Embed Size (px)
Citation preview
Genomic Evaluation Meetings - effective reporting of challenging variants
Olivera Spasic-Boskovic, Philip Twiss, Harjeet Rai,
Richard Sandford, Stephen Abbs
East Anglian Medical Genetics Service and Clinical Genetics
Addenbrooke’s Hospital, Hills Road, Cambridge, CB2 0QQ
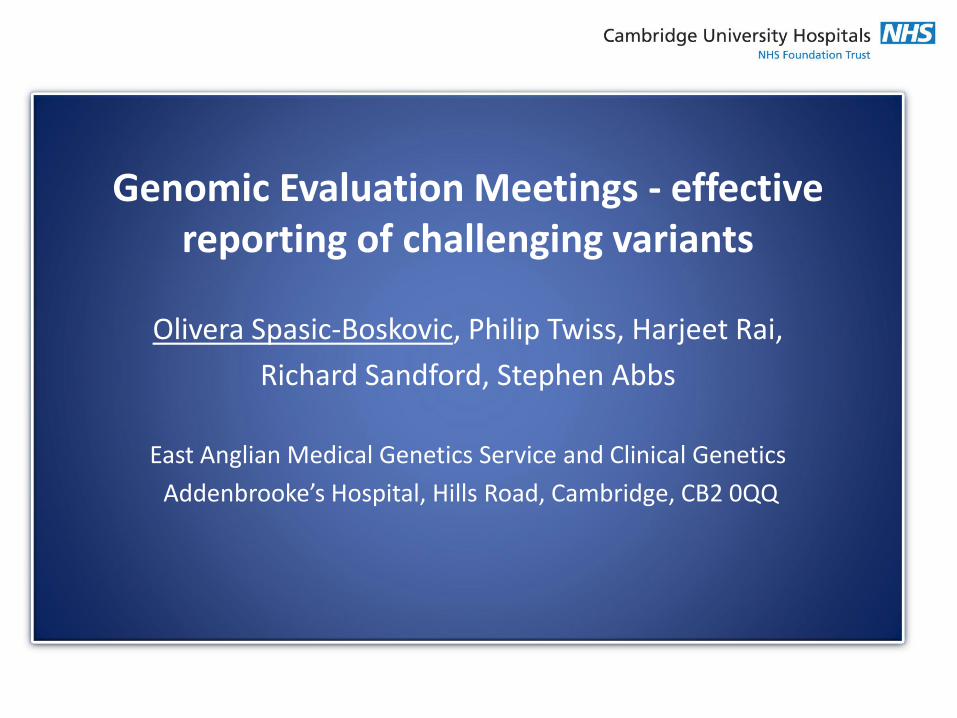
•Introduced for routine testing (Feb. 2014)
•Illumina TruSight One sequencing panel
•Targets 4,813 genes (62,000 exons)
•Over 2800 diagnostic tests performed
•Ability to test for large number of conditions
•Flexible and responsive to clinical referral
•Panels visible and readily accessible via (www.geneadviser.com)
OMIM
GEMINI - CE Genomic Medicine Innovative Initiative – Clinical Exome
20,000
GENES
5,000 CLINICALLY RELEVANT
• June 2015 - May 2016
• 16 sessions • 88 cases were presented and discussed • 123 variants • 75% of referrals were from our Clinical genetics • 15% External (out of East Anglia region) • 6% from other Addenbrooke’s departments • 4% from other hospitals in East Anglia
Genomic Evaluation Meetings (GEMs)

20% neurology
GEM discussed variants/panel
42% cardiac panels
14% other
0% 20% 40% 60% 80% 100%
missense
splice site
stop
frameshifts
synonymous
other
The most common changes discussed:
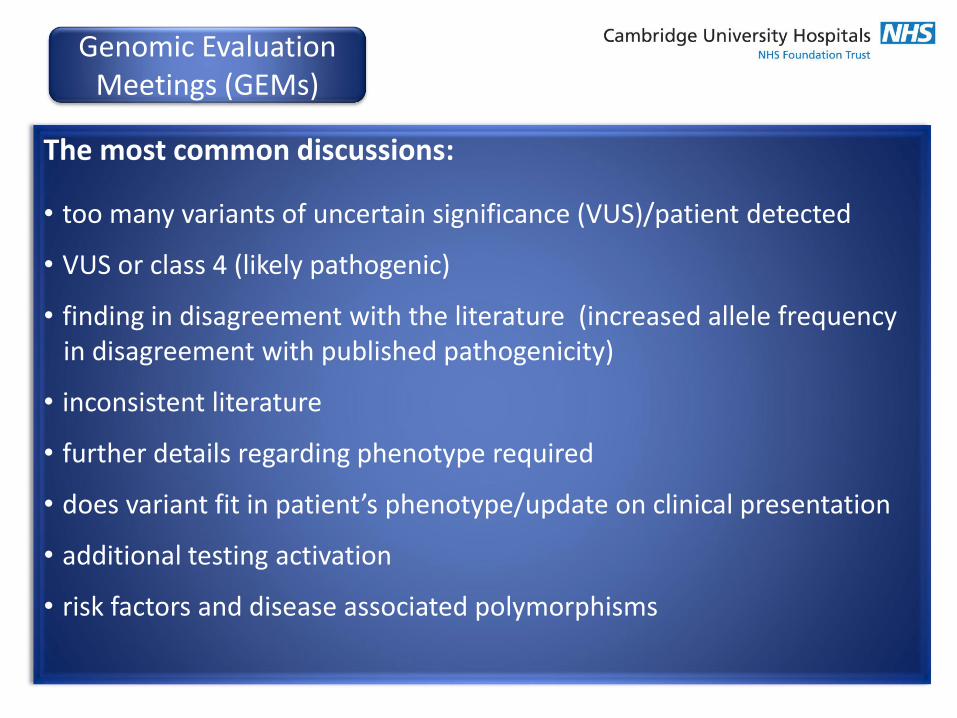
The most common discussions:
• too many variants of uncertain significance (VUS)/patient detected
• VUS or class 4 (likely pathogenic)
• finding in disagreement with the literature (increased allele frequency in disagreement with published pathogenicity)
• inconsistent literature
• further details regarding phenotype required
• does variant fit in patient’s phenotype/update on clinical presentation
• additional testing activation
• risk factors and disease associated polymorphisms
Genomic Evaluation Meetings (GEMs)
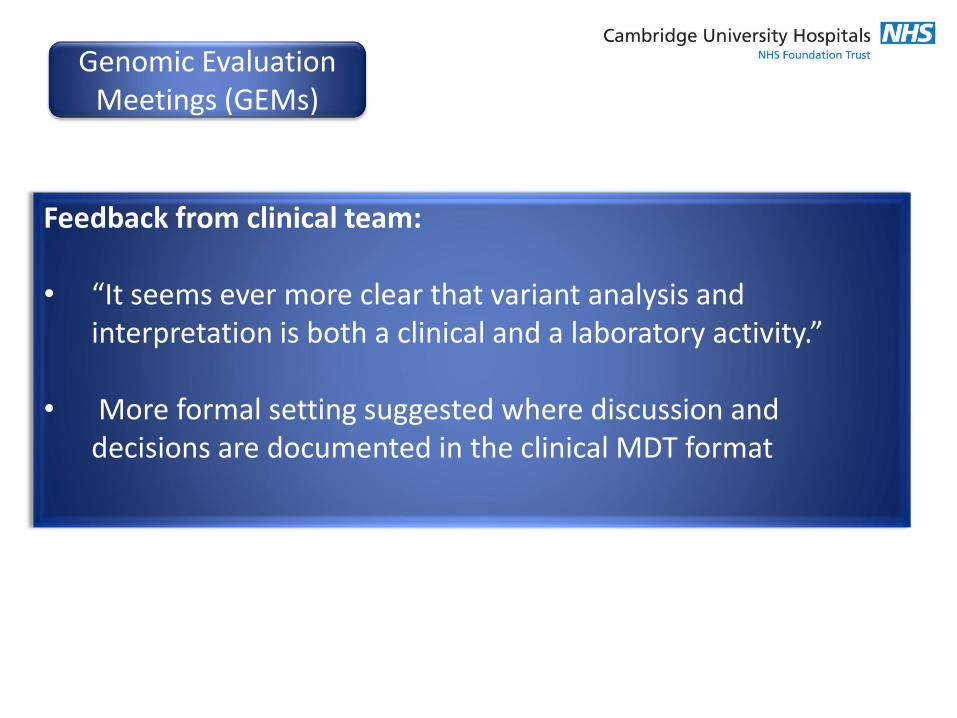
Feedback from clinical team:
• “It seems ever more clear that variant analysis and interpretation is both a clinical and a laboratory activity.”
• More formal setting suggested where discussion and decisions are documented in the clinical MDT format
Genomic Evaluation Meetings (GEMs)
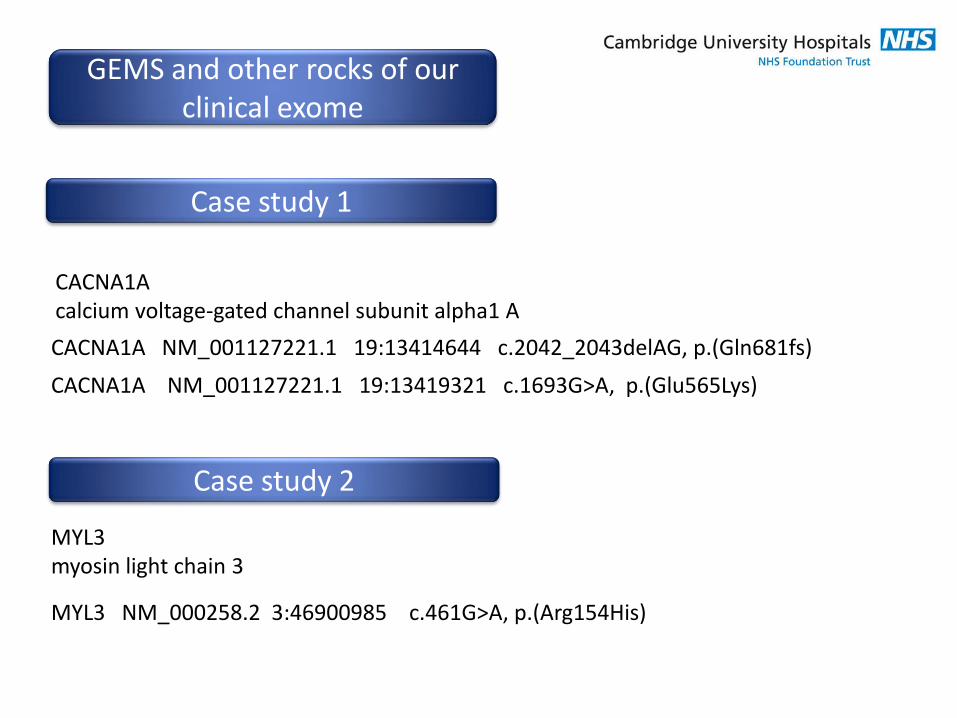
GEMS and other rocks of our clinical exome
CACNA1A calcium voltage-gated channel subunit alpha1 A CACNA1A NM_001127221.1 19:13414644 c.2042_2043delAG, p.(Gln681fs)
CACNA1A NM_001127221.1 19:13419321 c.1693G>A, p.(Glu565Lys)
MYL3 myosin light chain 3
MYL3 NM_000258.2 3:46900985 c.461G>A, p.(Arg154His)
Case study 1
Case study 2
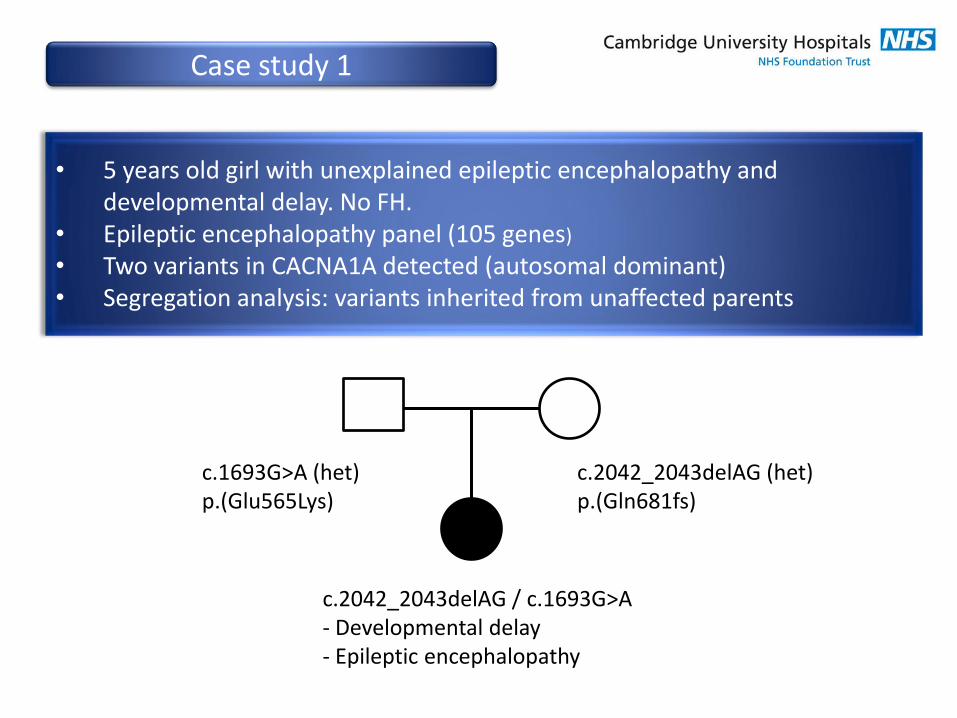
c.1693G>A (het) p.(Glu565Lys)
c.2042_2043delAG / c.1693G>A - Developmental delay - Epileptic encephalopathy
c.2042_2043delAG (het) p.(Gln681fs)
• 5 years old girl with unexplained epileptic encephalopathy and developmental delay. No FH.
• Epileptic encephalopathy panel (105 genes)
• Two variants in CACNA1A detected (autosomal dominant) • Segregation analysis: variants inherited from unaffected parents
Case study 1

Case study 1
G1295 gene transcript coordinates cDNA protein pathogenicity
CACNA1A NM_001127221.1 19:13419321 c.1693G>A p.(Glu565Lys) yes no N/A
inheritance AD (EA1,SCA6, FHM) ?x
ExAC 0 x
ESP 0 x
1000 genomes 0 x
GEMINI 0 x
HGMD not reported x
dbSNP not reported
ClinVar not reported
nucleotide highly conserved x
amino acid highly conserved x
splice site no effect on splicing x
effect on prot. small physicochemical difference between Glu-Lys x protein domain Ion transport x
PolyPhen probably damaging x
SIFT deleterious x
Mut. Taster disease causing x
PubMed not reported
comment inherited from unaffected father (CACNA1A - complete penetrance 80%) ?x
class: 3
• CACNA1A LoF variants previously reported with incomplete penetrance and variable expressivity
• Recently CACNA1A haploinsufficiency reported in epileptic encephalopathy
• No data on “compound heterozygosity” in CACNA1A
GEM discussion: • Contribution of CACNA1A variants to the phenotype of our patient?
Case study 1
GEM conclusions: • CACNA1A variants probably contribute however cannot explain patient’s
phenotype • Referral to 100.000 Genomics England Project
Case study 2
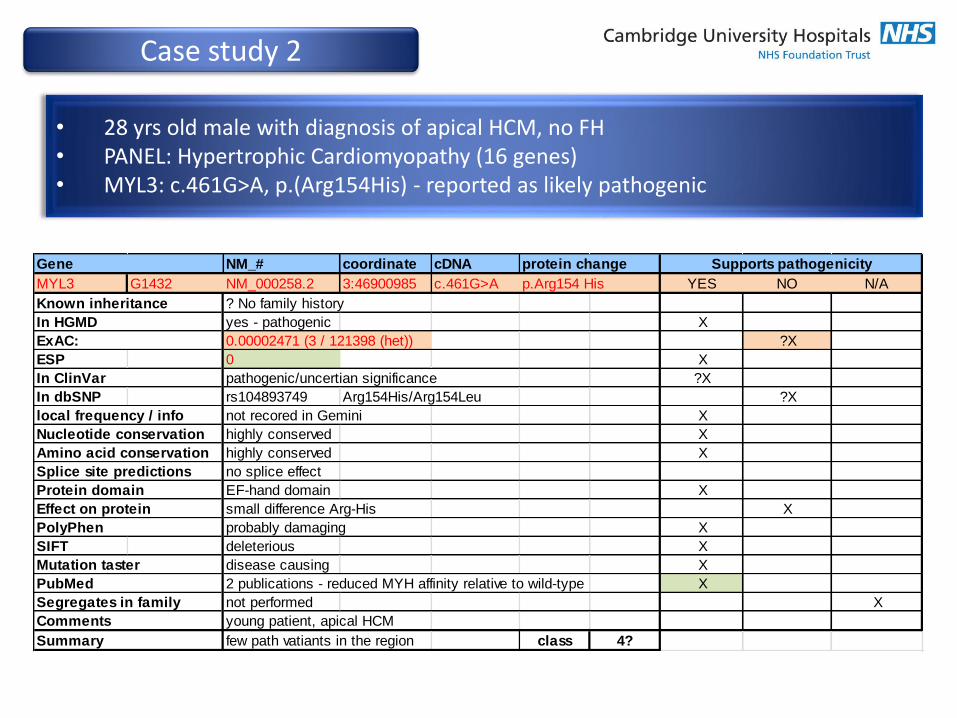
• 28 yrs old male with diagnosis of apical HCM, no FH • PANEL: Hypertrophic Cardiomyopathy (16 genes) • MYL3: c.461G>A, p.(Arg154His) - reported as likely pathogenic
NM_# coordinate cDNA protein change
MYL3 G1432 NM_000258.2 3:46900985 c.461G>A p.Arg154 His YES NO N/A
? No family history
yes - pathogenic X
0.00002471 (3 / 121398 (het)) ?X
ESP 0 X
pathogenic/uncertian significance ?X
In dbSNP rs104893749 Arg154His/Arg154Leu ?X
not recored in Gemini X
highly conserved X
highly conserved X
no splice effect
EF-hand domain X
small difference Arg-His X
probably damaging X
SIFT deleterious X
disease causing X
2 publications - reduced MYH affinity relative to wild-type X
Segregates in family not performed X
young patient, apical HCM
few path vatiants in the region class 4?
ExAC:
In ClinVar
local frequency / info
Nucleotide conservation
Gene Supports pathogenicity
Known inheritance
In HGMD
Summary
Effect on protein
PolyPhen
Mutation taster
PubMed
Amino acid conservation
Splice site predictions
Protein domain
Comments
Case study 2
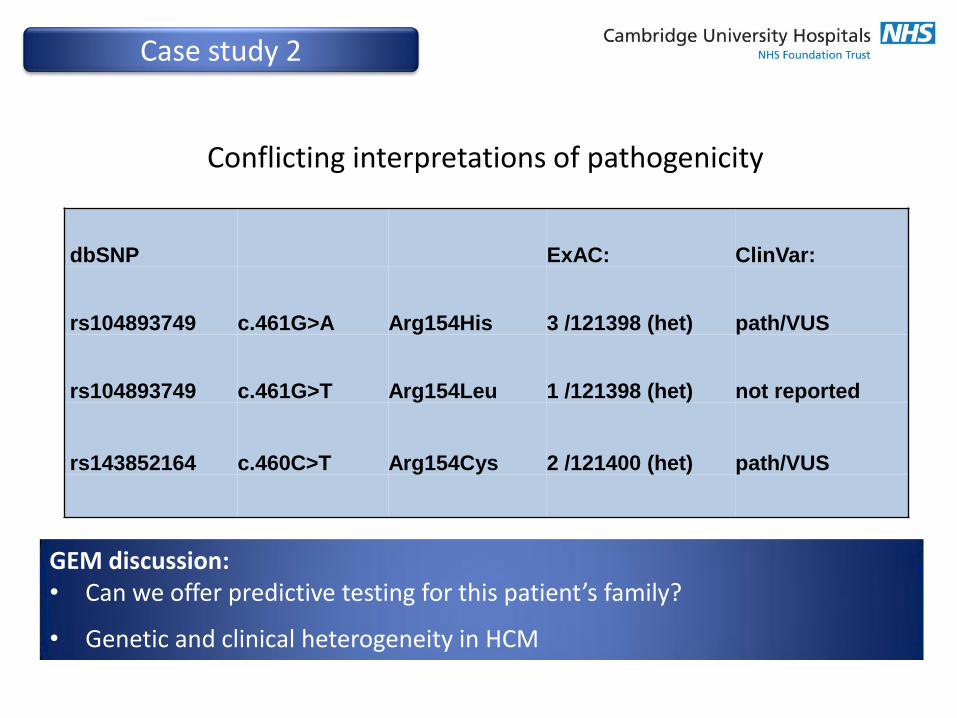
Conflicting interpretations of pathogenicity
dbSNP ExAC: ClinVar:
rs104893749 c.461G>A Arg154His 3 /121398 (het) path/VUS
rs104893749 c.461G>T Arg154Leu 1 /121398 (het) not reported
rs143852164 c.460C>T Arg154Cys 2 /121400 (het) path/VUS
GEM discussion: • Can we offer predictive testing for this patient’s family?
• Genetic and clinical heterogeneity in HCM
• GEM was established to facilitate the effective reporting of challenging variants
• Brought together clinical geneticists and clinical scientists to discuss the interpretation and reporting of rare variants
• Comprehensive approach to elucidate the pathogenic potential of variants and their relative contribution to phenotype
• This resulted in clarification for most of the variants
• Documented clinical MDT format from September 2016
Summary
Laboratory: Howard Martin, Fay Rodger, Jaycen Parr, Gillian Flavell
Bioinformatics: Kim Brugger, Matt Garner, Dilna Pushpajan
Database: Ian Johnson
Data analysis & reporting: Philip Twiss, Isabelle Delon, James Drummond, Ed Thompson, Namir Al-Hasso, Sarah Spiden, Julie Evans, Nick Gleadall, Gavin Fuller, Katerine Yeats, Harjeet Rai, Sally Halsall, Terence Elsey
Patient referral: Numerous Clinical Geneticists and clinicians around UK
Director of the Laboratory: Stephen Abbs
Acknowledgements