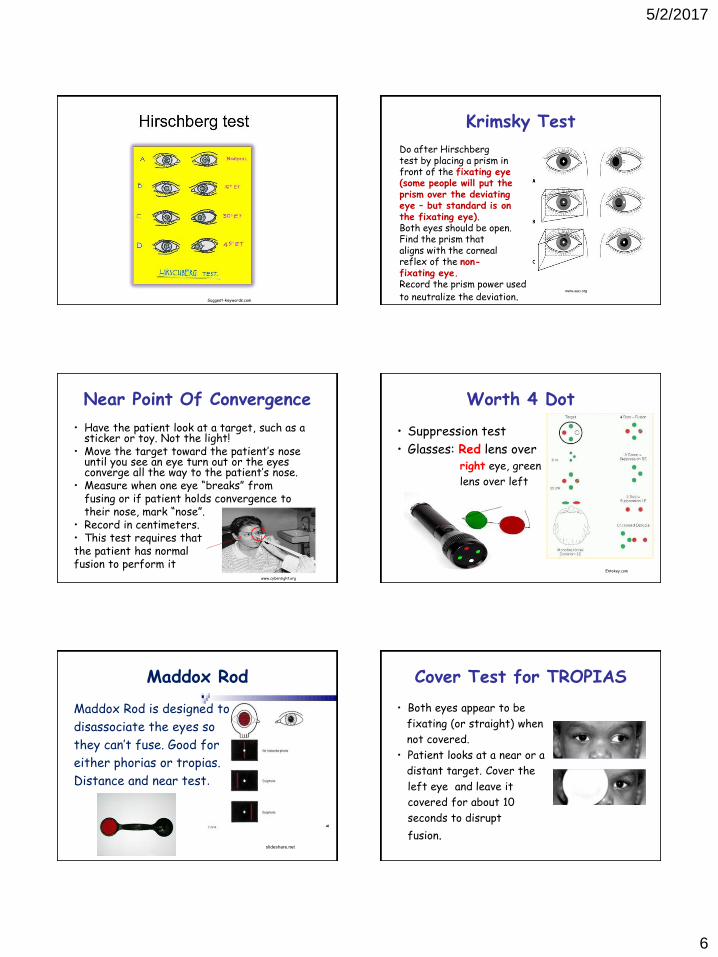
Hirschberg Test (Kappa Test)
Hirschberg is a gross test using points of light lined up on the pupil of each eye. Each millimeter of deviation from a normal straight
ahead position = approx. 7
degrees. So if the light is
displaced 3mm from
normal on, then it would
be estimated that there
was a 21 degree of
esotropia. Quizlet.com
5/2/2017
6
Suggest-keywords.com
Krimsky Test
Do after Hirschberg test by placing a prism in front of the fixating eye (some people will put the prism over the deviating eye – but standard is on the fixating eye). Both eyes should be open. Find the prism that aligns with the corneal reflex of the non- fixating eye. Record the prism power used to neutralize the deviation.
www.aao.org
Near Point Of Convergence
• Have the patient look at a target, such as a sticker or toy. Not the light!
• Move the target toward the patient’s nose until you see an eye turn out or the eyes converge all the way to the patient’s nose.
• Measure when one eye “breaks” from fusing or if patient holds convergence to their nose, mark “nose”. • Record in centimeters. • This test requires that the patient has normal fusion to perform it
www.cybersight.org
Worth 4 Dot
• Suppression test
• Glasses: Red lens over right eye, green
lens over left
Entokey.com
Maddox Rod
Maddox Rod is designed to
disassociate the eyes so
they can’t fuse. Good for
either phorias or tropias.
Distance and near test.
slideshare.net
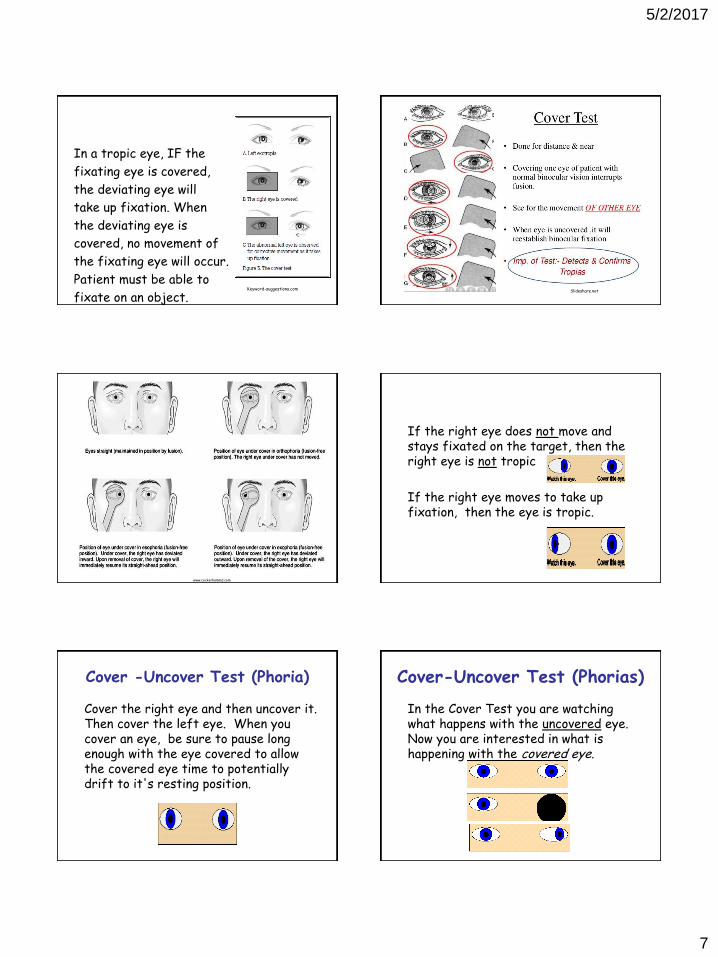
Cover Test for TROPIAS
• Both eyes appear to be
fixating (or straight) when
not covered.
• Patient looks at a near or a
distant target. Cover the
left eye and leave it
covered for about 10
seconds to disrupt
fusion.
5/2/2017
7
In a tropic eye, IF the
fixating eye is covered,
the deviating eye will
take up fixation. When
the deviating eye is
covered, no movement of
the fixating eye will occur.
Patient must be able to
fixate on an object. Keyword-suggestions.com Slideshare.net
www.cockerhammd.com
If the right eye does not move and stays fixated on the target, then the right eye is not tropic
If the right eye moves to take up fixation, then the eye is tropic.
Cover -Uncover Test (Phoria)
Cover the right eye and then uncover it. Then cover the left eye. When you cover an eye, be sure to pause long enough with the eye covered to allow the covered eye time to potentially drift to it's resting position.
Cover-Uncover Test (Phorias)
In the Cover Test you are watching what happens with the uncovered eye. Now you are interested in what is happening with the covered eye.
5/2/2017
8
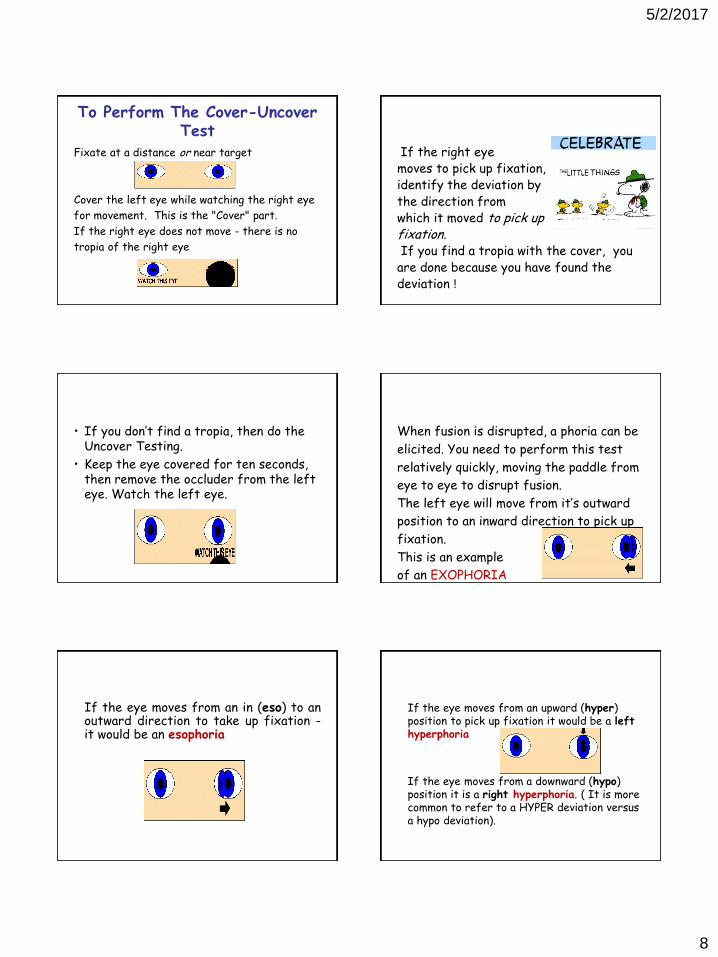
To Perform The Cover-Uncover Test
Fixate at a distance or near target
Cover the left eye while watching the right eye
for movement. This is the "Cover" part.
If the right eye does not move - there is no
tropia of the right eye
If the right eye moves to pick up fixation, identify the deviation by the direction from which it moved to pick up fixation. If you find a tropia with the cover, you are done because you have found the deviation !
• If you don’t find a tropia, then do the Uncover Testing.
• Keep the eye covered for ten seconds, then remove the occluder from the left eye. Watch the left eye.
When fusion is disrupted, a phoria can be
elicited. You need to perform this test
relatively quickly, moving the paddle from
eye to eye to disrupt fusion.
The left eye will move from it’s outward
position to an inward direction to pick up
fixation.
This is an example
of an EXOPHORIA
If the eye moves from an in (eso) to an outward direction to take up fixation - it would be an esophoria
If the eye moves from an upward (hyper) position to pick up fixation it would be a left hyperphoria
If the eye moves from a downward (hypo) position it is a right hyperphoria. ( It is more common to refer to a HYPER deviation versus a hypo deviation).
5/2/2017
9
What’s the Difference ?
The Cover Test tests for a tropia
The Cover-Uncover Test tests for a phoria
Stereopsis
Each eye captures a separate image then sends the two separate images to the brain. The two images arrive together and are combined into a single image. The mind combines the two images by matching the similarities and adding in the small differences that are missing. The combined image is a three dimensional stereo picture.
www.strabismus.org
vision3D.com
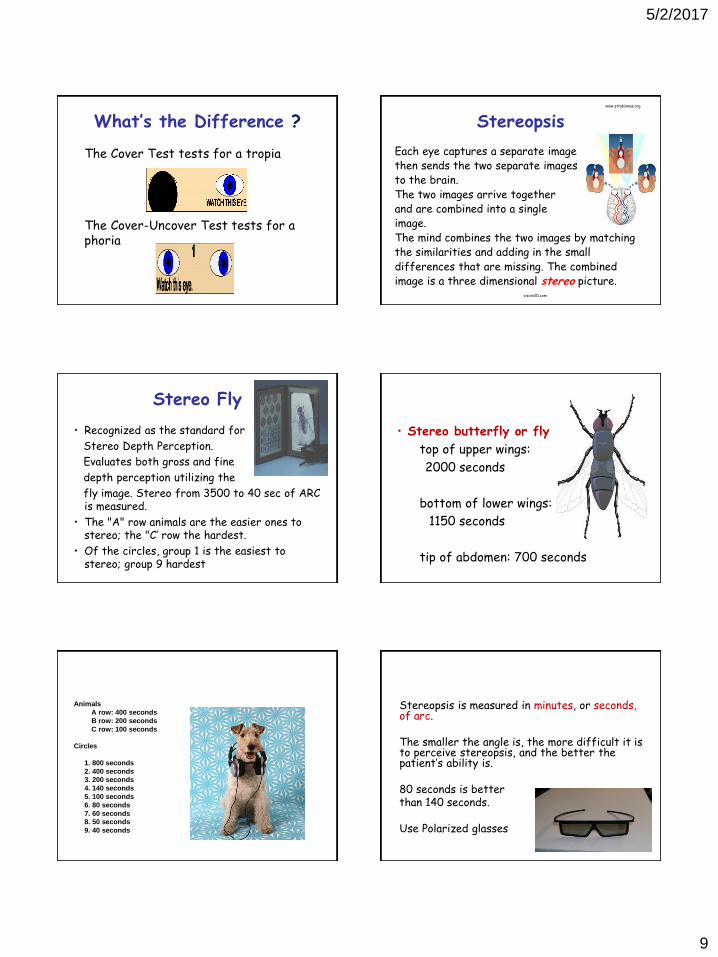
Stereo Fly
• Recognized as the standard for
Stereo Depth Perception.
Evaluates both gross and fine
depth perception utilizing the
fly image. Stereo from 3500 to 40 sec of ARC is measured.
• The "A" row animals are the easier ones to stereo; the "C’ row the hardest.
• Of the circles, group 1 is the easiest to stereo; group 9 hardest
• Stereo butterfly or fly
top of upper wings:
2000 seconds
bottom of lower wings:
1150 seconds
tip of abdomen: 700 seconds
Animals
A row: 400 seconds
B row: 200 seconds
C row: 100 seconds
Circles
1. 800 seconds
2. 400 seconds
3. 200 seconds
4. 140 seconds
5. 100 seconds
6. 80 seconds
7. 60 seconds
8. 50 seconds
9. 40 seconds
Stereopsis is measured in minutes, or seconds, of arc. The smaller the angle is, the more difficult it is to perceive stereopsis, and the better the patient’s ability is. 80 seconds is better than 140 seconds. Use Polarized glasses
5/2/2017
10
• dgh