Embed Size (px)
Citation preview
05/21/2015
1
PreoperativeAssessmentoftheGeriatricPatient
KelseyWalker,MD
GeriatricGrandRounds
May21,2015
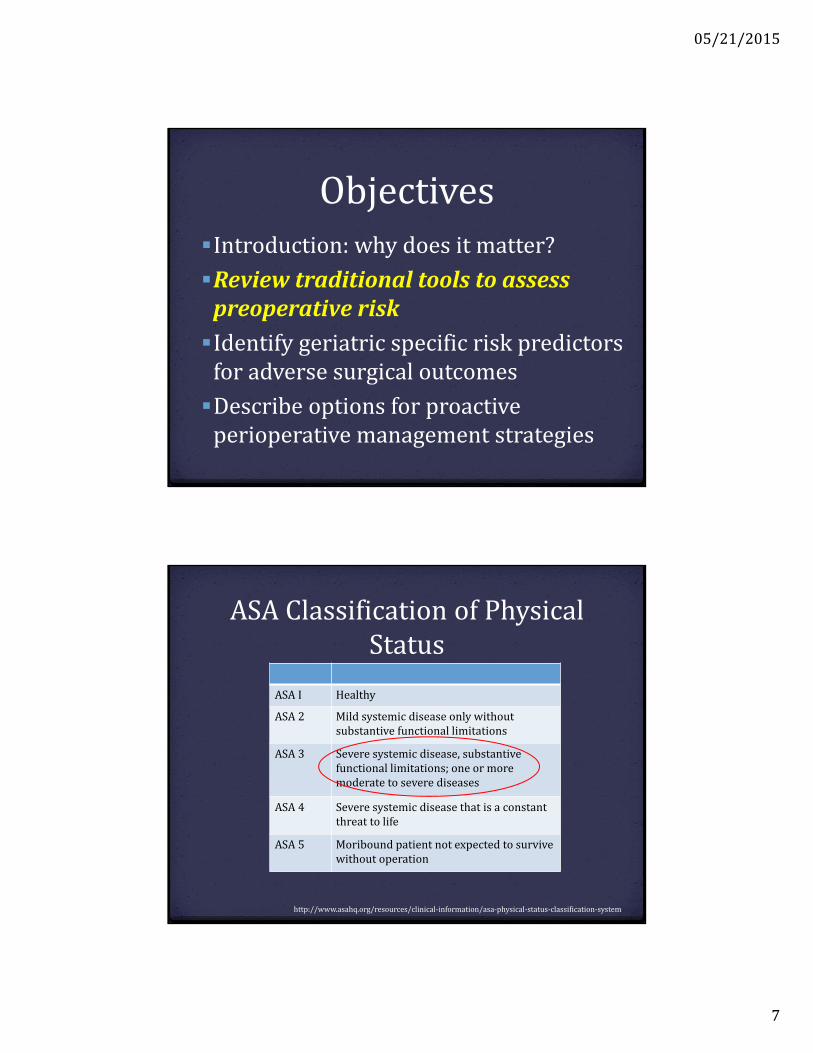
ObjectivesIntroduction:whydoesitmatter?
Reviewtraditionaltoolstoassesspreoperativerisk:valueandlimitations
Identifygeriatricspecificriskpredictorsforadversesurgicaloutcomes
Describeoptionsforproactiveperioperativemanagementstrategies
05/21/2015
2
ObjectivesIntroduction:whydoesitmatter?Reviewtraditionaltoolstoassesspreoperativerisk:valueandlimitations
Identifygeriatricspecificriskpredictorsforadversesurgicaloutcomes
Describeoptionsforproactiveperioperativemanagementstrategies
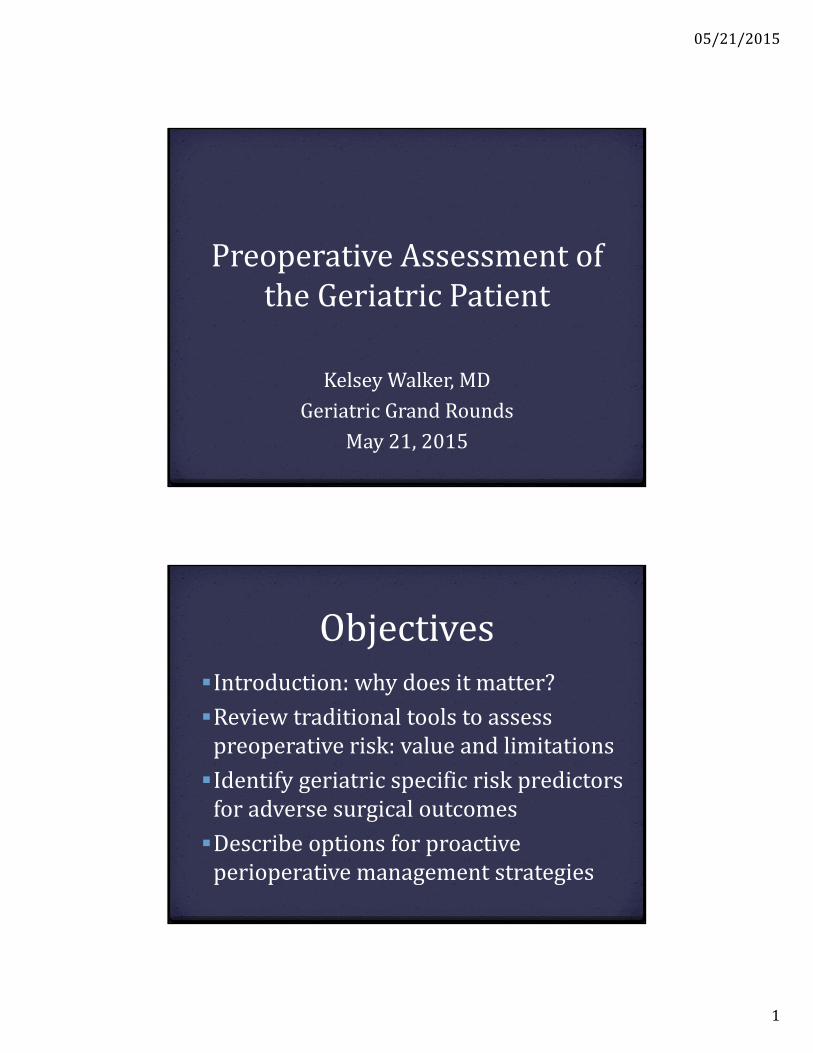
Whydoesitmatter?
2010USCensus
05/21/2015
3
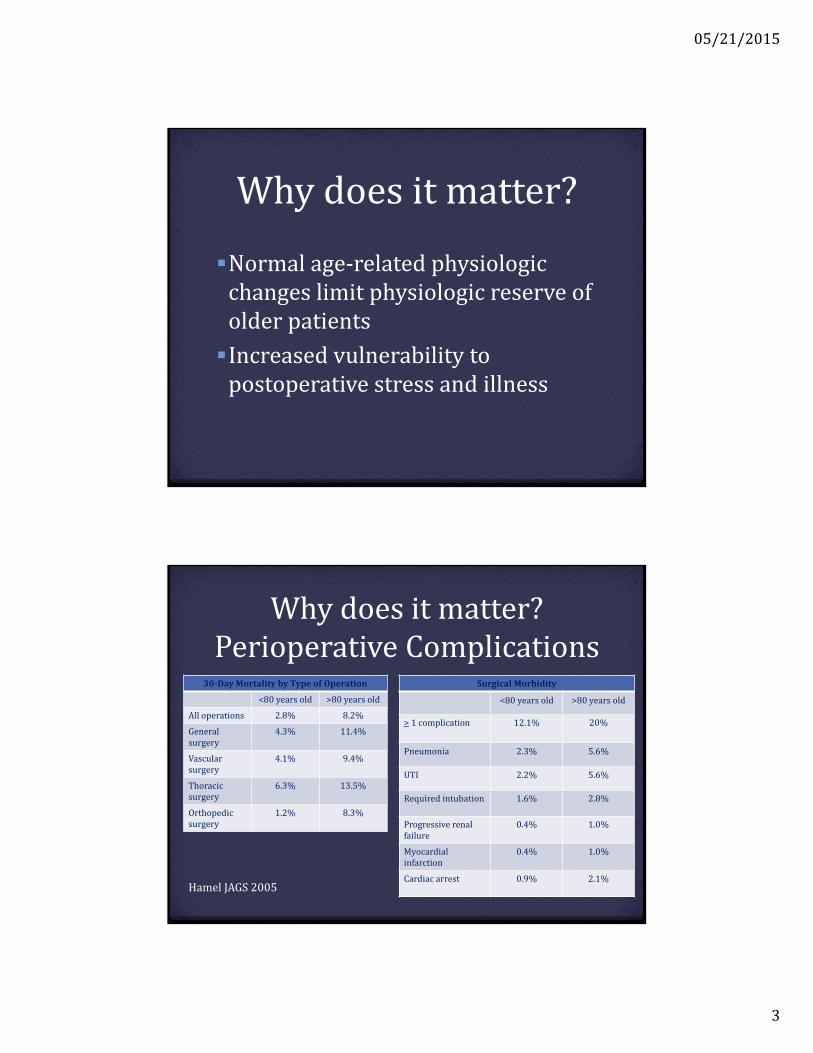
Whydoesitmatter?
Normalage‐relatedphysiologicchangeslimitphysiologicreserveofolderpatients
Increasedvulnerabilitytopostoperativestressandillness
Whydoesitmatter?PerioperativeComplications
30‐DayMortalitybyTypeofOperation
<80 yearsold >80yearsold
Alloperations 2.8% 8.2%
Generalsurgery
4.3% 11.4%
Vascularsurgery
4.1% 9.4%
Thoracicsurgery
6.3% 13.5%
Orthopedicsurgery
1.2% 8.3%
SurgicalMorbidity
<80 yearsold >80yearsold
> 1complication 12.1% 20%
Pneumonia 2.3% 5.6%
UTI 2.2% 5.6%
Required intubation 1.6% 2.8%
Progressiverenalfailure
0.4% 1.0%
Myocardialinfarction
0.4% 1.0%
Cardiacarrest 0.9% 2.1%HamelJAGS2005
05/21/2015
4
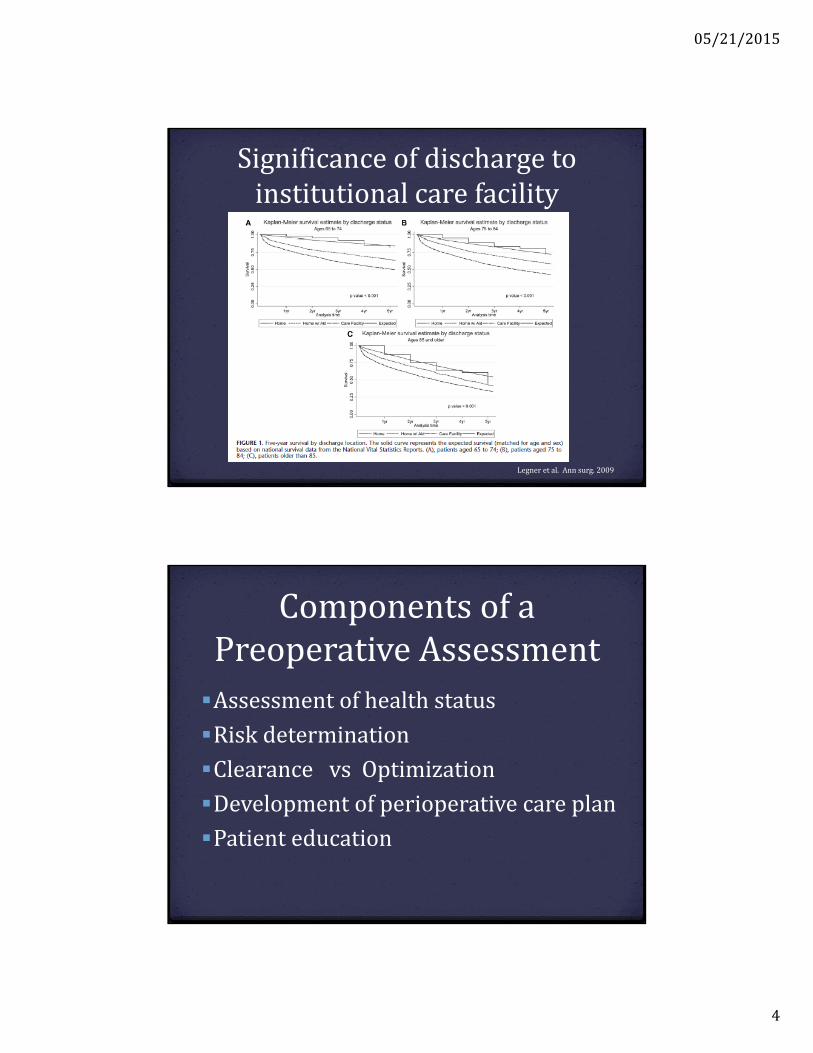
Significanceofdischargetoinstitutionalcarefacility
Legner etal.Annsurg.2009
ComponentsofaPreoperativeAssessment
Assessmentofhealthstatus
Riskdetermination
ClearancevsOptimization
Developmentofperioperativecareplan
Patienteducation
05/21/2015
5
Harvey76y/omalepresentingforpreoperativeevaluationfortotalkneearthroplasty(TKA)
Medicalhistory:
Hypertension
Atrialfibrillation
Diabetes
Hyperlipidemia
Osteoarthritis
SocialHistory:
Nonsmoker,socialetoh
Widowed,livesalonein2storyhome
Medications:
Metoprolol 25mgBID
Atorvastatin 40mgdaily
Warfarin 5mgdaily
Insulinglargine 15unitsQHS
Metformin 500mgBID
Acetaminophen1000mgq8hoursPRNpain
05/21/2015
6
PhysicalExam
Vitals:temp97.9F,pulse88,BP152/84,O296%RA,BMI20
General– well‐groomed.Ambulateswithslowantalgicgaitwiththeuseofacane.
CV‐ irregularlyirregular,nomurmur Pulm‐ lungsclear Abdomensoft,nt/nd Extremitieswithoutedema,braceonrightknee
Ancillarytests
Labs H/H:11.5/35.5;INR2.3 Creatinine1.1,fastingbloodglucose115,A1C7.2% Albumin2.9EKG‐ atrialfibrillation,normalaxis,normalintervals,noqwaves
05/21/2015
7
ObjectivesIntroduction:whydoesitmatter?
ReviewtraditionaltoolstoassesspreoperativeriskIdentifygeriatricspecificriskpredictorsforadversesurgicaloutcomes
Describeoptionsforproactiveperioperativemanagementstrategies
ASAClassificationofPhysicalStatus
ASAI Healthy
ASA 2 Mildsystemicdiseaseonlywithoutsubstantivefunctionallimitations
ASA 3 Severesystemicdisease,substantivefunctionallimitations;oneormoremoderatetoseverediseases
ASA 4 Severesystemicdiseasethatisaconstantthreattolife
ASA5 Moribound patientnotexpectedtosurvivewithout operation
http://www.asahq.org/resources/clinical‐information/asa‐physical‐status‐classification‐system
05/21/2015
8
Assessingcardiovascularrisk
Mostdevelopedandinvestigated
Incidence
perioperativecardiaccomplicationrates:2%inunselectedpatients
>5%inhigh‐riskpatients
25‐30%postoperativedeathsarefromcardiaccauses
RevisedCardiacRiskIndex(RCRI)
Publishedin1999
Derivedfrom2893patientsundergoingelectivemajornoncardiacprocedures
Validatedincohortof1422similarindividuals
Outcome:riskofcardiaccomplications
Leeetal.Circulation.1999
05/21/2015
9
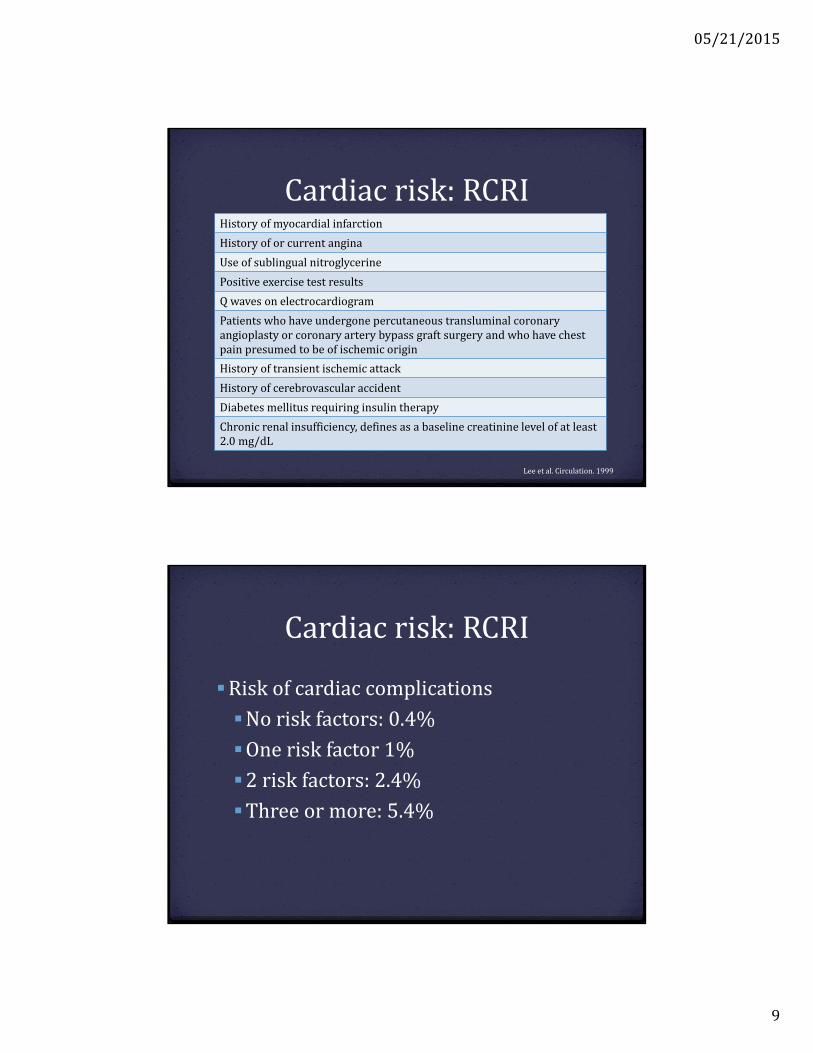
Cardiacrisk:RCRIHistoryofmyocardialinfarction
Historyoforcurrentangina
Useofsublingual nitroglycerine
Positive exercisetestresults
Qwavesonelectrocardiogram
Patientswhohaveundergonepercutaneoustransluminalcoronaryangioplastyorcoronaryarterybypassgraftsurgeryandwhohavechestpainpresumedtobeofischemicorigin
History oftransientischemicattack
Historyofcerebrovascular accident
Diabetesmellitusrequiringinsulin therapy
Chronicrenalinsufficiency, definesasabaselinecreatininelevelofatleast2.0mg/dL
Leeetal.Circulation.1999
Cardiacrisk:RCRI
Riskofcardiaccomplications
Noriskfactors:0.4%
Oneriskfactor1%
2riskfactors:2.4%
Threeormore:5.4%
05/21/2015
10
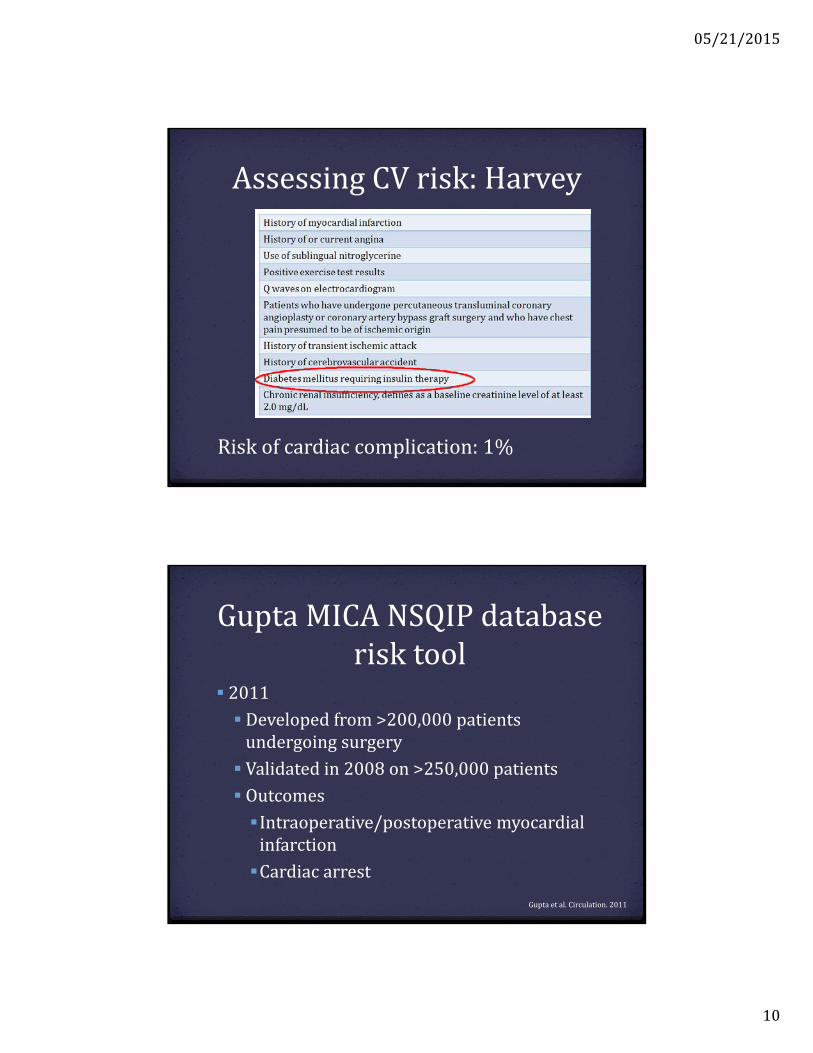
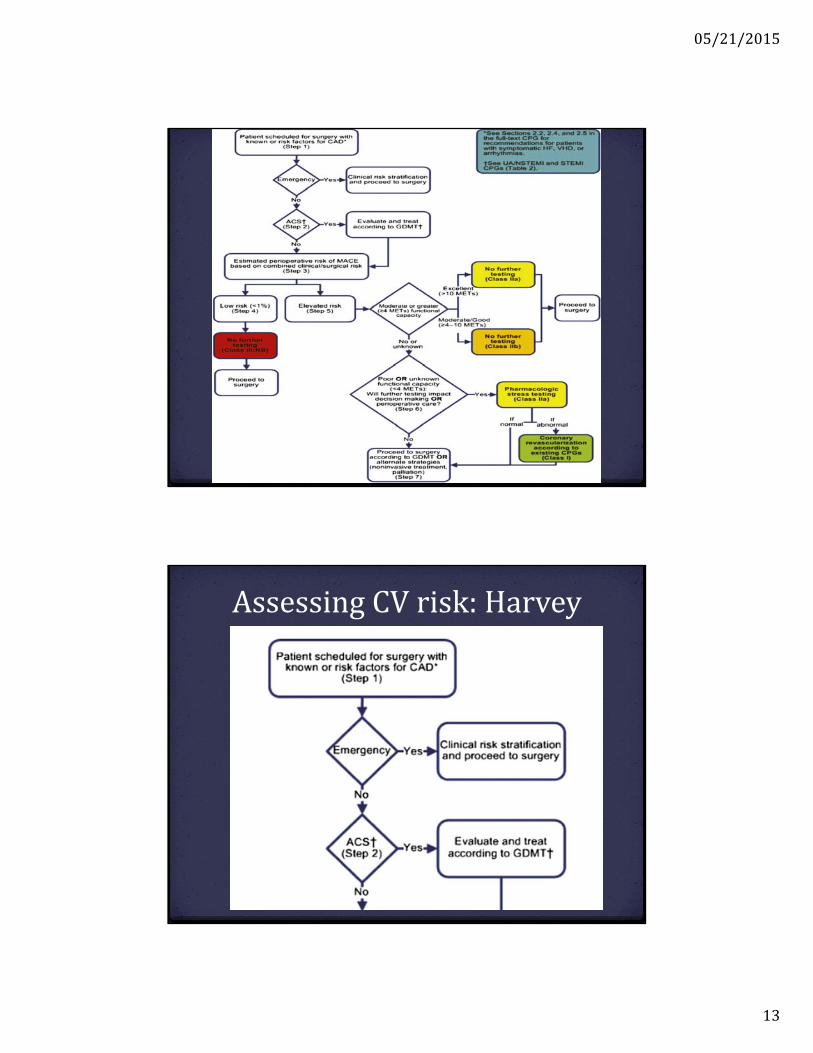
AssessingCVrisk:Harvey
Riskofcardiaccomplication:1%
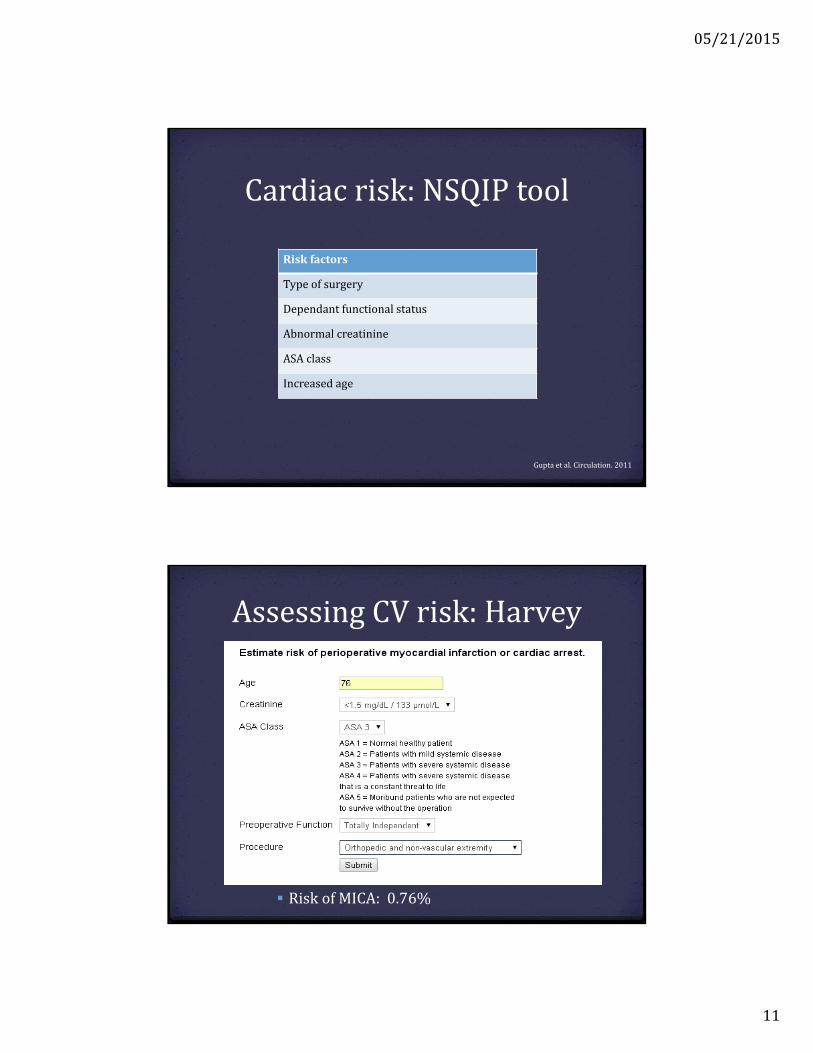
GuptaMICANSQIPdatabaserisktool
2011
Developedfrom>200,000patientsundergoingsurgery
Validatedin2008on>250,000patients
Outcomes
Intraoperative/postoperativemyocardialinfarction
Cardiacarrest
Guptaetal.Circulation.2011
05/21/2015
11
Cardiacrisk:NSQIPtool
Riskfactors
Typeofsurgery
Dependantfunctionalstatus
Abnormalcreatinine
ASAclass
Increased age
Guptaetal.Circulation.2011
AssessingCVrisk:Harvey
RiskofMICA:0.76%
05/21/2015
12
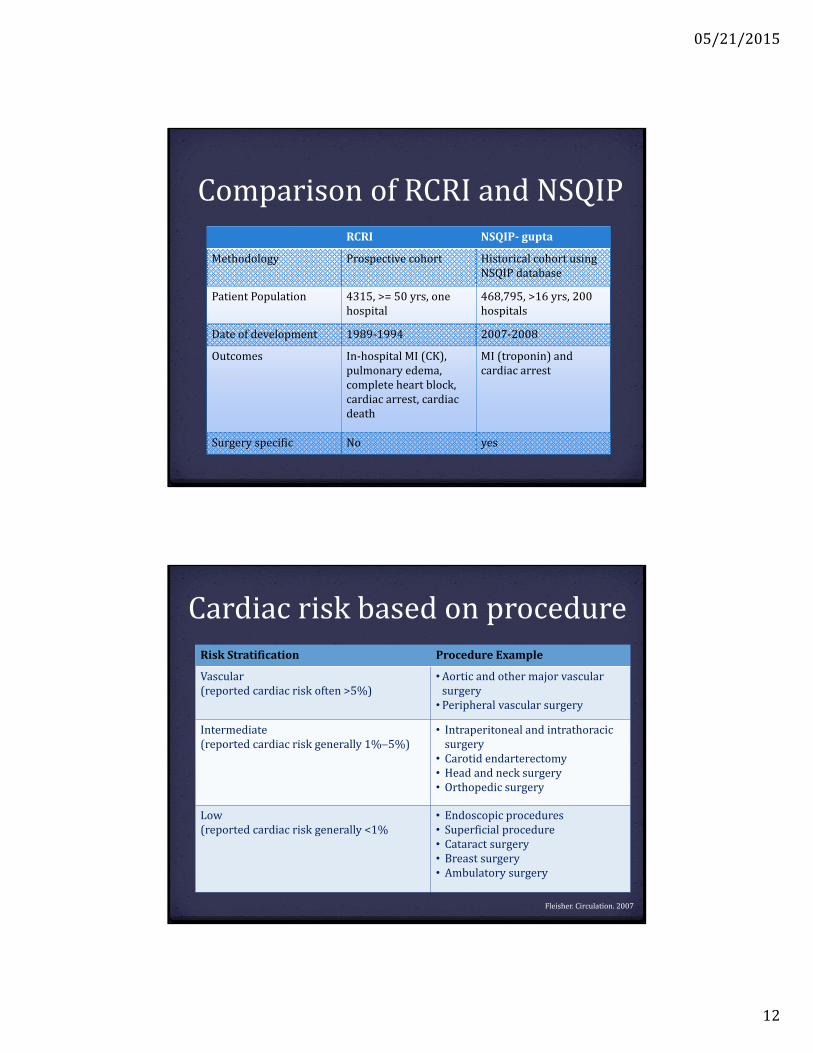
RCRI NSQIP‐ gupta
Methodology Prospectivecohort HistoricalcohortusingNSQIPdatabase
PatientPopulation 4315,>=50yrs,onehospital
468,795,>16yrs, 200hospitals
Dateofdevelopment 1989‐1994 2007‐2008
Outcomes In‐hospital MI(CK),pulmonaryedema,completeheartblock,cardiacarrest,cardiacdeath
MI(troponin)andcardiacarrest
Surgeryspecific No yes
ComparisonofRCRIandNSQIP
Cardiacriskbasedonprocedure
Fleisher.Circulation.2007
RiskStratification Procedure Example
Vascular(reportedcardiacriskoften>5%)
•Aorticandothermajor vascularsurgery•Peripheralvascularsurgery
Intermediate(reportedcardiacriskgenerally1%5%)
• Intraperitonealandintrathoracicsurgery
• Carotidendarterectomy• Head andnecksurgery• Orthopedicsurgery
Low(reportedcardiacriskgenerally<1%
• Endoscopicprocedures• Superficial procedure• Cataractsurgery• Breastsurgery• Ambulatorysurgery
05/21/2015
13
AssessingCVrisk:Harvey
05/21/2015
14
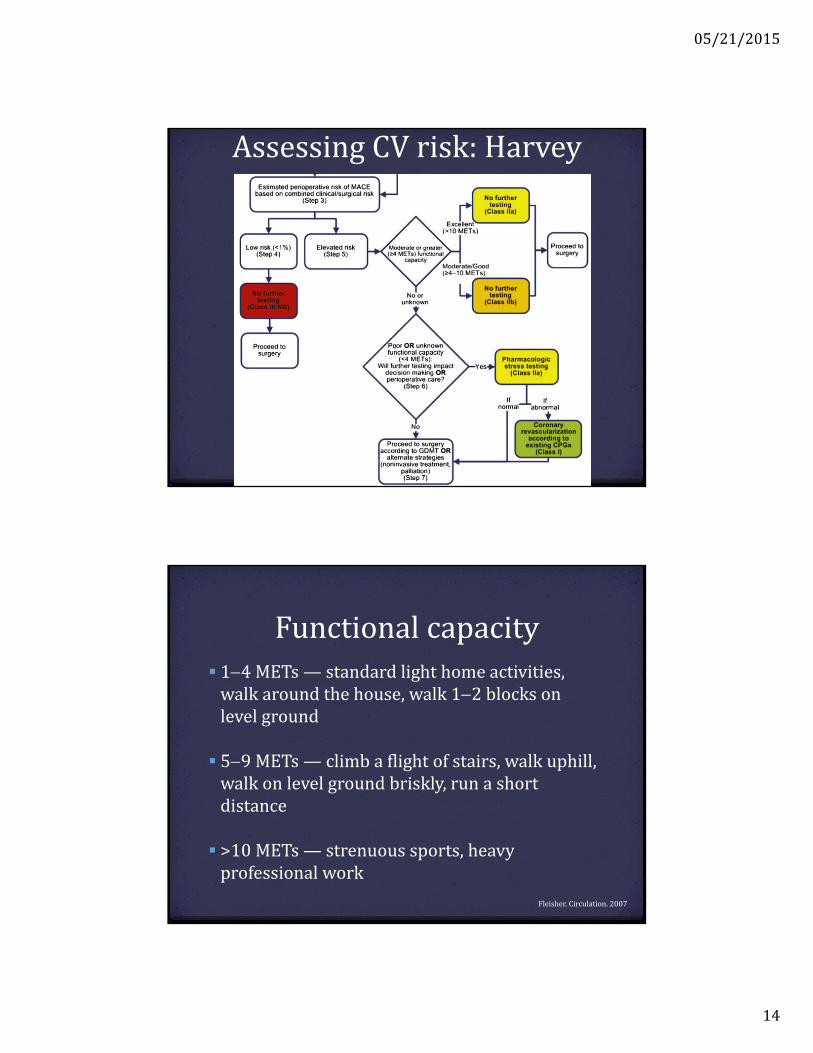
AssessingCVrisk:Harvey
Functionalcapacity 14METs— standardlighthomeactivities,walkaroundthehouse,walk12blocksonlevelground
59METs— climbaflightofstairs,walkuphill,walkonlevelgroundbriskly,runashortdistance
>10METs— strenuoussports,heavyprofessionalwork
Fleisher.Circulation.2007
05/21/2015
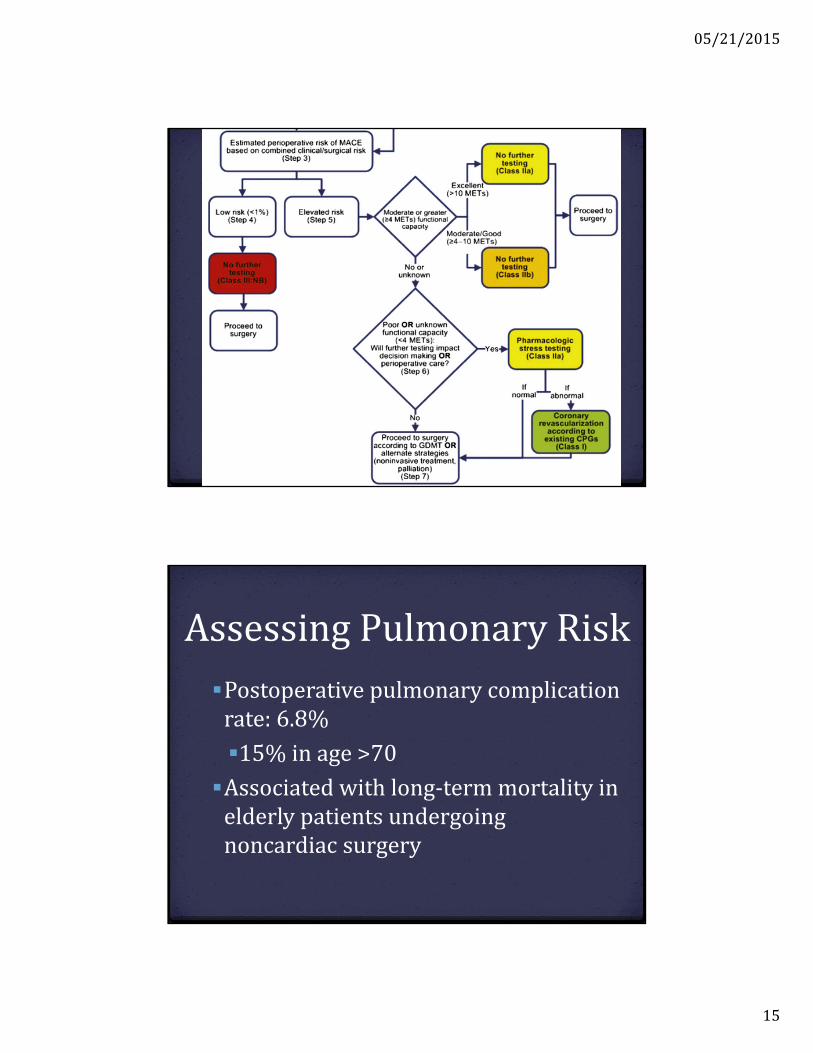
15
AssessingPulmonaryRisk
Postoperativepulmonarycomplicationrate:6.8%
15%inage>70
Associatedwithlong‐termmortalityinelderlypatientsundergoingnoncardiac surgery
05/21/2015
16
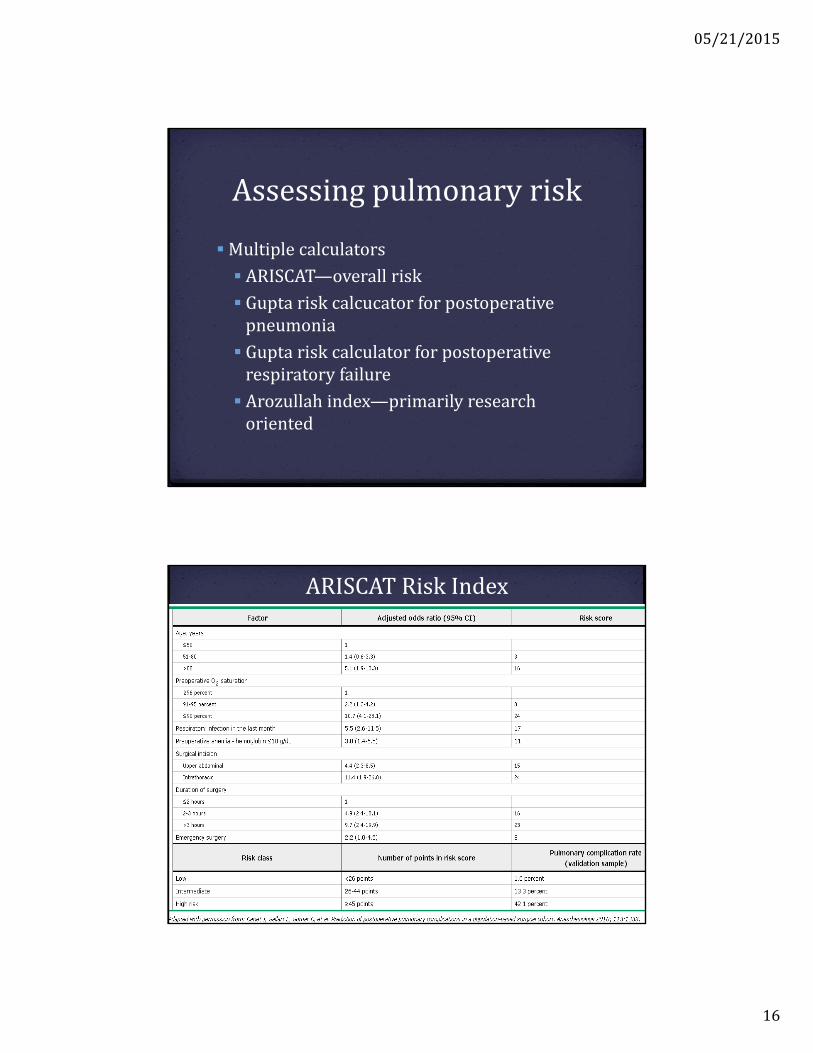
Assessingpulmonaryrisk
Multiplecalculators
ARISCAT—overallrisk
Guptariskcalcucator forpostoperativepneumonia
Guptariskcalculatorforpostoperativerespiratoryfailure
Arozullah index—primarilyresearchoriented
ARISCATRiskIndex
05/21/2015
17
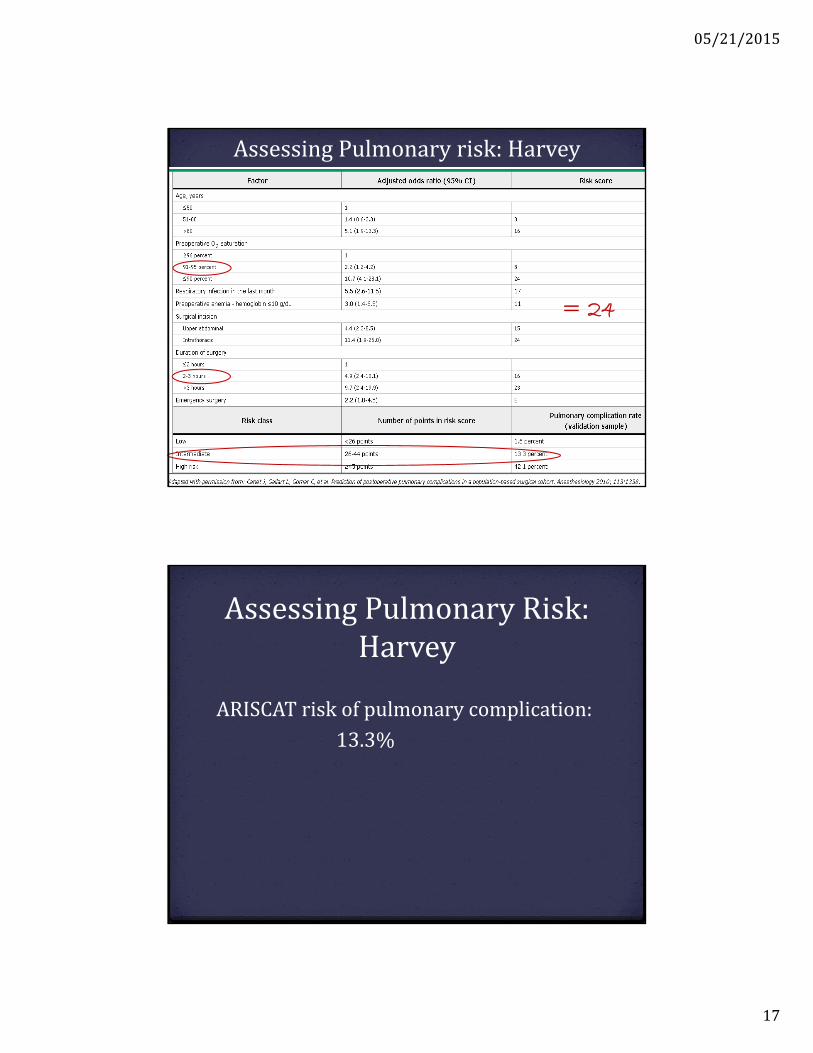
AssessingPulmonaryrisk:Harvey
= 24
AssessingPulmonaryRisk:Harvey
ARISCATriskofpulmonarycomplication:
13.3%
05/21/2015
18
Pulmonaryrisk
Interventions
OptimizationofasthmaandCOPD
Smokingcessation
Preoperativeinspiratorymuscletraining
Chowetal.JAmColl Surg.2012
HarveygoestotheOR
Harveydiscontinuedhiswarfarin5dayspriortosurgeryandisbridgedwithLMWH
Beta‐blockerandstatincontinued
Insulinandmetformin heldonthedayofsurgery
HarveyistakentotheOR,uncomplicatedTKA
05/21/2015
19
Harvey—postop
Post‐operativecourseiscomplicatedbypoorlycontrolledpainandconstipation
POD#2Harveybecomesdelirious…
…sitter,haloperidol,urinaryretention,catheter,pulledoutcatheter,hematuria,reinserted,UTI/sepsisandslowrehab
Dischargedtosub‐acuterehabonPOD#10stillconfused
Couldthishavebeenanticipated?
Traditionalpreoperativeevaluationstrategiesrisk‐stratifypatientsprimarilybasedonasingle‐organsystem
Outcomes:cardiacandpulmonarycomplications,organspecificmortality
05/21/2015
20
Butwhatabout…
Othercomplications—delirium,woundinfections,etc?
Functionalrecovery?
Needforinstitutionalization?
Lengthofstay?
Mortality?
Objectives
Introduction:whydoesitmatter?
Reviewtraditionaltoolstoassesspreoperativerisk:valueandlimitations
IdentifygeriatricspecificriskpredictorsforadversesurgicaloutcomesDescribeoptionsforproactiveperioperativemanagementstrategies
05/21/2015
21
Geriatricriskmeasures
Frailty
Functionalstatus/mobility
Cognition
Nutritionalstatus
Depression
Frailty
Stateofdecreasedphysiologicreserveandresistancetostressorsincreasedvulnerability
05/21/2015
22
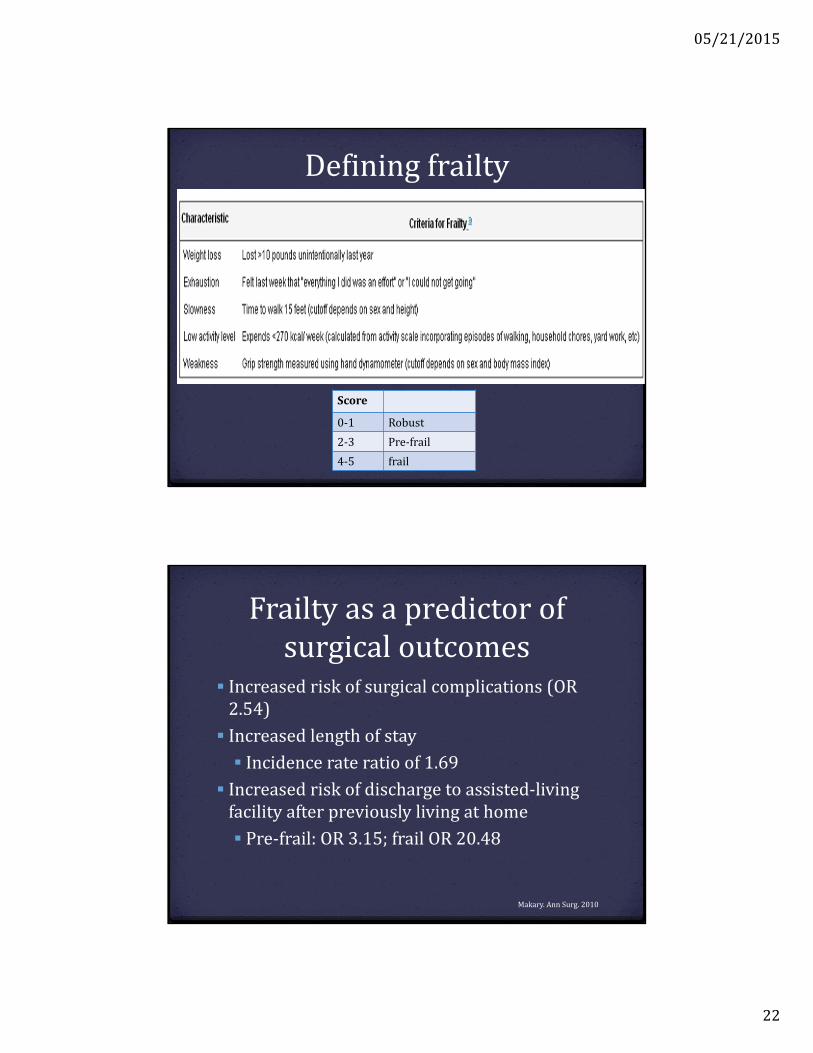
Definingfrailty
Score
0‐1 Robust
2‐3 Pre‐frail
4‐5 frail
Frailtyasapredictorofsurgicaloutcomes
Increasedriskofsurgicalcomplications(OR2.54)
Increasedlengthofstay
Incidencerateratioof1.69
Increasedriskofdischargetoassisted‐livingfacilityafterpreviouslylivingathome
Pre‐frail:OR3.15;frailOR20.48
Makary.AnnSurg.2010
05/21/2015
23
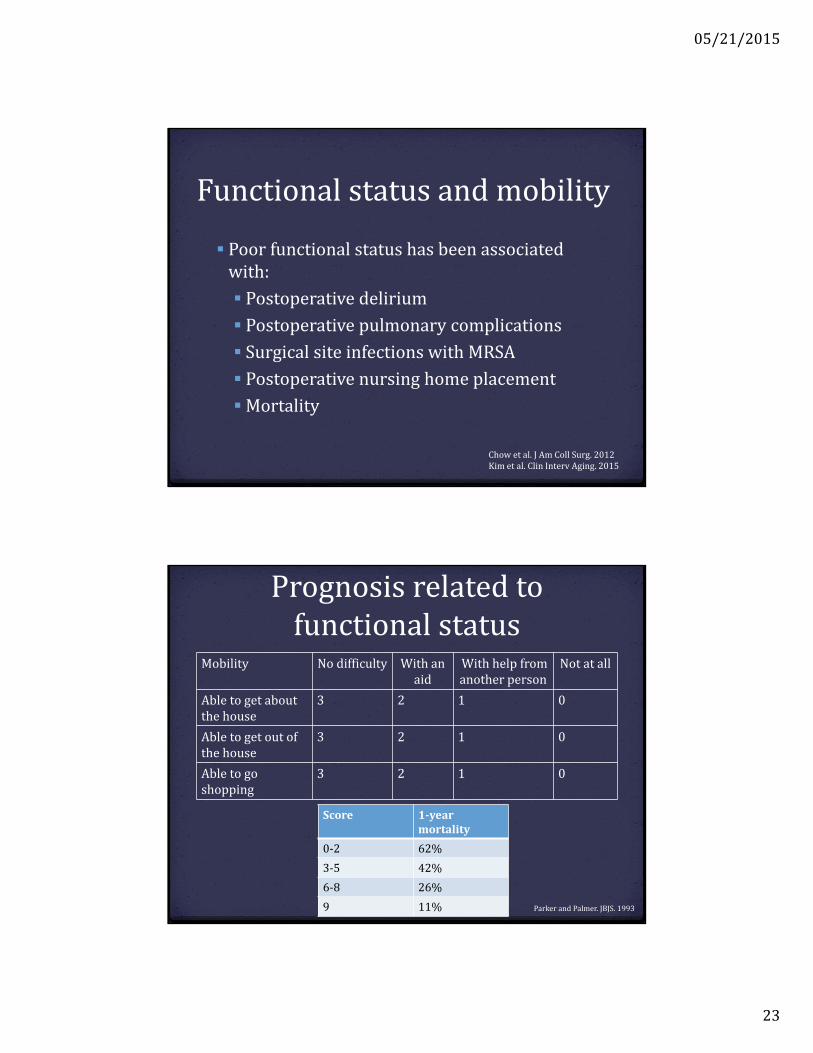
Functionalstatusandmobility
Poorfunctionalstatushasbeenassociatedwith:
Postoperativedelirium
Postoperativepulmonarycomplications
SurgicalsiteinfectionswithMRSA
Postoperativenursinghomeplacement
Mortality
Chowetal.JAmColl Surg.2012Kimetal.Clin Interv Aging.2015
Prognosisrelatedtofunctionalstatus
Score 1‐yearmortality
0‐2 62%
3‐5 42%
6‐8 26%
9 11%
Mobility Nodifficulty Withanaid
Withhelpfromanotherperson
Notatall
Abletogetaboutthehouse
3 2 1 0
Abletogetoutofthehouse
3 2 1 0
Abletogoshopping
3 2 1 0
ParkerandPalmer.JBJS.1993
05/21/2015
24
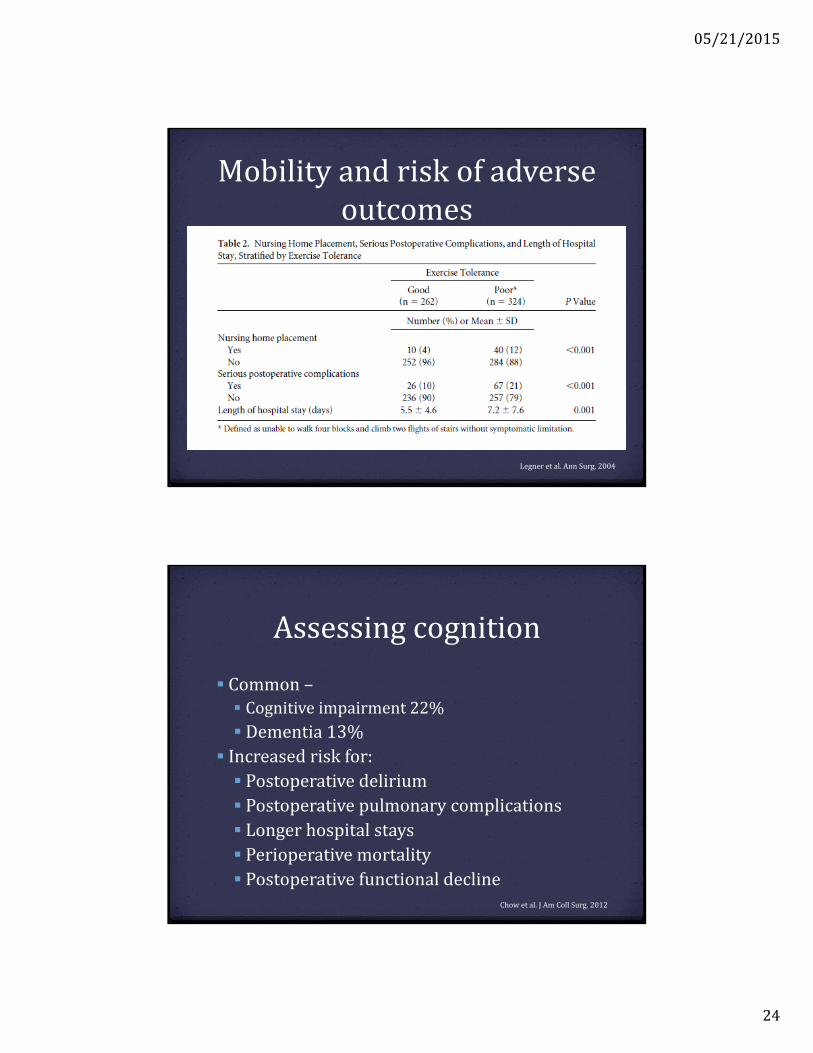
Mobilityandriskofadverseoutcomes
Legner etal.AnnSurg.2004
Assessingcognition
Common– Cognitiveimpairment22%
Dementia13% Increasedriskfor: Postoperativedelirium Postoperativepulmonarycomplications Longerhospitalstays Perioperativemortality Postoperativefunctionaldecline
Chowetal.JAmColl Surg.2012
05/21/2015
25
Assessingcognition
ConsiderscreeningallpatientswiththeMini‐Cog
Carefuldocumentationofpreoperativecognitivestatusmayhelpwithassessmentofpostoperativecognitivechanges
AssessingNutritionalStatus
Malnutritioniscommon:
5.8%communitydwellers
13.8%innursinghomes
38.7%hospitals
50.5%inrehabilitation
Increasedriskofmorbidity(particularyinfections)OR2.30‐3.47
05/21/2015
26
AssessingNutritionalStatus
Severenutritionalriskbasedon
BMI<18.5
Serumalbumin<3.0
Unintentionalweightloss
Ifpossible,considerpreoperativenutritionalassessmentbydietician
Depression
PrevalenceinUSgeriatricpopulation(>70)11%
Preoperativedepressionhasbeenassociatedwith
Increasedmortality
Increasedlengthofstay
Higherpainperceptionandincreasedanalgesicuse
05/21/2015
27
Harvey
FurtherhistoryrevealsthatHarveywaspreviouslyabletowalk2‐3blockswithacaneandclimb1flightofstairs;ambulationwasslowandlimitedbykneepain.Had12lbs ofunintentionalweightlossoverthelastyear;sonexpressesconcernaboutdepressionasHarveyfrequentlycomplainsoffatigueandweakness.Heisstilldrivingthoughrequiresassistancefromfamilymemberswithgroceryshopping.Sonhadbeenmanagingallfinancesduetoerrorsmadeonhis2014taxreturn.
Harvey
FurtherhistoryrevealsthatHarveywaspreviouslyabletowalk2‐3blockswithacaneandclimb1flightofstairs;ambulationwasslowandlimitedbykneepain.Had12lbs ofunintentionalweightlossoverthelastyear;familynoteshefrequentlyendorsesafeelingofgeneralfatigueandweakness.Isstilldrivingthoughrequiresassistancefromfamilymemberswithgroceryshopping.Sonhadbeenmanagingallfinancesduetoerrorsmadeonhis2014taxreturn.
Frailty
05/21/2015
28
Harvey
FurtherhistoryrevealsthatHarveywaspreviouslyabletowalk2‐3blockswithacaneandclimb1flightofstairs;ambulationwasslowandlimitedbykneepain.Had12lbs ofunintentionalweightlossoverthelastyear;familynoteshefrequentlyendorsesafeelingofgeneralfatigueandweakness.Isstilldrivingthoughrequiresassistancefromfamilymemberswithgroceryshopping.Sonhadbeenmanagingallfinancesduetoerrorsmadeonhis2014taxreturn.
Cognition
Mobility
Harvey
FurtherhistoryrevealsthatHarveywaspreviouslyabletowalk2‐3blockswithacaneandclimb1flightofstairs;ambulationwasslowandlimitedbykneepain.Had12lbs ofunintentionalweightlossoverthelastyear;sonexpressesconcernaboutdepressionasHarveyfrequentlycomplainsoffatigueandweakness.Heisstilldrivingthoughrequiresassistancefromfamilymemberswithgroceryshopping.Sonhadbeenmanagingallfinancesduetoerrorsmadeonhis2014taxreturn.
Nutrition
Depression
05/21/2015
29
Harvey
Harvey’ssoncalls.HenotifiesyouthatgivenHarvey’spoorprogresswiththerapytherecommendationhasbeenmadefordischargetoanursinghomefor24hourcare.
“Couldthishavebeenprevented?”
ObjectivesIntroduction:whydoesitmatter?
Reviewtraditionaltoolstoassesspreoperativerisk:valueandlimitations
Identifygeriatricspecificriskpredictorsforadversesurgicaloutcomes
Describeoptionsforproactiveperioperativemanagementstrategies
05/21/2015
30
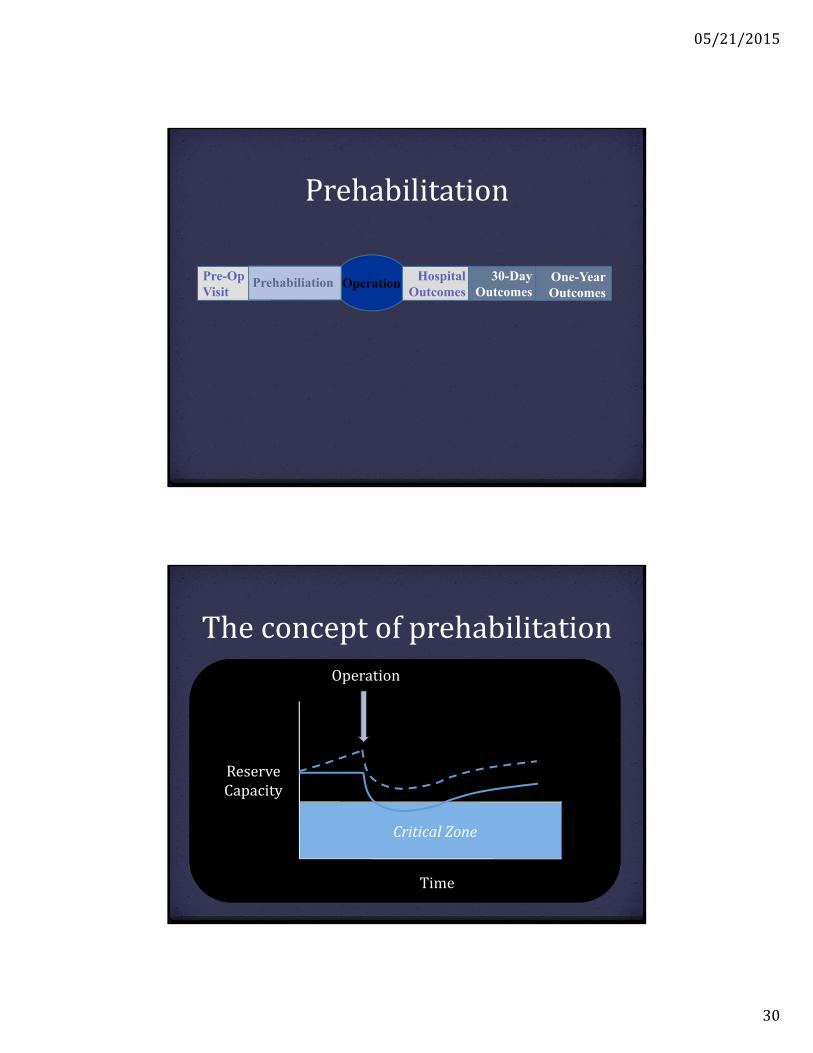
Pre-OpVisit
Operation HospitalOutcomes
30-DayOutcomes
One-YearOutcomes
Prehabiliation
Prehabilitation
Time
ReserveCapacity
CriticalZone
Operation
Theconceptofprehabilitation
05/21/2015
31
Puttingitalltogether
GeriatricSurgicalAssessmentPredicts:
Increasedcomplications
Longerlengthofstaty
Higherrateofdischargeinstitutionalization
Increasedthirtydayre‐admission
Higherhospitalcosts
Highersix‐monthhealthcarecosts
Robinson.AnnSurg.2009Robinson.JAmColl Surg.2011.Robinson.AmJSurg .2011.
05/21/2015
32
Mytake‐homepointsThepreoperativeassessmentisBIG!
Geriatricassessmentmarkerspredictriskforadverseoutcomes
Thisiskeyinanticipatoryguidanceandincounsellingpatientswhoareconsideringundergoinganelectiveprocedure
Prehabilitation mayimprovepost‐operativeoutcomes
Acknowledgements
Drs Shea,Bray‐Hall,Lum,Robbins,andHoffmanforreviewingmyslidesandlettingmepractice!
Dr ThomasRobinsonforassistancewithslides
05/21/2015
33
References
2014ACC/AHAGuidelineonPerioperativeCardiovascularEvaluationandManagementofPatients UndergoingNoncardiac Surgery:AReportoftheAmericanCollegeofCardiology/AmericanHeartAssociationTaskForceonPracticeGuidelines.JAmColl Cardiol.2014;64(22):e77‐e137
Canet J.Predictionofpostoperativepulmonarycomplicationsinapopulation‐basedsurgicalcohort. Anesthesiology.2010;113(6):1338
ChowWB,RosenthalRA,etal.Optimalpreoperativeassessmentofthegeriatricsurgicalpatient:Abestpracticesguidelinefrom theAmericanCollegeofSurgeonsNationalsurgicalqualityImprovementProgramandtheAmericanGeriatricsSociety.JournaloftheAmColl ofSurgeons.2012;215(4):453‐466
CohnSL,FleisherLA.Evaluationofcardiacriskpriortononcardiac surgery.UpToDate.2015Daabiss M.AmericanSocietyofAnaesthesiologists physicalstatusclassification.IndianJAnaesthe.2011;55(2):111‐115GuptaPK,GuptaH,Sundaram A,etal.Developmentandvalidationofariskcalculatorforpredictionofcardiacriskaftersurgery.
Circulation2011;124:381KimS,BrooksA,Groban L.Preoperativeassessmentoftheoldersurgicalpatient:honinginongeriatricsyndromes.Clinical
interventionsinAging.2015;10:13‐27LeeTH,Marcantonio ER,etal.Derivationandprospectivevalidationofasimpleindexforpredictionofcardiacriskofmajor
noncardiac surgery.Circulation.1999;100(10):1043.Legner VJ,Doerner D,etal.Riskfactorsfornursinghomeplacementfollowingmajornonemergent surgery.TheAmericanJournalof
Medicine.2004;117:82‐86Legner VJ,Massarweh NN,etal.Thesignificanceofdischargetoskilledcareafterabdominopelvicsurgeryinolderadults.Annalsof
Surgery.2009;249(2):250‐256Makary MA,Segev DL,etal.Frailtyasapredictorofsurgicaloutcomesinolderpatients.JournaloftheAmericanCollegeofSurgeons.
2010;210(6):901‐908ParkerMJ,PalmerCJ.Anewmobilityscoreforassessingmortalityafterhipfracture.Britisheditorialsocietyofboneand joint
surgery.1993;75(5):797‐798RobinsonTN,Eiseman B,WallaceJI,etal.Redefininggeriatricpreoperativeassessmentusingfrailty,disabilityandco‐morbidity.Ann
Surg.2009;250:449‐99SmetanaGW.Evaluationofpreoperativepulmonaryrisk.UpToDate.2015Xue QL.Thefrailtysyndrome:definitionandnaturalhistory.Clin Geriart Med.2011;27(1):1‐15Zambouri A.Preoperativeevaluationandpreparationforanesthesiaandsurgery.Hippokratia.2007;11(1):13‐21