Embed Size (px)
Citation preview
General introduction of nephrology
Xiaoqiang Ding M.D., Ph.D.
Department of nephrology
Zhongshan Hospital, Fudan University
Terminology
Kidney,renal
Nephrology
Scope of nephrology
Kidney diseases and other problems of the
urinary systems, no requirement for surgery
intervention
√ Glomerular disease:nephrotic syndrom, glomerulonephritis
√ Urinary tract infection
√ Interstitial nephritis
√ Acute renal failure or chronic renal failure
Blood purification: kidney disease or non-
kindey disease
Kidney functions
excreting metabolic waste products
√excreting redundant fluid and sodium
---hypertension
√eliminating dissoluable metabolic products,
exogenous drugs and toxins
---uremia
Kidney functions
Endocrine functions
√Erythropoiesis---erythropoietin
√Blood pressure---renin
√Bone and mineral metablism---VitD activation
Internal Environment Homeostasis regulation
fluid, acid-base homeostasis
√ Acid excretion---metabolic acidosis
√ Potassium excretion---hyperkalemia, hypokalemia
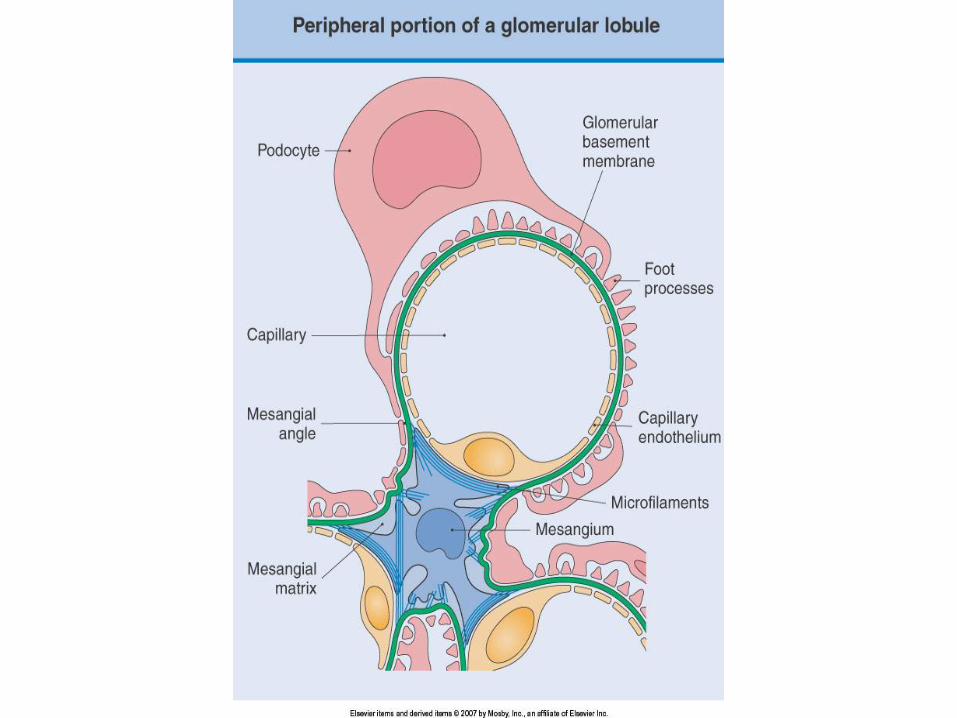
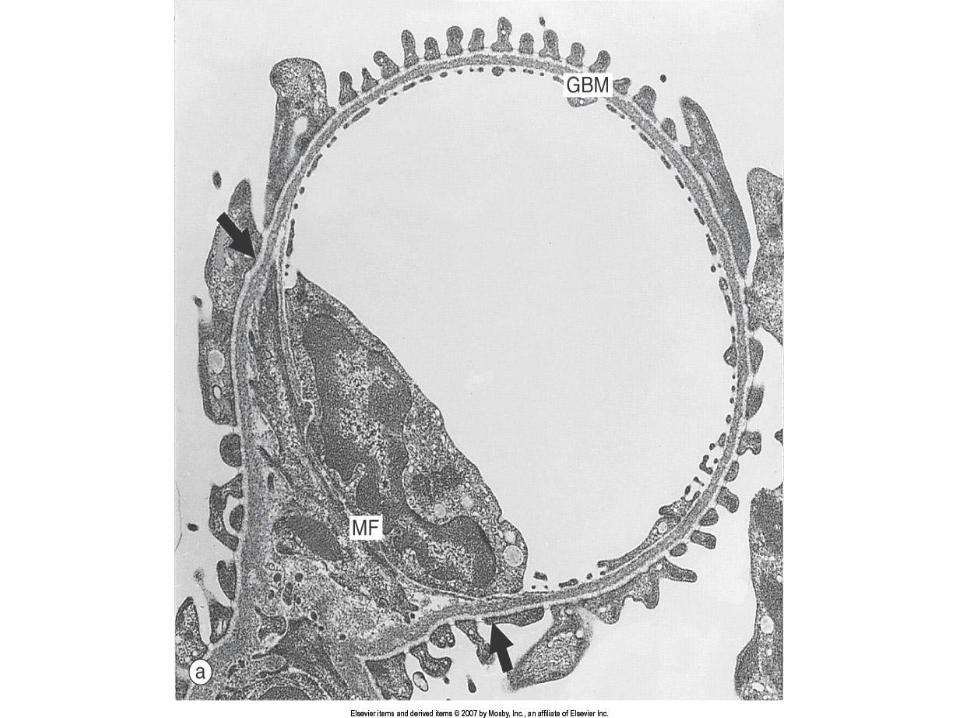

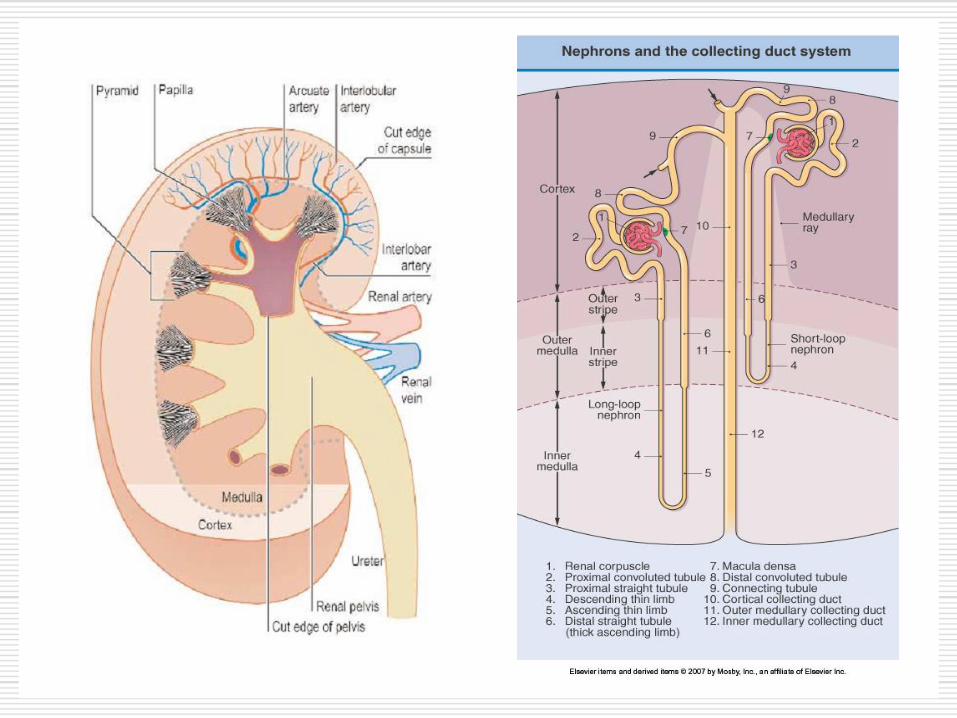
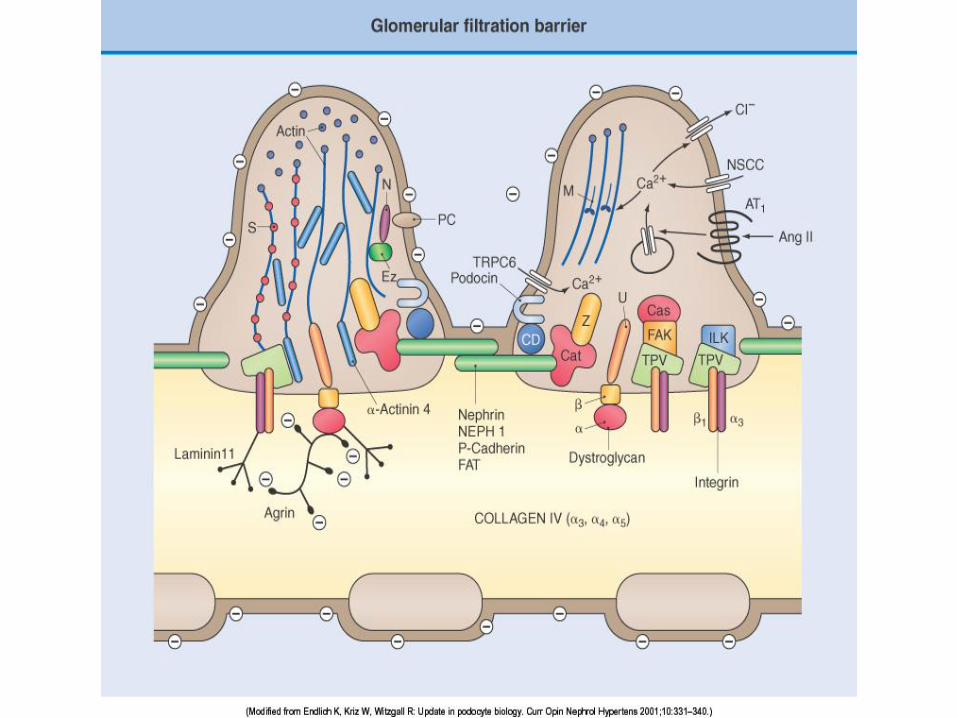
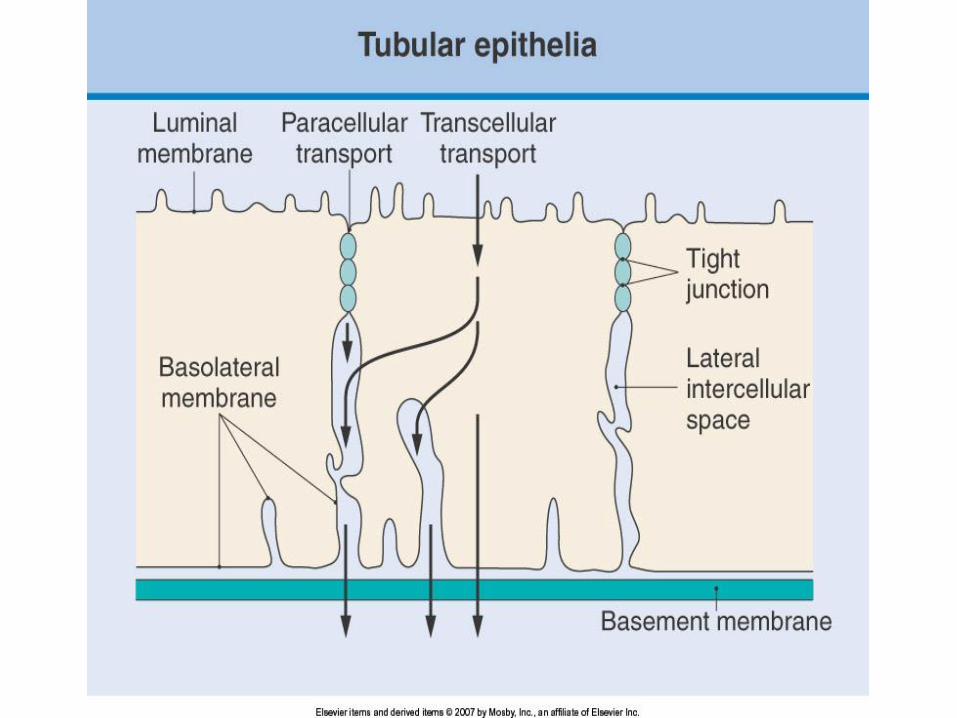
Foot processes
Endothelial fenestrae
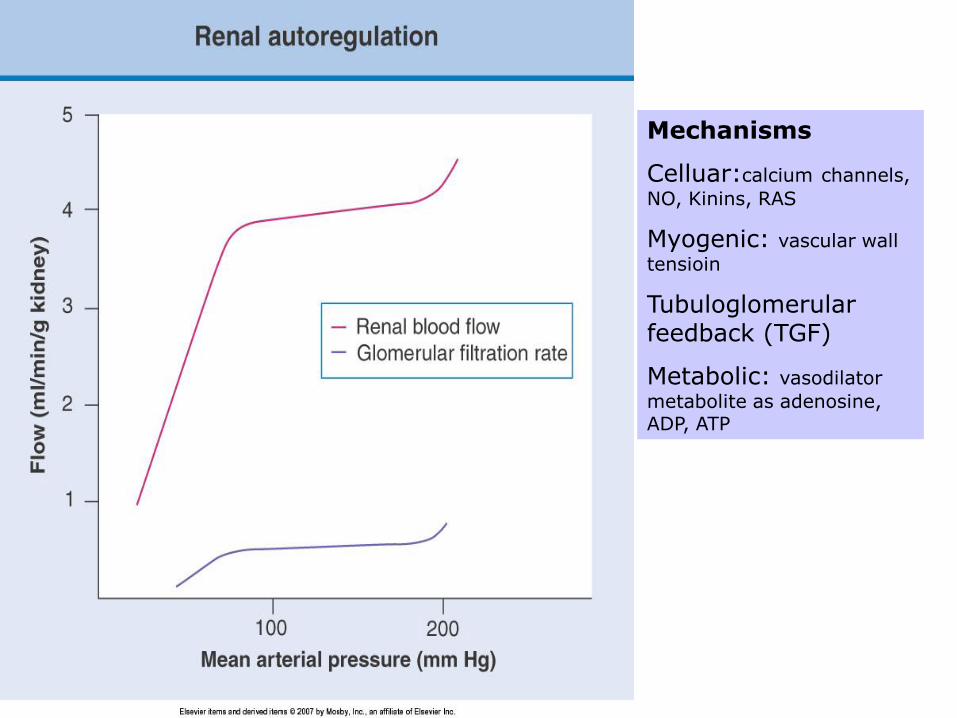
Mechanisms
Celluar:calcium channels,
NO, Kinins, RAS
Myogenic: vascular wall
tensioin
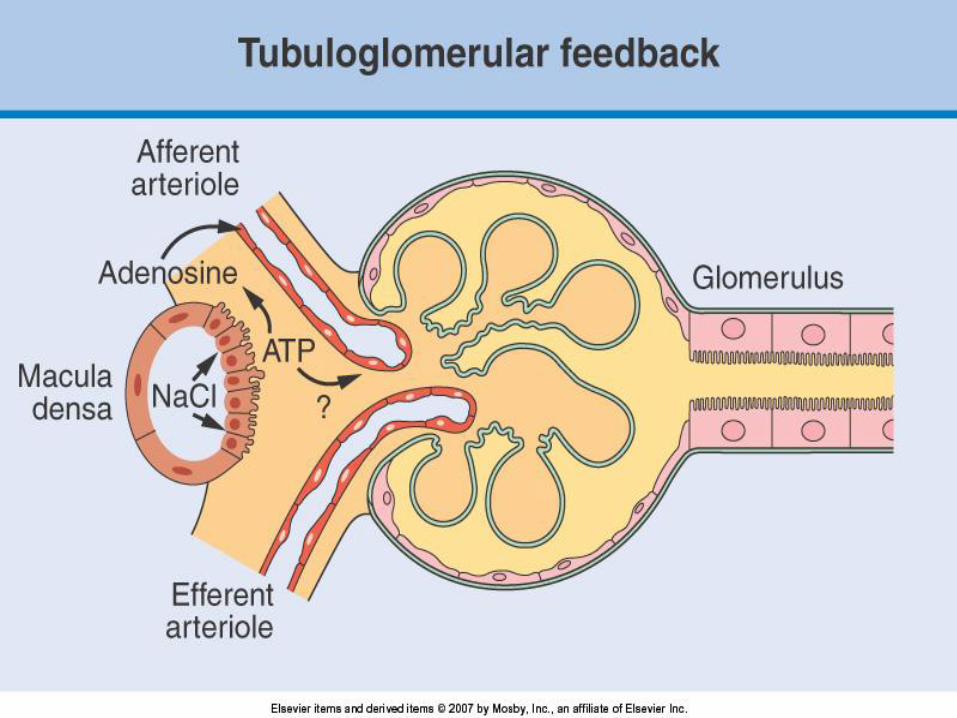
Tubuloglomerular feedback (TGF)
Metabolic: vasodilator
metabolite as adenosine, ADP, ATP
Adaptation to renal injury
Adaptation to renal injury ~ to nephron loss
Response to Reduction in Numbers of Functioning
Nephrons
Common Mechanisms of Progressive Renal
Disease
Adaptation Maladaptation
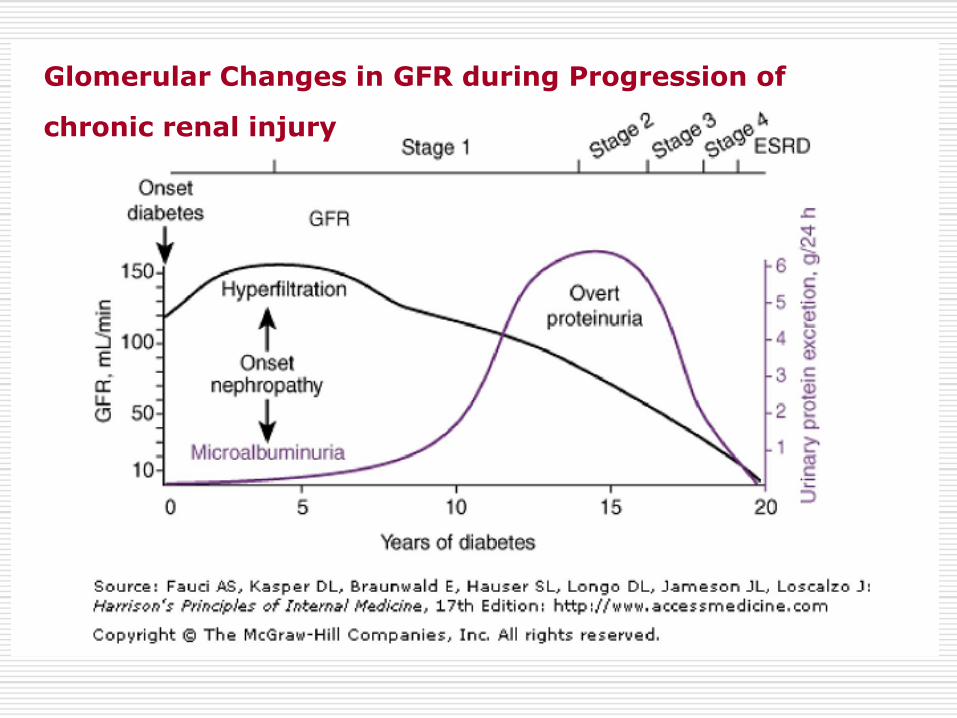
Glomerular Changes in GFR during Progression of
chronic renal injury
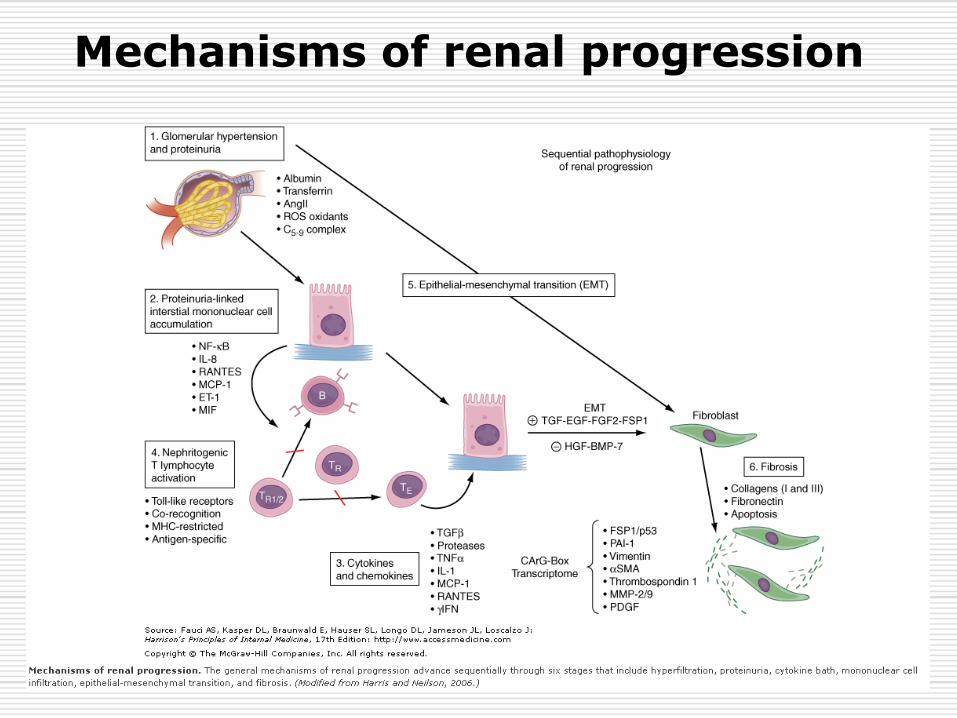
Mechanisms of renal progression
Adaptation to Nephron Loss
Structural and Functional Adaptation of the Kidney to
Nephron Loss
Alterations in Glomerular Physiology
Mediators of the Glomerular Hemodynamic Responses to Nephron Loss
Renal Hypertrophic Responses to Nephron Loss
Mechanisms of Renal Hypertrophy
Adaptation of Specific Tubule Functions in Response to
Nephron Loss
Adaptation in Proximal Tubule Solute Handling
Loop of Henle and Distal Nephron
Glomerulotubular Balance
Sodium Excretion and Extracellular Fluid Volume Regulation
Urinary Concentration and Dilution
Potassium Excretion
Acid-Base Regulation
Calcium and Phosphate
Structural and Functional Adaptation of the Kidney to Nephron Loss
Alterations in Glomerular Physiology
SNGFR (glomerular hyperfiltration glomerular hypertension)
Mediators of the Glomerular Hemodynamic Responses to
Nephron Loss
AII, aldosterone, natriuretic peptides (NP), endothelins (ET)
eicosanoids and bradykinin
Renal Hypertrophic Responses to Nephron Loss
Whole-Kidney Hypertrophic Responses/ Glomerular Enlargement
Cell size-increasing
Elasticity or growth of interstitial spaces
Mechanisms of Renal Hypertrophy
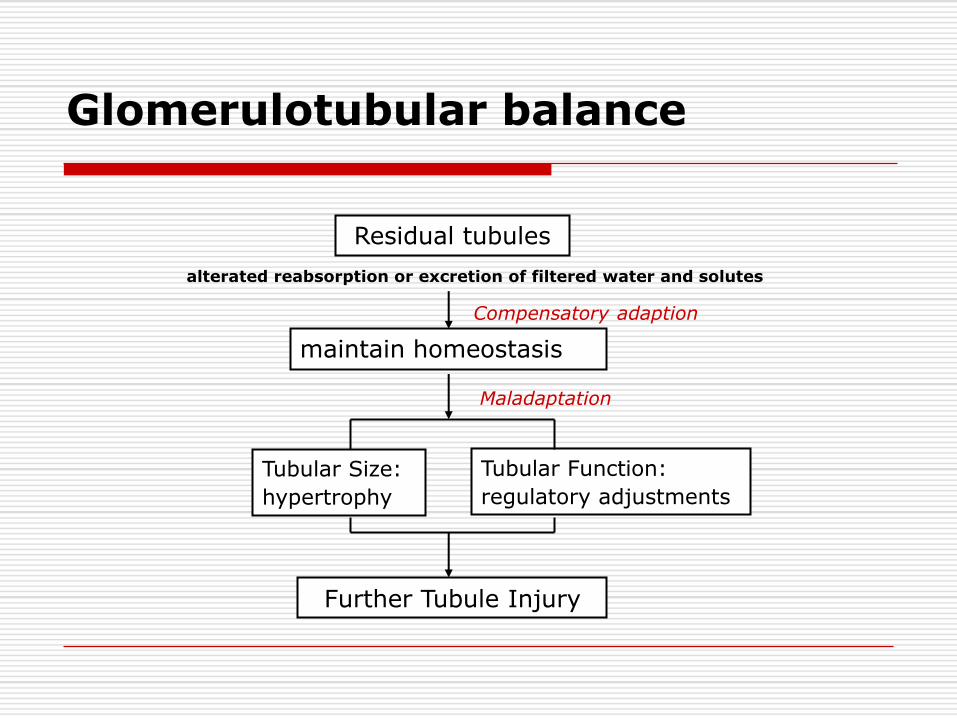
Glomerulotubular balance
alterated reabsorption or excretion of filtered water and solutes
maintain homeostasis
Compensatory adaption
Maladaptation
Tubular Size:
hypertrophy
Tubular Function:
regulatory adjustments
Further Tubule Injury
Residual tubules
Adaptation of Specific Tubule Functions in Response to Nephron Loss
Adaptation in Proximal Tubule Solute Handling
tubule size surface area transport activity
Loop of Henle and Distal Nephron
a major adaptive increase in active solute transport
Glomerulotubular Balance
Sodium Excretion and Extracellular Fluid Volume Regulation
Urinary Concentration and Dilution
Potassium Excretion
Acid-Base Regulation
Calcium and Phosphate

Response to Reduction in Numbers of Functioning Nephrons
Renal hypertrophy GFR
Loss of nephrons
persistent injury
>80% of renal mass-lose
Nephron: lose autoregulation
intraglomerular hypertension
Glomerulosclerosis
Tubular atroph and interstitial fibrosis
Compensatory adaption
Maladaptation
Proteinuria
tubuloglomerular feedback system
Nephron: lose autoregulation
progressive nephron destruction
vasoconstriction RAS
Long-Term Adverse Consequences of Adaptations to Nephron Loss
Hemodynamic Factors
Mechanisms of Hemodynamically Induced Injury
Non-hemodynamic Factors in the Development of Nephron Injury Following Extensive Renal Mass Ablation
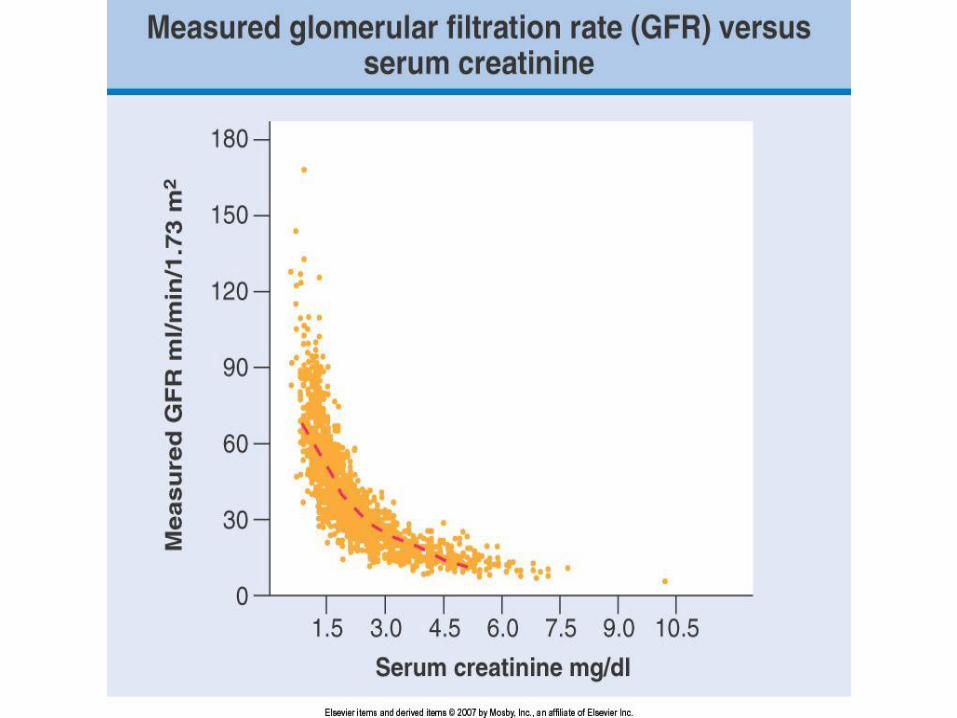
Diagnosis of kidney diseases
symptome
sign
Laboratory tests and imageology
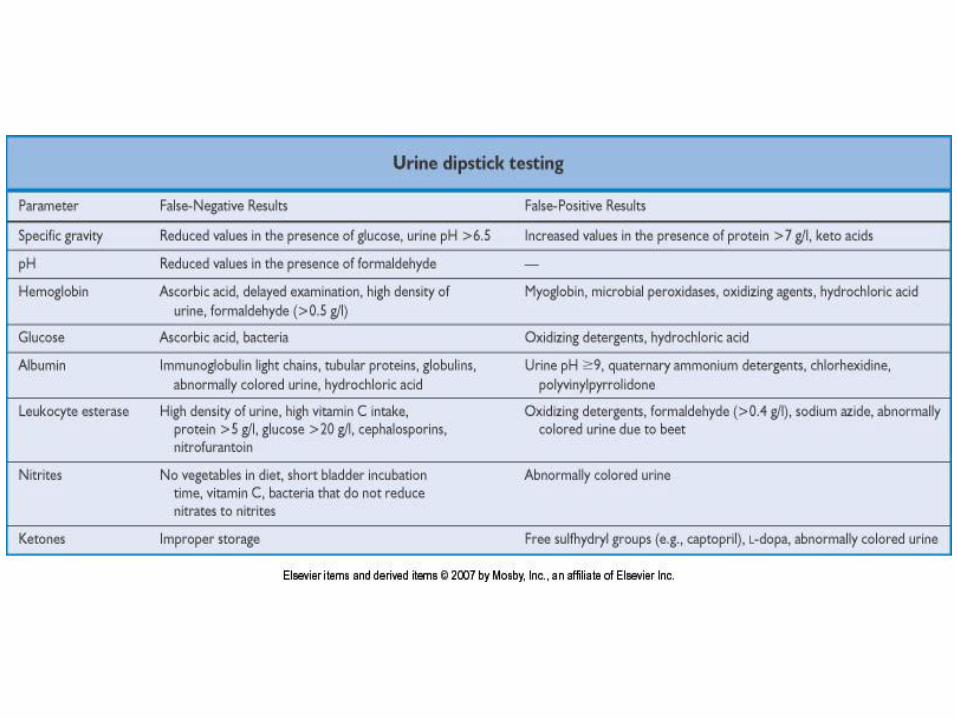
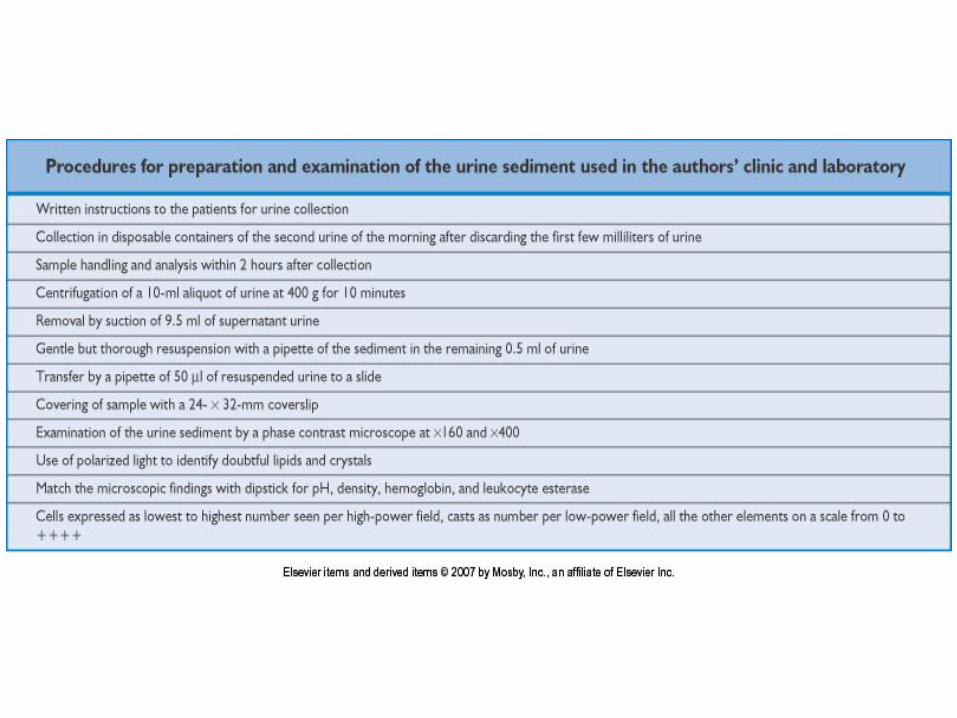
urinalysis
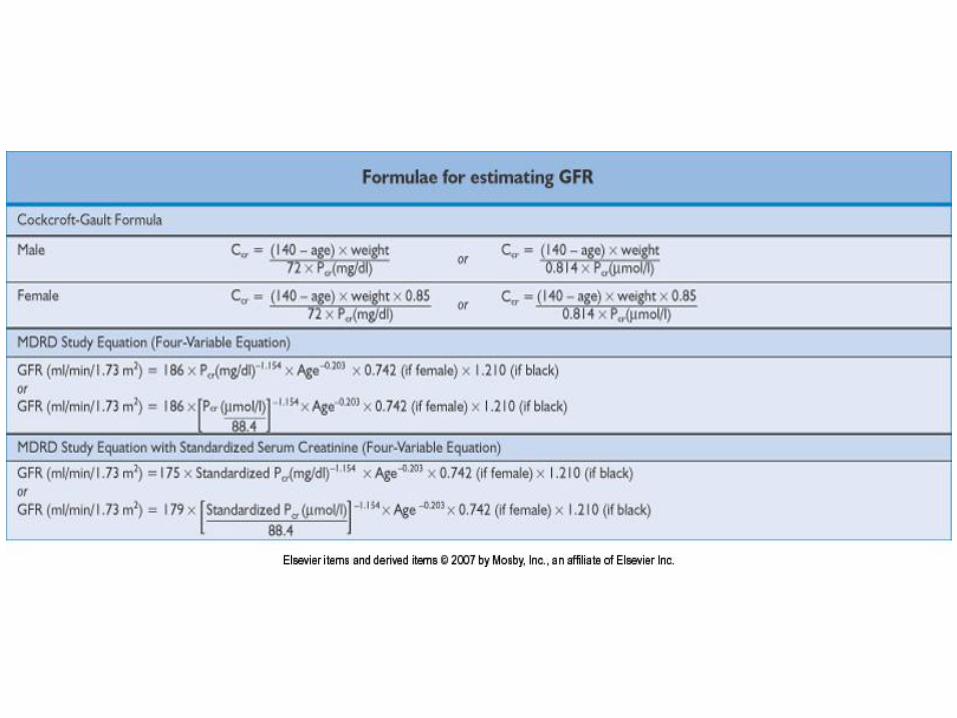
renal function
ultrasound
X-ray
Magnetic resonance imaging, MRI
Clinical manifestation
Proteinuria
Qualitation test: urine protein positive
Quantitation test: urine protein 150mg/d
Quantity of urine protein
Mild proteinuria < 1.5g/d
Moderate proteinuria 1.5-3.5g/d
Severe proteinuria > 3.5g/d or 50mg/kg/d
Fresh urine 10 ml
centrifugate 1500rmp5min
Microscopic hematuria
urine sediment RBC >3/HP
Macroscopic hematuria
pink or red > 1ml blood/1L urine
Hematuria
Hematuria
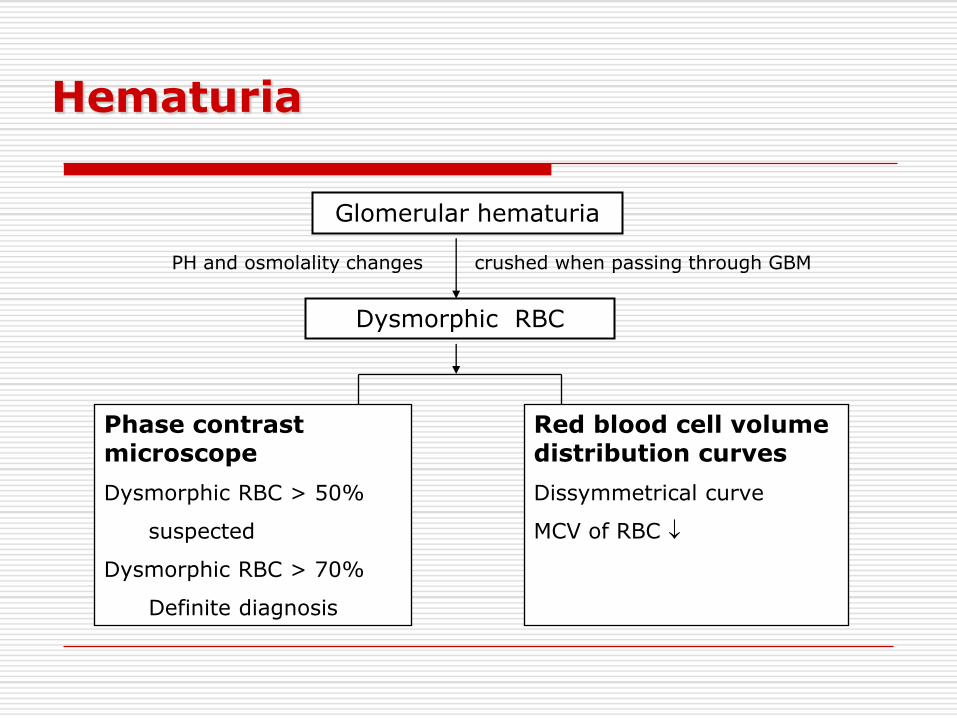
Glomerular hematuria
Dysmorphic RBC
PH and osmolality changes crushed when passing through GBM
Phase contrast microscope
Dysmorphic RBC > 50%
suspected
Dysmorphic RBC > 70%
Definite diagnosis
Red blood cell volume distribution curves
Dissymmetrical curve
MCV of RBC
Glomerulonephropathy
proteinuria as the chief complain, with or without
hematuria
Glomerulonephritis
hematuria as the chief complain, with or without
proteinuria
Clinical classificatioin
1. grave proteinuria Upr > 3.5g/d
2. hypoproteinemia Serum Alb < 30g/L
3. Severe edema
4. hyperlipemia
1+2 are necessary for diagnosis
Nephrotic syndrome
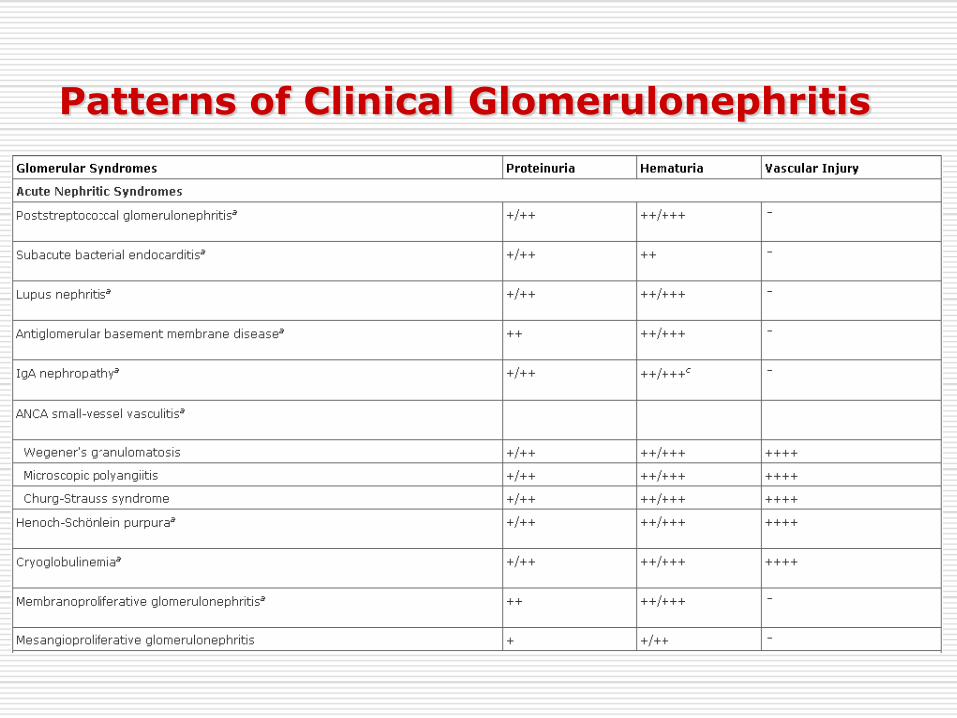
Patterns of Clinical Glomerulonephritis
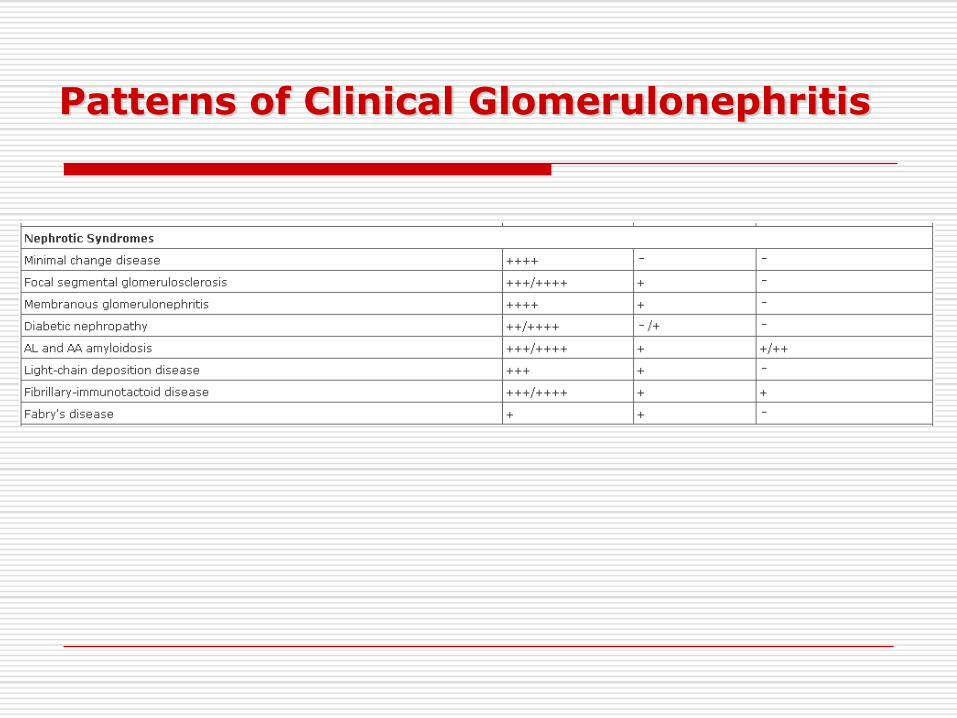
Patterns of Clinical Glomerulonephritis
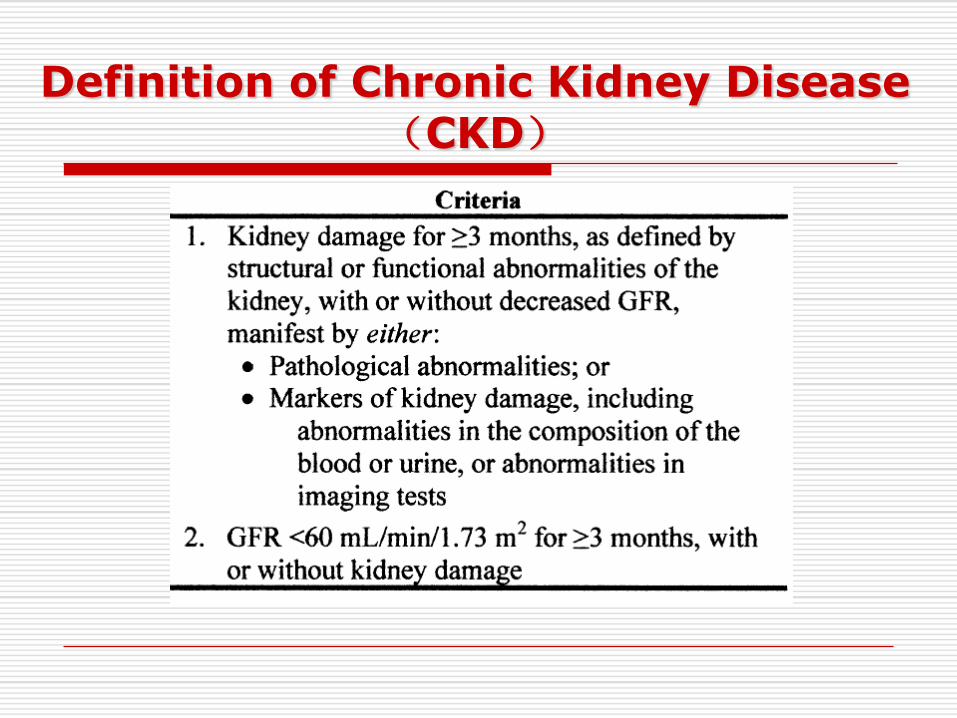
Definition of Chronic Kidney Disease (CKD)
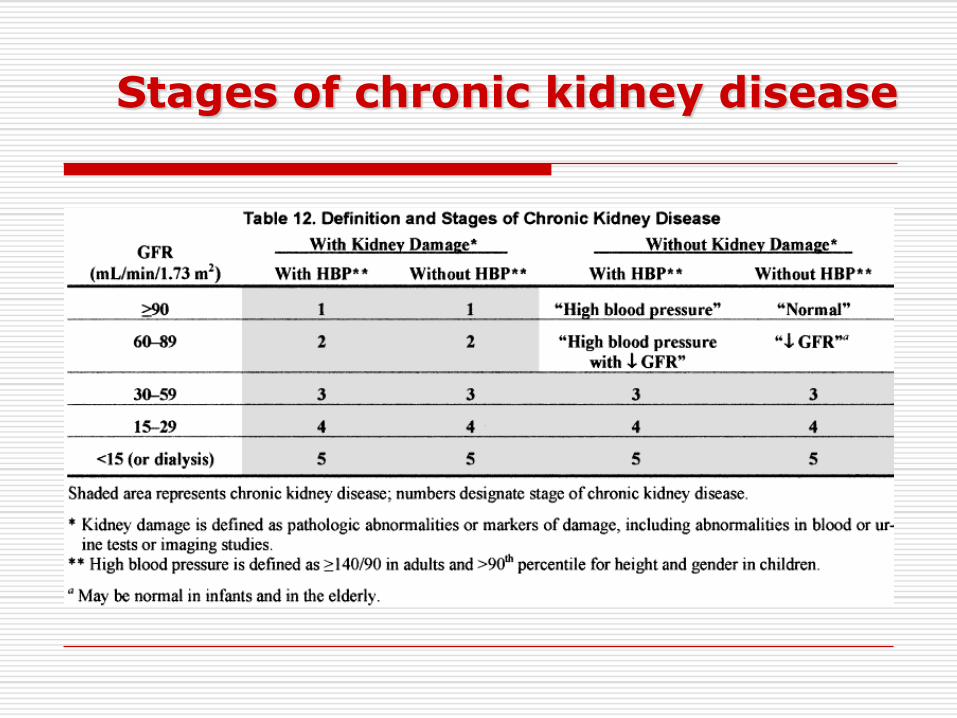
Stages of chronic kidney disease
0
500000
1000000
1500000
2000000
2500000
2010年 2030年
美国终末期肾衰患者的发病率
700,000
2,200,000
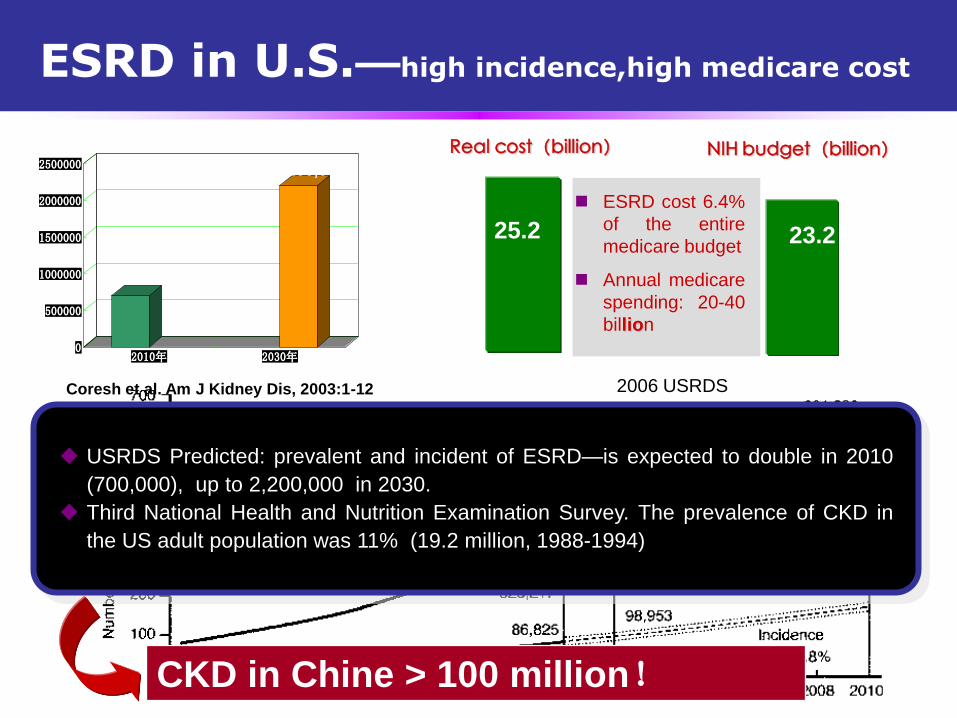
ESRD in U.S.—high incidence,high medicare cost
25.2 23.2
ESRD cost 6.4%
of the entire
medicare budget
Annual medicare
spending: 20-40
billion
Real cost(billion)
2006 USRDS
NIH budget(billion)
Coresh et al. Am J Kidney Dis, 2003:1-12
CKD in Chine > 100 million!
◆ USRDS Predicted: prevalent and incident of ESRD—is expected to double in 2010
(700,000), up to 2,200,000 in 2030.
◆ Third National Health and Nutrition Examination Survey. The prevalence of CKD in
the US adult population was 11% (19.2 million, 1988-1994)
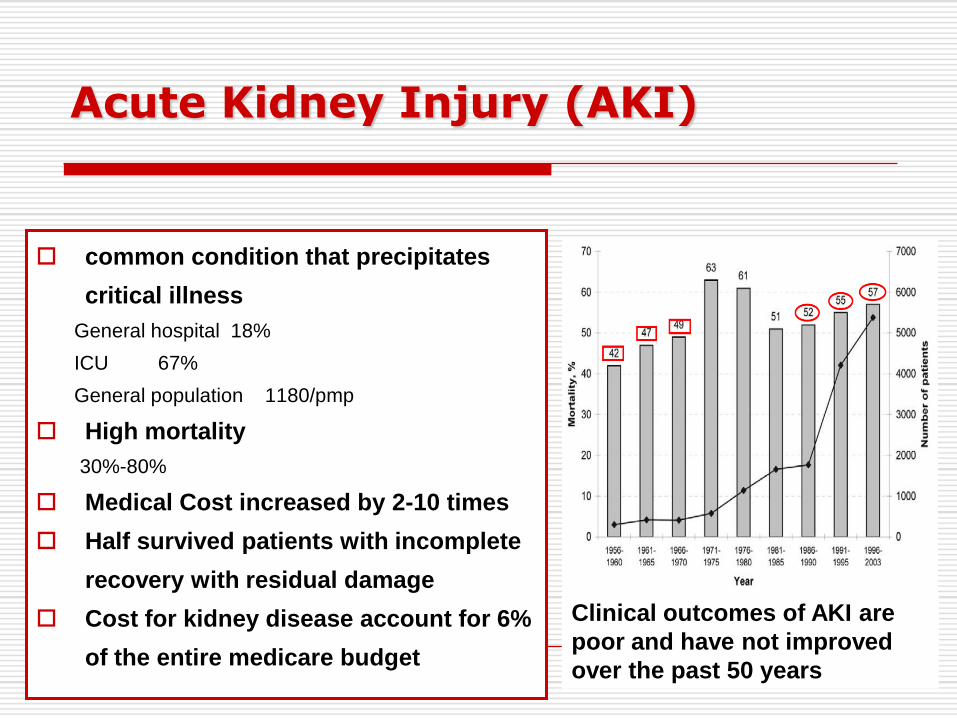
common condition that precipitates
critical illness
General hospital 18%
ICU 67%
General population 1180/pmp
High mortality
30%-80%
Medical Cost increased by 2-10 times
Half survived patients with incomplete
recovery with residual damage
Cost for kidney disease account for 6%
of the entire medicare budget
Acute Kidney Injury (AKI)
Clinical outcomes of AKI are
poor and have not improved
over the past 50 years
Prevention and Treatment of Kidney Disease
Disease-specific treatments
√Glomerulonephritis Immunosuppressive therapy
√Diabetic nephropathy Blood glucose control
√Hypertensive nephropathy anti-hypertension therapy
Non-specific treatments
√ Resting
√ Infection prevention
√ Diet
salt intake
low salt diet: sodium 2-3g/d,NaCl 5-6g/d
UNa or UCl 80-100mmol/d
Protein intake
low protein diet: protein 0.5-0.6g/kg/d
very low protein diet: protein 0.3-0.4g/kg/d
Prevention and Treatment of Kidney Disease
Non-specific treatments
√RAAS inhibitor
renin-angiotensin-aldosteron system
● Angiotensin II incrementally vasoconstricts the efferent
arteriole intraglmerlar hypertension
● RASi decrease intraglomerular capillary pressure decrease
proteinuria slow CKD progression
Prevention and Treatment of Kidney Disease
Non-specific treatments
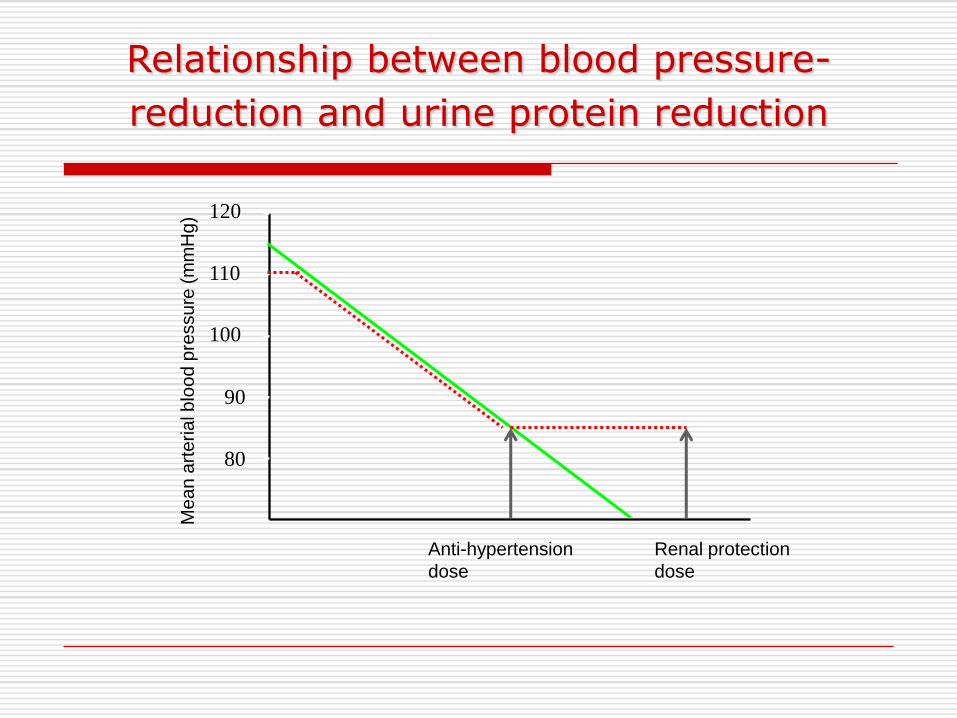
Anti-hypertension
dose
Renal protection
dose
Relationship between blood pressure-
reduction and urine protein reduction
Me
an
art
eria
l b
loo
d p
ressu
re (
mm
Hg
)
120
110
100
90
80
√Lipids control
● Renal mesangial cell and arterial smooth muscle cells share similar biologic
feathers
● Similar mechanism of glomerular sclerosis and artherosclerosis
√Correcting hyperuricemia
● 90% cases of hyperuricemia are secondary to kidney disease
● Hyperuricemia induce renal tubulointerstitial injury
√Avoiding renal toxic drugs
● aminoglycosieds, NSAIDs, renal toxic Chinese herb
Prevention and Treatment of Kidney Disease
Non-specific treatments
Key Points
Kidney functions
Adaptation to renal injury
Long-Term Adverse Consequences of
Adaptations to Nephron Loss
Taking home question
What is the Structural and Functional
Adaptation of the Kidney to Nephron Loss





![c. USA - fdjpkc.fudan.edu.cnfdjpkc.fudan.edu.cn/_upload/article/files/f5/3c/44... · A series of 10-amino-6,8,12,12a-tetrahydro-5H-thiazolo[4',5':4,5]pyrido[2,1-a] isoquinolines with](https://img.pdfslide.us/doc/110x75/6069a4d723417a32a2250d95/c-usa-a-series-of-10-amino-681212a-tetrahydro-5h-thiazolo4545pyrido21-a.jpg)