Embed Size (px)
Citation preview

1
Clinical Policy Title: Genetic testing for long QT syndrome
Clinical Policy Number: CCP.1037
Effective Date: Dec. 1, 2013
Initial Review Date: June 19, 2013
Most Recent Review Date: July 2, 2019
Next Review Date: June 2020
Related policies:
CCP.1236 Molecular targeted therapy
ABOUT THIS POLICY: AmeriHealth Caritas has developed clinical policies to assist with making coverage determinations. AmeriHealth Caritas’
clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by AmeriHealth Caritas when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. AmeriHealth Caritas’ clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. AmeriHealth Caritas’ clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, AmeriHealth Caritas will update its clinical policies as necessary. AmeriHealth Caritas’ clinical policies are not guarantees of payment.
Coverage policy AmeriHealth Caritas considers the use of genetic testing for long QT syndrome , also known as Familion testing, to be clinically proven and therefore medically necessary when the following criteria are met:
The individual has a close relative (first-, second- or third-degree) with a known long QT syndrome mutation.
The individual has a close relative (first-, second- or third-degree) diagnosed with long QT syndrome by clinical means and whose genetic status is unavailable.
The individual has palpitations, syncope and/or dizziness with a history of a close relative (first-, second-, or third-degree) who experienced a sudden cardiac death.
The individual has a prolonged QT interval on resting electrocardiogram (a corrected QTc) of greater than 440 msec without an identifiable acquired or external cause for the QTc prolongation (i.e., bradycardia, electrolyte imbalance or certain medications/drugs) (QTc values of ≥ 0.44 sec are treated as suspicious, CSANZ 2011.)
The individual has signs and/or symptoms indicating a moderate-to-high pretest probability of long QT syndrome using the Schwartz criteria (score of 2 – 3).
Limitations
Policy contains:
Familion testing.
Long QT syndrome subtypes.

2
All other uses of genetic testing for long QT syndrome/Familion testing are not medically necessary.
A negative genetic test in a clinically normal individual of a well-characterized family should eliminate the need for future testing (for the same individual), as genetic testing for a particular disease is usually performed once per lifetime.
Alternative covered services:
• Physical examination. • Electric conductivity tests: electrocardiogram, echocardiography. • Genetic counseling.
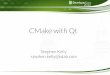
Background Long QT syndrome is a heart rhythm condition that can cause rapid and irregular heartbeats, leading to fainting spells, seizures, and (when the condition is extended), sudden death. A genetic condition, an estimated 1 in 2000 newborns have the disorder, or roughly 2,000 cases per year in the U.S. (Schartz, 2009). The syndrome is caused by mutations in a set of genes that code the protein subunits of cardiac ion channels. These ion channels are important for the electrical conductivity and signals of the heart. The electrical signals may be recorded by an electrocardiogram (ECG) and produce a characteristic waveform. The different components of the waveform are identified by the letters P, Q, R, S and T. The distinctive feature of long QT syndrome is the lengthening of the Q – T interval on an electrocardiogram (ECG). The Q – T interval on the waveform represents the duration of the electrical activation and deactivation of the heart ventricles, which are the lower, main pumping chambers of the heart. With the advent of genetic testing, there is evidence of an overlap of specific genotypes that cause the characteristic T wave shapes.
Long QT syndrome genetic mutations may lead to an increase in the Q – T Interval on an
electrocardiogram.
In medical genetics, testing is done to diagnose individuals who possess chromosomal, genetic variations associated with a high risk of having or transmittinglong QT syndrome. The abnormal mutations and variations in DNA sequencing that cause long QT syndrome are represented by abnormal allele configurations that are not found in the otherwise normal, healthy population. Genetic tests may be conducted for individuals who are asymptomatic or have a family member with this diagnosed genetic disorder. All first-degree relatives (i.e., siblings, parents and children) of an individual with an long QT syndrome gene mutation have up to a 50 percent risk of harboring the same mutation. Typically, long QT syndrome is inherited in an autosomal dominant pattern, in which a single mutation causes the
Normal Long QT

3
disease. The genetic material (DNA) used for testing may be obtained from a blood sample or may be gathered by a mouth swab. Laboratories are able to offer multi-gene cardiomyopathy/cardiac panels that test many genes (may contain 50 or more) in an effort to diagnose several cardiac conditions at one time. The importance of identifying individuals for an inherited cardiac arrhythmia is highlighted by the potential lethality of these syndromes, mostly due to ventricular tachyarrhythmias. Long QT syndrome usually affects children or young adults, although it may occur in otherwise healthy individuals of various ages. Most people with long QT syndrome are diagnosed either by family history, an episode of syncope, or by surviving a severe ventricular arrhythmia. For some unfortunate symptomatic individuals, the initial presentation of long QT syndrome symptoms leads to sudden cardiac death. The goal of genetic testing for long QT syndrome is to prevent sudden death through medical therapy, to counsel the individual and their family, and to assist with lifestyle changes (CSANZ, 2011). Literature suggests that long QT syndrome may be responsible for as many as 3,000 unexpected deaths in children and young adults in the United States each year (Modell, 2012). Younger individuals have a higher risk of unexpected sudden death than adults with a genetic cardiac disease. A family history of sudden death, possibly with genetic confirmation, may influence treatment decisions for those with suspected and ultimately confirmed long QT syndrome. Because this disease is a primarily an electrical disorder, most individuals have no evidence of structural heart disease or LV dysfunction, making the long-term prognosis excellent if the arrhythmia is controlled. Treatment may involve beta blockers, permanent pacing, or left cervicothoracic sympathectomy (Tracy, 2008). Long QT syndrome can also be an acquired condition from cardiovascular medications administered to predisposed patients, often in the Intensive Care Unit. Treatment of acquired long QT syndrome, which is essentially fatal, is essentially awareness, identification, and discontinuation of QT prolonging drugs (Beitland, 2014). Practice guideline statements from the American College of Cardiology Foundation (ACCF), American Heart Association (AHA), and European Society of Cardiology (ESC) have noted an evolving role for genetic testing of long QT syndrome in risk stratification and clinical decision-making (Zipes, 2006). This stance pertaining to the use of risk stratification and data from genetic analysis becoming of increasing import to meaningful clinical decision making was further addressed in the 2012 American College of Cardiology, American Heart Association Task Force, and European Society of Cardiology (ACCF/AHA/HRS) focused update incorporated into the ACCF/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities. Both independent reviews and professional society guidelines agree that genetic testing should not be used alone in making recommendations for a prognosis for long QT syndrome, though testing may be used to support clinical diagnosis and early detection of at-risk relatives (Ackerman, 2011).
Long QT syndrome subtypes
Variant Gene Name Frequency Current Affected
LQT1 KCNQ1 30 – 35% K+, alpha subunit
LQT2 KCNH2 25 – 30% K+, alpha subunit
LQT3 SCN5A 5 – 10% Na+, alpha subunit
LQT4 ANK2 1 – 2% Na+, targeting protein
LQT5 KCNE1 1% K+, beta subunit
LQT6 KCNE2 Rare K+, subunit

4
LQT7 KCNJ2 Rare K+, potassium channel
LQT8 CACNA1C Rare Ca++, alpha 1C subunit
LQT9 CAV3 Rare Na+, caveolin-3 protein
Long QT syndrome subtypes
Variant Gene Name Frequency Function
LQT10 SCN4B Rare Na+, beta subunit
LQT11 AKAP9 Rare K+, protein kinase
LQT12 SNTA1 Rare Na+, α1-syntrophin
LQT13 KCNJ5 Rare potassium channel
Searches: AmeriHealth Caritas searched PubMed and the databases of:
UK National Health Services Centre for Reviews and Dissemination.
Agency for Healthcare Research and Quality Guideline Clearinghouse.
The Centers for Medicare & Medicaid Services. Searches were conducted on May 28, 2019 using the terms “cardiac, genetic testing, Familion” and “long QT syndrome”. We included:
Systematic reviews, which pool results from multiple studies to achieve larger sample sizes and greater precision of effect estimation than in smaller primary studies. Systematic reviews use predetermined transparent methods to minimize bias, effectively treating the review as a scientific endeavor, and are thus rated highest in evidence-grading hierarchies.
Guidelines based on systematic reviews.
Economic analyses, such as cost-effectiveness, and benefit or utility studies (but not simple cost studies), reporting both costs and outcomes — sometimes referred to as efficiency studies — which also rank near the top of evidence hierarchies.
Findings The genetics of cardiac ion channelopathies are extremely varied. The number of genes that have been associated with causing long-QT syndrome has risen to 10, and there are hundreds of possible mutations in these genes that appear to be harmful. The Familion genetic test includes just five of the genes that are known to be associated with cardiac ion channelopathies and therefore the number of symptomatic first-degree relatives of those with known long QT syndrome mutations is high. The use of the Familion genetic test may potentially have clinical utility in patients with long QT syndrome. For first-degree relatives with known long QT syndrome mutations in 1 of 5 genes included in the test, the Familion genetic test can confirm the presence of the familial mutation. A negative result is also instructive, as with the high analytical sensitivity and low probability of a sporadic mutation, a negative result would indicate a low probability of the patient having long QT syndrome. Thus, use of the Familion genetic test in first-degree relatives of those with a known Long QT syndrome mutation may allow better use of prophylactic treatment for payers and avoidance of unnecessary restrictive activity for patients.

5
Genetic tests are regulated under the Clinical Laboratory Improvement Amendments Act of 1988. Premarketed approval from FDA is not required as long as the assay is performed in a laboratory facility that observes the CLIA regulations. The provider of the Familion genetic test has a current CLIA license. Long QT syndrome is a significant factor in certain fetal disorders. It accounted for 15 – 17 percent of fetal bradycardias of <110 beats per minute among fetuses with a normally structured heart; of patients with a significant prenatal finding of long QT syndrome, 17 – 35 percent exhibited reduced baseline fetal heart rate of 110 – 120 beats per minute on electronic cardiotocography (Ishikawa, 2013). Four articles on the cost-effectiveness of genetic testing for long QT syndrome in infants and young adults found testing in the early detection of long QT syndrome to be cost-effective compared with no testing in symptomatic cases, and not cost-effective when compared with watchful waiting in asymptomatic first-degree relatives of patients with established long QT syndrome; in neonates, testing was highly cost-effective when compared with any screening strategy (Gonzalez, 2015).
Policy updates: A total of no guidelines/other and three peer-reviewed references were added to this policy in 2017. No new guidelines or clinical references were identified in 2018. In 2019, we did not identify any newly published literature. The policy ID was changed from 04.01.02 to CCP.1037. References
Professional society guidelines/other:
Ackerman MJ, Priori SG, Williams S, et al. HRS/EHRA expert consensus statement on the state of genetic
testing for the channelopathies and cardiomyopathies this document was developed as a partnership
between the Heart Rhythm Society (HRS) and the European Heart Rhythm Association (EHRA). Heart
Rhythm. 2011;8(8):1308-1339. Doi: 10.1093/europace/eur245. Correction published: doi:
10.1093/europace/eur413.
Ackerman MJ, Priori SG, Williams S, et al. HRS/EHRA expert consensus statement on the state of genetic
testing for the channelopathies and cardiomyopathies: this document was developed as a partnership
between the Heart Rhythm Society (HRS) and the European Heart Rhythm Association (EHRA). Europace.
2011;13(8):1077-1109. Doi: 10.1093/europace/eur245.
American Academy of Pediatrics. Policy statement: pediatric sudden cardiac arrest. Pediatrics.
2012;129(4):e1094-e1102. Doi: 10.1542/peds.2012-0144.

6
Baylor College of Medicine. John Welsh cardiovascular diagnostic laboratory.
https://www.bcm.edu/departments/pediatrics/research/labs/diagnostic-testing. Accessed May 29,
2019.
Blue Cross Blue Shield Association (BCBSA), Technology Evaluation Center (TEC). Genetic testing for long
QT syndrome. 2007 TEC Assessments 2008;22(9). Chicago, IL.
http://www.sads.org/images/stories/bcbstecadvisory.pdf. Accessed May 29, 2019.
Epstein AE, DiMarco JP, Ellenboken KA, et al. ACC/AHA/HRS 2008 guidelines for device-based therapy of
cardiac rhythm abnormalities: a report of the American College of Cardiology/American Heart
Association/Heart Rhythm Society Task Force on Practice Guidelines. ACC/AHA/HRS, 2008. Circulation.
2008;17(21):e350-e408. Doi: 10.1161/CIRCUALTIONAHA.108.189742.
Epstein AE, DiMarco JP, Ellenbogen KA, et. al.,ACC/AHA/HRS 2008 guidelines for device-based therapy of
cardiac rhythm abnormalities: a report of the American College of Cardiology/American Heart
Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002
Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in
collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am
Coll Cardiol. 2008;51(21):e1-e62. Doi: 10.1016/j.jacc.2008.02.032.
Garratt CJ, Elliott P, Behr E, et al. Heart Rhythm UK Familial Sudden Cardiac Death Syndromes Statement
Development Group. Heart Rhythm UK position statement on clinical indications for implantable
cardioverter defibrillators in adult patients with familial sudden cardiac death syndromes. Europace.
2010 Aug; 12(8):1156-1175. Doi: 10.1093/europace/euq261.
Kapplinger JD, Tester DJ, Alders M, Benito B, et al. An international compendium of mutations in the
SCN5A-encoded cardiac sodium channel in patients referred for Brugada syndrome genetic testing.
Heart Rhythm. 2010;7(1):33-46. Doi: 10.1016/j.hrthm.2009.09.069.
Lehnart SE, Ackerman MJ, Benson DW Jr, et al. Inherited Arrhythmias: a National Heart, Lung, and Blood
Institute and Office of Rare Diseases workshop consensus report about the diagnosis, phenotyping,
molecular mechanisms, and therapeutic approaches for primary cardiomyopathies of gene mutations
affecting ion channel function. Circulation. 2007;116(20):2325-2245. Doi:
10.1161/CIRCULATIONAHA.107.711689.
National Center for Biotechnology Information (NCBI). Long QT syndrome 1: clinical laboratories.
http://www.ncbi.nlm.nih.gov/sites/GeneTests/lab/clinical_disease_id/115871?db=genetests. Accessed
May 30, 2019.
Skinner, J, et al. Guidelines for the diagnosis and management of familial long QT syndrome. The cardiac
Society of Australia and New Zealand (CSANZ). August 10, 2011.

7
http://www.csanz.edu.au/documents/guidelines/clinical_practice/Familial_Long_QT_Syndrome.pdf.
Accessed May 30, 2019.
Transgenomic, Inc. FAMILION® Comprehensive Genetic Tests for Cardiac Syndromes.
http://labs.transgenomic.com/cardiology-familion. Accessed April 17, 2018.
Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of
Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee
for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With
Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J Am Coll Cardiol.
2006;48(5):e247-346. Doi: 10.1016/j.jacc.2006.07.010.
Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of
Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee
for Practice Guidelines (writing committee to develop guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death): developed in collaboration with
the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114(10):e385-
484. Doi: 10.1161/CIRCULATIONAHA.106.178233.
Peer-reviewed references:
Ackerman MJ. Cardiac causes of sudden unexpected death in children and their relationship to seizures
and syncope: genetic testing for cardiac electropathies. Semin Pediatr Neurol. 2005;12(1):52-58. Doi:
10.1016/j.spen.2005.02.002.
Antzelevitch C, Pollevick GD, Cordeiro JM, et al. Loss-of-function mutations in the cardiac calcium
channel underlie a new clinical entity characterized by ST-segment elevation, short QT intervals, and
sudden cardiac death. Circulation. 2007;115(4):442-449. Doi: 10.1161/CIRCULATIONAHA.106.668392.
Barsheshet A, Goldenberg I, O-Uchi J, et al. Mutations in cytoplasmic loops of the KCNQ1 channel and
the risk of life-threatening events: implications for mutation-specific response to beta-blocker therapy in
type 1 long-QT syndrome. Circulation 2012;125(16):1988-1996. Doi:
10.1161/CIRCULATIONAHA.111.048041.
Beitland S, Platou ES, Sunde K. Drug-induced long QT syndrome and fatal arrhythmias in the intensive
care unit. Acta Anaesthesiol Scand. 2014;58(3):266-272. Doi: 10.1111/aas.12257.
Brenyo A., Huang, D., Aktas. M. Congenital long and short QT syndromes. Cardiology. 2012;122:237-247.
Doi: 10.1159/000339537.

8
Costa J, Lopes CM, Barsheshet A, et al. Combined assessment of sex- and mutation-specific information
for risk stratification in type 1 long QT syndrome. Heart Rhythm. 2012;9(6):892-898. Doi:
10.1016/j.hrthm.2012.01.020.
Goldenberg, I, Horr, S, Moss, A, et al. Risk for life-threatening cardiac events in patients with genotype-
confirmed long-QT syndrome and normal-range corrected QT intervals. J Am Coll Cardiol. 2011;57(1):51-
59. Doi: 10.1016/j.jacc.2010.07.038.
Gonzalez FM, Veneziano MA, Puggina A, Boccia S. A systematic review on the cost-effectiveness of
genetic and electrocardiogram testing for long QT syndrome in infants and young adults. Value Health.
2015;18(5):700-708. Doi: 10.1016/j.jval.2015.03.1788.
Ishikawa S, Yamada T, Kuwata T, et al. Fetal presentation of long QT syndrome--evaluation of prenatal
risk factors: a systematic review. Fetal Diagn Ther. 2013;33(1):1-7. Doi: 10.1159/000339150.
Kapa S, Tester DJ, Salisbury BA, et al. Genetic testing for long-QT syndrome: distinguishing pathogenic
mutations from benign variants. Circulation. 2009;120(18):1752-1760. Doi:
10.1161/CIRCULATIONAHA.109.863076.
Kapplinger JD, Tester DJ, Salisbury BA, et al. Spectrum and prevalence of mutations from the first 2,500
consecutive unrelated patients referred for the FAMILION long QT syndrome genetic test. Heart Rhythm.
2009;6:1297-1303. Doi: 10.1016/j.hrthm.2009.05.021.
Modell S, Bradley D, Lehmann M. Genetic testing for long QT syndrome and the category of cardiac ion
channelopathies. PLoS Curr. 2012. Doi:10.1371/4f9995f69e6c7.
Moss AJ, Goldenberg I. Importance of knowing the genotype and the specific mutation when managing
patients with long QT syndrome. Circ Arrhythm Electrophysiol. 2008;1(3):213-226. Doi:
10.1161/CIRCEP.108.796599.
Moss AJ, Shimizu W, Wilde AA, et al. Clinical aspects of type-1 long-QT syndrome by location, coding
type, and biophysical function of mutations involving the KCNQ1 gene. Circulations. 2007;115(19):2481-
2489. Doi: 10.1161/CIRCULATIONAHA.106.665406.
Refsgaard L, Holst AG, Sadjadieh G, et al. High prevalence of genetic variants previously associated with
LQT syndrome in new exome data. Eur J Hum Genet. 2012;20(8):905-908. Doi: 10.1038/ejhg.2012.23.
Schwartz PJ, Stramba-Badiale M, Crotti L, et al. Prevalence of the congenital long-QT syndrome.
Circulation. 2009;120(18):1761-1767. Doi: 10.1161/CIRCULATIONAHA.109.863209.

9
Sy RW, Chattha IS, Klein GJ, et al. Repolarization dynamics during exercise discriminate between LQT1
and LQT2 genotypes. J Cardiovasc Electrophysiol. 2010;21(11):1242-1246. Doi: 10.1111/j.1540-
8167.2010.01788.x.
Tester DJ, Ackerman MJ. Genetic testing for potentially lethal, highly treatable inherited
cardiomyopathies/channelopathies in clinical practice. Circulation. 2011;123(9):1021-1037. Doi:
10.1161/CIRCULATIONAHA.109.914838.
Taggart NW, Haglund CM, Tester DJ, Ackerman MJ. Diagnostic miscues in congenital long-QT syndrome.
Circulation. 2007;115(20):2613-2620. Doi: 10.1161/CIRCULATIONAHA.106.661082.
Vetter VL. Clues or miscues? How to make the right interpretation and correctly diagnose long-QT
syndrome. Circulation. 2007:115(20):2595-2598. Doi: 10.1161/CIRCULATIONAHA.107.700195.
Centers for Medicare & Medicaid Services National Coverage Determinations: No National Coverage Determinations identified as of the writing of this policy. Local Coverage Determinations L34519 Molecular Pathology Procedures.
Commonly submitted codes Below are the most commonly submitted codes for the service(s)/item(s) subject to this policy. This is not an exhaustive list of codes. Providers are expected to consult the appropriate coding manuals and bill accordingly.
CPT Code Description Comment
81403
Molecular pathology procedure, Level 4 (eg, analysis of single exon by DNA sequence analysis, analysis of >10 amplicons using multiplex PCR in 2 or more independent reactions, mutation scanning or duplication/deletion variants of 2-5 exons)
81405
Molecular pathology procedure, Level 6 (eg, analysis of 6-10 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 11-25 exons, regionally targeted cytogenomic array analysis) CASQ2 (calsequestrin 2 [cardiac muscle]) (eg, catecholaminergic polymorphic ventricular tachycardia), full gene sequence.
81406
Molecular pathology procedure level (Includes KCNH2 (potassium voltage-gated channel, subfamily H [eag-related], member 2) (eg, short QT syndrome, long QT syndrome), full gene sequence and KCNQ1 (potassium voltage-gated channel, KQT-like subfamily, member 1) (eg, short QT syndrome, long QT syndrome), full gene sequence
81407 Molecular pathology procedure level 8 (includes SCN5A (sodium channel,

10
CPT Code Description Comment
voltage-gated, type V, alpha subunit) (eg, familial dilated cardiomyopathy), full gene sequence
81408
Molecular pathology procedure level 7 analysis of >50 exons in a single gene by DNA sequence analysisRYR2 (ryanodine receptor 2 [cardiac]) (eg, catecholaminergic polymorphic ventricular tachycardia, arrhythmogenic right ventricular dysplasia), full gene sequence or targeted sequence analysis of > 50 exons.
81413
Cardiac ion channelopathies (e.g., Brugada syndrome, long QT syndrome, short QT syndrome, catecholaminergic polymorphic ventricular tachycardia); genomic sequence analysis panel, must include sequencing of at least 10 genes, including ANK2, CASQ2, CAV3, KCNE1, KCNE2, KCNH2, KCNJ2, KCNQ1, RYR2, and SCN5A
81414
Cardiac ion channelopathies (eg, Brugada syndrome, long QT syndrome, short QT syndrome, catecholaminergic polymorphic ventricular tachycardia); duplication/deletion gene analysis panel, must include analysis of at least 2 genes, including KCNH2 and KCNQ1
ICD-10 Code Description Comment
I45.81 Long QT syndrome.
Q23.8-Q23.9 Other and unspecified congenital malformations of aortic and mitral valves
Q24.8 Other specified congenital malformations of heart
HCPCS Level II Code
Description Comment
S0265 Genetic counseling, under physician supervision, each 15 minutes.