Embed Size (px)
Citation preview

GEOGRAPHICAL ASPECTS OF CANCER INCIDENCE IN SOUTHEAST ASIA
R. W. ARMSTRONG
University of Hawaii at Manoa
Abstract-Based on limited information for incidence and mortality from one population based registry (Singapore) and a number of hospital registries there are important differences in cancer incidence between Southeast Asian countries. Cancers of the oral cavity, pharynx, and liver have high incidence throughout the region; cancer of the nasopharynx in Chinese. Cancers of the oesophagus and stomach have high relative incidence in Burma and in Singapore, and cancer of the lung in Singapore. Cancer of the uterine cervix is the most important female cancer in the region except in the Philippines and Singapore. Cancer of the breast has its highest Southeast Asian incidence in the Philippines and its lowest in Singapore. The importance of cancer as a cause of illness and death is increasing in Southeast Asia as a function of its changing age structure and the continued improvement in conditions that extend life expectancy and suppress communicable diseases.
INTRODUCIION
According to a 1979 estimate, Southeast Asia has a population of about 346 million in its 11 nations (Table 1) [ 11. In this Asian region, an estimated 300,000 people die annually of cancer. This figure rep resents 8% of deaths from all causes, a proportion that has been steadily increasing in recent years and one that may be expected to reach the level experi- enced in most developed countries (around 20%) by the end of this century. Cancer is thus emerging as a more prominent cause of death and illness in South- east Asia and the medical, public health, and social problems that accompany it draw an increasing share of resources and public concern [23.
includes papers on general cancer incidence in Indo- nesia [4] and in the Philippines [YJ. Studies on gen- eral patterns have been published elsewhere for Malaysia [6], the Philippines [7], and Singapore [8]. Among numerous studies that have been made on cancers of particular bodily sites in Southeast Asia are those on cancers of the mouth [9], nasopharynx [lo, 11,123, oesophagus [133, lung [14], liver [lS, 163, cervix uteri [ 171, Burkitt’s lymphoma [18], and leuke- mia [19]. Most of these reports are chiefly clinical in content and make only brief reference to possible etiology or to geographical aspects of epidemiology.
THE SE’ITING
The literature on the geographical aspects of cancer The variety and complexity of race, ethnicity and in Southeast Asia is restricted to short references in culture in Southeast Asia cannot be overstressed in articles on cancer epidemiology, pathology, immuno- attempting to describe the geographical patterns of genetics, clinical medicine, and surgery. The First cancer which affect its ~pulation. People of Mongol- Asian Cancer Conference in Tokyo in 1973 resulted in oid extraction predominate, with an estimated 93% of the publication of a major monograph [3], which the total population being Malay peoples, and 5.6%
Table 1. Selected demographic statistics for Southeast Asian nations, 1979”
Nation
Age groups Life Deaths Infant deaths
Total Under 15 Over 64 expectancy rate per rate per Urban population years years years at 1000 1000 live population (millions) “/, “/, birth population births 0’
/o
Brunei Burma East Timor Indonesia Kampuchea Laos Malaysia Philippines Singapore Thailand Vietnam Total Southeast
Asia
02 43 3 66 32.9 40 4 51 0.7 42 3 40
140.9 44 2 50 8.9 45 3 45 3.7 42 3 40
13.3 41 4 66 46.2 43 3 58
2.4 31 4 71 46.2 43 3 61 50.1 41 4 48
345.5 43 3 50
4 14 21 14
:zr 6
10 5 9
18 13
23 I40 I75 91
150 175 44 80 12 68
115 97
11 18 12 15 27 32
100 13 22 21
* From 1979 World Population Data Sheet, Population Reference Bureau [l].
299
55M 14 3D---r

300 R. W. ARMSTRONG
Chinese. Approximately OS’, is of Negrito ancestry, 0.1”: Indian, and 0.2”, other Caucasian and mixed racial groups. Indigenous cultures flourished in South- east Asia before Indian and Chinese influences from about the second century B.C. Although these and later imported cultures had profound influence, the indigenous cultures nevertheless continued to develop civilisations on strongly individualistic lines [ZO].
Today, the proportions of national populations made up of various ethnic groups varies widely. For example, in Malaysia, the Chinese comprise, 347,; of the total population and in Indonesia ZY& while in numbers there are 4.5 million Chinese in Mafaysia and 3.2 million in Indonesia. Both the Chinese and Indian populations in Southeast Asia have immense political, social and economic significance despite their comparatively small number and proportion in the region as a whofe.
The use of ethnic fabefs such as Mday, Chinese, and Indian may often be too genera1 to be useful in cancer epidemiology because of the masking of im- portant cultural differences that exist between more specific ethnicities. For example, among the Malay it is usual to distinguish between the Malay of the lMalay peninsula, the favanese,’ the Boyanese and the Filipino; among the Chinese the Cantonese (Guang- dong hual, Hakka (Kejia hua), and Hokkien (Fujian hual; and among the Indian the Tamil, Malayali, and Ceylonese.
The physical and cultural environments and behav- ioral patterns of the many societies in Southeast Asia are of extraordinary range. Isolated tribaf societies live as sma11 bands in mountain jungfes, and practice a subsistence kind of agriculture that has seen little change in centuries. The majority of people hve in rural village contexts with an economy based on rice or fishing, where traditional lifestyles predominate but with modern influences. Plantations of rubber, sugar, oilpalm, and tea, lumber camps and mines for baux- ite, tin, petroleum and other minerais are the context of tiving for a sizeable minority. The towns and cities house varying proportions of national populations (Table l), in a variety of industrial and commercial settings, and in extremes of poverty and affluence, and modern and traditional sty&s.
In examining the retative importance of genetic, en- vjronmental~ and behavioral risk factors for cancer in Southeast Asia the variety of ethnicities, cultures, and environments, and the paucity of detailed information on these subjects. poses a formidable research prob- lem in itself. Major differences in the incidence of specific cancers have been established for some South- east Asian populations but the relative importance of genetic. environmental. or behavioraf factors in their etiologies is unknown. Genetic factors appear to play a small role in almost all cancers. influencing indivi- dual susceptibility to environmental and behavioral risk factors, and predisposition towards cancers of certain sites. Southeast Asian populations offer many situations where different racial. ethnic, and cultural groups can be contrasted for genetic studies. Genetic mixing of populations through intermarriage between ethnic groups has generally been uncommon in most populations in the region although there are some situations as in Thailand and in the Philippines where considerable mixing has taken place. In recent years
there has been an increase in mixed marriages es- pecially in urban areas. For example. in modern Singapore since 1960. intermarriage between Chinese subethnic groups has become more frequent [S].
The recent emergence of cancer in Southeast Ana as a prominent disease owes more to environmental and behavioral changes that have taken place since 1950, especially from modern economic development and political independence. Improved nutrition. water supply. sanitation. vector control. housing, and medi- cal services are among the many elements that ha%-e contributed to a reduction in the incidence and sever- ity of communicable diseases and to the promotion of healthier longer lives for larger proportions of the population. These changes are reflected in lower total death rates and infant death rates. and increased years of life expectancy as compared to the rates of 1950 (Table 1). However. considerable variation prevails in these statistics between and within countries and in large part this is a reNection of the degree of econ- omic, urban, and social development, political stab- ility, and peace, that have been enjoyed in recent years.
Increased longevity alone has led to an increase in prevalence of degenerative diseases of all kinds. including cancer, because more people after 1950 were living to ages where these diseases become significant. There were also environmental and behavioral changes that directly and indirectly helped to change cancer incidence, increasing the frequency of some bodily sites of the disease and decreasing others. Most obvious was the adoptian of cigarette smoking on a new, vaster scaie. Alterations in diets included a greater variety of foods. more fresh foods, increased amounts of fats and proteins, and greater use of pro- cessed and refined foods with consequent reduced ex- posure to natural contaminants, such as molds, but increased exposure to artificial chemical additives. With the expansion of industry, agricufture and min- ing more people were exposed to a broader range of chemical carcinogens. lirban air pollution from motor vehicle and factory exhausts. and rural stream pollution from agricultural chemicals and wastes. have become major local problems that may have risk of cancer. The carcinogenic risks associated with par- ticular occupational settings in Southeast Asia would appear to be higher than in comparable settings in older industrialized countries because of lower prior- ity given to worker educrrtion, to industrial safetv. and to pollution control, by local governments and indus- trialists.
Information on cancer incidence and mortality for Southeast Asia is quite limited and what is available is not representative of the population as a whole. A large proportion of people with the disease are never discovered because for a variety of reasons they are not seen by medical services capable of making an accurate diagnosis. Many communities in Southeast Asia prefer traditiona medical practices rather than modern scientific ones, and the majority of the popu- lation lives in rural areas and often remote from the urban centers where the diagnostic skills exist. Cause of death is accurately determined for a small fractron

Geographical aspects of cancer incidence in Southeast Asia 301
of populations, principally in urban hospitals. Only in Singapore are the majority of deaths certified as to cause by a scientifically trained medical practitioner.
Positive confirmation of cancer is made through histopathology-the microscopic examination of a specimen of tissue or cells taken from a bodily site suspected of having new, abnormal and malignant growth. Diagnosis of less certainty is made through clinical observation, with or without surgery and by X-ray. It is accepted practice in studies of cancer inci- dence to use only reports of cases that have been positively confirmed by histopathology, but official statistics often report numbers of cases diagnosed by less reliable means.
In Southeast Asia, the majority of positively con- firmed cancers are diagnosed by means of biopsy or smear specimens taken by physicians in hospitals or clinics prepared for such work, and examined by pathologists in laboratories equipped for histopathol- ogy. The specimens from walk-in patients are taken from cancer sites that are more accessible, for example, the skin, head and neck, breast, lung, liver, cervix uteri, and peripheral lymph nodes. A bias in reporting of cancer frequency by bodily site is thus produced. Only a relatively small number of sus- pected cancer cases come to surgery and necropsies are rarely performed to confirm a diagnosis so the frequency of cancers of sites deep in the body is underreported. There is an acute shortage of well- qualified pathologists in most Southeast Asian coun- tries and at times the work loads imposed on the few available are extreme. Most countries have one cen- tral laboratory for histopathology, with additional smaller laboratories attached to major regional hospi- tals From time to time laboratories in one country are without the services of a pathologist and diagnos- tic work may then be sent to neighboring countries.
The method of recording cancer cases varies greatly in kind and quality from country to country. Most important are cancer registries which aim to record all details of interest in epidemiological research, in- cluding follow-up of patients after treatment. Then there are the records of patients in special cancer treatment clinics, such as institutes for radiotherapy, and in hospital patient record files. These records give clinical and treatment information but usually little about the history or lifestyle of patients or about events subsequent to treatment. The records of path- ology laboratories give accurate diagnoses of cancer cases but only identify the patient’s name, sex, age, ethnic group and referring physician or clinic. Finally, death certificates which have been certified as to cause provide limited information on mortality patterns.
Only Singapore has the combination of physician, surgical, and pathological services, population census, and administrative capacities to support a population based cancer registry. The cancer registry was estab- lished in 1968 and provides the most complete and reliable data on cancer incidence in the region. The nearest comparable registries are for the populations of three prefectures in Japan, Bombay (India) and New Zealand. Mortality statistics in Singapore are also of high quality. Over 85% of all death certificates are certified as to cause of death by medical practi- tioners [21].
The National Cancer Institute of Thailand has
established a hospital-based national registry which has compiled data from 125 collaborating hospitals since 1974 [22]. The Philippine Cancer Society and the Department of Health of the Philippines jointly established a central tumor registry in 1968 based on 24 hospitals in Metro Manila. The Disease Intelli- gence Center of the Philippines Department of Health also compiles statistics on cancer morbidity and mor- tality based on information gathered by field health personnel [7]. Cancer is a notifiable disease in the Philippines, as in most countries of the region, but underreporting of new cases and of deaths is believed to be considerable, especially in rural and isolated parts of the country. In Malaysia a national cancer registry has been proposed but not yet instituted. Two special registries, one for oral cancers and one for nasopharyngeal carcinoma have functioned in Malay- sia [9,23], but otherwise the sources of cancer data are pathological and hospital records, and death cer- tificates. Approximately one third of Malaysian deaths are certified by medical practitioners as to cause.
In all other countries in Southeast Asia cancer inci- dence data must at present be obtained from hospital and pathological laboratory records. These are re- stricted to the provincial capital cities in Indonesia, and to the national capitals in Brunei, Burma, East Timor, Kampuchea, Laos and Vietnam. Data for East Timor, Kampuchea and Laos have not been pub- lished, and for the other countries only scattered pub- lished reports are available.
It is not necessary, of course, to have complete population based registries for entire countries to pro- vide valid data for the study of cancer epidemiology. The excellent local regional registries throughout the world attest to this; in fact, national registries are unusual. But it is important to assess the validity of data from each registry when it may be applied to larger populations than the one on which the registry is based. The Singapore cancer registry represents an urban population of 2.4 million with an ethnic com- position of Chinese 76%, Malay lSo/, Indian 7% and other 2%. Cancer incidence patterns in Singapore are probably representative of Malay, Chinese and Indian populations in other major cities of Southeast Asia. To what extent they are representative of rural popu- lations of similar ethnic composition is not known. but available evidence would suggest that the relative incidence in bodily site of the disease does not vary greatly between urban and rural populations.
For the present, the Singapore registry provides the only comprehensive information by bodily site of dis- ease, and by age, sex, and ethnicity of patients to allow international comparisons, observation of time trends, and computation of survival rates. Studies of time trends and survival rates will become possible in the near future when data for the first decade of the registry are published.
CANCER INCIDENCE PATTERNS
Cancer incidence as reported by the Singapore Cancer Registry for 1968-72 is given in Table 2. These rates have been age-standardized to the world popu- lation and comparison with data from 80 other ethnic and national populations, as reported by 59 cancer

301 R. W. .&KISTROYG
Table 2. Incidence of cancers of sclectea sates in Singapore. 196&‘2. b! ethnic group and sex: Rates per 100.000 population per year*
ICDN Chinese Malays Indtans 8th rev. Site
141 Tongue 143 -145 Mouth
146 Oropharynx 147 Nasopharynx 148 Hypopharynx 150 Oesophagus 151 Stomach 153 Colon 154 Rectum 155 Lrver 161 Larynx 167 Lung 172 Skin. melanoma 173 Skin. other 174 Breast 180 Cervix utert IX1 Choriocarcinoma IX? Corpus uteri 183 Ovary 185 Prostate 187 Penis 188 Bladder 193 Thyroid 200 Lymphoma
14&‘09 ,411 sitest
3.6 I.2 5.9 1.1 3.1
254.1 6.156
1.9 ‘.I 1.5
15.7 0.9
30.1 44.3 11.9 10.0 34.2
7.5 56.9
0.6 6.6
Total No. cases
0.6 2.0 0.5 3.1 0.2 0.4 7.1 4.8 0.0 0.2 6.4 ’ 0
18.0 ;:2 9.5 3.1 7.0 4.7 8.0 IA.6
0.7 1.1 17.3 13.9 0.3 0.4 4.9 4.6
19.4 ~~~ 18.6 ~~ 0.9 4.9 6.0
4.x 0.1
2.0 3.6 4. I 0.9 1.4 2.3
153.1 91.4 4.430 354
0.0 1.1
0.0 0.6 0.3 3.7 9.7 3.6 7,
6.X 05 75
0.0 3.3
17.6 11.6 I I 3s 6.3
0.6 3.8 ‘6 -.
96.4 369
4: s.6 ‘X 0.9 1. I 5.6
25.X 5.0 6.4
1 I.4 5.3
IO.!) 0.4 77 _.
* Rates dre age-standardized to the World populatton. Data from Singapot-c C‘anier Registry in Waterhouse cr ul. [Zl].
t Excluding 173 skin cancer other than melanoma of the hkin.
registries [?I], gives some indication of the relative
importance of cancer in Singapore. and in turn an
approximation for Southeast Asia. Cancers of all sites
(except cancer of the skin). had an incidence rate of
254.1 per 100.000 population in Singapore male
Chinese. which ranks 18th in world registry data. The
highest reported rate in a male population is 345.9 per
100,000 from the African population of Bulawayo.
Rhodesia. Nevertheless. the Singapore rate for male
Chinese is at a similar level to United States and
European rates for males and considerably higher
than rates for Japan. In contrast. are the Singapore
rates for malt Indians and male Malays which are
among the lowest reported, ranking 7Xth and 79th.
respectively. In Singapore fcmalcs. Indians rank 49th.
Chinese 60th and Malays 78th. The highest reported
world female rate is 2X1.9 per I00.000 population. for
Caucasians in Hawaii. The low rates in Malay males
and females in Singapore are believed to be due in
part to lower utilization of hospital facilities leading
to an underreporting of casts [Xl. This factor may
also apply to Chincsc females. as compared to Chi-
nese males, and would help to explain the markedly
lower incidence rate in fcmalcs. On balance. the cur-
rent Singapore cancer experience is uvcrage among
developed and underdeveloped countries alike, but
with the likelihood that the Malay component 01
the population has incidence rates that are less than
average.
The five most common sites of cancer in Chmesc.
Malays and Indians arc shown in Table 3. The tnci-
dence rates for cancers of the liver m Chinese (both
sexes). of the oesophagus in Chinese (both sexes) and
Indians (female). and of the nasopharynx in Chinese
(both sexes) and Mala>s (male). are among the highest
reported in the world. Cancer of the lung. the most
common cancer in male Chinese. has an unusually
high incidence rate in female Chinese tn comparison
to other countries. Other less common cancers of the
head and neck also have their highest reported fre-
quencies in Singapore. The highest inctdences of
cancer of the tongue and cancer of the oropharknx
occur in Singaporean Indian females. and cancers of
the mouth and of the hypophary 111 111 Indians of both
scses. Cancer of the thyroid gland is also notably high
in Indian females.
Available comparattve data on cancer incidence in
seven Southeast Asian countries is given for malt and
female populations. respectively. in Tables 4 and 5. It
must be stressed that these percentages show only the
relative frequency with which c‘mccrs of various
bodily sttcs were rcportcd. The) ;trc not incidence
rates relative to total popultions. as arc the rates for
Singapore in Table 2. Rclativc inctdcnce percentages
have to be intcrprctcd with rcspcct to proportion of
national population covcrcd and nature of diagnostic
service. The percentage incidcncc ligures for Singa-
pore arc the most ;tccuratc for reasons discussed
above. and the proportions for the other countrtes arc
less rcpresentativs hecaus~ they arc hascd on hospital
records only where diapnusc\ arc chietlv of cancers
accessible to biopsy. Ncverthelcss. some patterns 01

Geographical aspects of cancer incidence in Southeast Asia 303
Table 3. Five most frequent cancers in Singapore, 1968-72, by ethnic group and sex: incidence rates per 100,000 in parentheses*
Chinese Malays Indians
Rank M F M F M F
1 Lung (56.9) Breast (19.4) Liver (14.6) Breast (17.6) Stomach (25.8) Cervix (29.8) 2 Stomach (44.3) Cervix (18.6) Lung (13.9) Cervix (11.6) Liver (11.4) Breast (25.5) 3 Liver (34.2) Stomach (18.0) Stomach (9.2) Stomach (9.7) Lung (10.0) Stomach (21.5) 4 Oesophagus (20.1) Lung (17.3) Nasopharynx (4.8) Lung (7.5) Mouth (8.6) Mouth (16.9) 5 Nasopharynx (18.7) Colon (9.5) Prostate (4.8) Liver (6.8) Rectum (6.4) Colon (13.0)
* Rates are age-standardized to the World population. Data from Singapore Cancer Registry in Waterhouse et al. [2l].
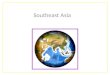
high incidence are clear and those cancer sites which are known to have higher frequency of occurrence in Southeast Asia are identified in Fig. 1.
Cancers of the oral cavity and pharynx have high incidence throughout the region for both males and females, especially in Indian populations. Cancers of the oral cavity, cheek, and lip are associated with the social custom of chewing betel, a practice common throughout Southeast Asia but especially in Vietnam, Laos, Kampuchea. Thailand, Malaysia, and the Philippines [24]. The betel quid that is chewed, and often left for long periods as a cud tucked in the cheek. is a mixture of areca nut, tobacco leaf, buyo leaf and lime containing several well-established carci- nogens. The practice is more common among poorer people in rural areas, but appears to be declining as the trend is for young people to take up cigarette smoking rather than betel chewing. Cancer of the nasopharynx has its highest incidence in the Chinese populations in all parts of the world, and within the subethnic groups the risk is highest for Cantonese, mid-range for Hakka. and lowest for Hokkien and
Teochiu [23]. Thus nasopharyngeal cancer is impor- tant wherever Chinese populations are settled in Southeast Asia. Because the Chinese live mostly in urban areas and utilize hospital services more than most other ethnic populations nasopharyngeal ‘cancer assumes a special prominence in Southeast Asia. This particular cancer has a moderate to high incidence in Malay male populations, and characteristically very low incidence in Indian and other Caucasian popula- tions (Table 2). Cancer of the larynx has an especially high incidence in Burma and Thailand [25].
Cancer of the oesophagus and stomach have high incidence in Burma and in Singapore, especially in Chinese and Indian populations. The high incidence of lung cancer in Singapore Chinese, especially females, has already been mentioned. Although ciga- rette smoking would appear to be a major factor in the etiology of lung cancer in males in Singapore, there is a large proportion of female lung cancer among non-smokers [14]. Cancer of the liver is prominent throughout Southeast Asia, especially in males, and in Thailand, Vietnam [26], and Singapore
Table 4. Relative incidence of cancer by site in selected Southeast Asian countries-Male
Total cases
Burma Indonesia (Rangoon) (Surabaya)
3450 659 Malaysia
1704
Philippines (Manila)
6771 Singapore Thailand Vietnam
6904 1733 3158
Buccal cavity and pharynx
Oesophagus Stomach Colon Rectum Liver Larynx Lung Bone Skin Prostate Lymphoma Leukemia Other
0
7.: 7”
29.0
0’
IG
9.2 14.5 2.7 2.3 *
7.7 7.4 3.1 2.7 0.8 3.7 1.3
36.8
0.2 0.3 0.9 1.5 *
5.2 8.5 0.2
14.6 0.3 4.4 3.0
31.9
4.9 5.0 2.6 4.9 3.9 3.5 7.5 1.8
12.9 1.8 2.0 0.1
31.1
% 16.0
0
1;;
1.6 6.6 6.5 15.8 4.1 4.2 4.2 3.9 8.0 13.1 2.2 2.7
13.5 19.7 4.0 0.6 4.3 2.5 5.1 1.3 6.5 1.5 3.1 3.1
20.9 13.9
2, 8.6
6.0 7.0 4.4 2.5
22.6 3.5
13.2 1.2 3.3 2.5 1.0 0.2
24.0
% 15.5
6.6 15.0 3.1 1.6 *
1.7 5.3 1.5 0.9 0.7 4.1 4.1
39.6
Years of record 1967
Data source
Hosp. Reference [II
* Not reported as separate site.
1964-68
Hosp.
PI
1969-71
Institute for Medical
Research
[61
1968-73 1968-72
Cancer Cancer Society Registry
c71 C2ll
1975
Nat. Cancer
Inst.
WI
1968-69
Hosp.
I?1

304 R. w. ,hMSTRONG
Table 5. Relative incidence of cancer by site in selected Southeast Astan countries-Female
Burma Indonesia Philippines (Rangoon) (Surabaya) Malaysia (Manila) Singapore Thailand Vtetnam
Total cases 3305 964 1676 9721 4962 1695 3969
Buccal cavity and pharynx
Oesophagus Stomach Colon Rectum Liver Larynx Lung Bone Skin Breast Cervix uteri Other uterus Lymphoma Leukemia Other
”
4.;
4.3 0.2 8.1 0.3 1.7 0.5 1.3 0.5 * *
2.2 1.0 4.6 0.6 2.6 0.1 1.5 7.9
19.1 23.0 24.4 31.7
4.0 2.3 1.5 2.3 1.2 1.9
19.4 17.0
0
ll.? 8.5 8.9 5.9
1.7 2.6 2.2 3.7 1.0 0.8 2.7 1.1 8.7
13.8 25.0
4.3 1.9
22.0
0.9 3.7 2.3 2.9 10.8 4.1 2.2 5.6 3.5 2.0 4.1 1.6 2.2 4.8 9.4 0.4 0.4 0.3 3.0 9.8 4.3 2.5 0.5 0.6 2.3 2.9 2.6
29.0 12.7 13.0 15.0 12.0 32.3 4.3 3.1 2.7 2.6 1.1 0.5 1.7 3.3 0.1
20.1 19.3 16.8
0
5.9 6.5
2.2 -.. >. I 2.3 1.5 *
0.4 2.1 1.1 I .o 9.1
34.0 5.6 2.5 3.0
‘3.0
Years of record 1967 196468 1969971 1968873 1968-72 1975 1968869
Data source
Hosp. Reference PI
* Not reported as separate site.
Surabaya Hosp.
PI
Institute for Medical
Research
C61
Cancer Cancer Society Registry
[71 c211
Nat. Cancer
Institute [22]
Hosp.
c21
in particular. In Thailand about 60% of cases of liver with the habit of eating raw fish. Cancers of the skin cancer are associated with cirrhosis, and SO?;, with occur with generally low incidence rates in most of liver fluke infestation [16]. The liver fluke. Opisfhor- Southeast Asia because of the protection afforded by this rirrrrini. is commonly found in Northeastern dark skin to actinic radiation. However. skin cancers Thailand and ingestion usually occurs in association occur with higher frequency in the Philippines and in
200 4cO 690 miles
Cervix
Ftg. I. Southeast Asia: Cancers of reported high incidence in national populations. and sources of cancer Incidence data.

Geographical aspects of cancer incidence in Southeast Asia 305
Indonesia than in the rest of the region. In the Philip- pines this is possibly due to larger proportions of the population with fair skin. while in Indonesia the higher frequency must be due, in part at least, to the present conditions of diagnosis which leads to an overreporting of the more superficial bodily cancer sites.
Cancer of the female breast has its highest inci- dence in Southeast Asia in the Philippines where rates are similar to those experienced in the United States. Elsewhere in the region cancer of the breast has low incidence rates in comparison to other countries. In Singapore the rates are. among the lowest reported by world cancer registries (Table 2). Cancer of the uterine cervix is the most prominent of the female cancers in all countries of Southeast Asia except in the Philip pines and Singapore (Table 5). This cancer is also the most important among Southeast Asian women in terms of potential control. A combined effort to expand periodic cytologic screening of female popula- tions, public education in hygiene, and improved domestic facilities for cleanliness has been suggested as a priority for reducing the risk of cervical cancer in the region [2].
GEOGRAPHICAL VARIATIONS
The incidence patterns suggest that there are some geographical variations between countries in South- east Asia in the frequency of certain bodily sites of the disease. Some of these variations are due to ethnic differences in the population, especially between Malays, Chinese, and Indians. Some of the variations are due to different socioeconomic conditions. For example, significant statistical differences were found in frequency among different sites of the disease in the cancer registry data from Metro Manila in the Philip pines in terms of education and outdoor occupations [7]. In males. cancers of the lung, pancreas, bladder, and prostate were associated with patients with school and college educations, while cancers of the mouth. oropharynx. oesophagus, stomach, and skin were associated with less education. In females, cancers of the lung. ovary. and breast were associated with higher levels of education and cancers of the mouth, tongue, and oropharynx with less. In both males and females cancers of the mouth and orophar- ynx were associated with outdoor occupations. These associations are in general agreement with those that have been reported by similar studies in other coun- tries [27]. As socioeconomic conditions improve, by modern indices. there is a decline in the incidence of cancers of the oesophagus and stomach and an in- crease in incidence of cancers of the colon. This trend is evident in Japan and can be expected to follow in Southeast Asia [2]. An isolated study of time-space relationships in patients with nasopharyngeal carci- noma as compared to a group of control subjects in Kuala Lumpur. Malaysia, found that the disease occurred more often among Chinese who followed more traditional lifestyles under poorer economic cir- cumstances. lived in older, poor quality housing in districts with more industry, heavier traffic. and least green space. and who ate less fresh foods and had little variety in meal patterns [28]. .
cancer in Southeast Asia is hampered by the lack of reliable incidence data for entire populations. For the present, detailed mapping of cancer incidence is there- fore not practicable except in limited circumstances. The known geographical variations are related to en- vironmental, behavioral, and possibly genetic factors, for example, climate, diet, occupation, education, tra- ditional customs, and ethnicity. The importance of cancer as a cause of illness and death can be expected to increase in Southeast Asia as a function of its present age structure and continued improvement in conditions that extend life expectancy and suppress communicable diseases. In turn, it becomes increas- ingly important to improve the availability of reliable data on cancer incidence and to refine our sketchy knowledge of geographical variations.
Acknowledgements-I wish to thank Dr M. J. Armstrong for reading and commenting on the paper in draft, MS Susan Ezawa for typing the manuscript, and Mr Tom Aaer for drafting Fig. 1.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Kesearch into geographical variations. as such. in 13.
REFERENCES
Population Reference Bureau. 1979 World Population
Data Sheer. Washington, D.C., 1979. Hirayama T. Strategy for cancer control in Asia. In Cancer in Asia (Edited by Hirayama T.), p. 1. Gann Monograph on Cancer Research No. 18. University of Tokyo Press, Tokyo, 1976. Hirayama T. (Ed.) Cancer in Asia. Gann Monograph on Cancer Research No. 18. University of Tokyo Press, Tokyo, 1976. Pringgoutomo S. Some aspects of the problem of cancer in Indonesia. In Cancer in Asia (Edited by Hir- ayama T.), p. 247. Gann Monograph on Cancer Research No. 18. University of Tokyo Press, Tokyo, 1976. Basa G. F. and Cruz-Basa A. G. Cancer control in the Philippines: problems and approaches. In Cancer in Asia (Edited by Hirayama T.). p. 287. Gann Mono- graph on Cancer Research No. 18. Universitv of Tokyo Press, Tokyo, 1976. Armstrong R. W. and Ahluwalia H. S. Cancer inci- dence in Malaysia. Natn. Cancer Insr. Mongr. 53, 53. 1979. Basa G. F., Hirayama T. and Cruz-Basa A. G. Cancer epidemiology in the Philippines. Natn. Cancer Inst. Monogr. 47, 45, 1977. Shanmugaratnam K. Cancer in Singapore+thnic and dialect group variations in cancer incidence. Singapore Med. .I. 14, 69, 1973. Ramanathan K. and Lakshimi S. Oral carcinoma in Peninsular Malaysia: racial variations in the Indians, Malays, Chinese, and Caucasians. In Cancer in Asia (Edited by Hirayama T.), p. 27. Gann Monograph on Cancer Research No. 18. University of Tokvo Press, Tokyo, 1976. Muir C. S. and Shanmugaratnam K. (Eds) Cancer of the Nasopharynx, Vol. I. UICC Monograph Series. Munksgaard, Copenhagen, 1967. Shanmugaratnam K. Studies on the etiology of naso- pharyngeal cancer. In Infernational Review qf Experi- mental Pathology, Vol. 10 (Edited by Richter G. W. and Epstein M. A.), p. 361. Academic Press. New York, 1971. Ho J. C. H. Nasopharyngeal carcinoma. In Advances in Cancer Research, Vol. 15 (Edited by Klein G. and Weinhouse S.), p. 57. Academic Press, New York. 1972. deJong U. W.. Breslow N.. Goh Ewe Hong J.. Srid-

306 R. W. .kMSTRONG
14.
15.
16.
17.
18.
19.
20.
21.
haran M. and Shanmugaratnam K. Aetiological factors in oesophageal cancer in Singapore Chinese. Inr. J. Cuncer 13, 291. 1974. MacLennan R., Da Costa J.. Day N. E.. Law C. H., Ng 22. Y. K. and Shamugaratnam K. Risk factors for lung cancer in Singapore Chinese. a population with high 23. female incidence rates. Int. J. Cancer 20, 854, 1977. Muir C. S. Cancer of the liver, pancreas, and perito- neum in Singapore. Br. J. Cancer 15, 30. 1961. Stitnimankarn T. Primary hepatic carcinoma in Thai- 24. land. In Cancer in Asia (Edited by Hirayama T.), p. 123. Gann Monograph on Cancer Research No. 18. University of Tokyo Press, Tokyo, 1976. 25. Chan L. K. C. The problem of uterine cervical carci- noma in Singapore and West Malaysia. Singapore Med. J. 11, 140. 1970. 26. Ramanathan K. Burkitt’s lymphoma in West Malaysia. Southeast Asian J. Trop. Med. Pub/. Hlrh 3, 249, 1972. Kwa S. B.. Siang S. C., Hanam E.. Chen B., Boo T. N., 27. Kit C. S., Paul F., Khow L. S. and Tan D. Leukemia in Singapore. Singapore Med. J. 9, 133, 1968. 28. Hall D. G. E. A History of South-East Asia, 3rd edn. Macmillan, London, 1968. Waterhouse J., Muir C. S., Correa P. and Powell J.
(Eds) Cancer Incidence in fire Conrlnrms. Vol. III. In- ternational Agency for Research on Cancer. Scientific Publications No. 15. Lyon. 1976. Thailand. Ministry of Public Health. National Cancer Institute. Cancer Starisrics IY7.S. Bangkok, 1978. Armstrong R. W., Kannan Kutty M.. Dharmalingam S. K. and Ponnudurai J. R. Incidence of nasopharyn- geal carcinoma in Malaysia. 1968-1977. Br. J. Came, 40, 557, 1979. Hopps H. C. Geographic pathology. In Parholog!,. 7th edn (Edited by Anderson W. A. D. and Kissane J. M.). p. 712. Mosby, St. Louis, 1977. Menakanit W., Muir C. S. and Jain D. K. Cancer in Chiang Mai, North Thailand. A relative frequency study. Br. J. Cancer 25, 225. 1971. Vu C. H., Nguyen V. P., Vi H. T., Nguyen V.. Dinh T. B. and Tran P. H. Le cancer du foie au Nord Viet- nam. Vietnam Med. (Hanoi) 87, 1963. Fraumeni J. F. (Ed.) Persons ar High Risk of Cancer. Academic Press, New York. 1975. Armstrong R. W., Kannan Kutty M. and Armstrong M. J. Self-specific environments associated with naso- pharyngeal carcinoma in Selangor. Malaysia. Sot. Sci. Med. 12D, 149, 1978.