Embed Size (px)
Citation preview

Poster Print Size: This poster template is 44” high by 44” wide. It can be used to print any poster with a 1:1 aspect ratio.
Placeholders: The various elements included in this poster are ones we often see in medical, research, and scientific posters. Feel free to edit, move, add, and delete items, or change the layout to suit your needs. Always check with your conference organizer for specific requirements.
Image Quality: You can place digital photos or logo art in your poster file by selecting the Insert, Picture command, or by using standard copy & paste. For best results, all graphic elements should be at least 150-200 pixels per inch in their final printed size. For instance, a 1600 x 1200 pixel photo will usually look fine up to 8“-10” wide on your printed poster.
To preview the print quality of images, select a magnification of 100% when previewing your poster. This will give you a good idea of what it will look like in print. If you are laying out a large poster and using half-scale dimensions, be sure to preview your graphics at 200% to see them at their final printed size.
Please note that graphics from websites (such as the logo on your hospital's or university's home page) will only be 72dpi and not suitable for printing.
[This sidebar area does not print.]
Change Color Theme: This template is designed to use the built-in color themes in the newer versions of PowerPoint.
To change the color theme, select the Design tab, then select the Colors drop-down list.
The default color theme for this template is “Office”, so you can always return to that after trying some of the alternatives.
Printing Your Poster: Once your poster file is ready, visit www.genigraphics.com to order a high-quality, affordable poster print. Every order receives a free design review and we can deliver as fast as next business day within the US and Canada.
Genigraphics® has been producing output from PowerPoint® longer than anyone in the industry; dating back to when we helped Microsoft® design the PowerPoint® software.
US and Canada: 1-800-790-4001
Email: [email protected]
[This sidebar area does not print.]
Carotid Sinus Sensitivity due to Deep Neck Scar after Neck
Dissection: Surgical Management with Interposition STSG
Aaron Dezube, BS1; Reza Ehsanian, MD PhD2; Scott Stephan Scott, MD2
Tufts University School of Medicine1, Vanderbilt Medical Center Department of Otolaryngology2, Nashville, TN
INTRODUCTION DISCUSSION
RESULTS
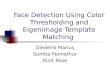
Figure 1. Computerized tomography (CT) at the level of the carotid
bifurcation demonstrating scar extension to the level of the carotid sinus.
ABSTRACT
METHODS AND MATERIALS
CONCLUSIONS
REFERENCES
CONTACT
2 months following scar release and STSG placement
(figure 3). There was full graft take and she noted
improvement in head motion with approximately 45 degree
contralateral head turning past the midline without
difficulty. Additionally, there was complete resolution of her
bradycardic symptoms and no syncopal episodes. She continues with full range of motion neck physical therapy.
The carotid sinus is an arterial baroreceptor located at
the bifurcation of the external and internal carotids.
This receptor responds to stretching of the arterial
wall leading to increases in firing frequency of action
potentials and vice versa if arterial blood pressure
suddenly decreases. The sinus nerve of Hering, a
branch of the glossopharyngeal nerve, innervates the
carotid sinus baroreceptors, which is different than the
baroreceptors located in the aortic arch innervated by
the vagus nerve.1 Efferent fibers from both receptors
descend in the vagus and cervical sympathetic
nerves respectively to the cardioinhibtory and
vasomotor centers. 2
Neck dissection is known to be associated with
multiple complications both intra-operatively and post-
operatively including scarring, bleeding, air leaks,
chylous fistulas, facial and cerebral edema, damage
to neurovasculature in the neck in addition to many
others.3 Post surgical scar causing contraction,
problems with cosmesis and functional movement
restriction following neck dissections has been a well-
documented entity.4 However, operation scars in
addition to enlarged lymph nodes, and head and neck
malignancies has only recently been postulated to
produce carotid sinus hypersensitivity,5,6,7,8,9.
: Recurrent episodes of asystole from carotid sinus
hypersensitivity triggered by positioning for head and
neck surgery.
In the case of our patient, she developed extensive
deep neck scarring as a result of neck dissection and
subsequent complications and revisions. Computed
topography illustrated the proximity of the scar to her
carotid sinus, which in the context of lightheadedness
and bradycardia with head turning suggested the scar
as the underlying cause. Therefore, while z-plasty is a
known technique for scar revision, little literature
exists discussing surgical revision of the scar as a
functional management of deep neck scar-induced
carotid sinus hypersensitivity following surgical
dissection of head and neck malignancies.
On Sept. 2014, the patient presented for revision of
her left neck scar. Intraoperative findings showed
tethering of the skin to a fibrosed supraclavicular
fascial flap and trapezius muscle edge from the
lateral clavicle to the level of the carotid bifurcation in
the setting of extreme left neck volume loss and
fibrosis (Figure 3) after failed free flap, infection, and
radiation. A serial Z-plasty scar revision was
performed with 8 2x2cm transposition flaps designed
with 45-degree angles of each limb.
During follow up the patient continued to experience a
symptomatic scar. The patient was noted to have two
more non-syncopal bradycardic episodes in rehab
confirming her previous diagnosis.
Revision surgery was performed which included full
thickness release of the supraclavicular fascial bands,
trapezius muscle down to fat. The head was placed
in full extension and contralateral head turn to
delineate the full area of skin deficiency and
immediate split thickness skin graft from the thigh
was interposed within this defect (Figure 2).
1 .Lown B, Levine SA: The carotid sinus. Clinical value of its stimulation. Circulation
1961. 23: 766-789.
2. Walter PF, Grawley IS, Dorney ER: Carotid sinus hypersentivity and syncope. Am J
Cardiol 1978, 42:396-403.
3. Flint PW, Haughey BH, Lund VJ, Niparko JK, Richardson MA, Robbins KT, Thomas
JR. (2010). Cummings Otolaryngology: Head and Neck Surgery (5th ed).
Philadelphia, PA: Mosby/Elsevier
4. Chugh SN (2012): Textbook of Clinical Electrocardiography for Postgraduates,
Residents and Practicing Physicians (3rd ed). Panama City, Panama. Jaypee
Brothers Medical Publishers
5. Patel AK, Yap VU, Fields J, Thomsen JH: Carotid sinus syncope induced by
malignant tumors in the neck. Arch Intern Med 1978, 42:396-403.
6. Farr HW: Carotid body tumors: a 40-year study. CA Cancer J Clin 1980, 30:260-265.
Noroozi N, Modabber A, Holze, Branchschweig T, Riediger D, Gerressen M,
Ghassemi A: Carotid sinus syndrome as the presenting symptom of
cysadenolymphoma. Head & Face Medicine 2012, 8:31.
7. Sutherland JA, Stobie P, Swarup V, Tierney SP, Lin-AC, Burke MC: Hypertensive
carotid sinus syndrome due to neurofibromatosis-1 and manifested by repeated
episodes of syncope. Pacing Clin Electrophysiol 2004, 27:1571-1573.
8. Trung AT, Sturgis EM, Rozner MA, Truong DT: Recurrent episodes of asystole from
carotid sinus hypersensitivity triggered by positioning for head and neck surgery.
Head Neck. 2013 Jan, 35(1): E28-30
Aaron Dezube, BS Tufts University School of Medicine Vanderbilt Medical Center Dept. of Otolaryngology [email protected] Phone: 617-306-0961
Neck dissection for head and neck
malignancies is associated with
multiple complications post
operatively. While scar is a known
complication, little literature exists
about functional changes due to scar
including carotid sinus sensitivity or
the surgical management of scar-
induced carotid sinus.
We herein describe a 70-year-old
woman who developed extensive left
sided deep neck scar following
chemoradiation, and surgical
management of her squamous cell
carcinoma (SCCa), which led to a
painful scar suspected of causing
carotid sinus sensitivity due to its
position relative to the carotid
bifurcation. Our case suggests a role
for surgical management of this
condition to improve not only
cosmesis but functional status as well.
This case report illustrates a complication of neck
dissection causing cicatricial carotid sinus sensitivity.
In addition, it describes a successful approach to
alleviate the functional sequelae of this cervical scar
contracture using scar revision and an interposition
STSG.
A 70-year-old Caucasian woman was initially treated
with chemoradiation for a right base-of-tongue
squamous cell carcinoma (SCCa). Twelve years later,
she was then diagnosed new T1N1 1.5 cm poorly
differentiated SCCa with basaloid features located on
her left posterior pharyngeal wall. She underwent a
posterior glossectomy with a left modified neck
dissection, infratemporal fossa resection of deep
extension of tumor and a retropharyngeal lymph node
and extended lateral pharyngectomy resulting in
closure with a secondary right anterolateral thigh free
flap for reconstruction. Due to venous congestion of
the free flap it was removed and replaced with a left
supraclavicular flap in 2013, which was complicated by
local infection, and subsequent sepsis and and
pneumonia.
On presentation to our Facial Plastics and
Reconstructive Surgery clinic, she complained of
prominent and painful scar band on the lateral left neck
extending down to the supraclavicular area. She had 3
documented episodes of syncope induced by neck
rotation or extension, other subclinical episodes of
lightheadedness and bradycardia with less prominent
head movement.
Computerized tomography (CT) showed extension of
the neck scar contracture into the plane of the
bifurcation of the carotid artery (Figure 1).
This represented a case of post-surgical cicatricial
carotid sinus hypersensitivity.
Level of carotid
sinus
Dense scar
tissue extending
from skin down
to carotid sinus
Figure 2: Intra-operative photo of scar band (left), release (middle) and
interposition STSG placement (right).
Figure 3: (Left) Pre-operative
photos demonstrating the scar,
level of volume loss and extent of
fibrosis present in patients left
neck. (Right) 2 months post-
operative showing graft take and
release of scar band.