Embed Size (px)
Citation preview
Geoffrey L. Rosenthal, MD, PhD November 9, 2010
Financial conflicts of interest: None
Identify most severe forms of cardiovascular disease in children
Discuss diagnosis and treatment of these disorders
Provide insight into the pervasiveness of “medicine” in the lives of families
Discuss functional limitations/expectations for children with these diagnoses
Address emerging science and research
Reduce backlog of cases by fast tracking applications
Reduce administrative costs of processing claims
Develop “List” of diagnoses which better discriminate children meeting cardiovascular disability criteria
Maintain a low rate of denying benefits when they should be allowed, and of allowing benefits when they should be denied
Identify diseases that are certain or near certain to cause disability or death within 12 months
Identify diseases that, by definition, cause disability
Single ventricle Hypoplastic Left Heart Syndrome (HLHS)▪ Aortic valve atresia
Tricuspid valve atresia Pulmonary atresia with intact ventricular
septum (PAIS or PAIVS)Long QTc Syndrome with aborted
sudden deathChildhood myocardial infarctionHeart transplantation
“Palliated” Cardiovascular Malformations, and “Repaired” Malformations with lifelong sequelae Single ventricle and complex two ventricle
lesions Channelopathies Cardiomyopathies Congenital Heart Disease with
comorbiditiesCongenital Heart Disease requiring specific
treatments/events
Hypoplastic left heart syndrome (HLHS) Aortic atresia, Mitral atresia, AA/MA
Pulmonary atresia with intact ventricular septum
Tricuspid atresia (all subtypes) Unbalanced atrioventricular canal (all
subtypes) Double inlet left ventricle Some forms of double outlet right ventricle Single ventricle with indeterminate
morphology
Diagnostic determination of single ventricle can be made with a very high degree of certainty using echocardiography
Resting cyanosis (paO2 < 60 Torr) pre-op and post-op while infants
Clinically significant risk of death in the first year of life (approximately 10-50+%)
Usually require 3 or more hospitalizations in first year of life for diagnosis, stabilization, surgery, and/or cardiac catheterization
Tetralogy of Fallot With pulm. atresia, absent pulm. valve syndrome,
discontinuous or hypoplastic pulm. arteries Transposition of the great arteries (d-TGA and
l-TGA, with or without other cardiac lesions) Pulmonary atresia with ventricular septal
defect and multiple aortopulmonary collaterals
Remaining forms of double outlet right ventricle
Critical aortic valve stenosis Shone’s complex Critical pulmonary valve stenosis
Total anomalous pulmonary venous return (all types)
Interrupted aortic arch (all types) Truncus arteriosus (all types) Ebstein’s anomaly diagnosed in
infancy (with or without associated lesions)
Heterotaxy syndrome (all types) Pulmonary vein stenosis/sclerosis
involving 2 or more pulmonary veins
Diagnosis of complex two ventricle lesions can be made with a very high degree of certainty using echocardiography
Precise anatomical diagnosis may require cMRI or cardiac catheterization
Resting cyanosis (paO2 < 60 Torr) pre-op for most, low cardiac output for remaining
Clinically significant risk of death in the first year of life (approximately 5-50+%)
Usually require 2 or more hospitalizations in first year of life for diagnosis, stabilization, surgery, and/or cardiac catheterization
Hospitalizations are often prolonged (LOS > 2 weeks)
Sequelae, residual lesions, need for nutritional support, need for home care is common
Long QT syndromesBrugada syndrome variantsAtrial arrhythmia syndromesShort QT syndromeCatecholaminergic ventricular
tachycardia
Diagnosis very reliable when based upon clinical features, family history, ECG, heart rhythm assessment, and genetic testing
Clinically significant risk of arrhythmia, syncope, and death
Most require medications and lifestyle modifications
Many have associated developmental/functional disabilities
Most require electrophysiology procedures, pacemaker, and/or internal cardioverter-defibrillator
Devices require lifestyle modification to prevent lead fracture and device malfunction
Devices may be associated with psychological symptoms (body image, anxiety, depression)
Often limit age-appropriate abilities at home, in school, and in the community
Hospitalizations may be prolonged (LOS > 2 weeks)


Autosomal, Gonosomal, or Mitochondrial Acquired (infectious, post-infarction,
post-bypass, toxic, nutritional) Dilated Hypertrophic Restrictive Arrhythmogenic right ventricular
dysplasia Many occur within defined systemic
syndromes
Anomalous left coronary arising from the pulmonary artery (ALCAPA)
Kawasaki Disease with coronary artery aneurysms
Anomalous left coronary arising from the right cusp and passing between the aorta and the pulmonary artery
The causes of myocardial infarction in children are different than in adults, but the outcomes are similar
Diagnosis very reliable when based upon clinical features, physiological assessment, family history, echocardiography, and genetic testing
Significant risk of arrhythmia, syncope, and sudden death
Most require medications, lifestyle modifications
Most have significant functional limitations Many have associated developmental
disabilities Some require palliative surgery, internal
cardioverter-defibrillator
Pediatric Heart Transplantation – Medical Urgency Status Codes
Status 1A and 1B patients meet criteria for compassionate allowance prior to transplant
Status 1A - “Registrant less than 18 yrs of age and meets at least one of the following criteria: (a) requires assistance with a ventilator; (b) requires assistance with a mechanical assist device; (c) requires assistance with a balloon pump; (d) is less than 6 months old with congenital or acquired heart disease exhibiting reactive pulmonary hypertension at greater than 50% of systemic level; (e) requires infusion of high dose or multiple inotropes; or (f) meets none of the criteria specified above but has a life expectancy without a heart transplant of less than 14 days”
Status 1B - “Registrant who (a) requires infusion of low dose single inotropes, (b) is less than 6 months old and does not meet the criteria for Status 1A, or (c) exhibits growth failure (see OPTN policies for definition).
Prematurity <37 weeks gestation Neuroradiographic signs of injury Microcephaly Post-operative seizures Developmental delay identified before
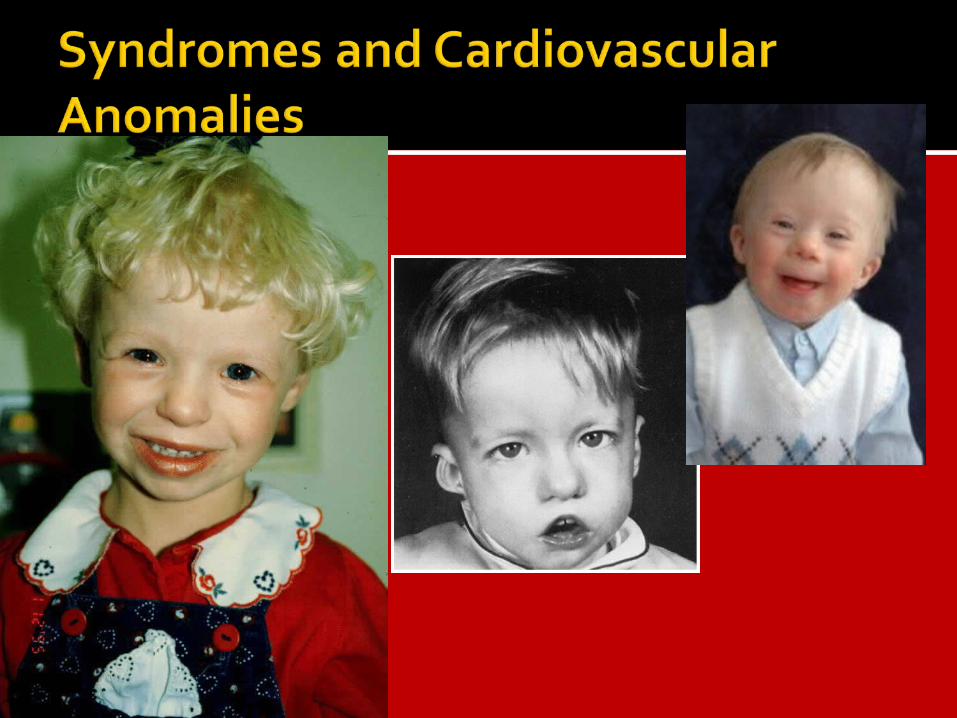
1 year of age Multiple congenital anomalies Syndromes associated with
developmental delay and functional impairment (Down, Williams, DiGeorge, CHARGE, Noonan, Jacobsen)
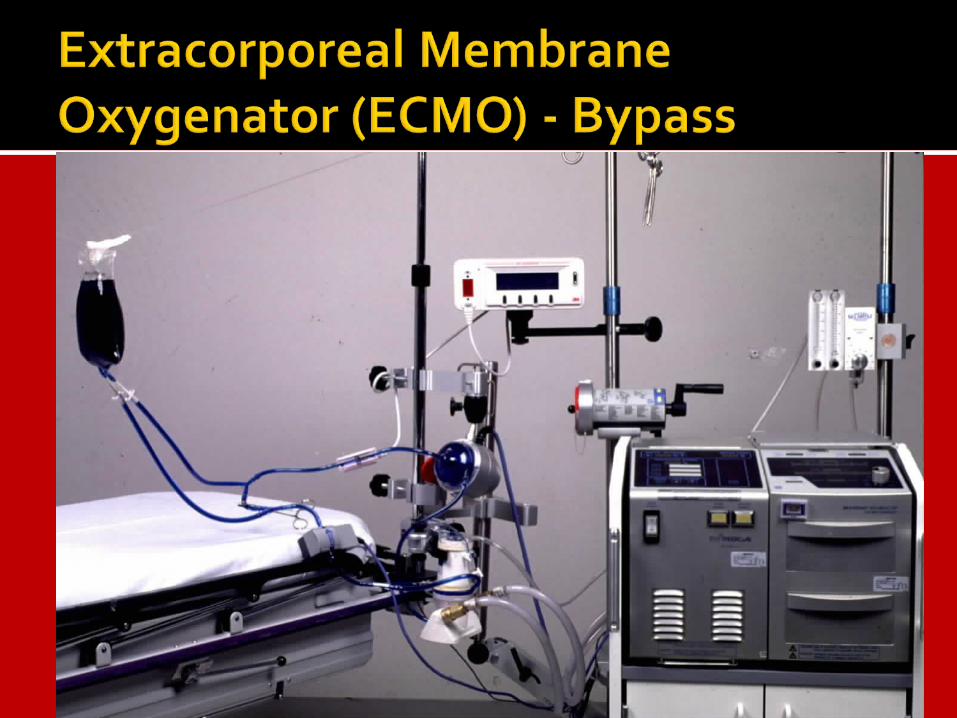
Length of stay in ICU > 2 weeksNeed for Cardiopulmonary
resuscitationNeed for mechanical circulatory
support (ECMO, VAD)Need for tracheostomyNeed for continuous infusion of
pulmonary vasodilators or inotropes
Prior fetal intervention

Thank you, Questions?