Embed Size (px)
Citation preview

Genetic Variability and Cancer
• Germline polymorphisms are frequent: 1 SNP every 400-1500 bp (> 1 per gene)
• Cancer has acquired mutations (some tumor “mutations” common: e.g. most CML has t(9;22); Rb has LOH relative to germline)
The Intl SNP Map Working Group Nature 2001

Relling & Dervieux 2001;1:99-108
Host and tumorgenomesaffect variabilityin anticancertherapy

Given Similar Schedule and Regimen, Pharmacogenetics should Have Similar
Implications for Children and Adults
• Host– developmental
changes expressed in somatic tissues contribute to child vs adult PK, PD differences
– germline poly-morphisms affect host similarly in children and adults
• Tumor– tumors different
children vs adults– germline
polymorphisms affect tumor response/invasive-ness similarly in children vs adults

Pharmacogenetics and Cancer
Polymorphisms in:• host metabolism• host distribution &
transport• host receptors &
targets• tumor receptors &
targets• pathogens
May affect:• cancer risk• host toxicity• tumor response• infectious
complications

GST Status affects Risk of Toxicity and Chance for Cure
anticancerdrug
free-radicalsor
electrophiles
more:less:less:
less:more:more:
inactivationtoxicityanticancer effect
inactivationtoxicityanticancer effect
mutant GST
wild-type GST
+
glutathione
H C CH2 CH2 C NH C NH CH2
NH2 CH2 COOH
SH
COOH HO

Glutathione S-Transferase Polymorphisms and Outcome ofChemotherapy in Childhood Acute Myeloid LeukemiaBy Stella M. Davies, Leslie L. Robison, Jonathan D. Buckley, Tom Tjoa, William G. Woods, Gretchen A. Radloff,Julie A. Ross, and John P. Perentesis J Clin Oncol 19:1279-1287.
N = 306Dex, VP, AraC, TG, dauno: standard vs intensive timing

GSTT1 genotype did not affect outcome with Standard timing, but did affect outcome with
Intensive timing5 yr Std
timingGST1+
StdtimingGST1-
InttimingGST1+
InttimingGST1-
Survival 41 35 59 43
DFS 47 53 64 47
Death inremission
28 26 12 33
(P < 0.05)
JCO 19:1279, 2001

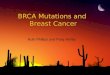
greater anticancer drug effectin breast cancer..... but .....higher risk of toxic death
in AML
Examples: Mutant GST associated with:
1.0
0.8
0.6
0.4
0.2
00 1 2 3 4 5 6 7 8
wild type
heterozygote
mutant
Years from Diagnosis
GST-P1
Cancer Res 60:5621-4, 2000
1.00
0.75
0.50
0.25
00 1 2 3 4 5 6 7 8
Time (years)
GST-T1
JCO 19:1279-87, 2001
(+)
(–)
Among women with breast cancer, GSTP1 mutation associated with improved survival

greater anticancer drug effectin breast cancer..... but .....higher risk of toxic death
in AML
Examples: Mutant GST associated with:
1.0
0.8
0.6
0.4
0.2
00 1 2 3 4 5 6 7 8
wild type
heterozygote
mutant
Years from Diagnosis
GST-P1
Cancer Res 60:5621-4, 2000
1.00
0.75
0.50
0.25
00 1 2 3 4 5 6 7 8
Time (years)
GST-T1
JCO 19:1279-87, 2001
(+)
(–)

• The effect of each polymorphism must be evaluated in the context of the disease and its therapy (e.g. intensifying therapy in GST wild-type pts may be correct in children with AML but not adults with breast cancer)

Tumor
2 tandemrepeats
TS
Good antitumorresponse to 5FU
TS activity
3 tandemrepeats
Poor antitumorresponse to 5FU
TS activity
28bp repeats5FUMP(active)
5FU Dihydro 5-FU (inactive)
enhancer region
Normal DPD ;Normal 5FU
TOLERABILIITY
exon13 exon15 exon13 exon14 exon15
exon13 exon14 exon15
AG GT AG GT AG GT
MUT:A Wt:G
mRNA
Non-functional protein functional protein
~97% wt~3% het
JCI 98:610-15, 1998JCO 19:1779-86, 2001
Low DPD ;High 5FUTOXICITY
DPD
Thymidylate synthase ( TS )
DPD - dihydropyrimidine dehydrogenase
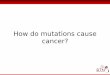
5FU toxicity andantitumor responseare affected bygenetic polymorphismsin DPD and TS
Gonzalez et al; Diasio et al

Relling & Dervieux Nature Ca Rev 2001;1:99-108
Tumor
2 tandemrepeats
TS
Good antitumorresponse to 5FU
TS activity
3 tandemrepeats
Poor antitumorresponse to 5FU
TS activity
28bp repeats5FUMP(active)
5FU Dihydro 5-FU (inactive)
enhancer region
Normal DPD ;Normal 5FU
TOLERABILIITY
exon13 exon15 exon13 exon14 exon15
exon13 exon14 exon15
AG GT AG GT AG GT
MUT:A Wt:G
mRNA
Non-functional protein functional protein
~97% wt~3% het
JCI 98:610-15, 1998JCO 19:1779-86, 2001
Low DPD ;High 5FUTOXICITY
DPD
Thymidylate synthase ( TS )
DPD - dihydropyrimidine dehydrogenase
5FU toxicity andantitumor responseare affected bygenetic polymorphismsin DPD and TS

Tumor
2 tandemrepeats
TS
Good antitumorresponse to 5FU
TS activity
3 tandemrepeats
Poor antitumorresponse to 5FU
TS activity
28bp repeats5FUMP(active)
5FU Dihydro 5-FU (inactive)
enhancer region
Normal DPD ;Normal 5FU
TOLERABILIITY
exon13 exon15 exon13 exon14 exon15
exon13 exon14 exon15
AG GT AG GT AG GT
MUT:A Wt:G
mRNA
Non-functional protein functional protein
~97% wt~3% het
JCI 98:610-15, 1998JCO 19:1779-86, 2001
Low DPD ;High 5FUTOXICITY
DPD
Thymidylate synthase ( TS )
DPD - dihydropyrimidine dehydrogenase
5FU toxicity andantitumor responseare affected bygenetic polymorphismsin DPD and TS
Relling & Dervieux Nature Ca Rev 2001;1:99-108

• > 1 polymorphism affects drug efficacy
• Germline polymorphisms also affect tumor responsiveness

DHF
THF
DHFR
TS
MTXglu
MTXglu
GARtf AICARtf
PRPPde novopurinesynthesis
GGH
MTXglu5
gluglu
n=7
MTXglu
RFC
diffusion
MTXgluMRP
THF5,10-CH2
MTHFR5-CH3THF
Homocysteine
Methionine
Polymorphisms in Gene Products for MTXMetabolism and Targets may Affect PK/PD

Greater oral mucositisindex (OMI) after MTX among BMT patients with mutant MTHFR C677Tgenotypes than amongpatients with C677Cgenotypes
Ulrich et al Blood 98:231-4, 2001

But MTHFR did not Affect Toxicity after HDMTX (with LV)

• The effect of each polymorphism may be dependent upon dose and schedule of the anticancer agent

Relling & Dervieux 2001;1:99-108
UGT1A1 Polymorphism affects risk of Irinotecan Toxicity

Thiopurine Methyltransferase(TPMT) Polymorphism affects6MP Pharmacodynamics
10
8
6
4
2
00 5 10 15 20 25 30
TPMT Activity
2000
1000
0Mut/Mut Wt/Mut Wt/Wt
HPRT
TGNs DNAincorporation
MP MeMPTPMT
toxicityrisk of relapse
myelosuppressionrisk secondary cancer
wt/wt
wt/m
m/m
Leukemia 14:567-72, 2000Relling & Dervieux Nature Ca Rev 2001;1:99-108

Cumulative Incidence of 6mp Dose Alterationsto Prevent Toxicity
During Continuation Therapy of Total XII
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.5 1 1.5 2 2.5
Years
CI
Homozygous Wild Types Heterozygotes Mutants
Relling et al JNCI, 1999



0
2
4
6
8
10
12
14
0 1 2 3 4 5
Antimetabolite Intensity Index*
Cum
ulat
ive
inci
denc
e (%
) br
ain
tum
or
XIX-RTSC
X-High
XII
Antimetabolite Intensity (during irradiation) vs Cumulative Risk of Brain Tumor
* Score = 1 for ITs during rads, -1 for LV during rads, 2 for systemic MTX during rads, 2 for full dose 6MP during rads
Lancet 1999

Www.pharmacogenetics.org

Drug Metabolizing Enzyme Polymorphisms
Drugs
secondarybrain tumor
thrombosis
arrhythmia Non-DrugInfluences
glucuronosyltransferase
polym orphism
cytochrom eP450
m utation
thiopurinem ethyl-
transferasemutation
cranialirradiation
pneumonia
folatedeficiencyasparaginase
macrolideantibiotics
thiopurine
potassiumchannel
polym orphismprothrombin
m utationtransporter
Polymorphisms in Drug Receptors, Targets, and Transporters

• Elucidating the clinical implications of each polymorphism may take a long time (AKA drugs have unintended consequences)

Incorporate Pharmacogenetics into all Clinical Trials
• Clinical trials are expensive
• freezing a tube of blood is cheap
• genotyping will get cheaper in the future
• obtain proper consent for future pharmacogenetic studies
• let’s not pretend we currently understand what to look at in the future

Polymorphisms Affecting Supportive Care Impact on Patient
Outcome
• Antimicrobials (K+ channels)
• cardiovascular agents (ACE, beta receptors)
• antithrombotics (CYP2C9, MTHFR, Factor V Leiden, prothrombin)

“Emphasis should not be focused on population averages, but rather on providing prescribers with the tools to determine the most effective and safest drug dosage for individual patients with a minimum of trial and error.”– Gerhard Levy, Clin Pharmacokin 34:323-
33, 1998