Embed Size (px)
Citation preview

Human subjects gave written,informed consent to the study protocol,which was approved by the YaleHuman Investigational Committee, andcomplies with the Declaration ofHelsinki Principles.
CONFLICT OF INTERESTThe authors state no conflict of interest.
ACKNOWLEDGMENTSWe thank Gerald Goh, Emily Hast, Vincent Klump,Akdes Serin, and Jade Wititsuwannakul for techni-cal assistance, Ben Yu for careful discussion of dataand potential mechanisms, and Murat Gunel forhelpful conversations. This work was supported bya Doris Duke Charitable Foundation ClinicalScientist Development Award to KAC, who is alsothe recipient of a NIH/NIAMS K08 award(K08AR056305), and by the Yale Center for Men-delian Genomics (NIH U54 HG006504). JLL isthe recipient of a NIH-NHLBI Medical StudentResearch Fellowship. This report was concurrentlysubmitted with the publication of Bryan K. Sun,Andrea Saggini, Kavita Y. Sarin, Jinah Kim, LatanyaBenjamin, Philip E. LeBoit, and Paul A. Khavari(2012) Mosaic activating RAS mutations in nevussebaceus and nevus sebaceus syndrome.
Jonathan L. Levinsohn1, Li C. Tian1,Lynn M. Boyden2, Jennifer M. McNiff1,Deepak Narayan3, Erin S. Loring2,Duri Yun4, Jeffrey L. Sugarman5,John D. Overton2,6, Shrikant M. Mane2,6,Richard P. Lifton2,6,7, Amy S. Paller4,Annette M. Wagner4, Richard J. Antaya1,8
and Keith A. Choate1
1Department of Dermatology, Yale UniversitySchool of Medicine, New Haven, Connecticut,USA; 2Department of Genetics, Yale UniversitySchool of Medicine, New Haven, Connecticut,USA; 3Department of Surgery, Yale UniversitySchool of Medicine, New Haven, Connecticut,USA; 4Department of Dermatology,Northwestern University, Feinberg School ofMedicine, Chicago, Illinois, USA; 5Departmentsof Dermatology and Family Medicine,University of California, San Francisco, SanFrancisco, California, USA; 6Yale Center forMendelian Genomics, New Haven,Connecticut, USA; 7Howard Hughes MedicalInstitute, Yale University School of Medicine,New Haven, Connecticut, USA and8Department of Pediatrics, Yale UniversitySchool of Medicine, New Haven, Connecticut, USAE-mail: [email protected]
This work was done in New Haven, Connecticut.
SUPPLEMENTARY MATERIAL
Supplementary material is linked to the onlineversion of the paper at http://www.nature.com/jid
REFERENCES
Blaschko A (1901) Die Nervenverteilung in derHaut in ihrer Beziehung zu den Erkrankungender Haut. Braumuller. Vienna, Austria andLeipzig, Germany
Cribier B, Scrivener Y, Grosshans E (2000) Tumorsarising in nevus sebaceus: a study of 596cases. J Am Acad Dermatol 42:263–8
Grewal T, Koese M, Tebar F et al. (2011) Differ-ential Regulation of RasGAPs in Cancer.Genes Cancer 2:288–97
Groesser L, Herschberger E, Ruetten A et al. (2012)Postzygotic HRAS and KRAS mutations causenevus sebaceous and Schimmelpenning syn-drome. Nat Genet 44:783–7
Hafner C, Toll A, Gantner S et al. (2012) Keratino-cytic epidermal nevi are associated with mosaicRAS mutations. J Med Genet 49:249–53
Knudson AG (2001) Two genetic hits (more or less)to cancer. Nat Rev Cancer 1:157–62
Lapouge G, Youssef KK, Vokaer B et al. (2011)Identifying the cellular origin of squamous skintumors. Proc Natl Acad Sci USA 108:7431–6
Moody MN, Landau JM, Goldberg LH (2012)Nevus sebaceus revisited. Pediat Dermatol29:15–23
Moss C, Larkins S, Stacey M et al. (1993) Epidermalmosaicism and Blaschko’s lines. J Med Genet30:752–5
Mukhopadhyay A, Krishnaswami SR, Yu BD (2011)Activated Kras alters epidermal homeostasisof mouse skin, resulting in redundant skin anddefective hair cycling. J Invest Dermatol131:311–9
Solomon LM, Esterly NB (1975) Epidermal andother congenital organoid nevi. Curr ProblPediatr 6:1–56
Tuveson DA, Shaw AT, Willis NA et al. (2004)Endogenous oncogenic K-ras(G12D) stimulatesproliferation and widespread neoplastic anddevelopmental defects. Cancer Cell 5:375–87
Waltz KM, Helm KF, Billingsley EM (1999) Thespectrum of epidermal nevi: a case of verru-cous epidermal nevus contiguous with nevussebaceus. Pediat Dermatol 16:211–3
Xin H, Matt D, Qin JZ et al. (1999) The sebaceousnevus: a nevus with deletions of the PTCHgene. Cancer Res 59:1834–6
Genetic Profiling of BRAF Inhibitor–InducedKeratoacanthomas Reveals No Induction of MAPKinase Pathway ExpressionJournal of Investigative Dermatology (2013) 133, 830–833; doi:10.1038/jid.2012.353; published online 27 September 2012
TO THE EDITORThe new RAF inhibitor vemurafenibrepresents one of the first specifi-cally targeted drugs for melanoma(Bollag et al., 2010; Flaherty et al.,2010; Joseph et al., 2010). However,some individuals receiving vemurafenibdevelop eruptive squamous neo-plasms such as keratoacanthomas (KAs)
(Chapman et al., 2011). KAs areusually considered low-grade squa-mous proliferations (Cribier et al.,1999; Clausen et al., 2006), and areoften interpreted as a subtype ofsquamous cell carcinoma (SCC). Theirclinical course involves rapid growthfollowed by spontaneous involution.The mechanism by which KAs
develop is still unknown. Improvedunderstanding of the molecular andgenetic basis of KA formation wouldallow their improved management.
To investigate genes involved in thedevelopment of KAs in patients receiv-ing vemurafenib, we obtained biopsyspecimens and studied gene expressionprofiles by a microarray approach; fulldetails are available in the Supplemen-tary Material online. These biopsieswere originally obtained by theAbbreviations: KA, keratoacanthoma; MAP, mitogen-activated protein; SCC, squamous cell carcinoma
RP Kulkarni et al.Genetic Profiling of BRAF Inhibitor–Induced Keratoacanthomas
830 Journal of Investigative Dermatology (2013), Volume 133

submitting clinician and preserved informalin for standard paraffin embed-ding and sectioning and histopathologi-cal interpretation from the PathologyDepartment. We extracted RNA fromthe lesional cells in the paraffin block tocreate complementary DNA libraries,which were then screened using theAffymetrix U133plus 2.0 array (SantaClara, CA). We compared profiles ofKAs that arose after drug treatment tospontaneous KAs (arising in patientswho did not receive vemurafenib),
normal skin, and of classic cutaneousSCC after confirming the original histo-pathological diagnosis; five samples ofeach type were analyzed and all KAswere in the proliferative stage.
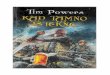
Unsupervised clustering of the mostvarying gene expression probes demon-strated that KA tumors were separablefrom both cutaneous SCC and normalskin (Figure 1a), but KAs from patientswith and without drug treatment werenot distinguishable from each other(Figure 1b). Having observed these
overall trends using unsupervised analy-sis, we used supervised analysis to con-firm that although there were 260 signi-ficantly differentially expressed probesbetween drug-induced KA and SCC,and 41 significantly differentially expre-ssed probes between drug-induced KAand normal skin, there were no probesthat were significantly differentiallyexpressed between drug-induced andspontaneous KAs (Bonferroni-correctedStudent’s t-test P-value p0.01). Weconcluded that drug-induced KA and
SCC 1SCC 2SCC 3SCC 4SCC 5SCC 6SCC 7SCC 8SCC 9
SCC 10Normal 1Normal 2Normal 3Normal 4Normal 5
KAD 5KA 6
KAD 2KA 8
KAD 3KAD 1KAD 4KA 10KA 9KA 7
KAD 5
KAD 2
KA 6
KA 8
KAD 3
KAD 1
KAD 4
KA 10
KA 9
KA 7
Figure 1. Unsupervised clustering of tumor and normal samples. (a, top) Clustering of all samples (squamous cell carcinoma (SCC), normal skin, and
keratoacanthoma (KA)/KA-drug). (b, bottom) Clustering of KA-drug versus KA tumors only. Hierarchical clustering of the top 500 most varying probes (highest,
coefficient of variation) segregates normal samples from SCC samples and both from all KA samples (spontaneous and drug derived). The normal samples form a
tight cluster. SCC tumors show overall similarity to normal tissue, with some tumors more similar to normal tissue than others. KA tumors are a distinct sample
group, but the type of KA tumor does not clearly distinguish the observed gene expression pattern.
RP Kulkarni et al.Genetic Profiling of BRAF Inhibitor–Induced Keratoacanthomas
www.jidonline.org 831

spontaneous KA tumors have the sameexpression profile.
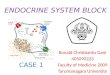
Recent reports have indicated thatdifferences in mitogen-activated protein(MAP) kinase gene expression arepotentially important for tumor progres-sion (Packer et al., 2009; Joseph et al.,2010; Nazarian et al., 2010; Poulikakoset al., 2010). In our data sets, genes ofthe MAP kinase pathway were notoverexpressed in either drug-inducedor spontaneous KA (relative to eachother or normal skin). To confirm this,we used quantitative reverse transcrip-tase–PCR to amplify several geneswithin the MAP kinase pathway andtransforming growth factor-b receptor 1.The results in Table 1 indicated nosignificant difference in expression.
We next examined downstreamtranscriptional targets of the MAP kinasepathway, including CCND1, DUSP6,SPRY2, ETV1, ETV5, FOSL1, andCXCL1, genes described as directlymodulated by vemurafenib inhibitionin BRAF V600E melanomas (Packeret al., 2009; Joseph et al., 2010). Nonewas found to be differentially expressed.
KAs and other squamous prolifera-tions generally occur on sun-damagedskin. The precise mechanisms thatunderlie the initiation and growth ofthese neoplasms remain unclear.Vemurafenib can activate the MAPkinase pathway in wild-type BRAF
melanoma in vitro, through either het-erodimerization of CRAF with BRAF oractivation of wild-type BRAF throughNRAS (Heidorn et al., 2010; Josephet al., 2010; Nazarian et al., 2010;Poulikakos et al., 2010). This effect istransient and may last only a few hours(Joseph et al., 2010). Side effects inmelanoma cells may be due tounintended activation of the MAPkinase or other pathways in wild-typeBRAF cells.
We found that in vemurafenib-asso-ciated KAs mRNA levels downstream ofBRAF are not increased relative tospontaneous KAs. These data suggestthat vemurafenib may accelerate a neo-plastic process in susceptible or sun-damaged keratinocytes, similar to theprocesses underlying spontaneous KAs,although any such activation is transi-ent. Hence, by biopsy time, enhancedactivation of the MAP kinase pathway isnot seen and there is no increase intranscripts of members of the MAPkinase pathway or of downstream tar-gets, despite continued therapy.
Another possibility is that vemurafe-nib and similar molecules cause differ-ent ‘‘off-target’’ effects that causeactivation through alternative mechan-isms. The induced effects may be dosedependent and additional studiesmay define the threshold at whichKAs occur in patients receiving
vemurafenib or related agents. Recently,Oberholzer et al. (2012) and Su et al.(2012) have noted that HRAS mutationsare overrepresented in vemurafenib-induced squamous neoplasms (in bothKA and SCC) compared with spontan-eous ones, and the drug may induceneoplastic proliferation in this setting.
One limitation of this study is thesmall sample size analyzed; nonethe-less, our findings indicate that KAsassociated with vemurafenib treatmenthave similar genetic profiles to sponta-neous KAs and similar expression of MAPkinase pathway genes. These data sug-gest that BRAF inhibitors may acceleratea neoplastic process in susceptiblekeratinocytes. However, any activationappears transient and drug-associatedKAs behave similarly as spontaneousKAs. Our results strongly suggest thatdrug-induced KAs should be treatedin a manner similar to spontaneousKAs. Although newer molecularly tar-geted drugs are presented as highlytarget specific, they may have ‘‘off-tar-get’’ effects on other proteins. Furtherstudy and monitoring will be impor-tant to fully understand the underlyingmechanisms.
CONFLICT OF INTERESTThe authors state no conflict of interest.
ACKNOWLEDGMENTSWe thank Jamie Zhou for his assistance with thereverse transcriptase–PCR experiments and AlistairCochran for a critical review of the manuscript.RPK acknowledges the Women’s DermatologicSociety for support. DJL acknowledges financialsupport from the Joseph B. Gould Foundation.SWB has received departmental funds fromthe Department of Pathology. No other fundingsources supported this research.
Rajan P. Kulkarni1, Seema Plaisier2,Seong H. Ra3, Xinmin Li3,Delphine J. Lee2, Joseph D. Hillman3
and Scott W. Binder3
1Division of Dermatology, UCLA MedicalCenter, Los Angeles, California, USA;2Department of Translational Immunology,Dirks/Dougherty Laboratory for CancerResearch, John Wayne Cancer Institute, SantaMonica, California, USA and 3Department ofPathology, UCLA Medical Center, Los Angeles,California, USAE-mail: [email protected] [email protected]
SUPPLEMENTARY MATERIAL
Supplementary material is linked to the onlineversion of the paper at http://www.nature.com/jid
Table 1. Fold differences in gene expression between the KA-drug andspontaneous KA samples, along with RT–PCR results for gene expression formain genes of the MAP kinase pathway and TGFbR1
GeneFold difference KA-drug
versus KAP-value folddifference
DDCT KA-drug versusKA
P-valueDDCT
ARAF �1.039 0.366 0.30 0.39
BRAF 1.012 0.822 0.10 0.75
CRAF 1.057 0.439 � 0.70 0.24
HRAS �1.048 0.106 0.90 0.11
KRAS �1.092 0.322 1.50 0.11
NRAS �1.017 0.841 0.20 0.69
MEK �1.019 0.838 4.00 0.14
ERK �1.031 0.302 0.30 0.54
TGFbR1 1.07 0.531 � 2.00 0.07
Abbreviations: KA, keratoacanthoma; MAP, mitogen-activated protein; RT–PCR; reverse transcriptase–PCR; TGFbR1, transforming growth factor b receptor 1.The expression of correlated probes was averaged and collapsed onto the t-test P-value. As noted, thereis no significant difference in gene expression from the microarray data or from RT–PCR data. For geneswhere multiple probes were available, the probe with smallest P-value is reported.
RP Kulkarni et al.Genetic Profiling of BRAF Inhibitor–Induced Keratoacanthomas
832 Journal of Investigative Dermatology (2013), Volume 133

REFERENCES
Bollag G, Hirth P, Tsai J et al. (2010) Clinicalefficacy of a RAF inhibitor needs broad targetblockade in BRAF-mutant melanoma. Nature467:596–9
Chapman PB, Hauschild A, Robert C et al. (2011)Improved survival with vemurafenib in mela-noma with BRAF V600E mutation. N Engl JMed 364:2507–16
Clausen OP, Aass HC, Beigi M et al. (2006) Arekeratoacanthomas variants of squamouscell carcinomas? A comparison of chromo-somal aberrations by comparative geno-mic hybridization. J Invest Dermatol 126:2308–15
Cribier B, Asch P, Grosshans E (1999) Differentiat-ing squamous cell carcinoma from kerato-acanthoma using histopathological criteria.
Is it possible? A study of 296 cases. Derma-tology 199:208–12
Flaherty KT, Puzanov I, Kim KB et al. (2010)Inhibition of mutated, activated BRAF in meta-static melanoma. N Engl J Med 363:809–19
Heidorn SJ, Milagre C, Whittaker S et al. (2010)Kinase-dead BRAF and oncogenic RAS coop-erate to drive tumor progression throughCRAF. Cell 140:209–21
Joseph EW, Pratilas CA, Poulikakos PI et al. (2010)The RAF inhibitor PLX4032 inhibits ERKsignaling and tumor cell proliferation in aV600E BRAF-selective manner. Proc NatlAcad Sci USA 107:14903–8
Nazarian R, Shi H, Wang Q et al. (2010) Melano-mas acquire resistance to B-RAF(V600E) inhi-bition by RTK or N-RAS upregulation. Nature468:973–7
Oberholzer PA, Kee D, Dziunycz P et al. (2012)RAS mutations are associated with thedevelopment of cutaneous squamous celltumors in patients treated with RAF inhibitors.J Clin Oncol 30:316–21
Packer LM, East P, Reis-Filho JS et al. (2009)Identification of direct transcriptionaltargets of (V600E)BRAF/MEK signalling inmelanoma. Pigment Cell Melanoma Res22:785–98
Poulikakos PI, Zhang C, Bollag G et al. (2010) RAFinhibitors transactivate RAF dimers and ERKsignalling in cells with wild-type BRAF. Nat-ure 464:427–30
Su F, Viros A, Milagre C et al. (2012) RASmutations in cutaneous squamous-cell carci-nomas in patients treated with BRAF inhibi-tors. N Engl J Med 366:207–15
A Single-Nucleotide Polymorphism in the Abcc6 GeneAssociates with Connective Tissue Mineralization in MiceSimilar to Targeted Models for Pseudoxanthoma ElasticumJournal of Investigative Dermatology (2013) 133, 833–836; doi:10.1038/jid.2012.340; published online 27 September 2012
TO THE EDITORPseudoxanthoma elasticum (PXE;OMIM#264800) is characterized byprogressive, late-onset, ectopic minera-lization of elastic fibers, clinically affect-ing skin, retina, and the cardiovascularsystem with considerable morbidity andoccasional mortality (Neldner, 1988). Itis an autosomal recessive disorder witha slight female preponderance and anestimated prevalence of B1 in 50,000–70,000. The clinical diagnosis is usuallymade through recognition of characteri-stic skin lesions, i.e., small, yellowishpapules on flexural areas progressivelycoalescing into plaques of inelastic,leathery skin. The cutaneous findingsare associated with angioid streaks inthe retina and mineralization of arterialblood vessels. Adding to the diagnosticdifficulty is the considerable phenotypicheterogeneity in age at onset and the
extent and severity of organ systeminvolvement. Since the identification ofmutations in the ATP-binding cassette,subfamily C, member 6 gene (ABCC6)as the genetic basis in the overwhelmingmajority of families with PXE, tremen-dous progress has been made inunderstanding the molecular genetics,clinical phenotypes, and pathogenesisof this disease (Uitto et al., 2010).
Mutations in the ABCC6 gene under-lie the classic form of PXE, and over 300distinct mutations representing over1,000 mutant alleles have been reported(Uitto et al., 2010). However, noapparent correlation has been establi-shed between PXE phenotypes and thenature or the position of the mutationsin ABCC6 (Pfendner et al., 2007).Genetic variations in gamma-glutamylcarboxylase (GGCX) (Vanakker et al.,2007; Li et al., 2009), secreted phospho-
protein 1 (SPP1) (Hendig et al., 2007),and xylosyltransferase I (XYLT) (Schonet al., 2006) genes, together withenvironmental risk factors such as diet(LaRusso et al., 2009), appear to modifythe phenotype with respect to the age atonset and the extent and severity oforgan involvement in PXE.
Understanding of the mechanismsunderlying PXE has been advanced bythe development of targeted mutantmice with genetic, histopathological,and ultrastructural features similar tothose in patients with PXE (Gorgelset al., 2005; Klement et al., 2005). Acharacteristic finding in the targetedmutant mouse (B6;129S1/SvImJ-Abcc6tm1Jfk) is the mineralization of thevibrissae dermal sheaths, the principalcomponents of which were calcium andphosphorus (Kavukcuoglu et al., 2012).This specialized hair follicle type is notfound in humans, and mineralizationof the vibrissae dermal sheath is veryunusual in mice. The genetic back-ground of mice can modify phenotypesassociated with a single gene mutationas is the case with this Abcc6tm1Jfk-null
Abbreviations: ATP-binding cassette, subfamily C, member 6 (gene symbol: Abcc6, mice; ABCC6, human;protein symbol for both: ABCC6); secreted phosphoprotein 1 (gene symbol: SPP1, human); SUMO/sentrin-specific peptidase 6 (gene symbol: SENP6, human; Senp6, mouse); xylosyltransferase I (gene symbol:XYLT, human; Xylt1 and 2, mouse); Casr, calcium-sensing receptor; DCC, dystrophic cardiac calcinosis;PXE, pseudoxanthoma elasticum; SNP, single-nucleotide polymorphism
A Berndt et al.Abcc6 Polymorphism and Ectopic Mineralization
www.jidonline.org 833