Embed Size (px)
Citation preview

General Internal Medicine Part II: Cancer Screening, Self-Care, and Doctoring
John D. Goodson, MD Massachusetts General Hospital
Harvard Medical School Boston
…and I have no disclosures

My Goals:
Review existing cancer screening recommendations and select controversies
• Colon cancer • Cervical cancer (HPV screening) • Breast cancer • Prostate cancer • Lung cancer
Consider how the disease prevention and health promotion agenda works in practice

The screening agenda First list: Hypertension Hypercholesterolemia Colon cancer Cervical cancer Breast cancer Prostate cancer Lung cancer Hep C Diabetes HIV STDs Skin cancer
Second list: Alcohol abuse Obesity Visual impairment Hearing impairment Balance Injury Opioids Hypothyroidism Osteoporosis Depression Abdominal Aortic Aneurism for men at risk

History of Screening
1900: Diabetes with urine sugar 1905: Syphilis 1917: US army for psychiatric disorders 1937: New York City cervical and breast cancer by PE 1960: Mammography 1963-1986: Health Insurance Plan of Greater NY RCT
of mammography Postgrad Med J 2004;80:493-469

Cancer screening: Key challenges
1. Tumor biology confounds screening recommendations
2. The value of screening has been actively questioned
3. Long term follow-up has only shown the promised benefits with colon CA
4. Should we pitch the screening agenda at all?

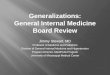
Tumor A
Tumor B
Tumor C
Tumor D
Metastatic spread
Regional spread Localized to organ
Microscopic Can
cer P
rogr
essi
on
Time
Screening intervals
Screening detection capability based on tumor biology and growth rates
A: Destined to become fatal B: Will become fatal C: Grows slowly but does not shorten life D: Remains undetectable

JAMA 2012;307:565-566 Ann Intern Med 2012;156:491-499
Screening doctrine challenged: 2012-2019
JAMA 2012 Ann Intern Med 2012

Benefits vs. burdens of cancer screening, US and Europe (2009 Meta-analysis)
Screened Years/Visits Cancers Deaths
Prevented
Breast CA (> 50 yrs) US 838 6/5866 18 Invasive 1 6 DCIS Europe 838 6/3352 15 Invasive 1 5 DCIS Prostate CA Europe 1410 9/2397 48 1
JAMA 2009;302:1685-1692

“..If we don’t continue to find and do research on cases of early breast cancer, we will never learn how to tell which cases have a good prognosis, and need less treatment, from cases with a bad prognosis, that need more treatment.”
Ann Intern Med 2013;158:60-61
The oncology community pushes back…

Colon cancer: The best case for screening
Stage 0 Stage II Stage IV 3-5 years
Surgical cure

Colorectal Cancer Recommendations (USPSTF, 2016): Screening at age 50 up to age 75, situational age 76-85, stop over 85. Recommendations (ACP): Screening at age 50, age 40 if high risk or 10 years younger than the age youngest relative diagnosed with colon CA. Stop age 75 if under 10 years of life expectancy American Cancer Society (2018): Start age 45

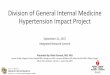
US Colonoscopy study, 2012: N = 2602, 1980-90, 23 yrs. follow up.
Study patients: Colonoscopy; Control: Expected incidence
Zauber AG et al. N Engl J Med 2012;366:687-696
53% reduction in mortality After TA
removal
US average
Col
on C
A m
orta
lity
No TAs
US pop

Standard colonography screening does not detect small polyps
Size of adenoma or CA
5mm 6mm 7mm 8mm 9mm 10mm Sensitivity of CT colonography 0.31 0.48 0.45 0.75 0.60 0.84
N Engl J Med 2008;359:2842-2943

What do you tell patients? Characteristics of colonic adenomas predict risk
(Polyp follow up trial, 15 935 patients, 1993-2013, 12.9 yrs. FU)
Colorectal cancer risk at 15 years, per 10 000 patient years
Risk Status: Advanced adenomas 20.0 (> 1.0 cm, high grade dysplasia, tubulovillous adenoma) Non-advanced adenoma 9.1* (< 1 cm.) No adenoma 8.9* * NS
JAMA 2018; 2021-31

5 year risk after a hyperplastic polyp is low (Indiana 2008, 1256/2436 patients rescreened at 5 yrs)
Advanced adenoma at Baseline 5 years*
Hyperplastic polyps 2% No polyps 1.1% *P=N.S.; No different risk of CA
JAMA 2008;359:1218-1224

US Multi-Society Task Force on Colorectal Cancer (2020)
JAMA Pre Pub online; November 2020
Baseline colonoscopy findings Surveillance interval No findings 10 yrs.
Hyperplasic polyps 10 yrs.
1-2 small (<10 mm) tubular adenomas 7-10 yrs.
3-4 small (<10 mm) tubular adenomas 3-5 yrs.
5-10 small (<10 mm) tubular adenomas 3 yrs.
Any adenoma >10 mm 3 yrs.
Sessile serrated >20mm or piecemeal resection 6 mos.

Screening thresholds over 75 years based on co-morbidities: Cost benefit analysis
(including complications) Years of age
76y 77y 78y 79y 80y 81y 82y 83y 84y 85y 86y None COL COL COL COL COL COL COL COL SIG SIG FIT
Mod COL COL COL COL COL SIG FIT FIT Severe COL COL SIG FIT FIT
Consider colonoscopy screening up to age 83 in those with no co-morbidities, any screening up through age 86
Ann Intern Med 2014;160: 750-759

Skill of colonoscopist may be related to mortality: Kaiser experience 1998-2010
0 10 20 30 40 50
Quintile 1
Quintile 2
Quintile 3
Quintile 4
Quintile 5
Percent reduction in cancer risk per year of follow-up based on adenoma detection
rates by quintile
Reduction in cancer risk per year of followup
NEJM 2014; 370:1298-1306
Over 40% lower CA mortality for colonoscopists with highest detection

A well done colonoscopy provides over 10 years of reassurance: Polish cohort
(Polish cohort, N = 165,887, 17.4 yrs. Follow-up. High quality* vs. low quality colonoscopy)
Ann Intern Med 2020: 173:81-91
Hazard ratios**: 0-5 yrs.=0.55 5.1-10 yrs.=0.54 10.1-17.4 yrs.=0.46 After 17.4 yrs. HR returned to baseline
*High quality = cecal intubation, “sufficient” prep, endoscopist with annual adenoma detection of > 20% **Observed vs. expected
0 5
10 15 20 25 30 35 40
0-5 years 5.1-10 years 10.1-17.4 years Low Quality High Quality
Col
on C
ance
r

Alternative strategies Flexible sig: Lower death rate from distal cancers Fecal occult blood: 9% lower death rate at 19.5 yrs. Fecal Immunochemical Testing (FIT), with and without
stool DNA (Immunochemical testing for blood with and without testing for DNA fragments): Widely variable performance (sensitivities 73-86%). Addition of DNA testing increases sensitivity up to 92% for CA or advanced neoplasms (Cologuard)

How good is the FIT? (UK cohort study. N = 5938, ages 60-72,
at “intermediate risk” = 3-4 small TAs or 1 TA > 10mm)
Sensitivity for Colon CA
Specificity for Colon CA
High heme threshold, harder to reach
Year 1 27.6% 94.1%
Years 1+2 62.5% 89.8% Years 1-3 77.3% 85.8%
Low heme threshold, easier to reach
Year 1 51.7% 86.2% Years 1+2 76.9% 77.6% Years 1-3 87.5% 70%
GUT 2019;68:1642-1652
72.4%of Colon CAs not detected at high threshold

Should the age of screening shift to 45 yrs.? The increase in colon cancer presenting under < 50
US National Cancer Data Base, 2015 vs. 2004 2004 2015
% of all colon CA presenting < 50 years of age
10.0% 12.2%* P < 0.001
Young adults presenting with Stage III/IV disease
40.0% 51.6%
*Increase primarily upper income non Hispanic males Cancer Online March 2019

The colon cancer inflection point at age 50 (Cross sectional cohort, 28% US population, 2000-2015 SEER registry)
JAMA Open Network 2020;3:e1920407
140% increase in situ 76% increase localized 30% increase regional 16% increase distant

Cervical cancer/HPV Screening Recommendations (USPSTF 2018): Age <21: No screening Age 21 (25)-30: PAP every 3 years Age 30-65: HPV +/- PAP every 5 years; PAP
every 3 years without HPV PAP testing not necessary after total abdominal hysterectomy
unrelated to cervical or vaginal cancer. PAP/HPV screening stops at 65 if no CIN* 2-3 for previous 20 yrs., neg PAPs or HPV for 10 yrs., most recent < 5 yrs. *Cervical intraepithelial neoplasia JAMA 2018;320:674-86

N Engl J Med 2013;369:2324-2331
The progression of HPV and the incidence of cervical cancer
HPV infection HSIL Cervical CA

Pap vs. HPV testing RCT, N =19 009, 224 Canadian practices, 4 yrs.
Number of new cases of premalignant findings per 1000 women after negative baseline testing
Premalignant findings at 4 year follow-up
Baseline negative
HPV
Baseline negative
PAP
Cases missed by PAP
Percentage cases
missed by PAP
Cervical intraepithelial neoplasia 3
1.4 5.4 4.03 75%
Cervical intraepithelial neoplasia 2
3.6 10 6.38 54%
JAMA 2018;320: 43-52

Breast cancer (without RFs) Recommendations (USPSTF, 2016): Biennial mammogram age 50-74 Biennial after age 40-49, “for women who place higher value on potential benefits...” Recommendation (ACS, 2015): Annual mammograms age 45-55 Biennial age 55 to age 75 with > 10 years life expectancy

Age, yrs 5 yr absolute breast cancer risk
Breast cancer incidence/100, 000
1-34 0.2 5.3 35-39 0.3 59.5 40-44 0.6 122.5 45-49 0.9 188.6 50-54 1.1 224.0 55-59 1.3 266.4 60-64 1.6 346.7 65-69 2.0 420.2 70-74 2.1 433.8 79-79 2.0 443.3 80-84 1.9 420.6 >85 2.5 354.4
Breast cancer 5 year absolute risk: The older the higher the risk!
JAMA 2015;314:1599-1614

More breast early breast CA found in the age of mammography
NEJM 2012;367:1998-2005
Early stage Late stage
% US Women with mammo
Breast CA incidence

The incidence of regional, late stage and distant disease has not changed
NEJM 2012;367:1998-2005
No change in incidence of late, regional or distant CA 1976 to 2008
Breast CA Per 100,000

Mammography associated with increased numbers of small and in-situ breast
tumors (1975-2010) Large breast cancers In situ breast cancers
NEJM 2016;375:1438-47

Benefits from screening mammograms are limited
Deaths prevented for 10,000 women over 10 years (100,000 mammograms)
Deaths prevented Mammograms per death prevented
39-49 years 2.9 34,482
50-59 years 7.7 12,977
60-69 years
21.3 4,694
70-74 years 12.5 8,000
Ann Intern Med 2016;164:244-55

Should you examine breasts? USPSTF neutral, ACS “qualified” No.
If not mammograms, then what?
“Potential harms of screening mammograms include overdiagnosis (i.e. finding a breast cancer that would not have clinically surfaced in the absence of screening) as well as the pain and anxiety associated with false-positive biopsies.” JAMA 2014; 311:1340
What does “clinically surfaced” mean if not by
Clinical Breast Exam (CBE)?

Interval breast Cancer: Manitoba cohort (N=69,025 women age 50-64 yrs. 7 yrs. follow-up)
Interval (between regular 2 yr. mammograms) breast cancers more likely to be ER/PR negative and higher grade. Mortality Hazard Ratio interval detected vs. mammogram detected cancer = 3.55
Stage Screening Interval I 63% 25% II 29% 45% III 6% 24% IV 1% 6%
JAMA Open Network 2020;3:e2018179
The value of the Clinical Breast Exam

Palpation techniques for CBE: Finger tips and hand relaxation
JAMA 2002;282:1276

Annual vs. Biennial Mammograms USPSTF 2016
Harms vs. benefits per 1000 women screened Ages 50-74 yrs
Annual Ages 50-74 yrs,
Biennial Fewer breast CA deaths 9 (5-10) 7 (4-9)
Life-years gained 145 (104-180) 122 (75-154)
False-positive 1798 (1706-2445) 953 (830-1325)
“Unnecessary” Biopsies 228 (219-317) 146 (121-205)
“Over-diagnosed” tumors 25 (12-68) 19 (11-34)
Ann Intern Med 2016;165:700-712

What do others say? Clinical exam Age Age to stop Interval
ACOG, 2017 Yes 40 offer 50 start
> 75 Annual or biennial
ACR, 2017 Neutral 40 None Annual ACS, 2015 No 45 > 10 yrs. life
expectancy
Annual 45-54 Biennial > 55
CTFPHC, 2018
No 50 Neutral 2-3 yrs.
NCCN, 2018 Yes 40 None Annual USPFTF, 2016 Neutral 40-49 consider
50 75 Biennial
WHO, 2016 Yes 50 75 Biennial Ann Intern Med 2019;170:547-560

Breast imaging reporting and data system assessment categories used
Category Assessment Likelihood ratio
for breast cancer diagnosis+
1 Negative 0.1 2 Benign finding 0.1 3 Probably benign finding; short-interval follow-up suggested 1.2 0 Need additional imaging evaluation 7.0 4 Suspicious abnormality – biopsy should be considered 125 5 Highly suggestive of malignancy 2200 +Likelihood ratios for risk of breast cancer diagnosis at first screening mammography

Screening at age 40 reduced breast cancer mortality
(UK RCT, invitation to mammogram, ages 39-41,1990-97, N = 160,921 22.8 year follow up (2020)
Lancet Oncol 2020;21:1165-72
25% reduction in breast cancer deaths for women invited to start screening ages 39-41 yrs. vs. screening at age 50 yrs. Benefit remained for 10 yrs.

Prostate Cancer Recommendations of USPSTF 2018: Age 55-69: Individualized. “Screening offers a small potential benefit…” Age > 70: No screening Recommendations of ACS 2016: Age > 50 or > 10 years life expectancy: Men should have “a chance to make an informed decision…” Age > 45 if first degree relative with prostate CA, African American

Rotterdam screening trial (2018) RCT: 1186 men, 1991-94, average age 64 yrs. PSA/DRE/TRUS screen
(4yr. Interval) vs. No screen 19 yr. follow-up. Baseline PSAs 1.2, 1.1)
52% reduction in prostate CA mortality among screened patients NNS = 67 to advert one prostate CA death
European Urol 2018; On line prepublication

16 year follow-up of the European RCT of prostate cancer screening (2-4 y) showed ongoing benefit
(2019: N = 182,160, age 55-69 at entry, 16 yrs. follow-up)
European Urology 2019;76:43-51
20% reduction of prostate Cancer mortality at 16 yrs. Number “invited” to prevent one cancer death fell: 1947 at 9 yrs., 742 at 13 yrs., 570 at 16 yrs. Number needed to diagnose at 13 yrs., = 18 (48 at 9 yrs.)

Prostate cancer screening reduced the incidence of metastatic disease vs. no change in breast metastatic disease
No change in metastatic breast cancer
Decline in metastatic prostate cancer
NEJM 2015; 373:1685-1687

RCT of prostate cancer treatment (2018)
NEJM 2018;379:2319-2329
RCT: 14 Scandinavian centers, men < 75 years, localized prostate CA. Prostatectomy vs. Watchful waiting; 29 yrs. FU
P Prostatectomy Watchful waiting 45 % reduction of
prostate cancer deaths NNT to prevent one prostate cancer death = 8.4 2.9 years of added life from radical prostatectomy
Mortality 19.6% vs. 31.3%

RCT of prostate cancer treatment
NEJM 2018;379:2319-2329
Radical Prostatectomy
Watchful Waiting
Death, % All 71.9 83.8 0.74 < 65 62.6 77.6 0.62 > 65 79.2 89.3 NS
RR
Death from prostate CA All 19.6 31.3 0.55 < 65 22.8 37.9 0.50 > 65 16.9 25.3 0.63
Distant metastasis All 26.6 43.3 0.54 < 65 30.8 49.4 0.49 > 65 23.2 37.7 0.59

What are the consequences of Prostate CA treatment?
USPSTF Meta-analysis N = 1,904,950 63 studies
JAMA 2018;319:1914-1931
Increased risk of urinary
incontinence
Increased risk of erectile
Dysfunction Prostatectomy 2.75 1.49
Radiation NS 1.31

Screening for Prostate Cancer… the debate continues
Swedish study of men 9 years after screening stopped showed a DECLINE in survival
Eur Uro 2013; 64: 703-9
Screening
No screening
Survival
When screening stopped, survival returned toward unscreened control level

What do other organizations recommend? Organization Recommendation Year
USPSTF Shared decision making, age 55-69 2018
Canadian Task Force Against 2014
American College of Preventive Medicine
Against 2016
AAFP Against 2012
American Urologic Association
Shared decision making, age 55–69 2015
ACP Shared decision-making, age 50–69 2015
National Comprehensive Cancer Network
Shared decision making, age 45–75 2016
NEJM 2017;376:1285-89

Multi-parametric MRI: A screening (UK N=576 “at risk” for prostate CA
mpMRI vs. TRUS guided bx. vs. template prostate mapping bx. 40% found to have Gleason > 7 CA)
Health Technol Assess 2018;10:1
Sensitivity Specificity Positive predictive power
Negative predictive power
TRUS Bx 48% 96% 90% 74%
mpMRI 93% 41% 51%
89%
17/158 with a negative mpMRI had a Gleason > 7 CA

Toronto UCSF Hopkins Goteborg ProtecT
Number 993 810 1298 474 545
Follow up, yrs.
6.4 5 5 8 10
Monitoring PSA Bx q 3-4
yrs.
PSA, US, Bx q 1-2
yrs.
PSA. DRE Bx q 1 yr.
PSA Bx q 2-3
yrs.
PSA
Threshold PSA double < 3 yrs.
Bx or “anxiety”
Bx Bx PSA > 50%
Definitive tx 27% 43% 36% 43% 53%
Mets 2.8% 0.12 % 0.4% 1.48% 6.06%
Prostate CA death
1.51% 0 0.15% 1.27% 1.47%
JAMA 2017; 317:2532-42
Enter “active surveillance:” Broadly defined

Active surveillance is more common in some states then others, 2010-2015
2010 2015
JAMA Open Network 2020;3:e2031349

What if the PSA is low? (PLCO* screening cohort, N=10,968, age 55-60, 13 yrs. follow-up)
PSA Any prostate CA in 13 yrs. Clinically significant prostate CA in 13 yrs. <0.49 0.8 (0.4-1.2) 0.4 (0-0.8) 0.50-0.99 3.2 (2.2-4.2) 1.5 (1.1-1.9) 1.00-1.99 11.2 (9.8-12.6) 5.4 (4.4-6.4) 2.00-2.99 24.0 (21.1-26.9) 10.6 (8.3-12.9) 3.00-3.99 36.9 (31.8-42.0) 15.3 (11.4-19.2) >4.00 53.7 (48.6-58.8) 29.5 (24.2-34.8)
*Prostate, lung, colorectal, ovarian
JAMA Open Network 2020;e1919284

USPSTF estimates 1000 men
offered PSA
screening over 10-15
years
240 with elevated
PSA
100 with CA
80 choose
treatment
1-2 deaths prevented 60 with side effects Ann Intern Med 2017;167:449-44

What are the long-term consequences of active monitoring vs. intervention? (UK RCT, N=1643, 50-69 yrs. localized CA, 6 yrs. follow-up:
Surgery vs. XRT vs. Active Monitoring) Outcome per 1000 patient yrs.
Active monitoring (AM)
Surgery Radiation Therapy
Treatment effect vs. AM
Death 1.5 0.9 0.7 No improvement Metastasis 6.3 2.4 3.0 Disease progression*
22.9 8.9 9.0 50% reduction
* Mets, androgen deprivation therapy, obstruction
55% of men in the Active Monitoring group received treatment NNT= to prevent 1 death = 178 for surgery and 137 for XRT NNT to prevent progression = 9 for surgery or XRT
Health Tech Ass 2020: 24. Online 8-2020

Prostate Cancer
Where do we stand? -Screening finds prostate cancer -Prostate cancer is multi-centric, sampling can be misleading -Low level prostate cancer (Gleason 6) is relatively indolent and can be watched with active surveillance -Emerging technologies are targeted toward non invasive staging (mpMRI) and better screening tools -Is it better to know and follow than not to know?

Lung cancer
Recommendation (USPSTF, 2015): Annual screening for lung cancer with low-dose computed tomography (LDCT)
-Ages 55 to 80 years who have a 30 pack-year smoking history -Currently smoke -Quit within the past 15 years.
Screening should be discontinued -Once a person has not smoked for 15 years -Develops a health problem that substantially limits life expectancy or the ability/willingness to have curative lung surgery.

Lung-RADS Classification Cancer present, % 1: No nodules, nodules with calcification 0.05
2: Nodules, solid or partially solid, < 6 mm 0.40
3: Nodules, solid, > 6 mm to <8 mm 1.70
4A: Nodule, solid > 8 mm to <15 mm 4.60
4B: Nodule, solid > 15 mm 23.50
ALL 0.80
Lung-RADS classification, National Lung Screening Trial
(N = 26,455, 3 year follow-up)
Ann Inter Med 2015;162:485-491

What are the outcomes from Lung CA screening at 10 years?
(Netherlands RCT, N=13,195 smokers, screening vs. no screening, 10 yrs. follow-up)
24% reduction in 10 yr. mortality Estimated 8.9% “over diagnosis”
N Engl J Med 2020;382:503-573

But…screening with annual low dose CT for High risk smokers leads to a “stage shift”
(Danish RCT, N = 4104, men and women, annual CTs for 5 years)
Thorax 2012;67: 296-301 0
10
20
30
40
50
60
70
Control Screening
Low stageHigh stageTotal

Follow-up of new low risk nodules (under 15 mm) and low density
(Netherlands cohort N = 1020 nodules)
1020 nodules
55 % resolve
52 % Not cancer
7 % Cancer
Thorax 2018;0:1-7

Do you take care of your self? How do you maintain poise in practice?

The world we share as physicians
We live with increasing levels of “complexity density.” Our roles as teachers (“doctors”), coaches, care managers, and decision makers demand continuous attention and balance. How do we put this all together?

Your knowledge forms the basis for trust What do patients expect of us?
• Confident • Empathetic • Humane • Personal • Forthright • Respectful • Thorough
Mayo Clin Proc 2006; 81:338-344

What can you do to build trust?
Practitioner skills to promote healing relationships: • Do the little things • Take time and listen • Be open • Find something to like, to love • Remove barriers • Let the patient explain • Share authority • Be committed and trustworthy
Ann Intern Med 2008;149:720-724

How good are you at self-care? Who is your doctor?

John Hopkins physician cohort: “Usual source of care” and likelihood of receiving prevention services, 1948-1997
Preventive No MD Has MD Adj. OR service, % (95% C.I.) FOB 36 68 0.26(0.18-0.38) Any colon screening 49 75 0.26(0.18-0.39) Mammogram 47 84 0.17(0.05-0.62) PSA 62 84 0.33(0.22-0.49) Influenza 59 78 0.48(0.30-0.58)

You have the right to protect the “sanctity” of your cognition
Nurses were interrupted for 53% of medications administered and interruptions had consequences
For each RN interruption: Procedural failures+ 12.1% higher Clinical errors++ 12.7%
+ Aseptic technique ++ Wrong dose

The crisis of colleague burnout
0
10
20
30
40
50
60
Primary care
Surg speciality
Med or Ped
specialty
2-10 yrs 11-20 yrs > 20 yrs
Percent burnout
Mayo Clin Proc 2013; 88:1358-1367
Early career MDs at the greatest risk

Our most enduring resource: The opportunity for a purposeful life
US Health and Retirement Study Cohort study: N = 6985. Born 1931-1941, follow-up 2019 (age range 68-78) 2006 interviews: Life purpose (7 items)
US Health and Retirement Study Cohort study: N = 6985. Born 1931-1941, follow-up 2019 (age range 68-78) 2006 interviews: Life purpose (7 items)
US Health and RUS Health and Retirement Study Cohort study: N = 6985. Born 1931-1941, follow-up 2019 (age range 68-78) 2006 interviews: Life purpose (7 items)

Lowest life purpose score had increased mortality X 2.43

Inventory of purposefulness
• Self-acceptance: Medicine as a lifelong choice • Environment mastery: Set limits • Positive relations: Socialization and collaboration • Purpose in life: Physicians as advocates and
agents for health • Personal Growth: Continuous learning • Autonomy: Medical decisions based on the
knowledge you own

Key Points
• Colon cancer screening is well supported. Colonoscopy is the best example. Know your colonoscopist.
• Breast and prostate cancer screening remain controversial. • Prostate MRIs are a breakthrough with caveats. • Lung cancer screening with CT is well supported. • Be sure not to neglect your own health promotion and
disease prevention.

Next steps
• Become a cancer screening advocate Colon cancer: Yes, 50-85, 40-49 if RFs Cervical cancer: Yes, 30-65. Breast cancer: Yes, 50-75, possibly 40-49 Prostate cancer: Consider 50-70 Lung cancer: Yes, 55-80, if over 30 PYs and current smoker or
stopped < 15yrs • Become a vaccination advocate • Become a healthy lifestyle advocate • Practice what you advocate

Thank you
Questions?