Embed Size (px)
Citation preview

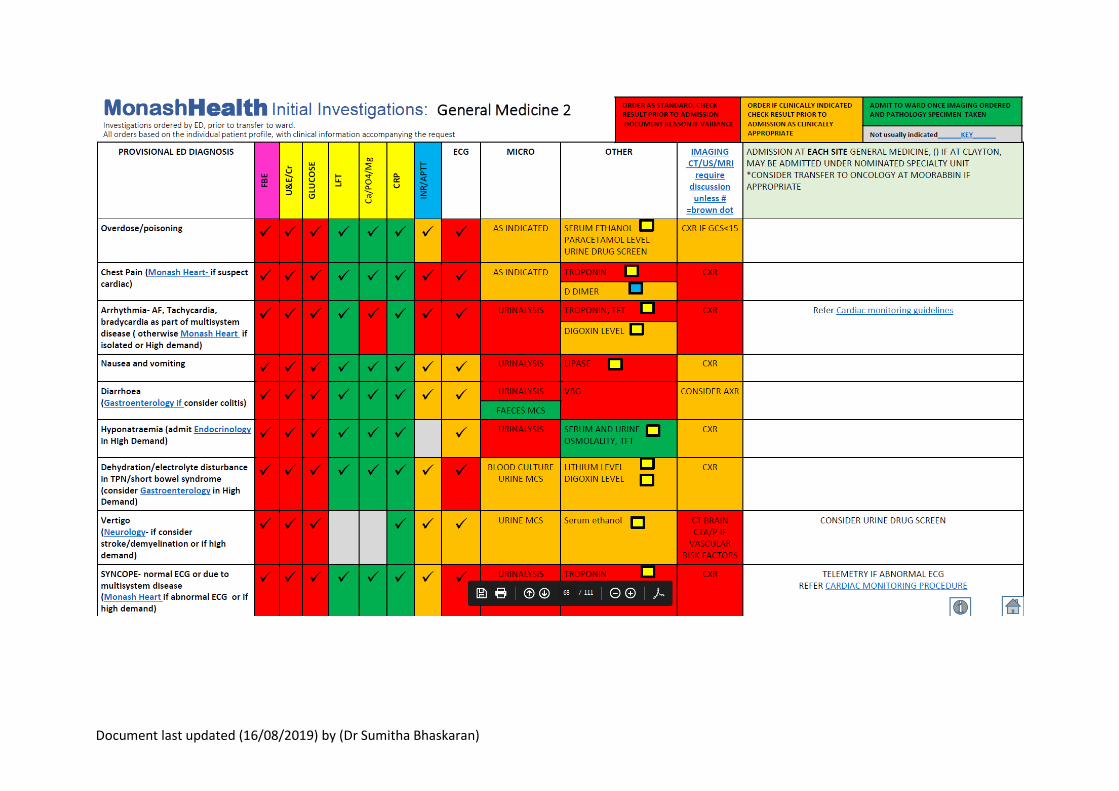
Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
General Medical Registrar Responsibilities
Welcome to Monash Medical Centre General Medicine. We hope you enjoy the experience. This
booklet is reference guide to the registrar roles in general medicine.
Handover
Clinical handover is a national standard and failure in handover is a major preventable harm.
Handover at MMC general medicine must be provided at the following times:
Between shifts
a. Morning Handover – 0800 at the Level 4 Conference room – attended by night
medical registrar and incoming day unit registrars, MAPs registrar and Intake
registrar
b. Afternoon handover – between day unit registrars and wards after hours
registrar
c. Evening handover – 2130 between ward after hours medical registrar, intake
registrar and incoming night registrar
Patients transferred between units / hospitals (Dandenong, Casey, Kingston, Moorabbin
Transfers)
Patients transferred from ICU
What to handover:
Sick patients – anyone who has had a recent MET call or a Code Blue during the shift
Patients that have had a fall during the shift
Patients transferred from units or another hospital during that shift
Deaths that occurred during that shift
Outstanding admissions / reviews
Outstanding investigations for follow up
Outstanding procedures

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
Intake Registrar
There are two intake registrars during the day. One registrar starts from 0800 to 1730 and the
second registrar starts from 1500 to 2200 on Mondays to Wednesdays and 1300 to 2200 on
Thursdays to Sundays.
The Intake registrar shares the role of carrying the MET call pager with the MAPs registrar.
- Mondays to Thursday : MAPS registrar carries MET call pager from 0800 – 1230, Intake
registrar carries MET pager from 1230 onwards
- Fridays: Intake registrar will carry MET call pager from 0800 as the MAPS registrar is at
clinic in the morning.
The role of the intake registrar is to take referrals from the Emergency Department for admission
and to assist with the coordination of flow of patients.
o Review time critical patients within 30 minutes of referral,
o Review all other referrals within one hour, or
o Agree a plan with ED and choose to see a patient on the ward within 4 hours (stable
patients only)
ii. If a referral to another inpatient unit is more appropriate, the admitting registrar must cross-
refer (not ED).
iii. If a specialty registrar thinks referral is not appropriate, they must cross-refer to the General
Medicine registrar / General Medical Consultant (again, not ED). The General Medicine
registrar will decide the unit that the patient is to be admitted under, after consultation with
the General Medicine Consultant on-call.
iv. Disputes which cannot be managed at registrar level must be escalated to consultant level.
v. Please see PROMPT document – Prioritising Patient Care
http://prompt/Search/download.aspx?filename=27248204\27248212\38752147.pdf
And the Initial Investigations Pathways –
https://system.prompt.org.au/Download/Document.aspx?id=34997967&code=801EC71FB25
D5128F6A0D857D9ADEFCD
Escalation to Consultant:
i. Issues that should be escalated to the consultant include: o Any concern about patient’s condition, or need assistance/clarification regarding
management plan o There is disagreement between staff, different specialty teams, patient, and/or
patient’s family regarding ongoing care. o There is a deterioration in a patient’s condition in such that the patient becomes:
Seriously ill patient, or existing stable patient becomes unstable
Referred/admitted to ICU
Code Blue call is made

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
Patient requires emergency and unplanned surgery o In the event of a MET call the consultant on-call should be informed in a timely fashion.
If there are multiple MET calls on the same patient, the on-call consultant should be notified more urgently.
o Decisions about treatment or discharge made on request/opinion of patient’s private consultant
o There is a serious adverse event, or prior to open disclosure ii. Please contact the on-call consultant every evening at 9pm to provide an update, especially
about unstable patients.
Patient transferred from external sites (Dandenong/Moorabbin/Casey/Kingston/other hospitals)
i. Any referrals you receive from an external hospital for admission to general medicine directly
MUST be discussed and accepted by the on-call general medicine consultant.
ii. Please see PROMPT document – Patient transfer between sites urgent and non-urgent (Adult) http://prompt/Search/download.aspx?filename=1826085\24476024\46910181.pdf
iii. Patients accepted under Gen Med from other units need to be documented in the admission book, and be handed over to subsequent admitting medical registrar if patient does not arrive during receiving registrar’s shift.
iv. If patient is to be transferred to a high-level monitoring unit (ICU, CCU, respiratory HDU, neuro HDU), the transferring team is to notify the respective teams (ICU, cardiology, respiratory, or neurology/neurosurgery).
v. If the patient is received in ED, the ED registrar is to receive and attend to the patient until the accepting team registrar arrives in ED.
Community Supports as Alternatives to Hospital Admission
Consider these referrals for the suitability of patients to be transferred directly to Kingston Centre
(please review ED to subacute transfer policy on prompt) or for discharge of patients to community
services such as complex care, Hospital in the Home or InReach.
Hospital In The Home:
Community Acquired Pneumonia
Cellulitis on IV antibiotics
Heart Failure for IV Frusemide
UTI on IV antibiotics
They are available 24 hours 7 days a week (including public holidays). Contact HITH consultant via
switchboard (0800 – 2200) or HITH nurse overnight (2200 to 0800)
InReach:
Serviced by Geriatricians from Monash Health with registrar and nursing support. InReach will
attend anyone from a nursing home (excluding SRS or boarding house). Consult family about
returning patient back to nursing home. Available 24 hours 7 days a week including public holidays
Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
Residential InReach: Call – on 1300 4467 3224 (1300 4 INREACH)
Complex Care:
Conditions such as COPD/Asthma/Heart failure where the presentation is preventable (excluding mental health as primary reason for presentation). On discharge the patient will be receive a comprehensive home based assessment, care coordination and timely responsive specialist care. Call - Complex Care ED Liaison – on 0410318425 (Business Hours – Mon- Fri) ED to Kingston Centre direct transfers Patients meeting suitability criteria may be transferred from ED to subacute (Kingston Centre directly). In order to utilise this process, patients need to physically be in ED or short stay. Transfers can only occur between 0800 – 1800, 7 days a week (for latest arrival to Kingston by 1900). If transport is delayed patients may stay in SSU for early morning departure, provided a bed is available at Kingston. See prompt document for suitability and process. http://prompt/Search/download.aspx?filename=27248204\27248212\43721036.pdf. Suitability Criteria:
- Patient is being assessed in ED - Patients with injuries who would normally function independently at home and no
surgery is required (eg stable non operative fractures or soft issue injuries) - Patients requiring geriatric evaluation due to increasing difficulty managing at home - Recurrent falls with no medical condition that require acute admission - Requiring stabilisation of chronic medical conditions but not acutely unwell - Well partner of a sick carer needing hospitalisation when respite is unavailable - Minor problems who need short term treatment away from home - Patient is safe for transfer and family and patient consent to transfer - Patients over 65 years with complex social needs not acutely unwell
Exclusions: - Infectious isolation needed - Significantly altered conscious stages - Recent head injuries - Hip pain unless fracture ruled out on CT or bone scan - Mental health issues, alcohol dependency - New dialysis arrangements - Acute delirium with behavioural concerns that are likely to worsen with transfer - Unable to tolerate transfer dur to pain - Absconding risk
First contact bed access to check for bed availability if available then contact Kingston Centre MET Registrar to discuss transfer on pager #8075 or by mobile via switchboard 92. If unable to contact Kingston MET registrar contact, Dr Helena Ng or Dr Han Mei Pan via switch on weekdays or the on-call consultant on weekends. Casey Suitable Transfer Any general medical patient requiring admission, if clinically suitable should be considered for Casey admission if beds are available.
Clinically Suitable

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
Stable patients not likely to require ICU/HDU or NIV
Specialty Input available o Psychiatry o Endocrinology (2 x weekly) o Neurology (2 x weekly) o ID (1 x weekly) o Urology & ENT o Beware: time of transfer for patients with Behaviours of Concern
o Limit to working hours with full staffing ratios
Not appropriate for patients requiring
Telemetry- for acute coronary syndrome
MRI
Requiring further/ongoing orthopaedic, vascular or plastics input as inpatient or acute General Surgical input (need for ongoing Gen Surg input should be discussed with Gen Surg at Casey)
Undifferentiated abdominal pain
Specialty input not mentioned above
1. Preference for patient transfer directly from the emergency department, to reduce clinical risk and provide continuity of care and a positive patient experience.
2. Inform the patient and NOK regarding transfer to Casey Hospital to the next available inpatient bed
3. The ED bed request should be updated by either the GML, ED Nurse In Charge, ED Medical to reflect Casey Gen Med. This process will then inform bed access and Casey Inpatient wards of a planned incoming transfer and the bed will allocated.
4. Clinical handover should occur when patient transport is imminent to ensure:
The patient is still stable and appropriate for transfer
The receiving registrar receiving the handover will be the registrar receiving the patient
5. Refer to Monash Health Procedure, Patient transfer between Sites –Adult http://prompt/Search/download.aspx?filename=1826085\24476024\38694688.pdf
6. Clinical handover to the Casey Registrar on ext- 82152 or pager #2538 using the ISBAR format. If the receiving registrar has any clinical concerns, this should be discussed with the Consultant on call for advice.

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
1. Blunt Chest Traumas in the Elderly (>65 years) i. Please see PROMPT document - Blunt chest trauma in the elderly: Assessment and Disposition.
ii. Blunt chest traumas in the elderly requires Acute General Surgery admission +/- Cardiothoracics referral depending on Chest trauma score (CTS).

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
2. Abdominal Pain i. Please see PROMPT documents – Emergency Department Abdominal Pain management
(Adult) Procedure and Abdominal Pain Referral ii. As a general rule, General Medicine does not admit patients with undifferentiated
abdominal pain, however we would admit patients with other provisional diagnoses (e.g. UTI, pneumonia, simple/uncomplicated gastroenteritis, palliative management for abdominal metastatic disease).
iii. “NOT Surgical/Not acute abdomen/Not for theatre” and other non-diagnostic comments are unacceptable as noted in the PROMPT protocol.
Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
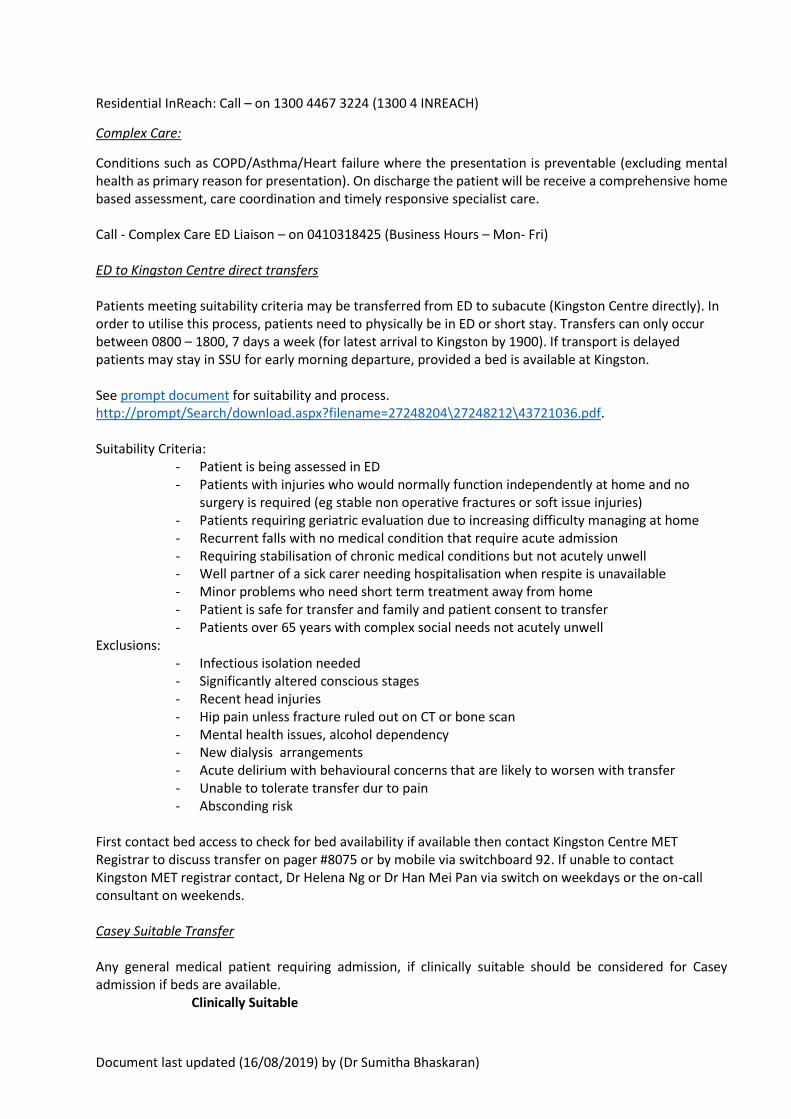
3. Acute, Severe Back Pain i. Please see PROMPT documents :
https://system.prompt.org.au/download/document.aspx?id=16104966&code=0D00F843887C6B7173E8A4C26E595878 And http://prompt/Search/download.aspx?filename=27248204/27248212/21271118.pdf It is important the criteria for urgent MRI below be documented both in the patient notes and on the imaging request
ii. There is no need to discuss with neurology/neurosurgery for approval prior to requesting MRI if patient fits criteria for urgent imaging.
Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
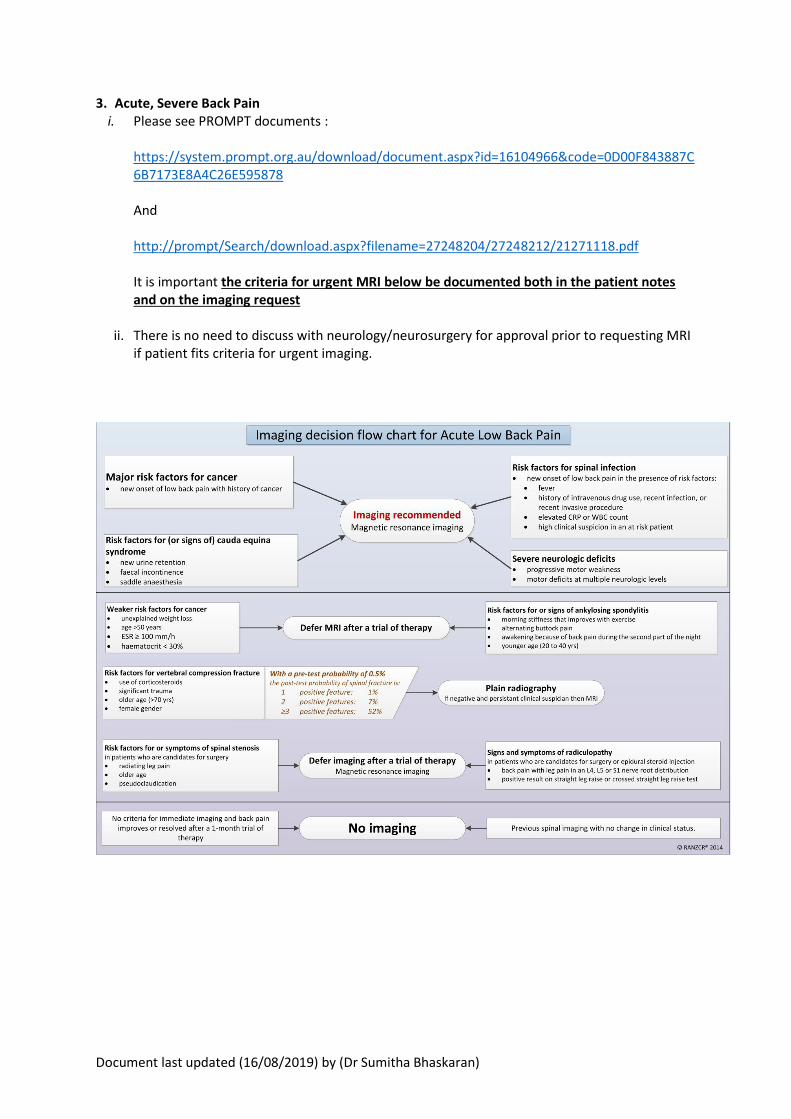
4. Sepsis - Please see PROMPT document – Sepsis Pathway (Adult)

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)


Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
Medical Assessment and Perioperative Service (MAPS)
registrar
The MAPS registrar carries the consults pager (#236) and MET pager (#120). The primary role of the
MAPS registrar is to provide comprehensive medical support to surgical, psychiatry and medical
speciality units across the hospital service.
MET Calls
The MAPS registrar is responsible for carrying the MET call pager from 0800 – 1230 most days except
Fridays. This role is shared with the intake registrar. The MAPS registrar must hold the met call pager
during the 0800 morning handover.
Handover
The MAPS registrar should attend the morning handover at the level 4 conference room every
morning to get a handover from the night registrar regarding any outstanding referrals that need to
be seen.
Code Greys
Code greys around the hospital require a medical trainee to attend, except those that occur in the
psychiatry ward and in ED.
• Code Grey is a medical response
• All general medical registrars are expected to complete Code Grey Training
• The MET call pager holding registrar and home unit of the patient are required to attend all
Code Greys
• The NM on code grey roster will lead the code grey (After hours NCO)
• The medical response is to:
• Work with the Code Grey team to deescalate the situation
• Determine if there is a medical trigger for the behaviour
• Refer for specialist input e.g. Drug & Alcohol team, Psychiatry, Pain Team,
Rehabilitation and Aged Care Liaison (RALs) for management of complex behaviours
• Put in place a plan to avert and avoid further Code Grey incidents in conjunction
with the home team
Escalate to on-call consultant / treating consultant if:
Code grey escalates to a MET call
If patient needs transfer to high acuity setting
Patient has multiple code greys in close succession with difficult to settle behaviours
Ensure you are code grey trained, if you have not received required training, please contact the
Head of Unit to organise training.

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
Refer to the acute behaviours disturbance guidelines for management strategies.
http://prompt/Search/download.aspx?filename=1824321\1824323\24417370.pdf
Consults and Take Over of Care
Most of these referrals will come from the surgical teams. If you are unsure about the management
of a patient you are consulting on discuss with the consultant rostered on for consults each week.
There is a roster of the consultants that are on for consults week by week in the gen med office on
the wall. (Check with Charmaine Martis / Jaclyn Gardner if in doubt)
All patients for takeover of care needs to be discussed with the consults consultant and accepted by
them. Once the consultant has accepted, inform the general medicine liaison nurse (0427 905 194)
with the patient details so that the patient can be added to the gen med list the following morning.
Clinics
Anaesthetic Clinic: Mondays 12.30pm
Introduce yourself to the anaesthetist working in clinics that day & ask them to direct you to any
patients that would benefit from a medical review. There will be some anaesthetic nurses that will
need you to screen the bloods of patients (particularly for anaemia). If someone is iron deficient,
without an obvious cause for the anaemia, refer them to the haematology anaemia clinic and
organise an iron infusion via HITH if they warrant one (this can be done via SMR).
Anaemia Clinic: Fridays 0830

Document last updated (16/08/2019) by (Dr Sumitha Bhaskaran)
Ward Registrars (Alpha and Delta Advanced Trainees +/- Bravo and
Echo registrars)
General Medicine Post-Discharge Clinic
Every Wednesday, 2pm, Day Treatment Centre, MMC
Registrars who attend: 2 advanced trainees – General Medicine Alpha and Delta Registrars (Gen
Med Bravo and Echo registrars may need to cover if the ATs are unavailable)
This clinic is designed to follow up patients who have been admitted and managed under the Clayton
Gen Med units, or patients who have been seen by the MAPS registrar as consults and discussed
with the Consults physician on-call. Direct referrals from other units or external referrals are not
accepted in this clinic.
Patients that are seen in this clinic should have clinical notes documented electronically on SMR,
using the “Gen Med Post Discharge Clinic E-Notes” template. They should also have a letter dictated
to their general practitioner/other relevant clinicians after the clinic, using Ozescribe/iMedX. Any
queries or issues regarding patients seen in the general medicine clinic should be discussed with Dr
Weejie Chee, or the Consults physician on-call should Dr Chee be unavailable.