Embed Size (px)
Citation preview

Welcome
Use the following buttons to help you move around.
To advance forward click the left mouse key or enter key.
To move backward one slide.
To end the tutorial.
To go to the home page.
To try a question again.
To link to a segment in this tutorial.
Yellow, underlined text displays the definition when you hover the cursor over the word.
Navigation Home Page
Click on any one of these buttons to view that segment of the tutorial.
Quick ReviewNormal Heart Function
Heart FailurePathophysiology
References
NeurohormonalTherapy
NeurohormonalPathways
Patient Assessment
Introduction
Case Study
Objectives
By the end of this tutorial the learner will Have an increased understanding of
heart failure pathophysiology Understand the neurohormonal
activation process Identify signs and symptoms of right and
left-sided heart failure Understand neurohormonal heart
medication therapy
Heart Failure Statistics There are about 5 million patients with
symptomatic CHF and close to 500,000 new cases every year.
This disorder accounts for 12-15 million office visits and 6.5 million hospital days.
About 300,000 patients die each year of CHF, and in spite of advances in treatment the number of deaths has been increasing steadily.
The total annual inpatient and outpatient costs in the US are at least $40 billion (drugs account for $500 million).
Mann, D, Heart Failure; A Companion to Braunwald’s Heart Disease 2004
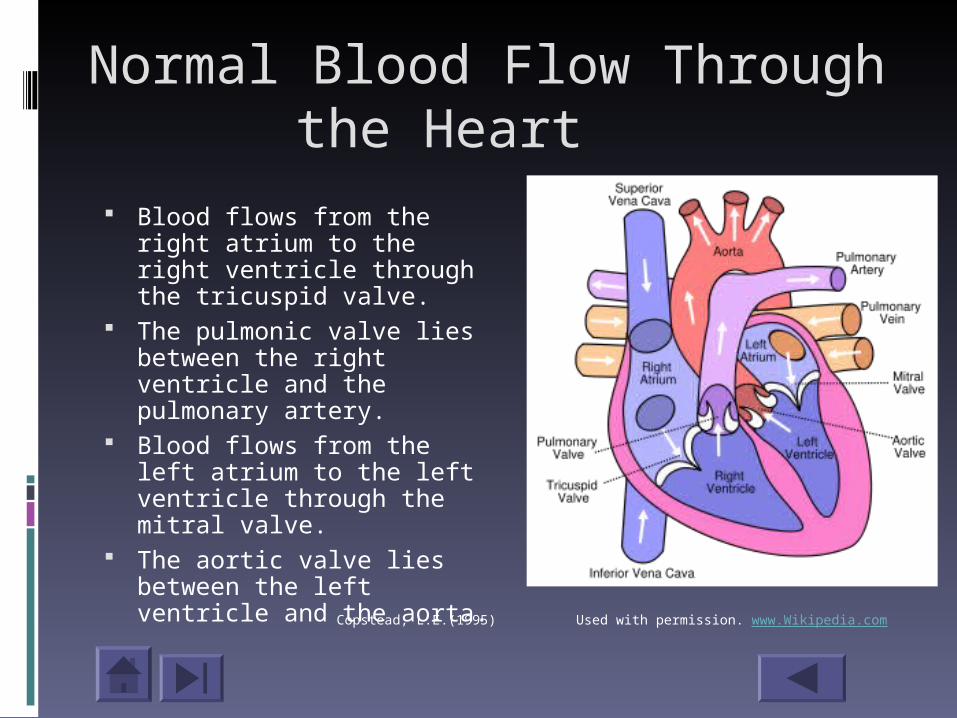
Normal Blood Flow Through the Heart
Blood flows from the right atrium to the right ventricle through the tricuspid valve.
The pulmonic valve lies between the right ventricle and the pulmonary artery.
Blood flows from the left atrium to the left ventricle through the mitral valve.
The aortic valve lies between the left ventricle and the aorta.
Copstead, L.E.(1995) Used with permission. www.Wikipedia.com
Cardiac Cycle The cardiac cycle is composed of a period of
contraction (systole) followed by a period of relaxation (diastole), or one heartbeat.
The cycle begins with ventricular filling, the ventricles are relaxed and blood flows in from the atria through the AV valves. Near the end of ventricular diastole, the atria contract, squeezing more blood through the AV valves in the ventricles.
The ventricles begin to contract immediately following atrial systole causing intraventricular pressure to rise and the AV valves to close. (This produces the S1 sound.) Copstead, L.E.(1995)

Cardiac Cycle With all four cardiac valves closed, ventricular pressure
rises rapidly and the blood within is forcefully compressed.
When ventricular pressure exceeds aortic pressure, the aortic valve is forced open and rapid ejection of blood occurs.
Relaxation phase begins with semilunar valve closure (S2) in response to falling ventricular pressures and ends when the AV valves open to allow for ventricular filling.
Opening of the AV valves signals the beginning of rapid ventricular filling and the start of another cardiac cycle.Copstead, L.E.(1995)

Heart terms to review
Cardiac Output This is the amount of blood that the heart pumps each minute.
Loading conditions The stretch imposed by the blood volume on the cardiac muscle
and the force that the muscle must generate to move the load.
Preload Is the volume of blood stretching the resting heart muscle and is
determined by the venous return to the heart.
Afterload Is the force that the contracting heart must generate to eject blood
from the filled heart.
Porth, C.M., et.al., (2005)
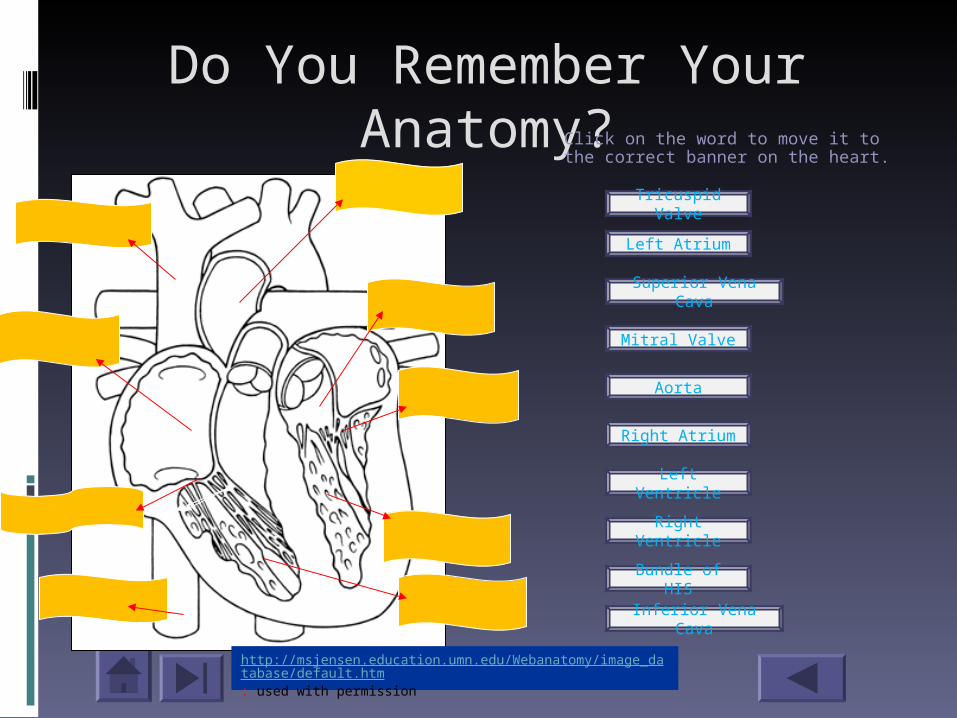
Do You Remember Your Anatomy?Click on the word to move it to the
correct banner on the heart.
http://msjensen.education.umn.edu/Webanatomy/image_database/default.htm: used with permission
Left Atrium
Superior Vena Cava
Mitral Valve
Aorta
Left Ventricle
Right Atrium
Right Ventricle
Bundle of HIS
Inferior Vena Cava
Tricuspid Valve

What is Heart Failure?
Heart failure is a syndrome that can be caused by a variety of conditions that result in damage to the myocardium and is recognized by a characteristic pattern of haemodynamic, renal, neural, and hormonal responses.
When heart failure develops, the heart is unable to provide adequate amounts of oxygenated blood to meet the needs of peripheral tissue or does so only at abnormally high intracardiac filling pressures.
Greenberg, B., Barnard, D. (2005)

Causes of Heart Failure
Myocardial Infarction (MI) Long standing pressure or volume
overload Myocyte damage caused by a viral
infection Damage caused by replacement of
normal myocardium by infiltrative diseases
Greenberg, B., & Barnard, D. (2005)
Risk Factors of Heart Failure
Hypertension Coronary Disease Valvular Disease MI Diabetes Mellitus Dyslipidemia Atrial Fibrillatin Smoking Physical Inactivity Systemic Inflammation (C-reactive protein)
Greenberg, B., & Barnard, D. (2005
Which conditions can result in damage to the myocardium? (There is more than one right answer)
Unstable Atherosclerotic plaquesRheumatic Heart DiseaseRaynaud’s Disease

Correct! Unstable atherosclerotic plaques rupture causing platelet aggregation and thrombus formation and eventual myocardial infarction.
Back to the question
Great job! Rheumatic fever is an acute immune-mediated inflammatory diseases that can lead to the development of chronic valvular disorders that produce permanent cardiac dysfunction.
Back to the question
Although this disease causes intense vasospasm of the arteries and arterioles of the fingers and toes, it does not cause damage to the myocardium.
Back to the question
Heart Failure Manifestations
Fluid retention and edema Shortness of breath and other respir
atory manifestations Fatigue and limited exercise toleranc
e Cachexia and malnutrition Cyanosis Elevated BNP levels
Porth, C.M., et.al., (2005)

Fluid Retention and Edema
Peripheral and portal edema occurs in right-sided heart failure 1 pint of accumulated fluid results in a 1 lb.
weight gain. As a rule, weight gain of > 2 lb in 24 hrs or 5 lb in one week is a sign of worsening heart failure.
Pulmonary edema occurs in left-sided heart failure When the pulmonary capillary filtration
pressure (nl.=10mmHg) exceeds the capillary osmotic pressure (nl.=25mm Hg) there is a shift of fluid from the intravascular into the interstitium of the lung.
© 2007 Microsoft
© 2007 MicrosoftPorth, C.M., et.al., (2005)
Back to CHF S/S
Shortness of Breath and other respiratory manifestations Due to the congestion of the
pulmonary circulation, the following symptoms are left-sided heart failure. Dyspnea Orthopnea Paroxysmal nocturnal dyspnea Cough Cheyne-Stokes respirations
Porth, C.M., et.al., (2005)
Back to CHF S/S
Fatigue and limited exercise tolerance
Decreased cardiac output from the left ventricle causes fatigue and limb weakness.
These symptoms progress as activity increases during the day.
© 2007 Microsoft
Porth, C.M., et.al., (2005)
Back to CHF S/S

Cachexia and Malnutrition
Congestion of the liver and gastrointestinal structures from right-sided heart failure impairs digestion and absorption creating a feeling of fullness.
www.daily-diabetic.com
Porth, C.M., et.al., (2005)Back to the CHF S/S
Cyanosis
Cyanosis around the lips and in the peripheral part of the extremities may develop from right and left -sided heart failure. Caused by arterial desaturation resulting from impaired pulmonary
gas exchange Caused by venous desaturation resulting from extensive extraction
of oxygen at the capillary level
Porth, C.M., et.al ., (2005) Back to CHF S/S

Elevated Brain natriuretic peptide (BNP) levels B-type natriuretic peptide is
synthesized and released by ventricular myocytes and fibroblasts in response to myocardial stretching.
Normal lab levels are < 100pg/mL BNP levels in CHF depend on other co-
morbidities. COPD, LVH, obesity, age can all effect the BNP level. (Levels from 100-400pg/mL are questionable for CHF. Values over 500pg/mL are likely due to CHF).Porth, C.M., et.al.,(2005)
Right-sided Heart failure
Occurs when the right side of the heart fails and there is a back up of blood in the systemic venous system
This causes an increase in pressure in which of the following areas?
(Click on the correct answers)
Right atriumRight ventricular end diastolicSystemic venous
Porth, C.M.,et.al., (2005)Porth, C.M.,et.al., (2005)
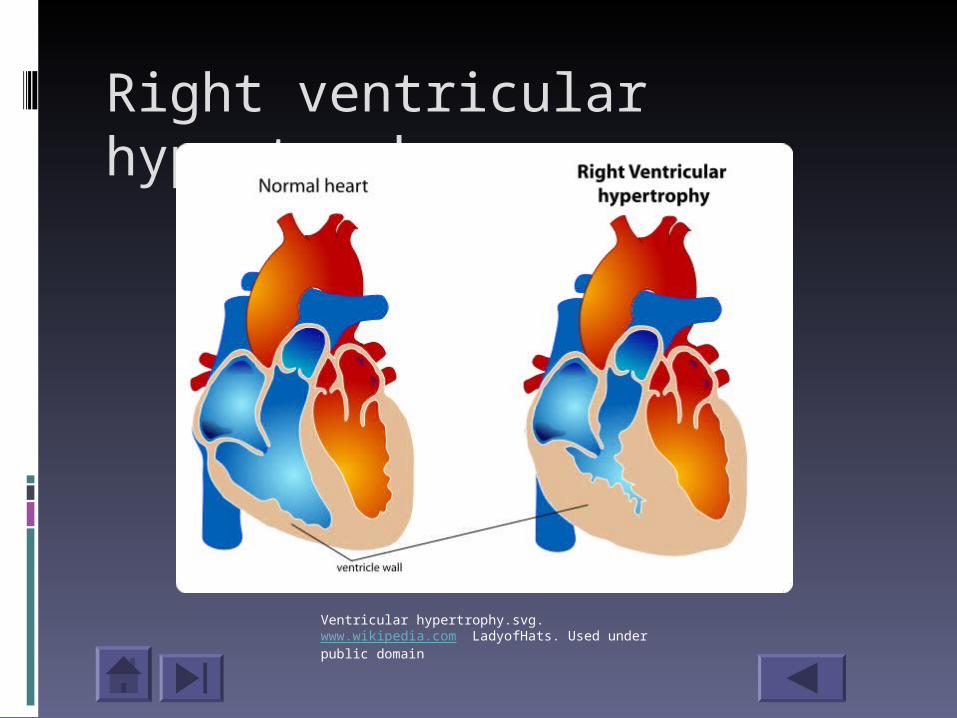
Right ventricular hypertrophy
Ventricular hypertrophy.svg. www.wikipedia.com LadyofHats. Used under public domain
Left-sided Heart Failure
Impairment of left heart function leads to a decrease in cardiac output, an increase in left atrial and left ventricular end-diastolic pressures and congestion in the pulmonary circulation.
Which of the following manifestations occur with left-sided heart failure?
(Click on the three correct answers)
Chronic dry coughDyspneaRight upper quadrant discomfort Lack of appetite and bloatingParoxysmal nocturnal dyspnea
Porth, C.M., et.al., (2005)
Adaptive Heart Failure Mechanisms
The net effect of these neurohormonal responses is to:
1. Produce arterial vasoconstriction (to help maintain arterial pressure)
2. Venous constriction (to increase venous pressure)
3. Increased blood volume.
The cardiac reserve is maintained initially through systemic neurohormonal activation of the sympathetic nervous system and the renin-angiotensin-aldosterone mechanism.
Greenberg, B., Barnard, D. (2005)
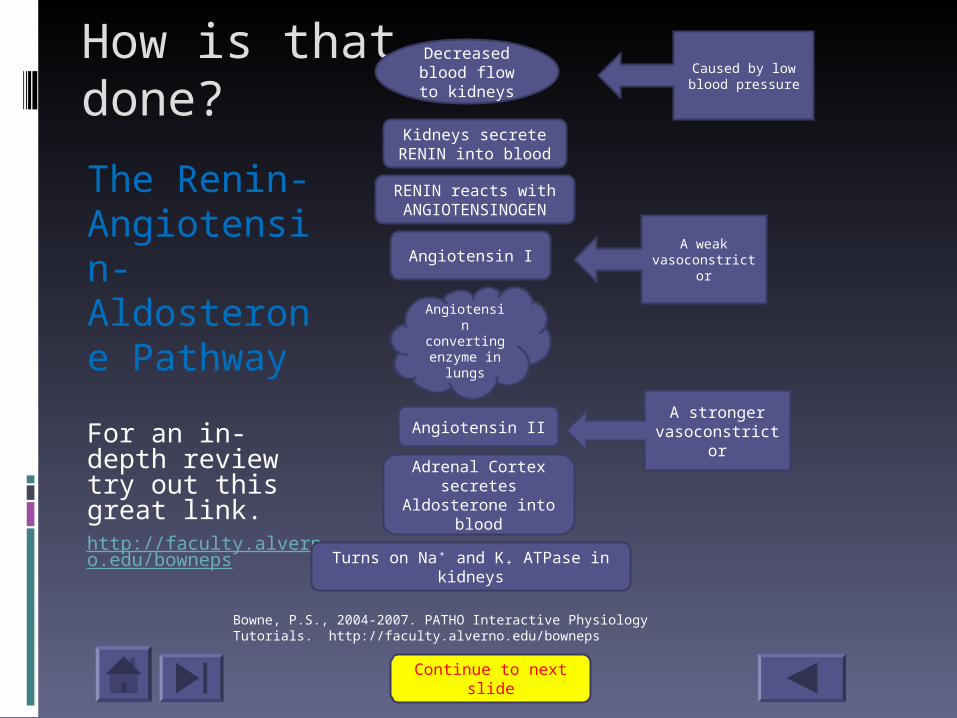
How is that done?
The Renin-Angiotensin-Aldosterone Pathway
For an in-depth review try out this great link. http://faculty.alverno.edu/bowneps
Decreased blood flow to
kidneys
Kidneys secrete RENIN into blood
RENIN reacts with ANGIOTENSINOGEN
A weak vasoconstrictor
Angiotensin I
Angiotensin converting enzyme in
lungs
Adrenal Cortex secretes
Aldosterone into blood
Turns on Na⁺ and K₊ ATPase in kidneys
Angiotensin II
Continue to next slide
A stronger vasoconstrictor
Bowne, P.S., 2004-2007. PATHO Interactive Physiology Tutorials. http://faculty.alverno.edu/bowneps
Caused by low blood pressure
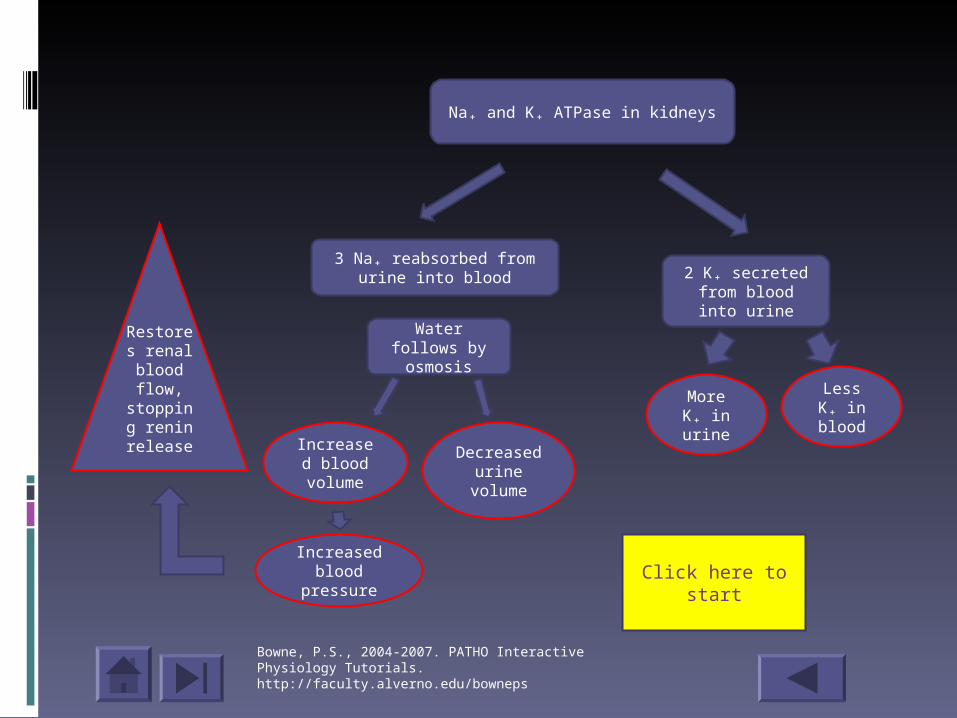
Na₊ and K₊ ATPase in kidneys
2 K₊ secreted from blood into
urine
3 Na₊ reabsorbed from urine into blood
Water follows by osmosis
Increased blood
volume
Increased blood
pressure
Decreased urine
volume
More K₊ in urine
Less K₊ in blood
Restores renal blood flow,
stopping renin
release
Click here to start
Bowne, P.S., 2004-2007. PATHO Interactive Physiology Tutorials. http://faculty.alverno.edu/bowneps
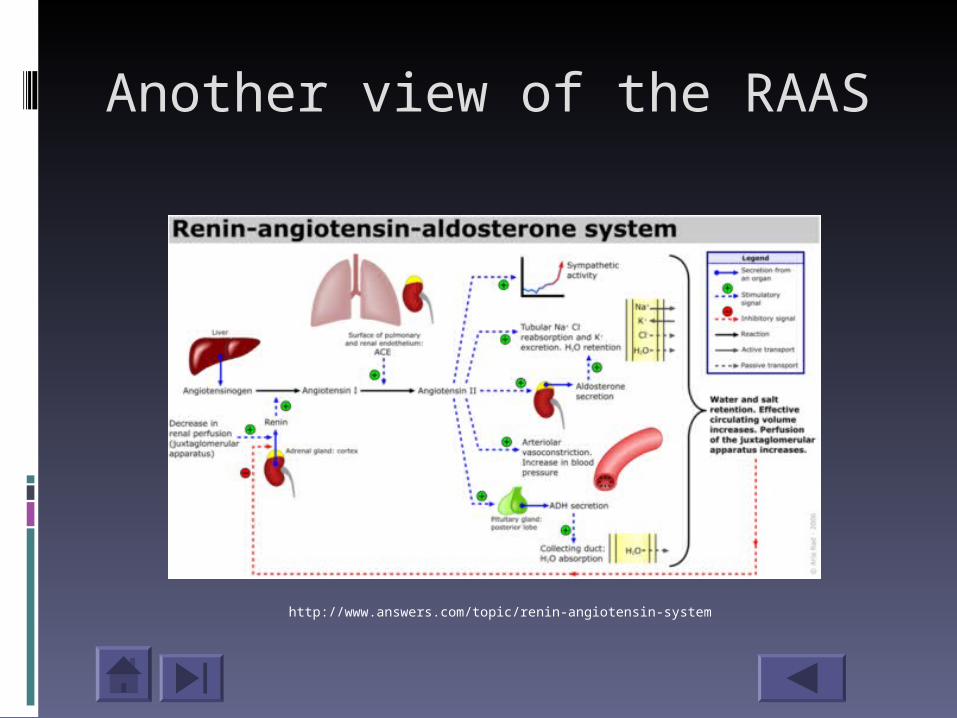
Another view of the RAAS
http://www.answers.com/topic/renin-angiotensin-system
When blood flow to the kidneys decreases, what directly turns on the Na⁺/K⁺ ATPase in the kidneys?
a. Angiotensin II
b. Aldosterone
c. Renin

Rethink your answer. Angiotensin II affects the Adrenal Cortex directly to secrete Aldosterone into the blood.
Back to the question

Great job! Aldosterone is secreted by the Adrenal Cortex and turns on the Na⁺/K⁺ ATPase in the kidneys.
Click to the next slide
Incorrect. The kidneys secrete renin, a large enzyme, into the bloodstream when there is a decreased blood flow to the kidneys. Renin acts on circulating Angiotensinogin to produce Angiotensin I (a weak vasoconstrictor).
Back to the question
Acute RAAS Effects
Acute effects of Angiotensin II are good and results in:
Enhanced CardiacOutput
Reduced Left
Ventricular filling
pressures
Porth, C.M.,et.al., (2005)Porth, C.M.,et.al., (2005)
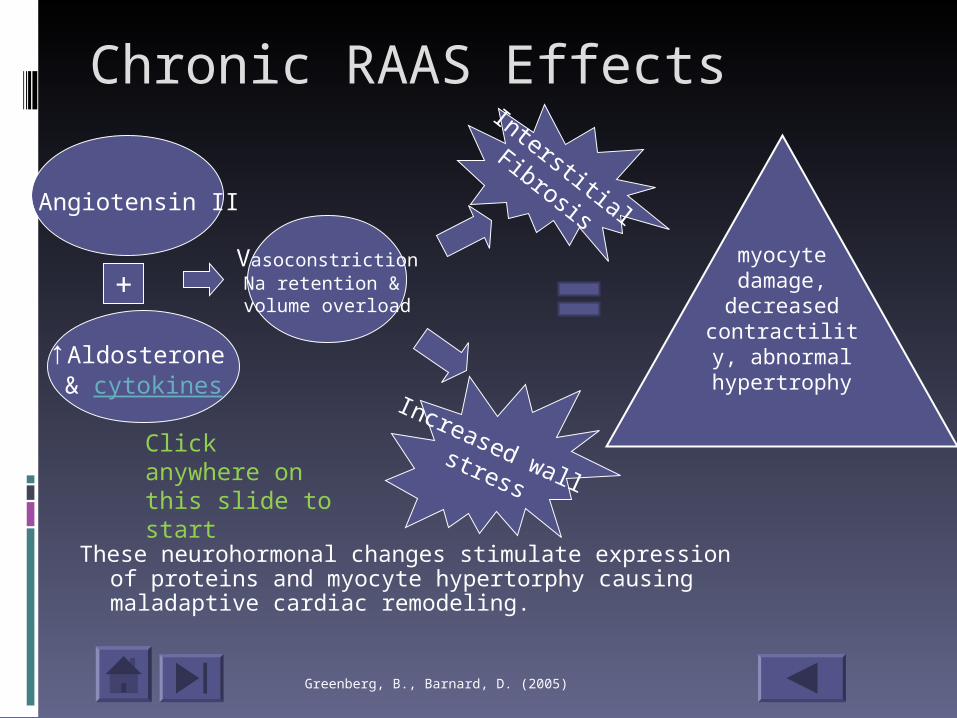
Chronic RAAS Effects
These neurohormonal changes stimulate expression of proteins and myocyte hypertorphy causing maladaptive cardiac remodeling.
↑Angiotensin II
↑Aldosterone & cytokines
VasoconstrictionNa retention &
volume overload+
Interstitial
Fibrosis
Increased wall stress
Click anywhere on this slide to start
Greenberg, B., Barnard, D. (2005)
myocyte damage,
decreased contractility,
abnormal hypertrophy
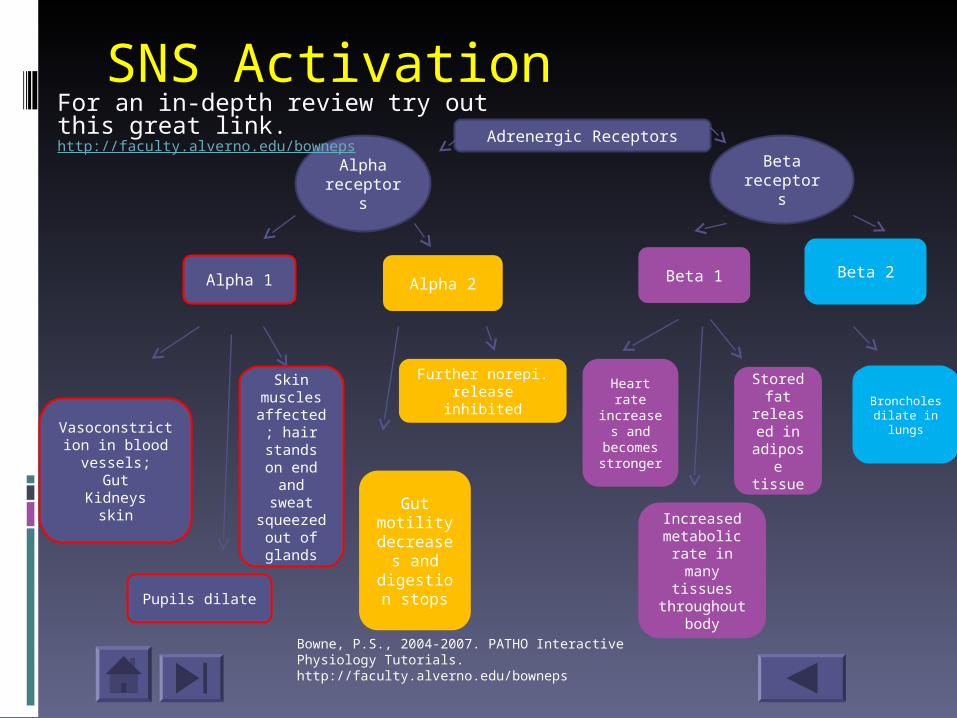
SNS ActivationAdrenergic Receptors
Alphareceptors
Beta receptors
Alpha 1 Alpha 2 Beta 1 Beta 2
Vasoconstriction in blood vessels;
GutKidneys
skin
Skin muscles affected;
hair stands on end and sweat
squeezed out of glands
Pupils dilate
Gut motility
decreases and
digestion stops
Further norepi. release inhibited Broncholes
dilate in lungs
Heart rate
increases and
becomes stronger
Stored fat
released in
adipose tissue
Increased metabolic
rate in many tissues
throughout body
For an in-depth review try out this great link.http://faculty.alverno.edu/bowneps
Bowne, P.S., 2004-2007. PATHO Interactive Physiology Tutorials. http://faculty.alverno.edu/bowneps
A B1 heart response from SNS activation
Has a positive inotropic effect on the heart
By increasing the Ca₊ that is available for interaction between the actin and myosin filaments the force of contraction improves.
Porth, C.M.,et.al., (2005)Porth, C.M.,et.al., (2005)
What happens throughout the body when the Sympathetic Nervous System is turned on? Choose 5 symptoms caused by the activation of the alpha receptors and 5 for the Beta receptors.
Alpha receptors Beta receptorsPupils dilateHeart rate increase
Stored fat released into bloodstream
Bronchioles dilate
Gut motility decrease
Hair on skin stands on end
Stronger heartbeat
Increase metabolic rate
Vasoconstriction in kidneys causing
decreased urine
Pallor, cold skin
Physiology of heart failure
Involves an interaction between two factors: A decrease in the pumping ability of the
heart with a consequent decrease in the cardiac reserve
The adaptive mechanisms that serve to maintain the cardiac output also contribute to the progression of heart failure.
Porth, C.M.,et.al., (2005)Porth, C.M.,et.al., (2005)
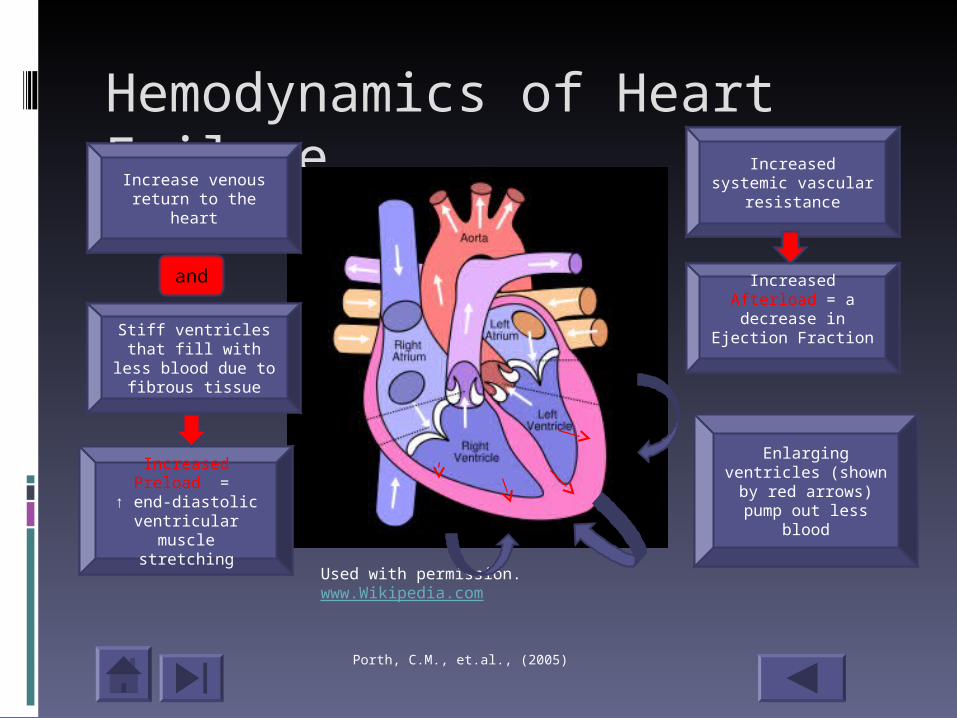
Hemodynamics of Heart Failure
Used with permission. www.Wikipedia.com
Stiff ventricles that fill with less blood
due to fibrous tissue
Enlarging ventricles (shown by red
arrows) pump out less blood
Increased Preload =
↑ end-diastolic ventricular muscle
stretching
Increased Afterload = a decrease in
Ejection Fraction
Porth, C.M., et.al., (2005)
Increase venous return to the heart
Increased systemic vascular resistance
and
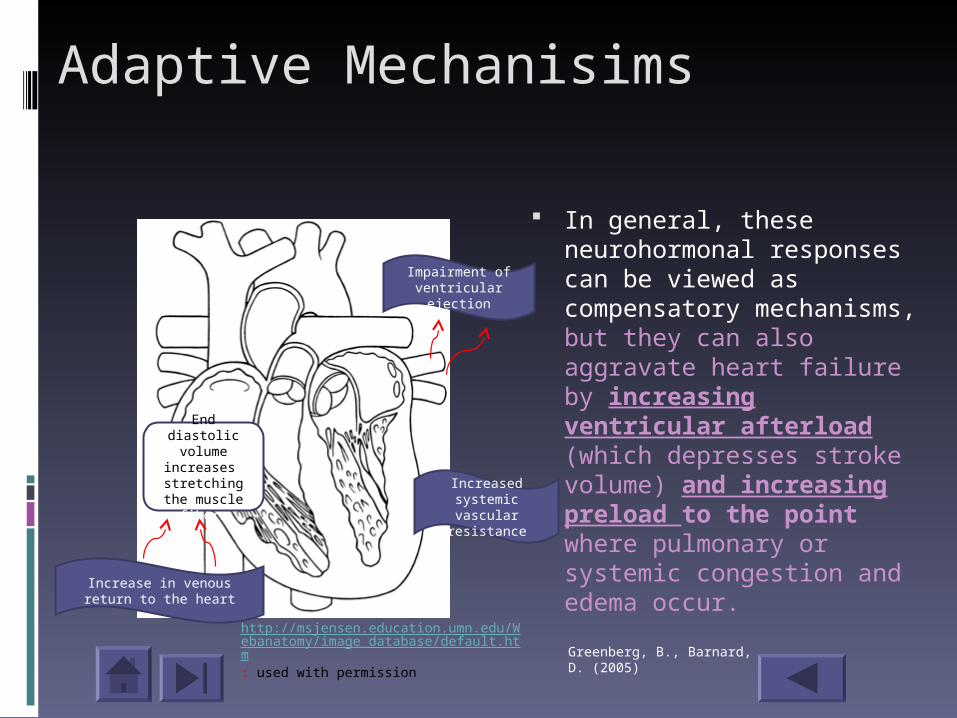
Adaptive Mechanisims
In general, these neurohormonal responses can be viewed as compensatory mechanisms, but they can also aggravate heart failure by increasing ventricular afterload (which depresses stroke volume) and increasing preload to the point where pulmonary or systemic congestion and edema occur.
End diastolic volume
increases stretching the muscle
fibers
Impairment of ventricular ejection
Increased systemic vascular
resistance
Increase in venous return to the heart
Greenberg, B., Barnard, D. (2005)
http://msjensen.education.umn.edu/Webanatomy/image_database/default.htm: used with permission
Cardiac Remodeling
It is manifested clinically by changes in cardiac size, shape, and function in response to cardiac injury or increased load.
The importance of remodeling as a pathogenic mechanism is incompletely understood, since factors leading to remodeling could be the major determinants of heart failure prognosis rather than ventricular dilation itself.
www.uptodate.com Cardiac Remodeling: Basic Concepts (2007)
Cardiac Remodeling
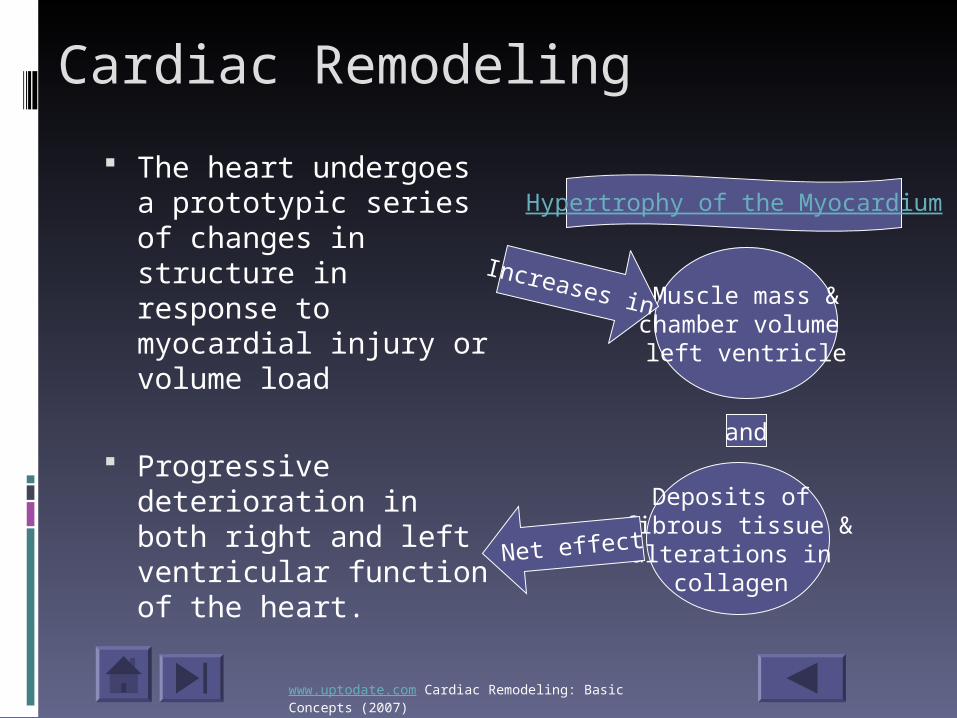
The heart undergoes a prototypic series of changes in structure in response to myocardial injury or volume load
Progressive deterioration in both right and left ventricular function of the heart.
Hypertrophy of the Myocardium
Muscle mass &chamber volume
left ventricle
Deposits of fibrous tissue &alterations in
collagen Net effect
and
Increases in
www.uptodate.com Cardiac Remodeling: Basic Concepts (2007)
Causes of Cardiac Remodeling Hemodynamic Factors
Pressure overload Volume overload
Neurohormonal Factors Angiotensin II Catecholamines Cytokines (tumor necrosis factor-a) Endothelin
Greenberg, B., & Barnard, D. (2005
Tumor necrosis factor-a
Tumor necrosis factor (TNF, cachexin or cachectin and formally known as tumor necrosis factor alpha) is a cytokine involved in systemic inflammation. TNF causes apoptotic cell death, cellular proliferation, differentiation, inflammation, and viral replication.
http://commons.wikimedia.org/wiki/Image:TNFa_Crystal_Structure.rsh.png#f Used under public domain
Back to the slide
Mann, D, Heart Failure; A Companion to Braunwald’s Heart Disease 2004
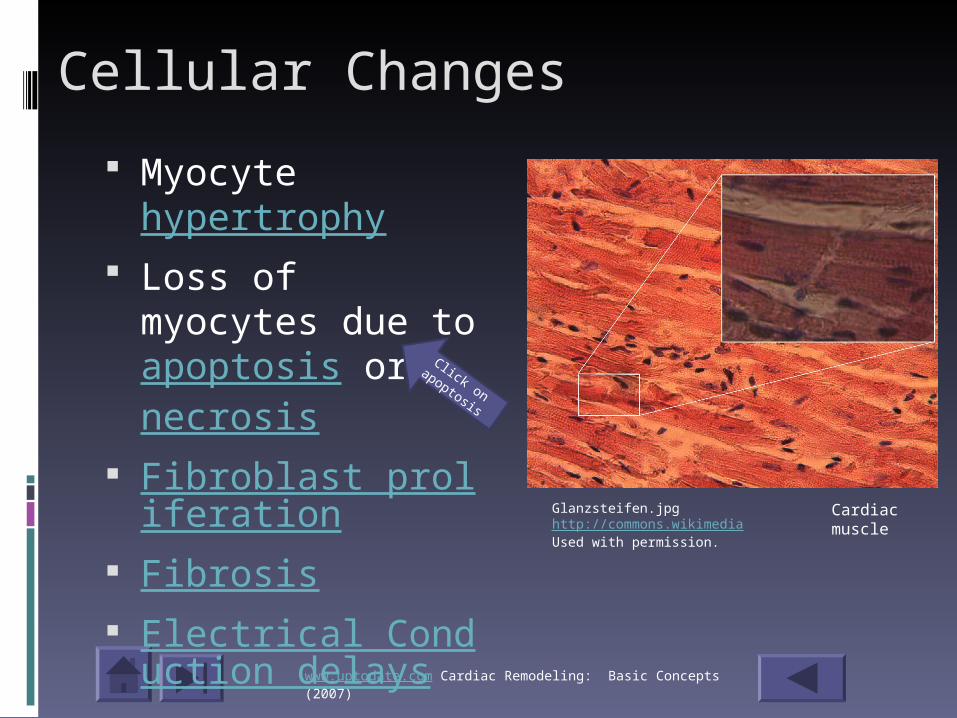
Cellular Changes
Myocyte hypertrophy
Loss of myocytes due to apoptosis or necrosis
Fibroblast proliferation
Fibrosis Electrical Conducti
on delays
www.uptodate.com Cardiac Remodeling: Basic Concepts (2007)
Glanzsteifen.jpg http://commons.wikimediaUsed with permission.
Cardiac muscle
Click on
apoptosis
Apoptosis
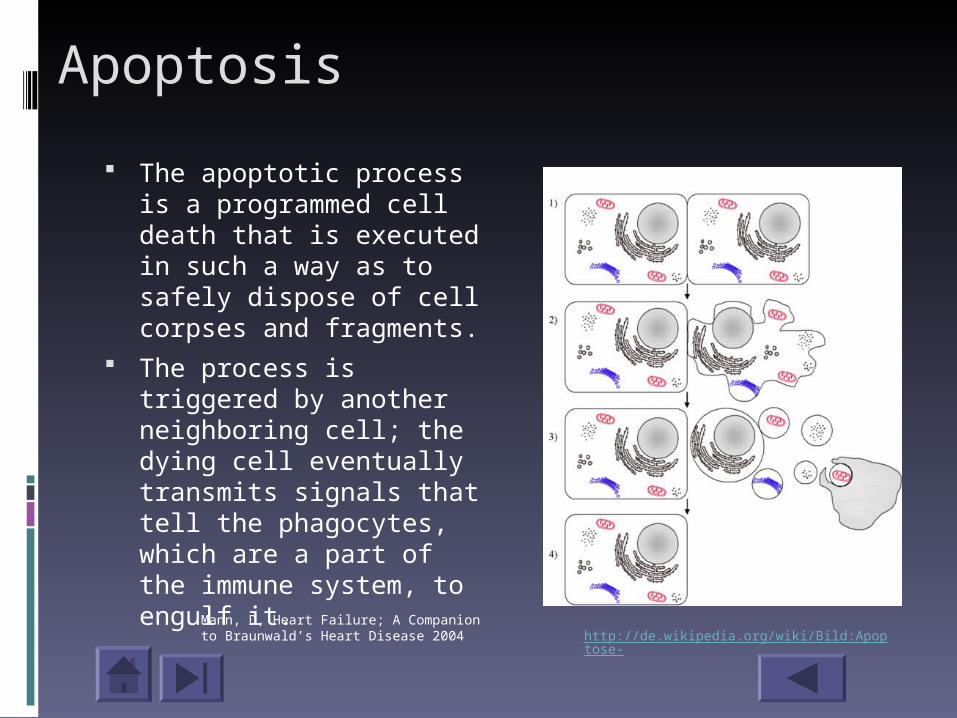
The apoptotic process is a programmed cell death that is executed in such a way as to safely dispose of cell corpses and fragments.
The process is triggered by another neighboring cell; the dying cell eventually transmits signals that tell the phagocytes, which are a part of the immune system, to engulf it.
http://de.wikipedia.org/wiki/Bild:Apoptose-Mann, D, Heart Failure; A Companion to Braunwald’s Heart Disease 2004
Voltage-gated ion channel
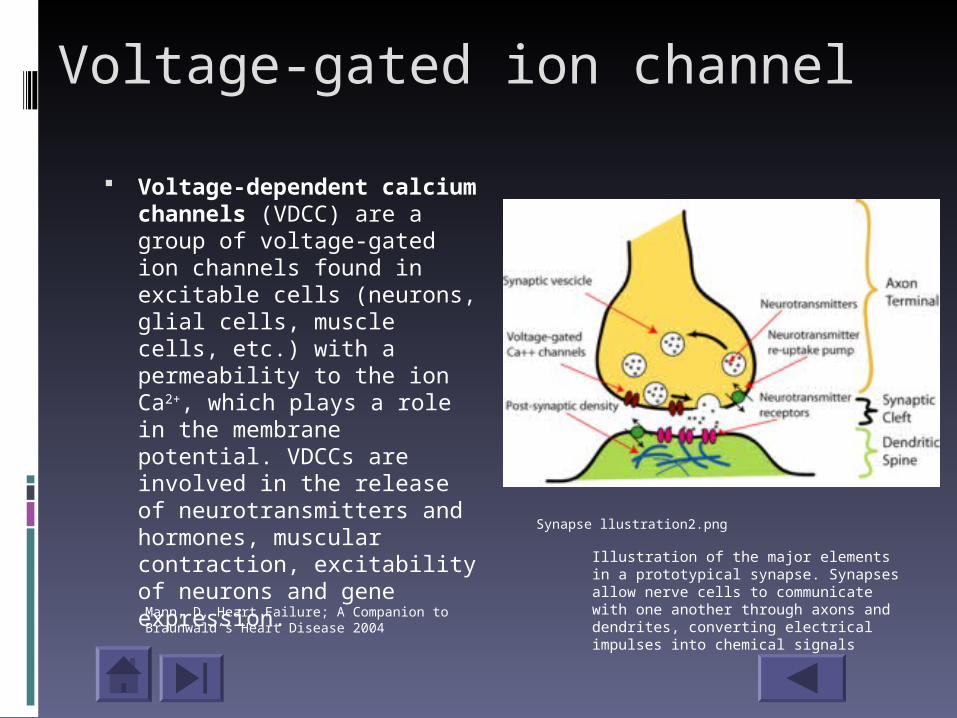
Voltage-dependent calcium channels (VDCC) are a group of voltage-gated ion channels found in excitable cells (neurons, glial cells, muscle cells, etc.) with a permeability to the ion Ca2+, which plays a role in the membrane potential. VDCCs are involved in the release of neurotransmitters and hormones, muscular contraction, excitability of neurons and gene expression.
Synapse llustration2.png
Mann, D, Heart Failure; A Companion to Braunwald’s Heart Disease 2004
Illustration of the major elements in a prototypical synapse. Synapses allow nerve cells to communicate with one another through axons and dendrites, converting electrical impulses into chemical signals
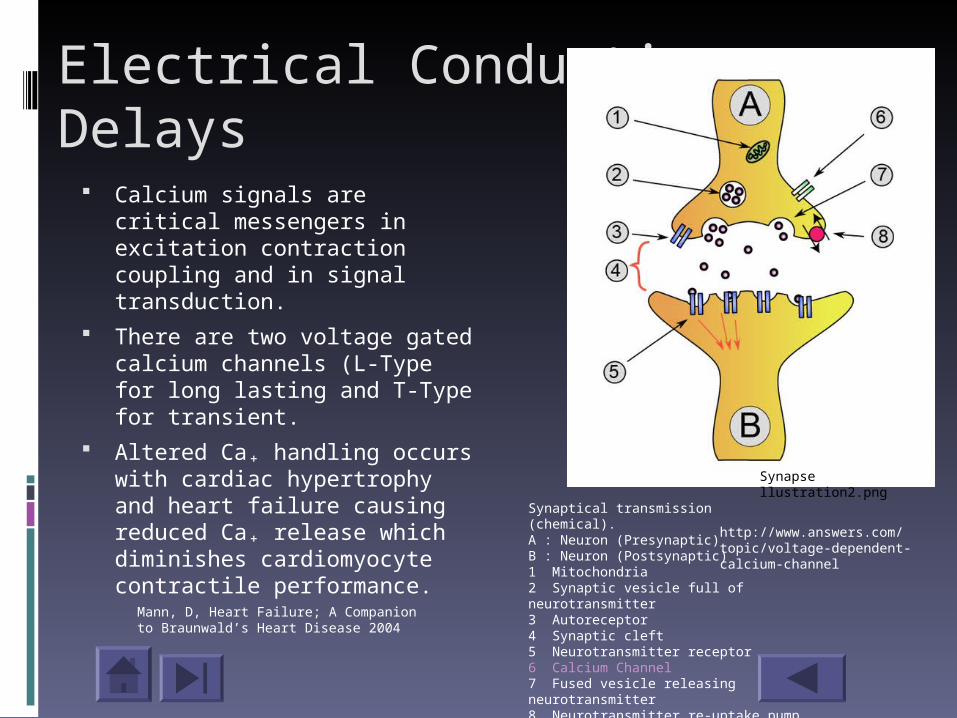
Electrical Conduction Delays
Calcium signals are critical messengers in excitation contraction coupling and in signal transduction.
There are two voltage gated calcium channels (L-Type for long lasting and T-Type for transient.
Altered Ca₊ handling occurs with cardiac hypertrophy and heart failure causing reduced Ca₊ release which diminishes cardiomyocyte contractile performance.
Synapse llustration2.png
http://www.answers.com/topic/voltage-dependent-calcium-channel
Synaptical transmission (chemical).A : Neuron (Presynaptic) B : Neuron (Postsynaptic)1 Mitochondria 2 Synaptic vesicle full of neurotransmitter 3 Autoreceptor 4 Synaptic cleft 5 Neurotransmitter receptor 6 Calcium Channel 7 Fused vesicle releasing neurotransmitter 8 Neurotransmitter re-uptake pump
Mann, D, Heart Failure; A Companion to Braunwald’s Heart Disease 2004

Summary of Heart Failure Pathophysiology
Myocardial Injury
Neuroendocrine activation (SNS, RAS)
Direct myocardial effects (remodeling,
LV dysfunction)
Disease progression
Hemodynamic abnormalities
(changes in pressure, volume and flow)
Symptomatology(exercise
intolerance)
MortalityGreenberg, B., & Barnard, D. (2005)
Neurohormonal Therapy
Strategies for the treatment of heart failure have focused on the use of agents that block angiotensin II production and the B-adrenergic system
Feldman, A.M., (2006)
Click here
ACE inhibitors work here to
prevent conversion
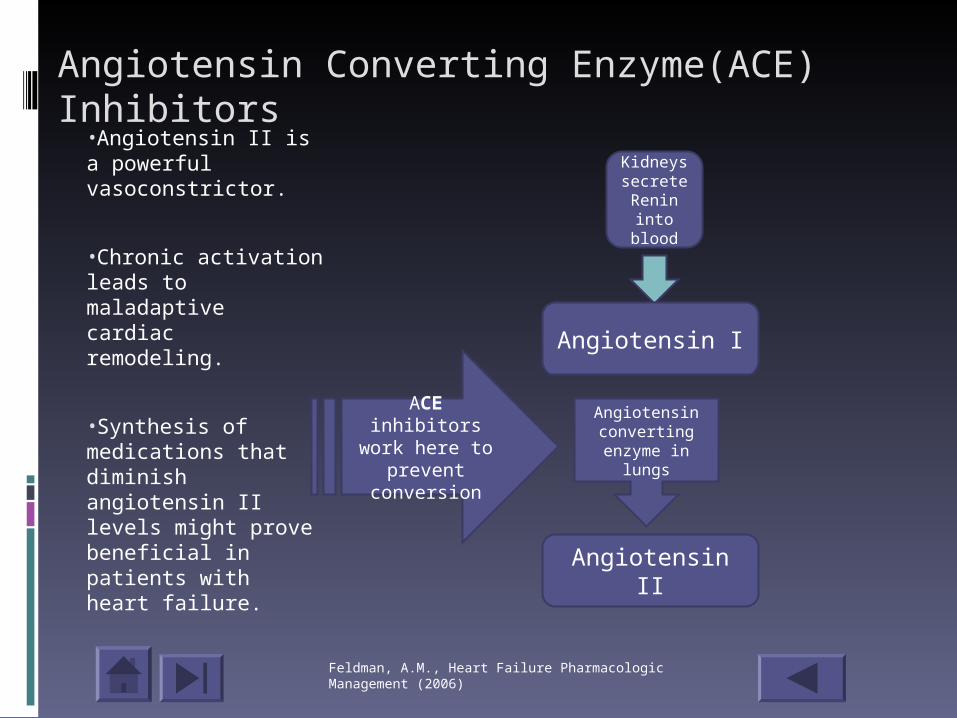
Angiotensin Converting Enzyme(ACE) Inhibitors
•Angiotensin II is a powerful vasoconstrictor.
•Chronic activation leads to maladaptive cardiac remodeling.
•Synthesis of medications that diminish angiotensin II levels might prove beneficial in patients with heart failure.
Angiotensin I
Kidneys secrete Renin into
blood
Angiotensin II
Angiotensin converting enzyme in
lungs
Feldman, A.M., Heart Failure Pharmacologic Management (2006)
FDA Approved ACE Inhibitors
Benazepril (Lotensin) Captopril (Capoten) Enalapril (Vasotec) Fosinopril (Monopril) Lisinopril (Prinivil) Moexipril (Aceon) Quiapril (Accupril) Ramipril (Altace) Trandolapril (Mavik)
Adverse Effects Hypotension Hyperkalemia Dry cough Acute renal failur
e Angioedema
FeldmanFeldman, A.M., Heart Failure Pharmacologic Management (2006)

Who should receive ACE Inhibitors?
ACE inhibitors should be used when: When there is any degree of
symptomatic heart failure Asymptomatic patients with left
ventricular (LV) dysfunction In patients at risk for developing LV
dysfunction
Feldman, A.M., Heart Failure Pharmacologic Management (2006)

Contraindications of ACE Inhibitors Angioedema Hypersensitivity (cough that’s intolerable)
Symptomatic hypotension Worsening renal function
Warn patients against use of nonsteroidal anti-inflammatory drugs as they can block favorable results of ACEI’s and can enhance its adverse effects.
Feldman, A.M., Heart Failure Pharmacologic Management (2006)
Click here
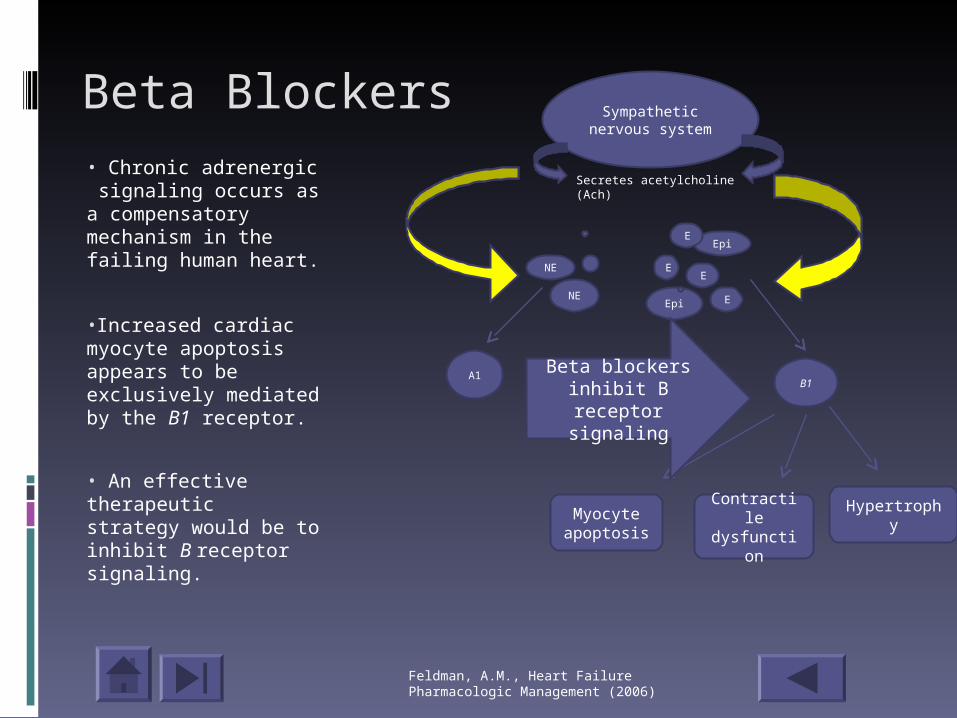
Beta Blockers• Chronic adrenergic signaling occurs as a compensatory mechanism in the failing human heart.
•Increased cardiac myocyte apoptosis appears to be exclusively mediated by the B1 receptor.
• An effective therapeutic strategy would be to inhibit B receptor signaling.
Sympathetic nervous system
Epi
Epi
E
E
E
NE
NEE
Secretes acetylcholine (Ach)
B1A1 Beta blockers
inhibit B receptor signaling
Myocyte apoptosis
Contractile dysfunction
Hypertrophy
Feldman, A.M., Heart Failure Pharmacologic Management (2006)
FDA Approved Beta Blockers
Adverse EffectsAV blockBronchospasmDizzinessHypotensionBradycardiaHypersensitivity
Metoprolol Bucindolol Bisoprolol Carvedilol Nebivolol
Feldman, A.M., Heart Failure Pharmacologic Management (2006)
Who should receive Beta Blockers?Beta blockers should be used when: In the presence of ACE inhibitor
therapy. Symptomatic left ventricular (LV)
systolic function. Post-infarct time period (even with
normal LV systolic function).
Feldman, A.M., Heart Failure Pharmacologic Management (2006)
Contraindications for Beta blockers Sinus node or conduction system
disease with bradycardia True reactive airway disease (COPD,
asthma, etc.) Abrupt discontinuation of Beta
blockers Cardiogenic shock Pulmonary edema
Feldman, A.M., Heart Failure Pharmacologic Management (2006)
Other medications
Diuretics Digitalis Aldosterone inhibitors Angiotensin Receptor Blocker’s
Feldman, A.M., Heart Failure Pharmacologic Management (2006)

Case Study #1
GB is a 54 year old black female who presented to the office for an initial exam. She reports shortness of breath and leg swelling. She has been experiencing nausea, vomiting and abdominal bloating over the past several weeks.
Case Study #1PMHx:Dyslipidemia
Severe Asthma (FEV1<80%)
Social:
Occasional smokerDenies alcohol
Caffeine, 1 cup/day
Minimal exercise
Married
Family Hx:
Premature heart disease
Medications:
Pantoprazole 40mg every day
ROS:
Dyspnea, bloating sensation
PE:
B/P 110/70, HR 74 Wt156. Lungs clear, Jugular vein distension (JVD) to jaw, ascites, edema +1 lower extremities, decreased urine output

Which is a risk factor for heart failure?
Choose all that apply Dyslipidemia Asthma 1 cup caffeine/day Family history of premature heart dis
ease

YEA! Dyslipidemia is a risk factor for heart disease and heart failure. Remember, this is a high ratio of total cholesterol to high-density lipoprotein cholesterol.
Click here for another choice
No, asthma is not a risk factor for heart failure.
Click here for another
choice
Caffeine, although constricts your blood vessels and increases your heart rate and blood pressure, is not a risk factor for heart failure.
Click here for
another choice
Correct, genetics is a risk factor for heart failure.
Click to get to next slide
Does GB have right or left-sided heart failure?
Click on the correct answer
Right-sided heart failure!
Left-sided heart failure!
Correct! Right –sided heart failure occurs when there is back up of blood in the venous system causing symptoms of abdominal bloating, ankle swelling and jugular vein distension.
Click here for
next slide
Think again! Look at all the s/s of GB, clear lungs, JVD, nausea, vomiting, and abdominal bloating, and ankle swelling. In this case, with clear lungs, her shortness of breath is caused by an enlarged liver and other abdominal organs that are pushing up on her diaphragm making it difficult for her to breath.
Click here to
try again

Which statement is true?
An increase in GB’s systemic vascular resistance caused an increase in her afterload leading to s/s of right-sided heart failure.
An increase in GB’s venous return to the heart caused an increase in her preload leading to s/s of right-sided heart failure.
This is not correct. The increase in systemic vascular resistance would make it harder for the left ventricle to pump blood out of the heart causing an increase in afterload.
Back to the
question
YEA! Great job! Increased venous return to the heart
increases end diastolic pressure in the ventricle causing cardiac muscle stretching and an increase in preload.

Which neurohormonal response created the preload? Renin-angiotensin-adlosterone
system
Sympathetic nervous system
Both the Renin-angiotension-aldosterone system and the sympathetic nervous system

You are partially correct. The aldosterone secreted from the adrenal gland turns on the Na⁺/K₊ ATPase which directly increased blood volume which increases the venous blood return to the heart.
Back to the
question
You are partially correct. The SNS alpha receptors do cause vasoconstriction to occur in the blood vessels of the gut, kidneys and skin which will increase venous blood return to the heart.
Back to the
question
Correct! You are putting it all together.
The Na/K ATPase is turned on during the renin-angiotensin-aldosterone sysstem causing increased blood volume and the SNS causes vasoconstriction to the blood vessels of the gut, kidneys and skin to increase venous blood return to the heart.
Would GB benefit from ACE or Beta blocker medications?
Choose one
ACE Inhibitor medication
Beta blocker medication
Both ACE inhibitors and Beta blockers
ACE inhibitor is the correct medication to use. Great job!
Click here for
next slide
Although a beta blocker is usually needed, this is not the right answer for GB. Try again.
Back to the
question
Severe Asthma
Click here to find GB’s medical history that could
contraindicate the use of beta blockers.
Usually this would be the correct answer. Think back. What does GB have in her medical history that could cause beta blockers to be contraindicated?
Back to the
question
Congratulations! You have completed the CHF tutorial. I hope you enjoyed it.
References
Bowne, P.S., 2004-2007. PATHO Interactive Physiology Tutorials. http://faculty.alverno.edu/bowneps
Colucci, W.S., (2007) . Pathophysiology of heart failure: Left ventricular pressure-volume relationships. Accessed through www.uptodate.com.
Demers, C., Mody, A., Teo, K., McKelvie, S. (2005). ACE Inhibitors in Heart Failure; what more do we need to know? American Journal Cardiovascular Drugs, 5 (6) 351-359.
Feldman, A.M., (2006). Heart Failure Pharmacologic Management. Malden, Ma: Blakewell Publishing.
Fuentes, V.L., (2007). Advances in Treatment of Heart Failure. WSAVA Congress. Accessed through http://www.vin.com/proceedings/Proceedings.plx?CID
Girod, S., Becker, A., Cardiac cell image accessed through http://commons.wikimedia . Retrieved April 23, 2007.
Greenberg, B.H., Barnard, D.D., (2005). Contemporary Diagnosis and Management of Heart Failure (3rd edition). Newtown, PA: Handbooks in Health Care Co.
References
Hebert, P.R., Foody, J.M., Hennekens, C.H. (2003). The Role of Inhibitors, Blockers, and Genetic Polymorphisms in the Treatment and Prevention of Heart Failure. Current Vascular Pharmacology.
Jensen, M., 1998-2006. WebAnatomy. http://msjensen.education.umn.edu/webanatomy/
Mann, D., et.al., (2004). Heart Failure; A Companion to Braunwald’s HEART DISEASE. Philadelphia, PA: Saunders.
Porth, C.M.,et.al., (2005). Pathophysiology; Concepts of Altered Health States (7th edition). Philadelphia, PA: Lippincott Williams and Wilkins
Sawyer, D., Colucci, W. (2004). Atlas of Heart Disease: Failure . Retrieved Apoptosis image April 23, 2007. http://de.wikipedia.org/wiki/Bild:Apoptose-german.png
Sheffield, S., 2000-6. GetBodySmart. ConceptCreators, Inc. http://www/getbodysmart.com/
www.wikpedia.com Heart images retrieved April 2, 2007.