Embed Size (px)
Citation preview

Geriatric Fracture Program
Stephen L. Kates, MDProfessor and ChairmanVirginia Commonwealth UniversityAugust, 2019

Disclosures
DateFooter 2
Research SupportIndustry: DePuy Synthes for resident research supportFoundation: AO Foundation (research grant)Government: NIH, AHRQ, PCORI
Consultant: American College of Surgeons
Journal Editor: Sage, Geriatric Orthopaedic Surgery and Rehabilitation
Concepts of an Organized programHow it worksStandardizing carePatient FlowResults
3

–Decrease morbidity and mortality–Decrease length of stay–Decrease time to surgery–Improve Quality of Care

The Program:• Fragility fractures older than 65
– Low energy– Fall from standing height– Long bone and pelvic fractures
• Lean methods to improve outcomes*• Co-management• Patient-centered protocol driven care
*Kates, Orthopaedic Clin North Am 2014

• Collaborative, interdisciplinary care– SW, PT, OT, nurses, patient care technicians
• Discharge planning begins at admission• Rapid pre-operative assessment• Early operative management• Joint patient ownership• Collegial environment

• Orthopaedics - Geriatrics• Physicians – PA’s, NP’s• Patient - family• Consultants• Hospital team - institution team
–Co-developed
–Agreement on local “best practices”
–Sensitivity to reasonable preferences/styles
–Compromise to the practical
–Avoid iatrogenic errors

Preprinted orders –Goal: insure medical stability–All admitted to orthopaedics
• Each service called once–Reduce ED time–Easiest patient to move out of ED–Early pain control- Fascia iliaca block

–Optimize condition• Pain control• Fluid management• Coagulation management• Establish goals of care (advanced directives)
• Functional assessment• Medication management

–Stratify risk–Optimize condition–Coordinate consults (rare!)–Support discharge planning

• Length of stay depends on:
–Rapid medical assessment–Rapid optimization–Operating room availability–Surgeon cooperation–Anesthesia cooperation–Patient / family cooperation–Rehabilitation bed availability

• Medical evaluation– Prompt– Optimize medical condition for OR– Minimize surgical risks
• Surgical fixation– < 24 hours– Shorter is better– Should have high priority in trauma room

Metabolic Bone workup on admission
DateFooter 14
Take good history including family historyCalcium25-OH Vitamin D levelPTH levelHistory of prior use of bisphosphonates or other therapies

Anticoagulants
DateFooter 15
Warfarin: safe to reverse Use oral vitamin KFFP for short term correction onlyINR ~ 1.5 target
Plavix or other platelet inhibitors- ignore and proceed with surgeryDirect anticoagulants- likely need 48 hours to reverse
no good antidote yet

ERASEnhanced Recovery after Surgery
DateFooter 16
Includes preop optimizationAllow carbohydrate rich liquid up to 2 hours preopAvoid opiatesEarly postop mobility

Echocardiography
DateFooter 17
Not usually indicatedAvoid getting them unless requested by geriatricsException: concern for severe aortic stenosis*
*Fleisher, LA, 2014 ACC/AHA guidelines, J Am Coll Cardiol 2014

• Full risk assessment reassures them• The patient IS optimized
– Complications in O.R. - Rare– Hydrated properly– Pain controlled
• Spinal and General have clinical equipoise • Avoid intraoperative hypotension• Functional capacity is predictive of outcomes

OptimizedNot febrileSkin healthy
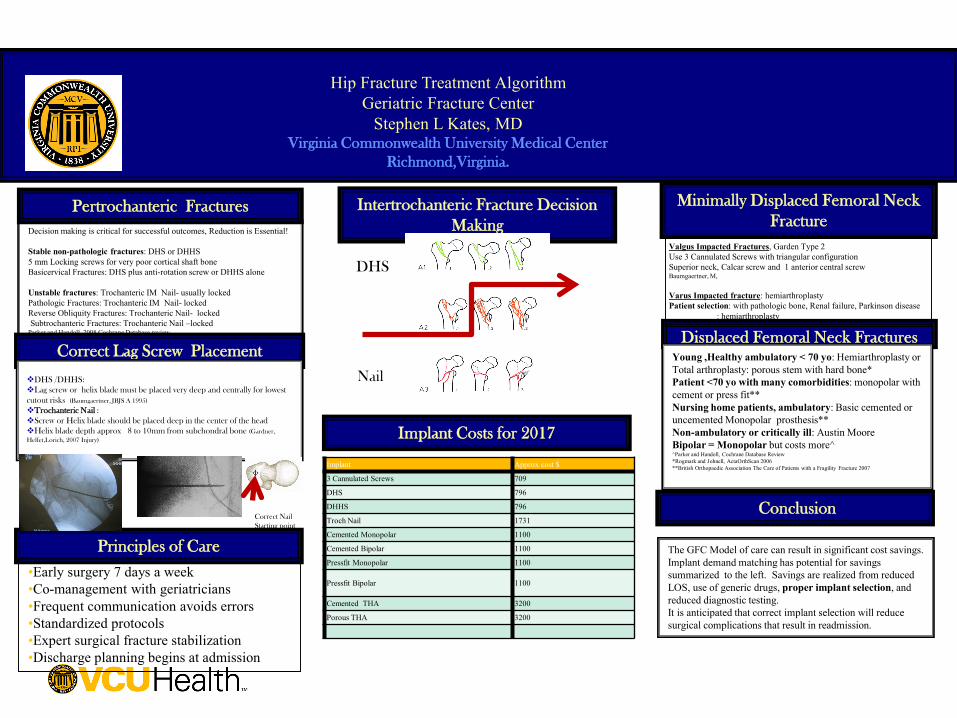
Minimally Displaced Femoral Neck Fracture
Decision making is critical for successful outcomes, Reduction is Essential!
Stable non-pathologic fractures: DHS or DHHS5 mm Locking screws for very poor cortical shaft boneBasicervical Fractures: DHS plus anti-rotation screw or DHHS alone
Unstable fractures: Trochanteric IM Nail- usually lockedPathologic Fractures: Trochanteric IM Nail- lockedReverse Obliquity Fractures: Trochanteric Nail- lockedSubtrochanteric Fractures: Trochanteric Nail –locked
Parker and Handoll, 2008 Cochrane Database review
Intertrochanteric Fracture Decision Making
Pertrochanteric Fractures
Correct Lag Screw Placement
Hip Fracture Treatment AlgorithmGeriatric Fracture Center
Stephen L Kates, MDVirginia Commonwealth University Medical Center
Richmond,Virginia.
DHS /DHHS:Lag screw or helix blade must be placed very deep and centrally for lowest cutout risks (Baumgaertner, JBJS A 1995)
Trochanteric Nail :Screw or Helix blade should be placed deep in the center of the headHelix blade depth approx 8 to 10mm from subchondral bone (Gardner, Helfet,Lorich, 2007 Injury)
The GFC Model of care can result in significant cost savings. Implant demand matching has potential for savings summarized to the left. Savings are realized from reduced LOS, use of generic drugs, proper implant selection, and reduced diagnostic testing.It is anticipated that correct implant selection will reduce surgical complications that result in readmission.
Implant Costs for 2017
Conclusion
Displaced Femoral Neck FracturesYoung ,Healthy ambulatory < 70 yo: Hemiarthroplasty or Total arthroplasty: porous stem with hard bone*Patient <70 yo with many comorbidities: monopolar with cement or press fit**Nursing home patients, ambulatory: Basic cemented or uncemented Monopolar prosthesis**Non-ambulatory or critically ill: Austin MooreBipolar = Monopolar but costs more^^Parker and Handoll, Cochrane Database Review*Rogmark and Johnell, ActaOrthScan 2006**British Orthopaedic Association The Care of Patients with a Fragility Fracture 2007
Valgus Impacted Fractures, Garden Type 2Use 3 Cannulated Screws with triangular configurationSuperior neck, Calcar screw and 1 anterior central screwBaumgaertner, M,
Varus Impacted fracture: hemiarthroplastyPatient selection: with pathologic bone, Renal failure, Parkinson disease
: hemiarthroplasty
Implant Approx cost $
3 Cannulated Screws 709
DHS 796
DHHS 796
Troch Nail 1731
Cemented Monopolar 1100
Cemented Bipolar 1100
Pressfit Monopolar 1100
Pressfit Bipolar 1100
Cemented THA 3200
Porous THA 3200
Principles of Care
•Early surgery 7 days a week•Co-management with geriatricians •Frequent communication avoids errors•Standardized protocols•Expert surgical fracture stabilization •Discharge planning begins at admission
DHS
Nail
Correct Nail Starting point
Pre-op planning• Keep patient warm• Carefully position the patient• Skin is often very fragile• Correct dose IV antibiotic – weight basedRight procedure• Correct implant choice• Rapid repair• Stable construct to allow WBAT

• Protocol driven• Standard hip fracture order set• Standardized nursing care plan• Care team is consistent about plan• SW finalizes discharge plan
– Supported by team

• Weight bearing as tolerated Day of Surgery**– Surgical stable repair– Most patients can’t limit weight bearing– Knee braces used rarely
• Multimodal pain control• DVT prophylaxis LMWH x 28 days• Remove “tethers”• Regular diet
** coming Joint Commission standard

Delirium
DateFooter 24
Major cause of complicationsHyperactive typeHypoactive typeAvoidance is bestRetain glasses and hearing aidsAvoid bad meds- Benadryl, H2 blockers, Benzo’sAvoid tethersFamily input helpsGood pain control
Delirium may become chronic

• Starts on admission• Most: SNF Rehabilitation• Some: LTC placement (or return)• Few: home with home care services• Team members support and consistent• Length of stay goal is 4 days

August 2019
Stephen L. Kates, MD
Thanks for your attention!





























