Embed Size (px)
Citation preview
Generalized Anxiety Disorder
A Patient-Centered, Evidence-Based Diagnostic and Treatment Process
A Presentation for the Students of Ohio University Heritage College of Osteopathic Medicine
Kendall L. Stewart, MD, MBA, DFAPANovember 29, 2011
Why is this important?
• Generalized Anxiety Disorder (GAD) is a very common disorder.
• The lifetime prevalence is 5-percent.• Females are affected about twice as
often.• In anxiety disorder clinics about 25-
percent of patients have presenting or comorbid GAD.
• Most of these patients will readily admit that they have been nervous worrywarts as long as they can remember.
• The usual course is chronic and fluctuating, and these people are worse during times of stress.
• There is a genetic contribution to the development of this disorder.1,2
• After mastering the information in this presentation, you will be able to– Describe how patients with GAD
often present,– Detail the diagnostic criteria,– Describe some of the associated
features,– List some differential diagnoses,– Write a preliminary treatment
plan, and– Identify some of the frequent
treatment challenges.
1 My mother was one of the worst worriers I’ve ever seen. She once woke me up to tell me about one ofher bad dreams. They experience every side effect and fret about the news.2 Our older son has inherited this tendency and once expressed his worry about my plane crashing.
How might a patient with GAD present?• This is a 53-year-old-man.• “I’ve been a worrywart for as
long as I can remember.”1,2
• “Most of what I worried about never happened, but I always think about the worst things that might occur.”
• “I always feel tense and restless.”
• “It’s like I’m trembling on the inside.”
• “Because of this, I’m often irritable.”
• “I have trouble falling asleep because I can’t get stuff off my mind.”
• “Sometimes I get so upset that I sweat, my mouth gets dry, my heart races.”
• “These symptoms come on gradually, not suddenly.”
• “My family doc put me on diazepam 20 years ago, and I couldn’t get by without it.”
• “I have never taken more than the doctor prescribed, but I can’t do without it.”
• You can listen to these patients describe their struggles here.
1 For these folk, there is always something to worry about.2 Three old men in the nursing home were worried about their bodily functions.
What associated features might you see?• Chronic muscle tension is common.• These patients may exhibit an exaggerated
startle response.• Mood disorders very frequently co-occur.• Other anxiety disorders also frequently co-occur.1,2
• These patients are also at higher risk for developing substance use disorders.
• The general medical disorders that are often associated with stress such as headache and irritable bowel syndrome are frequently present also.
• These patients frequently use somatic complaints to describe emotional discomfort.
1 50 to 90-percent of people with GAD have another mental disorder.2 The female-to-male ratio for GAD is 2-to-1.
What other diagnoses might you include in the differential diagnosis?
1 I experienced real anxiety waiting to hear about Jonathan..
• Normal anxiety1
– Waiting for 3 hours for news of your wife’s first C-section• Other anxiety disorders
– GAD may be the “foundation” disorder. • Anxiety secondary to a general medical condition
– Pheochromocytoma– Hyperthyroidism
• Substance-induced anxiety– Caffeine is the most common culprit.– Withdrawal from alcohol is also common.
• Anxiety secondary to other psychiatric disorders– All of them.
What might a typical treatment plan look like?• Generalized anxiety
– Provide reassurance.– Suggest discontinuance of all
caffeine.– Consider no treatment at all.1,2
– Try all non-medicinal interventions next.
– Use the anxiety pyramid.– Consider buspirone 15 mg twice
per day.– Consider rare benzodiazepine use.– Reserve chronic benzodiazepine
use for those people who• Do not respond adequately to any
other intervention• Respond dramatically to routine
medication use,• Do not suffer unacceptable side
effects, and• Do not abuse the medication.
• Other comorbid disorders– Diagnose and treat these conditions
vigorously.• Maladaptive attitudes and behaviors
– Consider cognitive behavioral psychotherapy (CBT)
• Education and self help– Provide educational resources.– Recommend a daily exercise regimen.– Recommend a healthy diet.– Suggest healthy distractions.– Recommend meditation.– Recommend online resources with
caution.– Recommend self-help groups with
caution.
1 These people are miserable, but they are not miserable enough to change.2 People with troubled marriages often see a psychiatrist as a last resort.
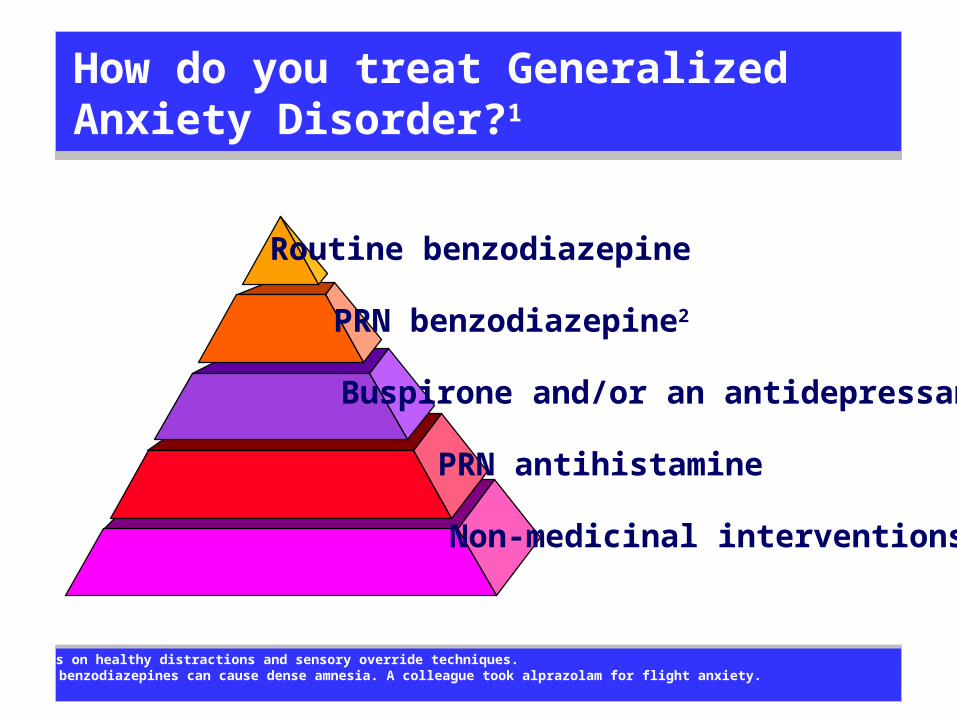
How do you treat Generalized Anxiety Disorder?1
Non-medicinal interventions
Buspirone and/or an antidepressant
PRN antihistamine
PRN benzodiazepine2
Routine benzodiazepine
1 Focus on healthy distractions and sensory override techniques.2 The benzodiazepines can cause dense amnesia. A colleague took alprazolam for flight anxiety.
What are some of the treatment challenges you can expect?
• These people are wired this way.• They do best when they are distracted.• They often confuse worry with love.• They sometimes demand pills, but they are often
willing to avoid them.• They annoy people around them, including their
physicians.1,2
• They always have physical complaints, and deciding when to order more tests and when not to is an ongoing challenge.
1 These folk are invested in their worries, and they love to talk about them. Staying awake can be a challenge.2 I can get a 30-second nap. Once, my notes flat lined. A mute child challenged a sleepy intern.
Where can you learn more?
• American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision, 2000
• Sadock, B. J. and Sadock V. A., Concise Textbook of Clinical Psychiatry, Third Edition, 2008
• Stern, et. al., Massachusetts General Hospital Comprehensive Clinical Psychiatry, 2008. You can read this text online here.
• Flaherty, AH, and Rost, NS, The Massachusetts Handbook of Neurology, April 2007
• Stead, L, Stead, SM and Kaufman, M, First Aid© for the Psychiatry Clerkship, Second Edition, March 2005
• Klamen, D, and Pan, P, Psychiatry Pre Test Self-Assessment and Review, Twelfth Edition, March 20093
• Oransky, I, and Blitzstein, S, Lange Q&A: Psychiatry, March 2007• Ratey, JJ, Spark: The Revolutionary New Science of Exercise and the Brain,
January 2008• Medina, John,
Brain Rules: 12 Principles for Surviving and Thriving at Home, Work and School, February 2008
• Stewart KL, “Dealing With Anxiety: A Practical Approach to Nervous Patients,” 2000
Where can you find evidence-based information about mental disorders?
• Explore the site maintained by the organization where evidence-based medicine began at McMaster University here.
• Sign up for the Medscape Best Evidence Newsletters in the specialties of your choice here.
• Subscribe to Evidence-Based Mental Health and search a database at the National Registry of Evidence-Based Programs and Practices maintained by the Substance Abuse and Mental Health Services Administration here.
• Explore a limited but useful database of mental health practices that have been "blessed" as evidence-based by various academic, administrative and advocacy groups collected by the Iowa Consortium for Mental Health here.
• Download this presentation and related presentations and white papers at www.KendallLStewartMD.com.
• Learn more about Southern Ohio Medical Center and the job opportunities there at www.SOMC.org.
• Review the exceptional medical education training opportunities at Southern Ohio Medical Center here.
How can you contact me?1
Kendall L. Stewart, M.D.VPMA and Chief Medical OfficerSouthern Ohio Medical Center
Chairman & CEOThe SOMC Medical Care Foundation, Inc.
1805 27th StreetWaller Building
Suite B01Portsmouth, Ohio 45662
740.356.8153
[email protected] [email protected]
www.somc.orgwww.KendallLStewartMD.com
1Speaking and consultation fees benefit the SOMC Endowment Fund.
Safety Quality Service Relationships Performance
Are there other questions?
Jeffrey Hill, DOOUCOM 1987
Darren Adams, DOOUCOM 2002