Embed Size (px)
Citation preview

Cardiac ToxicologyLalita A. Bharadwaj
C O N T E N T S1 Introduction2 Overview of the Heart2.1 Structure and Function of the Heart2.2 Blood Flow Through the Heart2.3 The Normal Heart Rate3 The Conduction System4 The Cardiac Action Potential5 Excitation–Contraction Coupling6 The Normal Electrocardiogram7 Cardiotoxic Chemicals8 Pharmaceutical Agents8.1 Chemotherapeutic Drugs8.2 Digitalis Glycosides8.3 Antiarrhythmic Drugs8.4 Tricyclic Antidepressants8.5 Antihistamines8.6 Aliphatic Alcohols8.7 Hydrocarbons8.8 Volatile Substance Abuse8.9 Metals9 Air Pollution
10 ConclusionsReferencesFurther Reading
1 INTRODUCTION
One of the most important organ systems required formaintaining homeostasis in the human body is the cardio-vascular system. The cardiovascular system is the trans-port system of the human body and its functions are todeliver oxygen, nutrients and other substances to cellsand to remove waste products of cellular metabolism.The cardiovascular system is composed of three basiccomponents: the heart, the blood vessels and the blood.The heart weighs less than one pound in an adult, isthe size of a fist, lies obliquely in the mediastinum andserves as a pump imparting pressure to blood, therebyestablishing a pressure gradient that is required for bloodto flow to the tissues of the human body. The bloodvessels serve as the passageways through which bloodis distributed from the heart to all parts of the body.Blood vessels also redirect blood back to the heart and
form a closed-circuit circulatory system. Finally, theblood, the third component of the cardiovascular system,serves as the transport medium within which nutrients,oxygen and waste products are dissolved or suspended.Numerous control mechanisms regulate and integrate thediverse functions and component parts of the cardiovas-cular system, so that blood is supplied to body areasaccording to tissue-specific needs. These essential controlmechanisms ensure a constant internal homeostatic envi-ronment that surrounds each body cell, regardless ofdiffering demands for nutrients or removal of waste prod-ucts. The normal functioning of the cardiovascular systemis essential for life. Toxicity to the component parts of thecardiovascular system can lead to devastating irreparabledamage to the normal functioning of all systems of thehuman body. Toxicity can also result in sudden death dueto cardiac arrest.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

2 General, Applied and Systems Toxicology
Diseases of the cardiovascular system are the maincause of death in the UK and Canada and accountfor approximately 200 000 and 75 000 deaths each year,respectively (British Heart Foundation, 2006; BritishHeart Foundation Promotion Research Group, 2005;Heart and Stroke Foundation of Canada, 2004). Diseasesof the cardiovascular system are associated with dysfunc-tion of the component parts of the cardiovascular system;namely the heart, the blood vessels of the heart and body,and the blood. Currently the main forms of cardiovasculardisease (CVD) are divided into coronary heart disease(CHD) and stroke. About half (48%) of all CVD deathsare associated with CHD and approximately one quarterwith stroke. CVD not only affects the elderly, but is alsothe third leading cause of premature death under the ageof 75. In 2006, CVD resulted in just over 53 000 prema-ture deaths in the UK alone (British Heart Foundation,2006).
Extensive clinical and statistical studies have identifiedseveral factors that increase the risk of CVD. The majorrisk factors contributing to the high prevalence rateof CVD in Canada and the UK are associated withbehavioural risk factors. Behavioural risk factors areconsidered factors in one’s personal life that can beeliminated or reduced through lifestyle or behaviouralchanges (World Health Organization, 2002; Sandersonet al., 2009). Some behavioural risk factors include:smoking, physical inactivity, high blood pressure,dyslipidaemias, obesity and diabetes. Although the riskof CVD is primarily associated with lifestyle factors,there are several factors that contribute to an increasedrisk of CVD that cannot be controlled. These includeage, gender, family history and ethnicity. More recentlythere has been a growing interest in the role of low-levelchronic exposure to environmental pollutants in thecause of CVD. Environmental factors are considered keydeterminants of CVD. Although lifestyle choices, suchas smoking, diet and exercise, are viewed as major envi-ronmental influences, the contribution of pollutants andenvironmental chemicals is less clear. There is a growingbody of research evidence that suggests that exposure topollutants and chemicals could elevate the risk of CVD(O’Toole et al., 2008). Epidemiological studies reportthat exposure to fine particles present in ambient air isassociated with an increase in cardiovascular mortalityand statistically significant relationships between particu-late air pollution and ischaemic heart disease, arrhythmiasand heart failure have been reported (Puett et al., 2008).
It has been known for decades that certain chemi-cals; both industrial and pharmaceutical, can specificallyaffect the cardiovascular system. Chemicals that target theheart are classed as cardiotoxins and will be specificallydiscussed in this chapter. Cardiotoxins exert their effectson the heart both directly and indirectly. The degreeof their effects on the heart is mainly associated withdosage and exposure period (Wu, 2008). Cardiotoxins can
induce functional or structural effects on the heart. Chem-icals can produce functional alterations in the heart byaffecting its normal physiological function. For example,cardiotoxic chemicals may alter the normal pumpingaction of the heart by inducing arrhythmias. Cardiotoxinscan selectively induce structural damage to the heart byaltering its cellular components. Cardiotoxins may affectthe architectural structure of the heart through direct alter-ations of the myocardial cells. Structural toxicants maydirectly affect the cardiomyocyte membrane integrity,ion transport and energy supply systems. In general,cardiotoxicity results as a secondary consequence ofpharmaceutical/industrial chemical overdoses. Functionalalterations in the heart can occur after a single expo-sure or they may last only during the exposure periodto the cardiotoxic compound. More permanent structuraland functional changes result as side effects, after admin-istration of an overdose or as a result of the initiation ofan inflammatory response following repeated long-termexposures.
A few well-known cardiotoxic agents are chemicallyclassed as plant- and animal-derived toxins, heavy metals,aliphatic alcohols and hydrocarbons, aldehydes, gases(CO), carcinogens and pharmaceutical agents utilized inthe treatment of cancer, high blood pressure (antihy-pertensive drugs), arrhythmias and depression (tricyclicantidepressants), and anaesthetics (such as bupivacaineand halogenated hydrocarbon anaesthetics). Environ-mental pollutants, including particulate matter, polyaro-matic hydrocarbons and metals are suspected to be asso-ciated with CVD; however, the contribution of environ-mental contaminant exposures to CVD is still incom-pletely understood.
In summary, cardiotoxins lead to the development ofheart muscle damage and eventually result in the lossof normal heart function. The heart becomes weakerand is not as efficient in pumping and therefore circu-lating blood; the main function of the heart. Cardiotoxinsaffect the normal function of the heart through anumber of indirect and direct mechanisms that result inbiochemical and electrophysiological alterations. Directtoxic effects include those where the cardiomyocyte isdirectly affected. These effects on the cardiomyocyteinclude alterations in the plasma membranes abilityfor ion transport, and the ability of the cardiomy-ocyte to generate force and energy. Generally, chem-icals influence the electrical and contractile propertiesof the heart. Chemicals may affect the heart throughtheir effects on heart rate (chronotropic), conductivity(dromotropic), excitability (bathmotropic) or contractility(ionotropic). Indirect damage can occur as a result ofthe cardiomyocytes’ sensitivity to hypoxia, and loss ofhomeostatic mechanisms of the body responsible foracid–base and electrolyte balance. In general, chem-icals can depress oxygen uptake and interfere withcardiac energy metabolism (carbon monoxide), inter-fere with normal calcium homeostasis and interfere
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 3
with cardiac contraction and impulse conduction (metals,β-adrenergic agents), induce direct damage, resulting inmyocardial necrosis (antihypertensives), produce cardiacarrhythmias (respiratory tract irritants) and interfere withnucleic acid synthesis (anticancer agents). The mecha-nisms of cardiotoxicity are complex and differ substan-tially amongst the classes of chemicals known to inducecardiotoxicity. In this chapter, several cardiotoxic chemi-cals will be overviewed, along with their mechanisms oftoxicity.
2 OVERVIEW OF THE HEART
2.1 Structure and Function of the Heart
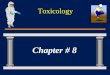
The heart is composed of three layers: the pericardium,the myocardium and the endocardium (Figure 1). Thepericardium is a double-walled membranous sac thatencloses the heart. It acts as a physical barrier, anchorsthe heart in the mediastinum and protects the heart frominfection and inflammation arising from the pleural cavityand lungs. The myocardium is composed of cardiacmuscle. Cardiomyocytes, the cells of the cardiac muscleare composed of long, narrow fibres that contain bundlesof longitudinally arranged myofibrils, a nucleus, super-abundance of mitochondria, sarcoplasmic reticulum (SR)and a plasma membrane or sarcolemma that enclosesthe cell. Cardiomyocytes, due to their unique featuresand arrangement in the myocardium, are able to transmitaction potentials quickly from cell to cell and main-tain high levels of energy synthesis to maintain bloodpressure and the regular pumping action of the heart;essential for the circulation of nutrients and gases tothe cells of the human body. There are two special-ized types of cardiac muscle cells. A majority of cardiaccells that make up the myocardium are contractile cells.These cells perform the mechanical work of impartingpressure to blood for circulation through the body. Thecardiac muscle is divided into two separate networks,one atrial and one ventricular. Within these networks,the cardiomyocytes are in close physical contact throughtransverse thickenings of the sarcolemma or interca-lated discs. These discs function to allow action poten-tials to pass from cell to cell very rapidly and effi-ciently, thus each network, atria and ventricles, contractas one functional unit. There is no direct physicalcontact between atrial and ventricular myocardium, thusa specialized conduction system is present to facili-tate and coordinate the electrical excitation from theatria to the ventricles to ensure synchronization betweenatrial and ventricular pumping, and a normal heartrate.
There are a small number of cardiac cells, auto-rhythmic cells, that do not contract, but are specializedfor initiating and conducting action potentials. These
3
2 1
Figure 1 Wall of the heart. This section of the heartshows the (1) pericardium, (2) the myocardium and (3)the endocardium. (Reproduced with permission from JohnRoss, 1999.)
cells are responsible for the excitation and contractionof the contractile cells of the myocardium. They arefound in specific locations in the myocardium callednodes. These include the sinoatrial node (SAN) andatrioventricular node (AVN), the AV bundle (bundle ofHis) and the Purkinje fibres. The third and final layer,the endocardium, is the internal lining of the myocardiumand is comprised of connective tissue. The endocardiumis continuous with the lining of the endothelium thatlines the blood vessels of the circulatory system ofthe body and thus creates a continuous closed-circuitsystem.
2.2 Blood Flow Through the Heart
The heart is the centre of the cardiovascular system.Generally, the cardiovascular system is divided into twoseparate vascular loops. These include the pulmonarycirculation, which carries blood between the heart and thelungs, and the systemic circulation, which carries bloodbetween the heart and organ systems.
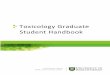
The heart is divided into right and left halves andis composed of four chambers; the right and left atria,and right and left ventricles (Figure 2). The atrialand ventricular chambers of the heart are separatedby electrically nonconductive fibrous tissue. Thesechambers are essential in facilitating the movement ofblood from the heart to the body. The right heart cham-bers pump deoxygenated blood through the pulmonary
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

4 General, Applied and Systems Toxicology
Superior vena cava(from upper body)
Right pulmonaryarteries (to right lung)
Left pulmonaryarteries (to left lung)
Pulmonaryartery
Aorta (to body)
Right pulmonaryveins (from right lung)
Left pulmonaryveins (from left lung)
Pulmonary valve
Direction of blood flow
Right ventricle
Left ventricle
Mitral valve
Left atrium
Septum
Right atrium
Tricuspid valveInferior vena cava(from lower body)
Aortic valve
Figure 2 Chambers of the heart. The heart has four chambers: the left atrium, the right atrium, the right ventricle andthe left ventricle. During diastole, blood flows into the atria, atrioventricular valves are pushed open and blood beginsto fill the ventricles. Atrial systole ejects blood remaining in the atria out into the ventricles. During ventricular systole,the ventricles contract, pushing blood out through semilunar valves into the pulmonary artery (right ventricle) and theaorta (left ventricle). (From http://www.nhlbi.nih.gov/ . . . /arr/arr howheartwork.html.) (Reproduced from U.S. Departmentof Health and Human Services.)
circulation and the left heart pumps blood through thesystemic circulation. The right heart generally consistsof structures located on the right side of the heart.These include the right atrium, AV valve (tricuspidvalve) and ventricle, the pulmonary semilunar valveand the pulmonary artery. The left heart consists of thepulmonary vein, left atrium, AV valve (mitral valve) andventricle, the semilunar aortic valve and the aorta.
The opening and closing of valves, controlled by theblood pressure changes in the heart chambers, and thecontraction and relaxation of the myocardium controlthe movement of blood through the heart. Duringrelaxation of the myocardium, or diastole, deoxygenatedblood continuously flows through the great venousvessels (inferior and superior vena cava) and thecoronary sinus to the right atrium, and oxygenated bloodflows from the pulmonary veins into the left atrium.During diastole, blood passively flows from the atriainto the ventricles through the opened AV valves, andventricular pressure rises above atrial pressure, resultingin the closure of the AV valves. During contraction of themyocardium, or systole, ventricular pressure rises abovearterial pressure, the semilunar valves open and blood isforced from the ventricles into their respective arteries.
2.3 The Normal Heart Rate
The continuous pumping (beating) action of the heartis a result of the rhythmic contraction (systole) and
relaxation (diastole) of the myocardium of the heart wall.In a normal adult the heart beats an average of about 70beats per minute. The continuous rhythmic beating of themyocardium is highly dependent upon the transmissionof electrical impulses or cardiac action potentials throughthe cardiac muscle. Heart rate can be altered by changesin autonomic nervous system activity. For example,increased parasympathetic activity can slow the heart ratebelow normal resting (bradycardia is defined as a restingheart rate below 60 beats per minute) and an increasedsympathetic activity will augment the heart rate abovenormal (tachycardia is defined as a heart rate of above180 beats per minute). Cardiac muscle is capable ofgenerating action potentials without nervous stimulationas a result of specialized cardiac muscle that is part of theheart’s specialized conduction system. A complete heart-beat, or cardiac cycle, consists of the contraction (systole)and relaxation (diastole) of both atria and ventricles.
3 THE CONDUCTION SYSTEM
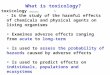
The conduction system is composed of specializedmuscle tissue that generates and distributes electricalimpulses that stimulate cardiac muscle to contract(Figure 3). These include the SAN, a small specializedregion in the right atrial wall located near the openingof the superior vena cava; the AVN, a small bundle ofspecialized cardiac muscle cells located at the base of
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 5
Rightatrium
Rightventricle
Leftventricle
Leftatrium
Sinusnode
Atrioventricularnode
His bundle
Rightbundlebranch
Leftbundlebranch
Electrical impulsespreads from sinusnode throughoutleft and right atria
Electrical impulsespreads from bundlebranches throughoutleft and rightventricles
Figure 3 Specialized cardiac muscle cells in the wall of the heart rapidly conduct an electrical impulse throughout themyocardium. Signals are initiated at the pacemaker (sinoatrial node; SAN) and spread to the rest of the atrial myocardiumand to the atrioventricular node. The AVN then initiates signals that are conducted throughout the ventricles by wayof the bundle of His and Purkinje fibres. (From http://www.bioen.utah.edu/faculty/sri/Lab8 humancardiovascular.htm.)(Reproduced with permission from Marquette Electronics, 2006.)
the right atrium just above the junction of the atria andventricles; the AV bundle (bundle of His), a tract ofspecialized cells that originates at the AVN and entersthe interventricular septum, where it divides to form theright and left bundle branches, and travels down theseptum to the tip of the ventricular chambers and backtowards the atria along the outer walls; the Purkinjefibres, small fibres that emerge from the bundle branchesand pass into the myocardium of the ventricles.
The sinoatrial node, also known as the pacemakersets the basic pace for the heart rate, generating about100–110 action potentials per minute. The average paceof an adult heart is approximately 72 beats per minute.The SAN is under vagal control at rest. Vagal tone bringsthe resting heart rate down to the normal rate of 60–72beats per minute. The SAN generates action potentialsfaster than other components of the conduction systemand therefore sets the beating rhythm of the heart. Oncethe SA node initiates an action potential, the impulsespreads quickly over both atria and causes them tocontract (P wave on an electrocardiogram (ECG)). Theaction potential originating in the SAN is transmittedfrom the atria to the ventricular myocardium throughfibres travelling to the AVN. The action potential is thentransmitted to the bundle of His, the left and right bundlebranches and finally to the Purkinje fibres of the heartwall to result in contraction of the ventricular muscle(QRS wave on an ECG).
Chemicals may disturb the conduction system of theheart and lead to alterations in heart rate, cardiac impulse
origin and conduction velocity. Arrhythmias (dysrhyth-mias) or deviations from ‘normal sinus rhythm’ maymanifest as a change in heart rate (tachycardia or brady-cardia), a disturbance in impulse formation or conduction(AV block) or as premature contractions arising fromareas within the heart and outside the normal conduc-tion sequence, as a result of augmented excitabilityand/or re-entry excitation. In summary, alterations in theconduction system can manifest as dysfunctions in heartrate (chronotropic) contractility (inotropy), conductivity(dromotropy) excitability/irritability (bathmotropy) andin the ability of the heart to relax (lusitropy).
4 THE CARDIAC ACTION POTENTIAL
Movement of ions into and out of the cell creates anelectrical difference across the cell membrane called themembrane potential. The resting membrane potential ofnon-nodal myocardial cells is between −80 and −90 mV.These include the atrial and ventricular myocytes, andthe Purkinje cells of the heart. The resting membranepotential of the SAN and AVN are between −50 and−60 mV and −60 and −70 mV respectively. Duringdepolarization, the inside of the cell becomes less nega-tively charged. The various phases of the cardiac actionpotential are related to changes in the permeability of thecell membrane to ions, primarily to sodium and potas-sium. Typically, normal myocardial cell depolarizationand repolarization occurs in four phases.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

6 General, Applied and Systems Toxicology
−100
−500 3
21
4 4
0
mV
+50
Ventricular myocyteaction potential
iNa
iCa(L)
iKto
iK iK
Figure 4 Ventricular action potential. Cardiac contrac-tile cells remain at a resting membrane potential of−90 mV until excited. The rising phase of the actionpotential is caused by fast sodium influx and thefalling phase by a fast potassium efflux. The plateauphase of the action potential results from a slowinflux of calcium coupled with a marked decrease inpotassium permeability. (Image obtained from Cardiovas-cular Physiology Concepts, Dr. Richard E Klabunde, PhDat http://www.cvphysiology.com/Arrhythmias/A004.htm.)(Reproduced with permission from Klabunde, 2008.)
Phase 4 of the non-nodal myocardial cells (Figure 4)represents the resting membrane potential of the cells.The resting membrane potential is maintained duringthis phase because of the movement of potassium ionsthrough potassium channels. In Phase 4, positive potas-sium (K+) ions are moving out of the cell, making themembrane potential more negative inside. At the sametime there is no movement of sodium (Na+) or calcium(Ca2+) into or out of the cell. This is primarily due tothe closure of fast sodium channels and (L-type) slowcalcium channels. When non-nodal myocardial cells arerapidly depolarized to their threshold voltage of about−70 mV, there is a rapid depolarization (Phase 0) thatis caused by an inwardly directed movement of Na+into the cell. This occurs through the opening of fastNa+-channels on the sarcolemma. At the same time,potassium channels close and movement of K+ out ofthe cell ceases. Therefore, the membrane potential movestowards a more positive value and away from its restingmembrane potential of −80 to −90 mV.
Phase 1 represents an initial repolarization that isof short duration and is caused by the outward move-ment of K+. This movement is primarily due to theopening of a unique K+ channel located in the myocar-dial membrane. At approximately the same time as K+is moving outward, and when the membrane potentialhas depolarized to approximately −40 mV, slow Ca2+channels open, calcium moves into the cells and Phase 2
−60
−30
4
0 3
4
0
mV
+30SA Node
Threshold
iK
iCa(L)
iCa(T)
if if
Figure 5 Nodal action potential. The membrane potentialof cardiac autorhythmic cells does not remain constantbetween action potentials. Following an action potential,the membrane slowly depolarizes to a threshold as aresult of inactivation of potassium channels, followed bythe opening of transient calcium channels. At the sametime, less potassium is leaving the cells and sodiumcontinues to leak into the cell, and the cell slowly depo-larizes to the threshold. Once the threshold is reached,longer-lasting L-type calcium channels open. There isa rapid influx of calcium, resulting in the initiation ofan action potential. The fall back to resting membranepotential results from rapid potassium efflux upon acti-vation of the potassium channels. (Figure obtained fromCardiovascular Physiology Concepts Richard E. Klabunde,PhD http://www.cvphysiology.com/Arrhythmias/A004.htm.)(Reproduced with permission from Klabunde, 2008.)
or the plateau of the action potential results. Repolariza-tion, or Phase 3, of the myocardial action potential occurswhen the movement of K+ out of the cell increases dueto complete opening of the K+ channels and closing ofthe Ca2+ channels.
In summary, the action potential in nonpacemakercells of the myocardium is primarily determined by thechanges in fast Na+, slow Ca2+ and K+ channels andthe movement of these ions across the sarcolemma.
Cells within the SAN and the AVN are characterizedas having no true resting potential and have the abilityto generate regular, spontaneous action potentials. Nodalaction potentials, unlike non-nodal myocardial cells, aredivided into three phases (Phases 4, 0 and 3) (Figure 5).Phase 4 of the action potential in these cells is consid-ered the phase of spontaneous depolarization (pacemakerpotential) or the period where an action potential is trig-gered once the membrane potential reaches a thresholdbetween −40 and −30 mV. Phase 4, starts when themembrane potential is about −60 mV. At this membranepotential, slow Na+ channels are open and there is aslow inward movement of Na+ into the cell. Addition-ally, during Phase 4 there is a slow decline in the outwardmovement of K+, as the K+ channels, responsible forPhase 3 or repolarization, continue to close. This fallin K+ conductance (gK+) also contributes to the ability
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 7
for spontaneous depolarization. The slow inward move-ment of Na+ causes the membrane potential to beginto spontaneously depolarize resulting in the initiationof Phase 4 of the pacemaker action potential. Phase0 is the depolarization phase of the action potential.The depolarizing current in these myocardial cells isprimarily a result of the movement of Ca2+ throughslow Ca2+ channels. The movement of Na+ through fastNa+ channels is responsible for the depolarization ofthe nonpacemaker myocytes of the heart. In fact, thereare no fast Na+ channels operating in nodal cells. Asa result these cells depolarize more slowly and pace-maker action potentials are sometimes referred to as‘slow-response’ action potentials. Phase 0, when depo-larization begins and the membrane potential reachesapproximately −50 mV, the transient or T-type Ca2+channels open and Ca2+ moves into the cells. The move-ment of Ca2+ into the cells results in movement of themembrane potential to a more positive value. As themembrane continues to depolarize and moves towardsa more positive, value, a second Ca2+ channel opens.Opening of this channel occurs around a membranepotential of −40 mV. These Ca2+ channels are called thelong-lasting or L-Type Ca2+ channels. The L-Type chan-nels open and result in the movement of more Ca2+ intothe cell until the action potential threshold is reached(usually between −40 and −30 mV). Thus, Phase 0 ordepolarization in nodal tissue is primarily caused by anincreased Ca2+ conductance (gCa2+) through the L-typeCa2+ channels that begin to open towards the end ofPhase 4. The movement of Ca2+ through the L-type Ca2+channels is not rapid, and thus the rate of depolariza-tion (slope of Phase 0) is much slower than that foundin other cardiac cells (e.g. the nonpacemaker cells, theatrial and ventricular myocytes, and the Purkinje cells).Phase 3, or repolarization, follows phase 0. The move-ment back towards the resting membrane potential inPhase 3 is a result of the movement of K+ ions outof the cell. Once the cell is completely repolarized at amembrane potential of about −60 mV, the cycle is spon-taneously repeated. Phase 3 or repolarization occurs asK+ channels open (increased conductance, gK+). Thisresults in an increasing outward-directed, hyperpolarizingK+ current. At the same time, the L-type Ca2+ channelsclose, gCa2+ decreases and the inward depolarizing Ca2+currents diminish, resulting in the re-establishment of theresting membrane potential.
The normal initiation and propagation of myocardialaction potentials is essential for the proper functioningof the heart. Alterations in ion movements, membranepotential or transmission of cardiac action potentialsthrough the heart muscle can lead to severe disturbancesin the normal cardiac rhythm and contractile ability ofthe heart. It is well characterized that some chemicalagents cause disturbances in the normal formation andconduction of cardiac action potentials by their alterationof normal ionic gradients and fluxes across the membrane
of cardiomyoctes. For example, some metals, such asbarium, affect the normal formation of cardiac actionpotentials. Barium, because of its charge (2+), can carrycurrents across the membrane in place of calcium ions,thus reducing the normal resting membrane potentialof the cell. When the resting membrane potential isreduced or modified to a more positive value, the cellsare more likely to have an increased automaticity. Dueto a reduction in resting membrane potential, the cell ismore readily excitable and will depolarize prior to itsnormal time course. This results in a premature impulseformation and contraction of myocardial cells, resultingin both alterations in normal heart rate (or arrhythmias)and contraction.
Antiarrhythmic drugs are known to alter the conductionof action potentials in non-nodal tissue of the heart.These drugs block the specific ion channels important inthe normal generation of action potentials in non-nodaltissue. Sodium-channel blockers, such as quinidine, caninactivate the fast sodium channels and reduce the rateof depolarization (decrease the slope of phase 0) ofnon-nodal tissue, thus reducing the propagation rate of theaction potential, and slowing conduction and ultimatelycontraction of the heart. Calcium-channel blockers, suchas verapamil and diltiazem, affect Phase 2 of the actionpotential. Verapamil blocks the slow inward calciumcurrent, an action that decreases the concentration ofintracellular calcium and thus contractile activity of theheart decreases. Potassium-channel blockers delay Phase3, or repolarization, by blocking the potassium channels.When the action potential of a cardiac cell fails to returnto the resting level along its normal timeframe, a secondaction potential may arise (early after depolarization).In this case, where repolarization is delayed, a seconddepolarization may occur prematurely, and this can leadto premature contractions of the heart and altered heartrhythms ultimately affecting the blood supply to thesystemic and pulmonary circulations, and oxygen to thebody tissues.
Chemicals may also alter impulse conduction in nodaltissue. Chemicals, such as cardiac glycosides, may delaythe propagation of electrical impulses in the conduc-tion tissue of the heart. For example, digitalis glyco-sides will increase the refractory period in the AVNand thus decrease impulse conduction in this section ofthe conduction system. If the effect is severe enough,conduction will be blocked at the AVN. Chemicalsmay also modify the sensitivity of the conductionsystem to endogenous agents. For example, halogenatedhydrocarbons, such as chloroform, have been shownto sensitize the heart to the effects of catecholaminesand sympathomimetic agents. Thus, in the case ofa previous exposure to halogenated hydrocarbons, thenormal catecholamine effects (increased heart rate, forceof contraction) are exaggerated at lower internal concen-trations. Additionally, as the catecholamine dosage isincreased, there is risk for the development of rhythm
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

8 General, Applied and Systems Toxicology
(tachycardia) and contraction (premature contractions)dysfunctions.
5 EXCITATION–CONTRACTIONCOUPLING
Excitation–contraction coupling (ECC) is the processwhereby a cardiac action potential triggers a myocyteto contract. When a myocyte is depolarized by anaction potential, calcium ions enter the cell, throughL-type calcium channels located on the sarcolemma,during Phase 2 of the action potential. Calcium trig-gers a subsequent release of stored calcium from theSR through calcium-release channels. The intracellularcalcium concentration is increased. Free intracellularcalcium binds to a protein, troponin-C (TN-C), which ispart of a regulatory complex attached to thin contractilefilaments (actin myofilaments). The binding of calcium toTN-C induces a conformational change in the regulatorycomplex and a site on actin is exposed and able to bindto the myosin head of the thick contractile filament. Thisbinding results in the hydrolysis of adenosine triphos-phate (ATP), which supplies energy for a conformationalchange to occur in the actin–myosin complex, resultingin cross-bridge cycling (actin and myosin filamentsslide past each) and contraction of the cardiomyocyte.Cross-bridge cycling occurs as long as the cytosoliccalcium remains elevated. At the end of Phase 2, calciumentry into the cell slows and calcium is sequestered bythe SR by an ATP-dependent calcium pump (sarcoen-doplasmic reticulum calcium-ATPase), thus lowering thecytosolic calcium concentration; actin-myosin interactionstops and the myocardial cell relaxes.
Contraction of the myocardium is highly dependenton the availability of ATP and calcium. Mecha-nisms that enhance the concentration of cytosoliccalcium increase the amount of ATP hydrolysedand the force generated by the actin and myosininteractions, as well as the velocity of shortening.Physiologically, cytosolic calcium concentrations areinfluenced primarily by β-adrenergic stimulation.β-adrenergic stimulation increases the force andshortening velocity of contraction (i.e. positive inotropy)and increases the rate of relaxation (i.e. positivelusitropy). Mechanisms that alter ATP availability willalso impact the normal contraction of the myocardialcell.
Chemical agents can alter the force of myocardialcontraction by affecting any of the steps involved inthe ECC process. Generally, agents that alter intracel-lular calcium levels interfere with the autonomic nervoussystem control of the heart, alter metabolic processesfor energy production/utilization, oxygen and nutrientdelivery and the process of ECC will impact the forceof myocardial contraction. Additionally, disturbances in
the integrity of the myocardial cell membrane, ion move-ments and membrane-bound enzyme activity will alterthe propagation and duration of the myocardial actionpotential and thus alter contractile strength. Alterationsin the normal function of myofilaments of the conductionsystem will also alter contraction, leading to alterationsin force and development.
6 THE NORMAL ELECTROCARDIOGRAM
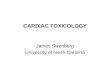
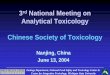
Electrical impulse transmission through the conductionsystem generates currents that can be detected on thesurface of the skin and recorded using an electrocardio-graph. The recording of the sum of all cardiac potentials(a full cardiac cycle) is called an electrocardiogram orECG (Figure 6). This type of recording is performed toevaluate symptoms of heart disease, to detect abnormali-ties in heart rate or conduction and to evaluate effective-ness and side effects of therapeutic agents. There are threevery distinct waves recorded during each cardiac cycle.The first is called the P wave and it represents atrial depo-larization. The atria contract a fraction of a second afterthe P wave begins. The second wave, called the QRSwave or complex represents the sum of all ventricularmuscle cell depolarization. This wave begins as a down-ward deflection, then continues as an upward triangularwave and finishes as a downward wave. The ventri-cles undergo contraction shortly after the QRS complexbegins. The third wave, the T wave indicates ventricularrepolarization.
There are several intervals and segments on the ECGand they provide information on the rate of conduction.The PR interval, measured from the beginning of the Pwave to the beginning of the QRS wave, is a measureof the conduction time from the beginning of atrialexcitation to the beginning of ventricular excitation orthe time necessary for impulses to be transmitted fromthe SA node through the atrium, AVN and His–Purkinjesystem. The PR interval normally ranges from 0.12to 0.2 seconds. The ST segment represents the timeduring which the ventricles are contracting and emptying.The QT interval lasts approximately 0.4 seconds andis sometimes referred to as the electrical systole of theventricles. The TP interval represents the time when theheart is in diastole and ventricular filling is taking place.
7 CARDIOTOXIC CHEMICALS
Chemicals known to induce cardiotoxicity can be classedchemically or by therapeutic usage. Aliphatic alcohols,aldehydes, glycols, halogenated alkanes, heavy metalsand biotoxins, as well as cardiovascular, central nervoussystem and chemotherapeutic agents have all been iden-tified as cardiotoxic chemicals. Cardiotoxicity is highly
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 9
QRScomplex
R
P
S
Q
TPR
segment
PR interval
(A) (B)
QT interval
STsegment
Sinoatrial(SA) node
Atrioventricular(AV) node
RA = Right atrium
RA
RV
LA
LV
LA = Left atriumRV = Right ventricle
LV = Left ventricle
Figure 6 A normal electrocardiogram of a single heartbeat illustrating the electrical changes that complement the cardiaccycle. Three waves accompany the cardiac cycle and these include the P-wave, a small upward deflection indicatingatrial depolarization, the QRS-wave, indicating ventricular depolarization or the spread of electrical impulses throughthe ventricles and the T-wave, indicating ventricular repolarization. (Reproduced with permission from EncyclopediaBritannica, 2008.)
dependent on dose, route magnitude, and frequency andduration of exposure. Cardiotoxicants can be placedinto the basic categories of pharmaceuticals, industrialchemicals and natural products. Pharmaceuticals withcardiotoxic action include antineoplastic, anaesthetics,psychotropics and antibiotics. In general, pharmaceuticalcardiotoxic effects are seen only when the dose exceedsthe therapeutic range.
Many pharmaceutical agents have been withdrawnfrom the market or severely restricted to specific indi-cations because of unexpected adverse events, includingfatalities. Cardiac abnormalities are one of the majorcauses of withdrawal of drugs or restriction in theirlabelling. Among these unintended effects, drug-inducedarrhythmogenic death is the most dramatic. In 2004,rofecoxib (Vioxx), a nonsteroidal anti-inflammatorydrug marketed by Merck & Co. to treat osteoarthritisand chronic pain was withdrawn due to concerns aboutincreased risk of heart attack and stroke associated withlong-term high-dosage use. The mechanism proposedto be associated with rofecoxib cardiotoxicity wasthe suppression of prostacyclin, a vasodilator andanticlotting agent.
Cisapride (Propulsid), a gastrointestinal pharmaceu-tical used to treat nocturnal heartburn as well as a varietyof other gastrointestinal disorders was withdrawn in 2000,due to its association with acquired long QT syndromeand ventricular arrhythmias. The cardiotoxic effects weresuspected to be due to blockade of one or more typesof K+ channel currents in the human heart, resulting
in dysrhythmias and cardiac arrest. Commonly knownpharmaceutical agents that alter heart function will bediscussed in the following section.
8 PHARMACEUTICAL AGENTS
8.1 Chemotherapeutic Drugs
Chemotherapeutic drugs are used in the treatment ofmalignant tumours. They include anthracyclines such asdoxorubicin and daunorubicin and alkylating agents. Theanthracycline class is the best known of the chemothera-peutic agents that cause cardiotoxicity. Alkylating agentssuch as cyclophosphamide, ifosfamide, cisplatin, carmus-tine, busulfan, chlormethine and mitomycin have alsobeen associated with cardiotoxicity.
Anthracycline antibiotics such as doxorubicin (i.e.adriamycin) and daunorubicin are some of the mosteffective chemotherapeutic agents used in the treat-ment of cancer and have been used for over 30 years.These drugs are used effectively in the treatment ofleukaemias, lymphomas and adenocardinomas. However,the utility of these pharmaceuticals is limited by cumu-lative, dose-related, progressive myocardial damage thateventually leads to congestive heart failure (CHF) (Shanet al., 1996). The incidence of anthracycline-inducedheart failure represents approximately 1% of patients with
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

10 General, Applied and Systems Toxicology
advanced heart failure due to ventricular systolic dysfunc-tion (Praga et al., 1979). A number of risk factors maypredispose a person to cardiotoxicty under chemotherapy.These are cumulative dose (anthracyclines, mitomycin);total dose administered during a day or a courseof treatment (cyclophosphamide, ifosfamide); rate ofadministration (anthracyclines, fluorouracil); schedule ofadministration (anthracyclines) and other factors, suchas age, gender and history of pre-existing cardiovas-cular disorders (Von Hoff et al., 1979). Anthracyclinesare well-known cardiotoxins and are known to inducearrhythmias, left ventricular failure and cardiomyopathyfollowing long-term usage (Lenaz and Page, 1976).
Anthracycline-induced cardiotoxicity has been clas-sified into three distinct types. First, acute or suba-cute injury can occur immediately after treatment. Thisrare form of cardiotoxicity may cause transient arrhyth-mias, a pericardial/myocardial inflammatory syndrome oracute failure of the left ventricle. Second, anthracyclinescan induce chronic cardiotoxicity resulting in cardiomy-opathy (Ferrans, 1978; Von Hoff et al., 1977; Bristowet al., 1978a; Friedman et al., 1978; Haq et al., 1985).This is a more common form of damage and is consid-ered the most important. Chronic anthracycline-inducedcardiomyopathy characteristically presents within oneyear of treatment. In a series of more than 3900 patientstreated with anthracycline, Von Hoff et al. (1977) notedthat CHF secondary to anthracycline-induced chroniccardiomyopathy occurred 0–231 days after the comple-tion of anthracycline therapy. Finally, late-onset anthra-cycline cardiotoxicity may manifest years to decadesafter anthracycline treatment and is increasingly beingrecognized, causing late-onset ventricular dysfunctionand arrhythmias (Schwartz et al., 1987).
Acute and subacute cardiac toxicity, which occurimmediately after a single dose of an anthracycline ora course of anthracycline therapy, are uncommon undercurrent treatment protocols. However, several distinct,early cardiotoxic effects of anthracyclines have beendescribed. First, electrophysiologic abnormalities mayresult in nonspecific ST and T-wave changes, decreasedQRS voltage and prolongation of the QT interval. Sinustachycardia is the most common rhythm disturbance,but arrhythmias, including ventricular, supraventricularand junctional tachycardias, AV and bundle-branch blockhave been reported (Steinberg et al., 1987; Lenaz andPage, 1976; Ferrans, 1978; Von Hoff et al., 1977; Bristowet al., 1978a).
The incidence of CHF secondary to doxorubicin(anthracycline)-induced cardiomyopathy depends on thecumulative dose of the drug. At total doses of less than400 mg m−2 body surface area, the incidence of CHFis approximately 0.14%; and this incidence increases to7% at doses of 550 mg m−2 body surface area and to18% at doses of 700 mg m−2 body surface area (VonHoff et al., 1979). The rapid increase in clinical toxi-city observed at doses greater than 550 mg m−2 body
surface area has made a 550 mg dose the empiric limitingdose for doxorubicin-induced cardiotoxicity (Von Hoffet al., 1979; Praga et al., 1979). Doses in excess of1000 mg m−2 body surface area can be well tolerated bysome patients (Henderson et al., 1989; Bristow et al.,1978a), however appreciable decreases in left ventric-ular ejection fraction have been documented at doses aslow as 300 mg m−2 body surface area (Bristow et al.,1978a; Cortes et al., 1975). Histopathologic changescharacteristic of doxorubicin-induced cardiotoxicity havebeen observed at doses as low as 183 mg m−2 bodysurface area, which is one third less than the conven-tional limiting dose. In general, a substantial propor-tion of patients will experience anthracycline-inducedcardiac damage while receiving standard treatment regi-mens, whereas others can tolerate cumulative doses twiceas large as the conventional limiting dose (Friedmanet al., 1978). Age remains a significant risk factor toanthracycline cardiotoxicity, with patients older than 65years having triple the risk of doxorubicin-related CHFcompared with younger patients at the same cumulativedose (Von Hoff et al., 1979).
It is hypothesized that the toxicity of anthracyclinesis associated with oxidative stress, loss of mitochondrialintegrity, disrupted calcium homeostasis and altered geneexpression leading to apoptosis (Doroshow, 1983; 1991;Dorowshow et al., 1980; Ito et al., 1990; Rajagopalanet al., 1988). Anthracycline-induced cardiac injury hasbeen based upon studies in animals and cell cultures.Although anthracycline-induced injury appears to bemultifactorial, a common denominator among most ofthe proposed mechanisms is cellular damage mediated byreactive oxygen species. However, it is not clear why thismechanism would be preferential to inducing cardiotoxiceffects.
Anthracyclines have been shown to induce membranedamage via lipid peroxidation in all tissues, includingthe heart (Doroshow, 1983). The formation of ROSis induced by the quinone moiety of anthracyclines;however, oxidative stress is also known to occur viainduction of nitric oxide synthase, leading to nitric oxideand peroxynitrite formation. This latter mechanism ofoxidative stress has been linked to nitration and inactiva-tion of key enzymes in the heart that include myofibrillarcreatine kinase, which is a critical energetic controller ofcardiomyocyte contractility. Myofibrillar creatine kinasehas been demonstrated to be a particularly sensitivetarget of peroxynitrite-induced nitration and inactiva-tion. Anthracyclines are also known to cause impairmentof membrane binding, assembly and enzymatic activityof mitochondrial creatine kinase, although the conse-quences of this impairment are not clear (Olson et al.,1974; Kusuoka et al., 1991; Holmberg and Williams,1990).
In the heart, like other tissue, anthracyclinesintercalate into nucleic acids, causing suppression of
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 11
DNA, RNA and protein synthesis. Some transcrip-tional regulatory proteins that appear important forregulation of cardiac-specific genes appear particularlysusceptible to anthracyclines. Myocyte cell death byboth apoptosis and necrosis has also been implicated inanthracycline-induced cardiotoxicity. It is proposed thata net loss of cells’ apoptotic and necrotic mechanismscontributes to its cardiotoxicity and heart failure.Recently in vivo studies have demonstrated that anthra-cyclines have a selective inhibition of cardiac musclegene expression for actin, troponin, myosin light-chain2 and the M isoform of creatine kinase in vivo. Othersuspected theories for anthracycline-induced myocardialdamage include free-radical-mediated myocardialinjury (Doroshow, 1983; Rajagopalan et al., 1988),myocyte damage from calcium overload (Holmberg andWilliams, 1990), disturbances in myocardial adrenergicfunction (Wakasugi et al., 1992), release of vasoactiveamines (Bristow et al., 1983) and cellular toxicityfrom metabolites of anthracycline therapeutics, such asdoxorubicin.
Anthracyclines also induce changes in adrenergic func-tion and impart abnormalities in Ca2+ handling, both ofwhich are critical components in the regulation of cardiacfunction. Down-regulation of myocardial β-adrenergicreceptors, resulting in adrenergic dysfunction, has alsobeen demonstrated in anthracycline-induced ventriculardysfunction (Tong et al., 1991; Robison and Giri, 1986;Fujita et al., 1991). However, the extent to which each ofthese mechanisms contributes to the dose-dependent heartfailure in anthracycline-treated patients remains some-what controversial.
It has also been hypothesized that proinflammatorycytokines may be directly relevant to anthracycline-induced cardiac injury. Recent reports have indicatedthat circulating proinflammatory cytokines may be linkedto anthracycline-induced ventricular dysfunction andcardiomyopathy (Ehrke et al., 1986). Doxorubicin hasbeen shown to induce the release of tumour necrosisfactor from macrophages and of interleukin-2 from mono-cytes (Shi et al., 1993).
In summary, the cause of anthracycline-inducedcardiotoxicity is multifactorial; however, a large bodyof evidence points to two major mechanisms: calciumoverload and free-radical-mediated myocyte damage.Increased oxygen-radical activity generated through thesemiquinone moiety of the doxorubicin molecule cancause lipid peroxidation and cell injury. Additionally,anthracycline-induced intracellular calcium overloadmay also lead to myocyte death. Doxorubicin has beenshown to activate the calcium-release channel acrossthe SR and causes calcium influx into the myocyte.Free-radical-induced cell-membrane damage has beendemonstrated with calcium influx, suggesting that thesetwo cellular mechanisms of anthracycline-inducedcardiotoxic may be linked.
8.2 Digitalis Glycosides
Cardiac glycosides have been used for centuries astherapeutic agents for the treatment of heart diseasesand are one of the most commonly described cardiacdrugs. Cardiac glycosides, known as a class of digitalis,are widely used in the pharmaceutical treatment of CHFand atrial tachyarrhythmias (The Digitalis InvestigationGroup, 1997). Digitalis derivatives are found in severalplants, including oleander, foxglove and lily of the valley.Digoxin and other cardiac glycosides exert their effectson myocardial contractility through their effects on ionhomeostasis.
In patients with heart failure, cardiac glycosides exerta positive inotropic effect by indirectly increasing intra-cellular calcium levels through inhibiting the plasmamembrane Na+-K+ ATPase. This inhibition results inan increase in intracellular sodium, which in turninhibits Na+/Ca2+ exchange and ultimately leads toan increase in calcium levels and a positive inotropiceffect. The therapeutic index of digitalis is narrow andthus patients are susceptible to arrhythmias in caseswhere the therapeutic window is compromised. Althoughdigoxin-induced arrhythmias are a common clinical issuein patients being treated for heart disease, the underlyingcellular mechanisms of these arrhythmias are yet to beelucidated.
There are several theories that have been proposedregarding the arrhythmic effects of digoxin. The toxicarrhythmogenic effects of cardiac glycosides are said tobe due to a combination of direct and indirect effectson the myocardium (Kemmerer, 2008). It is proposedthat digoxin induces arrhythmias by causing oscilla-tory fluctuations in cardiac resting membrane poten-tial. It is proposed that digoxin increases the rate andamount of Ca2+-induced calcium release from the cardiacSR vesicles (McGarry and Williams, 1993) and asa result induces an oscillatory fluctuation in cardiacresting membrane potential, an increase in myocardialautomaticity and ultimately the development of cardiacarrhythmias. Both systolic and diastolic intracellularcalcium concentrations increase during digitalis-inducedarrhythmias leading to the notion that calcium overloadcontributes to the overall arrhythmogenic effects of digi-talis. It is believed that spontaneous cycles of calciumrelease and reuptake ensue resulting in afterdepolariza-tions (abnormal depolarizations of cardiac myocytes thatinterrupt Phases 2, 3 or 4 of the cardiac action poten-tial and lead to cardiac arrhythmias) and aftercontractions(Hauptman and Kelly, 1999).
There is some evidence to suggest that increasedcardiac sympathetic activity is involved in digitalis-induced cardiotoxicity. Experimental studies demonstratethat stimulation of central α-adrenoceptors depressescardiotoxicity (Chen et al., 1991; Thomas and Stephen,1991), whereas β-adrenoceptor blockers (Mest et al.,
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

12 General, Applied and Systems Toxicology
1995; Nakanishi et al., 1992) can reduce these arrhyth-mias. Other proposed mechanisms of toxicity includethe involvement of nitric oxide (Altug et al., 1999),cyclo-oxygenase products (Mest et al., 1981; Moffatet al., 1986; 1987), ROS (Schlieper and Tawfik, 1987;Ark et al., 1999; Tian et al., 2003) and magnesium(Kafiluddi et al., 1989).
In summary, digitalis glycosides alter the normalcontractile and rhythmic function of the heart. Theyalter impulse formation and conduction through theireffect on ion homeostasis. Cardiac glycosides indirectlyincrease intracellular calcium levels through inhibitionof the plasma membrane Na+-K+ ATPase resulting ina positive inotropy. Additionally the magnitude of theresting membrane potential is reduced and in myocardialautomaticity is increased, leading to increased suscepti-bility for arrhythmias.
8.3 Antiarrhythmic Drugs
Antiarrhythmic drugs affect the heart by directly or indi-rectly altering membrane ion conductance across themembrane of the myocardial cell. Antiarrhythmic drugssuch as the fast Na+-channel blockers (Class I), whichinclude lidocaine, procainamide, quinidine and phenytoinimpair intraventricular conduction. These agents can beresponsible for life-threatening arrhythmias after eitheran accidental intravenous administration or enhancedabsorption from an injection site. Accidental intravenousinjection in humans or experimental injection in labora-tory animals has been shown to result in a variety ofcardiac tachyarrhythmias, including the common occur-rence of ventricular fibrillation. The mechanisms bywhich Class I antiarrhythmics produce cardiac rhythmdisturbances are incompletely characterized, but havebeen assumed to result from excessive blockade of Na+channels. However, interactions with Ca2+ channels, K+channels and SR-associated calcium channels, as wellas many other ion channels and enzymes have beendemonstrated (MacMahon et al., 1988; Hondeghem andKatzung, 1977; Bolger et al., 1987; Castle, 1990; Kindleret al., 1999; Tovey et al., 1998). Any of these actionson membrane-associated ion channels could potentiallytrigger arrhythmias and account for cardiotoxicity.
8.4 Tricyclic Antidepressants
Cyclic antidepressants have been used in the treatmentof major depression since the late 1950s. Currently,cyclic antidepressants are also utilized in the treatment ofchronic pain syndromes and for migraines. Cyclic antide-pressants were identified to have a low threshold for toxi-city following reports of overdose shortly after their use
in the 1950s. Although in the past 10 years, the prescrip-tion of cyclic antidepressants has declined significantlywith the arrival of selective serotonin reuptake inhibitors(SSRIs), they remain second only to analgesics as themost common drugs implicated in overdose fatalities. Themost commonly prescribed cyclic antidepressants includethe following: amitriptyline, desipramine, imipramine,nortriptyline, doxepin and clomipramine (Hong et al.,1974; Coull et al., 1970; Curry et al., 1971).
Significant adverse effects are generally seen at dosesof greater than 20 mg kg−1 d−1, in aged patients withpre-existing heart disease, and in situations where drugadministration is uncontrolled long term (Freeman et al.,1969; Rasmussen, 1965). The toxic effects of cyclicantidepressants are primarily related to the pharmaco-logic effects of these drugs (Cairncross and Gershon,1962). Cyclic antidepressants exhibit a number of phar-macologic effects that include anticholinergic and anti-histamine activity, α-adrenergic blockade, inhibition ofnorepinephrine and serotonin reuptake and blockade offast sodium channels in myocardial cells, resulting inquinidine-like effects on the heart (Robinson, 1965;Williams and Sherter, 1971; Rosenbaum et al., 1969;Sacks et al., 1968). The most serious adverse effectsof cyclic antidepressant toxicity are due to centralnervous system effects and cardiovascular instability.Depressed mental status is generally caused by the anti-histamine and anticholinergic properties of cyclic antide-pressants. Life-threatening cardiovascular complicationsare due to impaired conduction from fast sodium-channelblockade. The impairment decreases the slope of Phase0 depolarization, widens the QRS complex, and prolongsthe PR and QT intervals, resulting in alterations incardiac conduction. Impaired cardiac conduction maylead to heart block and unstable ventricular arrhyth-mias or asystole. Cyclic antidepressants have also beenshown to directly depress myocardial contractility andinduce profound hypotension, due to vasodilatation fromdirect α-adrenergic blockade in serious poisoning situa-tions.
8.5 Antihistamines
Antihistamines are the most widely used drugs in thetreatment of allergic reactions of all kinds. Their mainaction is to counter the effects of histamine, one ofthe chemicals released in the body when there is anallergic reaction. The antihistamine drugs, known asH1 blockers, block the action of histamine on certainreceptors, known as H1 receptors. Several clinicallyuseful drugs (such as chlophenamine (formally chlor-pheniramine), brompheniramine, triprolidine, hydrox-yzine and diphenhydramine), able to antagonize theeffects of histamine at the level of the H1 receptor,were developed in the late 1940s and early 1950s.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 13
Following the development and success of these earlyantihistamines (first-generation antihistamines), hundredsof new antihistamine drugs (second-generation antihis-tamines) were synthesized and marketed with outstandingsuccess. The more recently introduced antihistaminesinclude: acrivastine, astemizole, cetirizine, ebastine, levo-carbastine, loratadine, fexofenadine, ketotifen and oxato-mide. These second-generation antihistamine drugs hadimproved selectivity for histamine receptors and lacksedative effects (Taglialatela et al., 2000).
Despite the enormous therapeutic effects of thesedrugs (both first- and second-generation antihistamines)in the treatment of allergies, in the mid 1980s severalreports appeared in the literature indicating theoccurrence of cardiotoxicity after the administration ofastemizole or terfenadine, two of the most successfulsecond-generation antihistamines on the market(Soldovieri et al., 2008). Astemizole and terfenadinewere withdrawn from the market in several countriesbecause they caused the rare occurrence of torsades depointes (TdPs) (Paakkari, 2002). TdPs is a potentiallyfatal polymorphic ventricular arrhythmia that occursin the setting of a marked prolongation of the QTinterval either in patients taking intentional or accidentaloverdoses of these two antihistamines or in insubjectswith predisposing CVD (Taglialatela et al., 2000). Themetabolic products of astemizole, desmethyl astemizoleand norastemizole are cardiotoxic, whereas fexofena-dine, the active metabolite of terfenadine is devoid ofcardiotoxicity. Terfenadine and astemizole were shownto cause a prolonged QT-interval in the ECG (Paakkari,2002). This effect was soon demonstrated to be associ-ated with an impaired repolarization of cardiomyocytesdue to a selective blockade of cardiac potassium currents(Paakkari, 2002; Soldovieri et al., 2008).
8.6 Aliphatic Alcohols
Ethanol consumption has been associated with a varietyof CVD. In the 1950s evidence began to emergeto suggest that alcohol has a direct toxic effect onthe myocardium. Over the last 25 years research hasbeen conducted to characterize the cardiotoxicity asso-ciated with alcohol consumption and it is now wellrecognized that the heart is a primary target for thedamaging effects of excessive ethanol consumption(Urbano-Marquez et al., 1989). Upon autopsy, individ-uals who have consumed excessive amounts of alcoholhave been observed to have cardiac enlargement, oftenwith thickened regions of the endocardium and otherpathological and histological symptoms of heart failure,such as interstitial fibrosis, hypertrophy and atrophyof myocytes, together with focal regions of myocar-dial necrosis (Teragaki et al., 1993). Alcohol use has
been shown to have numerous effects on the cardiovas-cular system. It has been associated with arrhythmias,heart failure, cardiomyopathy, hypertension and stroke.The most prevalent form of alcoholic heart disease iscardiomyopathy, which is characterized by depressedcardiac output, reduced myocardial contractility and dila-tion of all four chambers of the heart (Richardson et al.,1986). Alcoholic cardiomyopathy develops primarilyafter prolonged periods of sustained and daily heavydrinking, generally exceeding a period of 10 years.
Ethanol has been shown to induce structural changesthat often precede functional alterations in the heart. Anincrease in left ventricular mass is a common struc-tural change that often precedes contractile alterations.Impairment of cardiac function appears to develop incre-mentally with increasing ethanol consumption until overtalcoholic cardiomyopathy manifests itself. Progression tocardiomyopathy is associated with substantial ventricularand atrial dilation, as well as mitral valve regurgitation,which may be associated with ethanol-induced papillarymuscle insufficiency (Teragaki et al., 1993; Nakanishiet al., 1990). Ethanol is also known to cause rhythmeffects of the heart and there are a number of abnormal-ities that may be associated with resulting arrhythmiasseen in alcoholics. Alcoholics often have atrial dysrhyth-mias and these may be attributed to effects on conductiontimes and increases in action potential refractory periods(Teragaki et al., 1993; Regan, 1978).
Reports on the short-term effects of ethanol ingestionare somewhat contradictory. Some studies indicate thatacute ethanol ingestion induces a direct negative inotropicand chronotropic effect on the myocardium (Thomaset al., 1994). However, others have reported no changeor enhancement of rhythm and contractility. The mostcommon observation following acute ethanol ingestionis a modest increase in heart rate, which is assumed tobe a secondary consequence of the action of ethanol onautonomic regulation of the heart (Patel et al., 1997).Acute ethanol intake has been shown to increase systolictime in healthy volunteers. Under conditions of auto-nomic blockade, increases in systolic times are said tobe associated with reduced myocardial contractility andblood ethanol levels of approximately 110 mg dl−1 (or20 mM) (Ahmed et al., 1973; Child et al., 1979).
Investigations into the cellular mechanisms of the acuteethanol affects on contractile function have been mainlybased on experiments in animal models. In vivo exper-imentation on the effects of ethanol on cardiac contrac-tility, in animals as well as in humans, is complicated dueto the indirect effects ethanol has on other elements ofthe cardiovascular system. However, a number of studiesin dogs have demonstrated that ethanol, at blood levelsbetween 70–310 mg dl−1, causes decreased contractilefunction (Mendoza et al., 1971). The acute effect ofethanol is more pronounced under conditions of auto-nomic blockade (Child et al., 1979). In vitro investiga-tions of acute ethanol affects on isolated cardiac muscle
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

14 General, Applied and Systems Toxicology
preparations have indicated that ethanol concentrations of20–200 mM depress cardiac contractility (Hirota et al.,1976). Ethanol concentrations of 70 mM have beenshown to decrease the rate and tension development inrats, ferrets and canines and in human foetal cardiacmuscle preparations (Gimeno et al., 1961; Kobayashiet al., 1979; Richards et al., 1989). Animal studieshave linked acute ethanol exposure with direct nega-tive inotropic effects on the heart and these appear tobe independent of the neuronal and vascular effects ofethanol.
There are several theories that have emerged regardingthe mechanisms of reduced contractile function followingacute ethanol exposures. These include the interferenceof ECC. A number of steps in the ECC have beenproposed as targets of ethanol action. These include theion channels that are responsible for the generation andconduction of action potentials, the release of stored Ca2+from the SR required for contraction, the resequestrationof stored Ca2+ for myocardial relaxation and finally theactivation of contractile proteins by Ca2+ (Richards et al.,1989; Thomas et al., 1991).
The effects of chronic alcohol consumption on cardiacfunction have been examined in a variety of animalmodels. These include the rat, mouse, dog, turkey andrhesus monkey. Structural, metabolic and functionalalterations in cardiac function have been observed inexperimental animal studies of chronic ethanol expo-sure. Experimental studies of chronic ethanol intake inanimals have demonstrated structural abnormalities ofthe heart. The effects observed include a character-istic increased ratio of heart weight to body weight,pronounced left ventricular dilation, reduction in the totalnumber of myocytes comprising the left ventricle, disten-tion of the mitochondrial matrix, swelling of the SRand T-tubules, dehiscence of intercalated discs, disrup-tion of the myofibrillar structure and accumulation oflipid droplets (Segel et al., 1975; Thomas et al., 1980;Bing, 1982). Chronic ethanol feeding in animal studieshas also demonstrated an influence on the metabolicprocesses of the heart. The most pronounced effectdemonstrated is on the capacity of the myocyte foroxidative metabolism. Numerous studies have reported areduced efficiency of mitochondrial oxidative phosphory-lation (Bing, 1982). It has been reported that the reducedoxidative metabolism of heart mitochondria is associatedwith a reduction in fatty acid oxidation and increase intriglyceride deposition in the heart tissue (Bing, 1982). Inaddition, ethanol metabolites have been shown to affectcardiac contractile function. The best characterized ofthese metabolites is acetaldehyde, which has been demon-strated to decrease action potential duration in Purkinjefibres, inhibit Na+/K+-ATPase activity in sarcolemmaand enhance catecholamine release at concentrations of>0.4 mM (Sorrell and Tuma, 1987).
Ethanol metabolites, such as fatty acid ethyl esters, thatare a result of nonoxidative ethanol metabolism, have
been shown to accumulate in the hearts of ethanol-fedanimals (Lange, 1991). These metabolites have beensuggested to disrupt sarcolemma functions. A varietyof long-term ethanol feeding studies in animals havedemonstrated clear and consistent depressive effects oncardiac contraction and increase in the vulnerability ofthe heart to fibrillation following acute ethanol adminis-tration.
In summary, ethanol has acute negative inotropiceffects on the heart, which are mediated by direct actionon the cardiac muscle. Some theories have arisen inregard to the mechanisms of cardiotoxity induced byacute ethanol exposures, but the alteration of intracel-lular calcium seems to stand out as a major mechanismfor cardiac dysfunction following acute exposures. Thechronic effects of long-term frequent episodes of ethanolconsumption on cardiac function is assumed to be aresult of the cumulative effects of the cardiac actions ofthis agent ultimately leading to degeneration of contrac-tile function and cardiomyopathy. The mechanism ofcardiac damage produced by chronic alcohol exposureremains unclear. However, several theories have arisenbased on clinical and experimental evidence derivedfrom human and animal studies. Proposed mechanismsof toxicity include: the generation of toxic metabo-lites, interference with normal metabolic processes, alter-ations in mitochondrial structure, alteration in calciummetabolism and glutathione content, inhibition of proteinsynthesis, fatty acid ester accumulation, inhibition ofcalcium–myofilament interactions and disruption of cellmembrane structure.
8.7 Hydrocarbons
A variety of hydrocarbons, with and without halogensubstitution, have long been known to sensitize theheart to adrenaline-induced arrhythmias (Himmel, 2008;Hermann and Vial, 1935; Garb and Chenoweth, 1948;Hays, 1972; Reinhardt et al., 1973). For example,chlorofluorocarbons (CFCs) have been demonstrated toproduce ventricular arrhythmias. CFC exposure studies indogs have demonstrated the ability of this hydrocarbon tosensitize the myocardium to exogenous adrenaline. Rein-hardt et al. (1971) exposed dogs to varying concentrationsof CFC-12 for periods of 0.5–10 minutes and found thata concentration of CFC-12 in air of 250 g m−3 (5%) sensi-tized the heart to an intravenous dose of adrenaline (8 µg(kg body weight)−1). Similar findings were observed inrabbit exposure studies; however, the arrhythmogenicthresholds of CFCs are known to be dependent upon theanimal species and concentration of exogenous adrenaline(Lessard and Paulet, 1986).
The arrhythmogenic potency of CFCs, derived throughinhalation studies, has been shown to be dependent on the
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 15
degree of fluorination. It has been shown that as fluori-nation increases within a homologous series of CFCs,the arrythmogenic potency decreases. For example, forthe chlorofluoromethanes, the arrhythmogenic potency ofCFC-11 seems to be greater than that of CFC-12. Asimilar pattern has been observed in fully halogenatedethanes (CFC-113 > CCF-114 > CFC-115) (Reinhardtet al., 1971; 1973; Clark and Tinston, 1972a; 1972b;Wills, 1972). Through animal studies it appears that acritical blood level of CFC is needed to cause cardiacsensitization. It has been hypothesized that differencesin cardiac sensitization among various CFCs may reflectdifferences in absorption characteristics rather than mech-anisms of action at the molecular level (Jack, 1971;Taylor et al., 1971; Clark and Tinston, 1972a; Azar et al.,1973). Similarities in the lowest venous blood concen-trations associated with cardiac sensitization in variousanimal studies suggest that these CFCs act in a similarand nonspecific manner in causing arrhythmias. Thishypothesis is somewhat supported by basic similaritiesin cardiac sensitization caused by these and other halo-substituted hydrocarbons.
Inhalational exposure studies in animals havedemonstrated mixed results regarding the effects ofCFCs on heart rate. Through these numerous studiesit appears that any observed changes induced by aninhalational exposure to CFC is highly dependenton the use of anaesthetic in experimental design, theCFCs, CFC concentration and animal species. Forexample, inhalation of CFC-12 in a gas mixture givento anaesthetized animals has been reported to causebradycardia in mice (Aviado and Belej, 1974), rats(Doherty and Aviado, 1975) and dogs (Flowers andHoran, 1972). No change in heart rate has been observedin monkeys (Belej et al., 1974), rats (Friedman et al.,1973; Watanabe and Aviado, 1975) and cats (Harriset al., 1971). However, tachycardia has been induced inanaesthetized monkeys and unanaesthetized rats (Aviadoand Smith, 1975; Watanabe and Aviado, 1975).
Chlorofluorocarbon gases may exert their effects oncardiac rhythm in two ways; directly on the myocardiumand indirectly through sensitization of the ventricularmyocardium to endogenous catecholamines (Taylor et al.,1971; Aviado and Belej, 1974). The latter theory isconsistent with the blocking of CFC-induced arrhyth-mias by propranolol. Electrophysiological analysis ofCFC-induced effects on different cardiac cells indicatesthat arrhythmias are a result of nonspecific impairmentof the membrane properties and notably the inhibition oftransmembrane ionic currents (Lessard and Paulet, 1985;1986).
Several investigators have attempted to determine ifCFCs affect oxidative phosphorylation. However, theCFCs, CFC-12 and CFC-114 were shown not to affectoxygen consumption or oxidative phosphorylation inmitochondria isolated from the liver, lung, brain, heart orkidney of exposed rats (Griffin et al., 1972). Subsequent
in vitro studies conducted with liver and heart mitochon-dria supported the in vivo findings, also indicating noeffects on either oxidation or phosphorylation (Griffinet al., 1972).
In summary, hydrocarbons have long been known tosensitize the heart to adrenaline-induced arrhythmias;however, the mechanisms of action are not well eluci-dated, fully investigated and understood. Further studiesare required to determine the exact mechanisms of action,although it is proposed that hydrocarbons, halogenated ornot, seem to induce cardiac sensitization through a similarmechanism of action.
8.8 Volatile Substance Abuse
Volatile substance abuse (VSA), referred to as gluesniffing, inhalant abuse, solvent abuse, is the deliberateinhalation of volatile substance for the purposes ofachieving intoxication, has been reported in many partof the world and occurs most commonly in adolescents,individuals living in remote and rural communities,and in individuals whose occupations provide access tothese substances (Flanagan and Ives, 1994). Solventsfrom contact adhesives, including toluene and gasoline,in addition to halogenated solvents and volatile organichydrocarbons (aliphatic hydrocarbons, alkyl halides,alkyl nitrites, aromatic hydrocarbons, ethers andketones), such as those present in cigarette-lighter refills,aerosol propellants, halocarbon fire extinguishers andinhalational anaesthetics are chemical agents that areutilized by volatile substance abusers (Flanagan andIves, 1994; Linden, 1990). In the UK, the most commontypes of substance abused today are butane lighter fueland aerosol inhalers (Harris, 2006). There are also alarge number of deaths annually occurring in the UKas a result of VSA. Substances that are inhaled forthe purpose of recreational self-intoxication have theability to cause asphyxia, arrhythmias, cardiovasculardepression, neurological dysfunction and mucosal,pulmonary and skin irritation following acute exposures.The major risk following acute poisoning is suddendeath. Arrhythmias leading to cardiac arrest are thoughtto be the major causes of sudden death in cases of acutepoisoning. Like CFCs, the aliphatic hydrocarbons foundin solvents utilized by solvent abusers can sensitizethe myocardium to the effects of catecholamines,which can then predispose exposed individuals totachydysrhythmias, which can result in syncope orsudden death.
Deaths occurring from VSA can be classified as a resultof either direct or indirect toxic mechanisms (Harris,2006). Direct toxic effects are thought to account forover half of all VSA-associated deaths in the UK andare thought to be associated with mechanisms related to
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

16 General, Applied and Systems Toxicology
cardiac arrhythmia, vagal inhibition, respiratory depres-sion and anoxia (Shepard, 1989).
Cardiac arrhythmia is considered the most commoncause of direct death in individuals who are termedsolvent abusers (Harris, 2006). Cardiac arrhythmias arisedue to the process of cardiac sensitization. Inhaledvolatile compounds sensitize the myocardium to theeffects of circulating catecholamines. Intravenous admin-istration of epinephrine, in attempted emergency resus-citations, has been associated with cardiac arrest inVSA users admitted to emergency wards (Lawrence,1987).
8.9 Metals
Human exposures to heavy metals have been associatedwith a variety of diseases, including cardiovascular disor-ders. Cadmium, lead, arsenic, cobalt, manganese, nickeland barium have all been associated with CVD.
Arsenic is an environmental toxicant, which has beenused by physicians for more than 2000 years to treatdiseases ranging from cancer to syphilis and tubercu-losis. Arsenic trioxide has also been shown to be clini-cally effective in treating acute promyelocytic leukaemia.However, its use clinically has been restricted due toits cardiotoxic effects (Freeman, 2007). Arsenic is alsoan element found in multiple compounds commonlyencountered in the environment. Human exposure to inor-ganic and organic arsenicals can occur from a varietyof sources, including occupational, medical and envi-ronmental (Lee and Fraumeni, 1969; Watanabe et al.,2004; Westervelt et al., 2001). Whether exposure occursfrom medical therapy (as with the use of arsenictrioxide in cancer treatment) or accidental malicious acutepoisoning, the cardiac effects of high-level acute arsenicexposure are well documented (Westervelt et al., 2001;Hall and Harruff, 1989; Little et al., 1990). Arsenic expo-sure is associated with direct myocardial injury, cardiacarrhythmias and cardiomyopathy (Benowitz, 1992; Gold-smith and From, 1980). Arsenic trioxide has beenshown to cause QT prolongation, TdPs and suddendeath. The exact mechanism by which arsenic trioxidecauses myocardial toxicity remains unclear, although itis believed that arsenic produces extensive organ damageby combining with protein thiol groups. Earlier reportspredicted that oxidative stress might play a crucial role incardiac and vascular abnormalities in different types ofCVDs (Haidara et al., 2006; Dhalla et al., 2000; Bashiret al., 2006). Emerging research also indicates that apop-tosis of terminally differentiated cardiomyocytes maycontribute to the development of myocardial infarction(MI) and CHF. Apoptosis is known to play an importantrole in the pathogenesis of a variety of CVDs, however,the role in acute and chronic myocyte loss associated witharsenic exposures remains to be fully elucidated.
Excessive amounts of cobalt are known to becardiotoxic. Congestive cardiomyopathy has beenreported in people who drank large quantities of beerto which cobalt had been added as a foam stabilizer(Morin and Daniel, 1967; Kesteloot et al., 1968; Sullivanet al., 1969) and in those receiving oral cobalt therapy(Manifold et al., 1978). Although cobalt exposure isassociated with cardiotoxicity, the mechanism for thistoxicity remains unclear.
Cobalt given as a daily subcutaneous injection of cobaltchloride for eight days at doses of 1, 5, 20 and 50 mg(kg bw)−1, produced a marked and dose-dependent accu-mulation of cobalt in the myocardium and a decreasein manganese-superoxide dismutase. Myocardial acutecobalt cardiotoxicity may involve a reduction of intrinsicscavengers resulting in an increased vulnerability tooxygen free-radical toxicity. Cobalt cardiotoxicity mayalso be attributed to its antagonistic action towards theCa2+ ion, as well as its ability to form complexes withmacromolecules. Cobalt interacts with sulfhydryl groupsto impair thiol-enzyme activities (Alexander, 1972). Ina dog model, cobalt myocardial toxicity was character-ized by vacuolation and loss of myofibres (Sanduskyet al., 1981a) with histochemical evidence of severe mito-chondrial damage (Sandusky et al., 1981b). The effectsobserved were hypothesized to be related to cobalt–thiolgroup interaction resulting in citric acid cycle malfunc-tion (Jarvis et al., 1992) and a decrease in myocardialenergetics.
Lead exposure has also been associated with anincreased incidence of CHD, stroke, peripheral arterialdisease (Schober et al., 2006; Lustberg and Silbergeld,2002; Menke et al., 2006; Navas-Acien et al., 2004) andwith cardiovascular function abnormalities, such as leftventricular hypertrophy and alterations in cardiac rhythm(Cheng et al., 1998; Schwartz, 1991). The link betweenlow-level lead exposure and hypertension has been inten-sively studied for many years and an association betweenblood pressure, increases risk of atherosclerosis andcardiovascular mortality has been reported (Rossi, 2008;Patrick, 2006). Animal studies support the possibilitythat lead exposure promotes hypertension and acceler-ates CVD. Chronic treatment of rats with low levels oflead in the drinking water has been shown to elevateblood pressure (Marques et al., 2001). This increase inblood pressure has been linked to the ability of lead metalto increase ROS generation, to inactivate nitric oxidesynthase and to a decrease in nitric oxide.
Like lead, cadmium has also been shown to increaseatherosclerosis in animal models (Subramanyam et al.,1992; Revis et al., 1981) and environmental exposureto cadmium has been suggested to be particularly toxicto heart and blood vessels, in part because of theability of cadmium to increase free-radical generation.Overall, metals that diminish antioxidant defences orincrease radical production could increase the risk ofCVD.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 17
9 AIR POLLUTION
Environmental factors are considered key determinantsof CVD. Although lifestyle choices, such as smoking,diet and exercise are viewed as major environmentalinfluences, the contribution of pollutants and environ-mental chemicals is less clear. Accumulating evidencesuggests that exposure to air pollutants and chemicals inambient air could elevate the risk of CVD. One onlyhas to look back at history to remember the suddenrise in mortality rates and the estimated 4000 prematuredeaths that resulted in 1952 as a result of the great smogin London, England. In December 1952 on days 7 and8, smoke and sulphur dioxide concentrations rose from0.49 to 4.46 mg m−3 and 0.41 to 3.83 mg m−3 respec-tively. It was estimated that 4000 deaths had occurredas a result of the great smog and the main causes forthese deaths were associated with respiratory diseaseand CVD. Respiratory diseases such as emphysema andbronchitis were reported to account for approximately59% of the deaths recorded during the time of the greatsmog. CVD was reported to account for approximately22% of the deaths recorded. Many current epidemi-ological studies report that exposure to fine particlespresent in ambient air is associated with an increase incardiovascular mortality (Yang and Omaye, 2009; Puettet al., 2008; Simkhovick et al., 2008). Statistically signif-icant relationships between particulate air pollution andischaemic heart disease, arrhythmias and heart failurehave been reported. An elevated risk for acute MI (Lankiet al., 2006; Peters et al., 2001) and cardiorespiratorysymptoms (de Hartog et al., 2003) has been reportedin relation to air pollution. Animal studies show thatexposure to ambient air particles increases peripheralthrombosis and atherosclerotic lesion formation. Expo-sures to arsenic, lead, cadmium, pollutant gases, solventsand pesticides have also been linked to increased inci-dence of CVD. Mechanistically, these effects have beenattributed to changes in the synthesis or reactivity of nitricoxide that may be caused by environmental oxidantsor increased endogenous production of reactive oxygenspecies. Alveolar inflammation induced by particles mayeither directly or via oxidative stress lead to systemicinflammation with increased levels of blood coagula-bility, progression of atherosclerosis and destabilizationor even rupture of vulnerable plaques, resulting in acuteischaemic events (Brook et al., 2004; Seaton et al., 1995)and myocardial infarct.
However, future studies are required to identify thecontribution of individual pollutants, as well as mixturesto specific aspects of CVD and myocardial injury. Addi-tionally, the underlying physiological and molecularmechanisms of cardiotoxicity associated with exposuresto environmental contaminants need to be further eluci-dated.
10 CONCLUSIONS
Impaired pump function is the common end point ofcardiotoxicity. Toxicity generally results due to an injuryto the heart muscle and/or an alteration in the conductionsystem of the heart, leading to electrical disturbances thatresult in arrhythmias. The myocardium is very vulnerableto damage as it has no regenerative capacity and injuryto the myocardium can occur as a result of indirect anddirect toxic mechanisms. Some general mechanisms ofinjury to the myocardium of the heart include interferencewith ion homeostasis (Na+, K+, Ca2+), damage throughaltered or insufficient blood supply to the heart muscle,oxidative stress, as a result of ischaemia/reperfusioninjury, organellar dysfunction, as a result of lack of ionichomeostasis, alterations of metabolism and mitochondrialinjury.
Alterations in ion channels can occur as a resultof a primary alteration in ion channels, signalling orcalcium-handling proteins, structural changes in themyocytes or extracellular matrix and changes in theactivity of the neurohumoral system. Inhibition ofNa+/K+-ATPase leads to an increase in intracellularcalcium and a decrease in conduction velocity; Na+-channel blockade decreases conduction velocity, K+-channel blockage decreases repolarization and Ca2+-channel blockade (L-type channel, calcium release) canlead to a decrease in AV conduction.
Pro-oxidant/antioxidant balance determines the degreeof myocardial oxidative stress. Lipid peroxidation canimpair the sarcolemma, cause mitochondrial and SRdysfunction and alter calcium homeostasis. These oxida-tive effects contribute to arrhythmias, myocardial stun-ning and myocyte death.
Cytotoxic calcium overload caused by SR dysfunc-tion, sarcolemmal injury, Na+/K+-ATPase inactivationor sympathetic activation is another common mecha-nism of cardiotoxicity. It results in the breakdown ofhigh-energy phosphates, blebbing of plasma membrane,activation of Ca2+-dependent phospholipases and neutralproteases, Ca2+-activated DNA fragmentation and Ca2+activation on oncocytic and apoptotic cell death. Apop-tosis predominates soon after toxicant-induced injury andis a prominent feature in heart failure. Overall, cardiotoxi-city occurs as a result of affects on biochemical, structuraland functional abnormalities induced by overexposure tocardiotoxic agents.
REFERENCES
Ahmed, S., Levinson, G. E. and Regan, T. J. (1973). Depressionof myocardial contractility with low doses of ethanol innormal man. Circulation , 48, 378–385.
Alexander, C. S. (1972). Cobalt-beer cardiomyopathy. A clin-ical and pathologic study of twenty-eight cases. AmericanJournal of Medicine, 53, 395–417.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

18 General, Applied and Systems Toxicology
Altug, S., Uzun, O., Demiryurek, A. T., Cakici, I., Abacioglu,N. and Kanzik, I. (1999). The role of nitric oxide indigoxin-induced arrhythmias in guinea pigs. Pharmacologyand Toxicology , 84, 3–8.
Ark, M., Cakici, I., Sariahmetoglu, M. and Kanzik, I. (1999).Does prevention of free radical reactions influence digoxinarrhythmias? General Pharmacology and Toxicology , 32,627–630.
Aviado, D. M. and Belej, M. A. (1974). Toxicity of aerosolpropellants on the respiratory and circulatory systems. I.Cardiac arrhythmia in the mouse. Toxicology , 2, 31–42.
Aviado, D. M. and Smith, D. G. (1975). Toxicity of aerosolpropellants in the respiratory and circulatory systems. VIII.Respiration and circulation in primates. Toxicology , 3,241–252.
Azar, A., Trochimowicz, H. J., Terrill, J. B. and Mullin, L. S.(1973). Blood levels of fluorocarbon related to cardiac sensi-tization. American Industrial Hygiene Association Journal ,34, 102–109.
Bashir, S., Sharma, Y., Irshad, M., Nag, T. C., Tiwari, M.,Kabra, M. and Dogra, T. D. (2006). Arsenic induced apop-tosis in rat liver following repeated 60 days exposure. Toxi-cology , 217, 63–70.
Belej, M. A., Smith, D. G. and Aviado, D. M. (1974). Toxi-cology of aerosol propellants in the respiratory and circula-tory systems. IV. Cardiotoxicity in the monkey. Toxicology ,2, 381–395.
Benowitz, N. L. (1992). Cardiotoxicity in the workplace.Occupational Medicine, 7, 465–478.
Bing, R. J. (1982). Effect of alcohol on the heart and cardiacmetabolism. The FASEB Journal , 41, 2443–2446.
Bolger, G. T., Marcus, K. A., Daly, J. W. and Skolnick,P. (1987). Local anesthetics differentiate dihydropyridinecalcium antagonist binding sites in rat brain and cardiacmembranes. The Journal of Pharmacology and ExperimentalTherapeutics , 240, 922–930.
Bristow, M. R., Billingham, M. E., Mason, J. W. and Daniels,J. R. (1978a). Clinical spectrum of anthracycline antibioticcardiotoxicity. Cancer Treatment Reports , 62, 873–879.
Bristow, M. R., Kantrowitz, N. E., Harrison, W. D., Minobe, W.A., Sageman, W. S. and Billingham, M. E. (1983). Mediationof subacute anthracycline cardiotoxicity in rabbits by cardiachistamine release. Journal of Cardiovascular Pharmacology ,5, 913–919.
British Heart Foundation (2006). Coronary Heart DiseaseStatistics. 2006 Edition. http://www.heartstats.org/datapage.asp?id=7998 (accessed 6 May 2009).
British Heart Foundation Promotion Research Group (2005).European Cardiovascular Disease Statistics. 2005 Edition.
Brook, R. D., Franklin, B., Cascio, W., Hong, Y., Howard, G.,Lipsett, M., Luepker, R., Mittleman, M., Samet, J., Smith, S.C., Jr and Tager, I. (2004). Air pollution and cardiovasculardisease: a statement for healthcare professionals from theExpert Panel on Population and Prevention Science of theAmerican Heart Association. Expert Panel on Populationand Prevention Science of the American Heart Association.Circulation , 109, 2655–2671.
Cairncross, K. and Gershon, S. (1962). A pharmacological basisfor cardiovascular complications of imipramine medication.The Medical Journal of Australia , 2, 372–375.
Castle, N. A. (1990). Bupivacaine inhibits the transient outwardK+ current but not the inward rectifier in rat ventricular
myocytes. The Journal of Pharmacology and ExperimentalTherapeutics , 255, 1038–1046.
Chen, S. A., Liu, R. H., Ting, T. H., Chang, M. S.,Chang, B. N. and Kuo, J. S. (1991). Termination ofdigitalis-induced ventricular tachycardias by clonidineinvolves central alpha-adrenoceptors in cats. British Journalof Pharmacology , 103, 1114–1118.
Cheng, Y., Schwartz, J., Vokonas, P. S., Weiss, S. T., Aro,A. and Hu, H. (1998). Electrocardiographic conductiondisturbances in association with low-level lead exposure (theNormative Aging Study). American Journal of Cardiology ,82, 594–599.
Child, J. S., Kovick, R. B., Levisman, J. A. and Pearce, M. L.(1979). Cardiac effects of acute ethanol ingestion unmaskedby autonomic blockade. Circulation , 59, 120–125.
Clark, D. G. and Tinston, D. J. (1972a). The influence offluorocarbon propellants on the arrhythmogenic activities ofadrenaline and isoprenaline. Proceedings of the EuropeanSociety for the Study of Drug Toxicity , 13, 212–217.
Clark, D. G. and Tinston, D. J. (1972b). Cardiac effectsof isoproterenol, hypoxia, hypercapnia, and fluorocarbonpropellants and their use in asthma inhalers. Annals ofAllergy , 30, 536–541.
Cortes, E. P., Lutman, G., Wanka, J., Wang, J. J., Pickren, J. andWallace, J. (1975). Adriamycin (NSC-123127) cardiotoxi-city: a clinicopathologic correlation. Cancer ChemotherapyReports , 6, 215–225.
Coull, D. C., Crooks, J., Dingwall-Fordyce, I., Scott, A. M.and Weir, R. D. (1970). Amitriptyline and cardiac disease.Lancet , 2, 590–591.
Curry, S. H., Lader, M. H., Mould, G. P. and Sakalis, G.(1971). Pharmacology of chlorpromazine; clinical studies.British Journal of Pharmacology , 41, 431P.
Dhalla, N. S., Temsah, R. M. and Netticadan, T. (2000). Roleof oxidative stress in cardiovascular diseases. Journal ofHypertension , 18, 655–673.
Doherty, R. E. and Aviado, D. M. (1975). Toxicity of aerosolpropellants in the respiratory and circulatory systems. VI.Influence of cardiac and pulmonary vascular lesions in therat. Toxicology , 3, 213–224.
Doroshow, J. H. (1983). Effect of anthracycline antibiotics onoxygen radical formation in rat heart. Cancer Research , 43,460–472.
Doroshow, J. H. (1991). Doxorubicin-induced cardiototoxicity.New England Journal of Medicine, 324, 843–845.
Doroshow, J. H., Locker, J. Y. and Myers, C. E. (1980).Enzymatic defences of the mouse heart against reactiveoxygen metabolites: alterations produced by doxorubicin.Journal of Clinical Investigation , 65, 128–135.
Ehrke, M. J., Maccubbin, D., Ryoyama, K., Cohen, S. A. andMihich, E. (1986). Correlation between adriamycin-inducedaugmentation of interleukin 2 production and ofcell-mediated cytotoxicity in mice. Cancer Research , 46,54–60.
Ferrans, V. J. (1978). Overview of cardiac pathology in relationto anthracycline cardiotoxicity. Cancer Treatment Reports ,62, 955–961.
Flanagan, R. J. and Ives, R. J. (1994). Volatile substance abuse.Bulletin on Narcotics , 46, 49–78.
Flowers, N. C. and Horan, L. H. (1972). Effects of respira-tory acidosis on the cardiac response to aerosol inhalation.Clinical Research , 20, 619.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 19
Freeman, K. (2007). Arsenic upsets heartbeat: Possible earlywarning for cardiovascular risk. Environmental HealthPerspectives , 115, A262.
Freeman, J. W., Mundy, G. R. and Beattie, R. R. (1969).Cardiac abnormalities in poisoning with tricyclic antidepres-sants. British Medical Journal , 2, 610–611.
Friedman, M. A., Bozdech, M. J., Billingham, M. E. and Rider,A. K. (1978). Doxorubicin cardiotoxicity. Serial endomy-ocardial biopsies and systolic time intervals. The Journal ofthe American Medical Association , 240, 1603–1606.
Friedman, S. A., Cammarato, M. and Aviado, D. M. (1973).Toxicity of aerosol propellants on the respiratory systems.II. Respiratory and bronchopulmonary effects in the rat.Toxicology , 1, 345–355.
Fujita, N., Hiroe, M., Ohta, Y., Horie, T. and Hosoda, S. (1991).Chronic effects of metoprolol on myocardial ß-adrenergicreceptors in doxorubicin-induced cardiac damage in rats.Journal of Cardiovascular Pharmacology , 17, 656–661.
Garb, S. and Chenoweth, M. B. (1948). Studies onhydrocarbon-epinephrine induced ventricular fibrilla-tion. The Journal of Pharmacology and ExperimentalTherapeutics , 94, 12–18.
Gimeno, A. L., Gimeno, M. F. and Webb, J. L. (1961). Effectsof ethanol on cellular membrane potentials and contractilityof isolated rat atrium. The American Journal of Physiology ,203, 194–196.
Goldsmith, S. and From, A. H. (1980). Arsenic-induced atypicalventricular tachycardia. New England Journal of Medicine,303, 1096–1098.
Griffin, T. B., Byard, J. L. and Coulston, F. (1972). Toxico-logical responses to halogenated hydrocarbons. In Appraisalof Halogenated Fire Extinguishing Agents , Proceedings ofa Symposium, 11–12 April, Washington, DC. US NationalAcademy of Science, Washington, DC, pp. 136–147.
Haidara, M. A., Yassin, H. Z., Rateb, M., Ammar, H. andZorkani, M. A. (2006). Role of oxidative stress in devel-opment of cardiovascular complications in diabetes mellitus.Current Vascular Pharmacology , 4, 215–227.
Hall, J. C. and Harruff, R. (1989). Fatal cardiac arrhythmia in apatient with interstitial myocarditis related to chronic arsenicpoisoning. Southern Medical Journal , 82, 1557–1560.
Haq, M. M., Legha, S. S., Choksi, J., Hortobagyi, G. N.,Benjamin, R. S. and Ewer, M. (1985). Doxorubicin-inducedcongestive heart failure in adults. Cancer , 56, 1361–1365.
Harris, D. (2006). Volatile substance abuse. Archives of Diseasein Childhood: Education and Practice Edition , 91, 93–100.
Harris, W. S., Kilen, S. M., Taylor, G. J. and Levitsky, S.(1971). Evidence from animals and man that freon depressesmyocardial contractility. Circulation , 44, 119.
de Hartog, J. J., Hoek, G., Peters, A., Timonen, K. L.,Ibald-Mulli, A., Brunekreef, B., Heinrich, J., Tiittanen, P.,van Wijnen, J. H., Kreyling, W., Kulmala, M. and Pekkanen,J. (2003). Effects of fine and ultrafine particles on cardiores-piratory symptoms in elderly subjects with coronary heartdisease: the ULTRA study. American Journal of Epidemi-ology , 157, 613–623.
Hauptman, P. J. and Kelly, R. A. (1999). Digitalis. Circulation ,99, 1265–1270.
Hays, H. W. (1972). Etiology of Cardiac Arrhythmias. Proceed-ings of the 3rd Annual Conference on Environmental Toxi-cology, Fairborn, Ohio, 25–27 October, National Technical
Information Service, Springfield, pp. 173–183. (NTIS ADReport No. 7737166).
Heart and Stroke Foundation of Canada (2004). Quick Facts.http://www.heartandstroke.ca .
Henderson, I. C., Allegra, J. C., Woodcock, T., Wolff, S.,Bryan, S. and Cartwright, K. (1989). Randomized clinicaltrial comparing mitoxantrone with doxorubicin in previouslytreated patients with metastatic breast cancer. Journal ofClinical Oncology , 7, 560–571.
Hermann, H. and Vial, J. (1935). Nouvelles syncopescardiaques par association toxique de l’adrenaline et dedivers produits organiques volatiles. Comptes rendus del’Academie des Sciences , 119, 1316–1317.
Himmel, H. M. (2008). Mechanisms involved in cardiac sensi-tization by volatile anesthetics: general applicability to halo-genated hydrocarbons. Critical Reviews in Toxicology , 38,773–803.
Hirota, Y., Bing, O. H. L. and Abelmann, W. H. (1976).Effect of ethanol on contraction and relaxation of isolatedrat ventricular muscle. Journal of Molecular and CellularCardiology , 8, 727–732.
Holmberg, S. R. and Williams, A. J. (1990). Patterns of inter-action between anthraquinone drugs and the calcium-releasechannel from cardiac sarcoplasmic reticulum. CirculationResearch , 67, 272–283.
Hondeghem, L. M. and Katzung, B. G. (1977). Time- andvoltage-dependent interactions of antiarrhythmic drugs withcardiac sodium channels. Biochimica et Biophysica Acta ,472, 373–398.
Hong, W. K., Mauer, P., Hochman, R., Caslowitz, J. G. andParaskos, J. A. (1974). Amitriptyline cardiotoxicity. Chest ,66, 304–306.
Ito, H., Miller, S. C., Billingham, M. E., Akimoto, H., Torti,S. V. and Wade, R. (1990). Doxorubicin selectively inhibitsmuscle gene expression in cardiac muscle cells in vivo andin vitro. Proceedings of the National Academy of Sciences ofthe United States of America , 87, 4275–4279.
Jack, D. (1971). Sniffing syndrome. British Medical Journal ,2, 708–709.
Jarvis, J. Q., Hammond, E., Meier, R. and Robinson, C. (1992).Cobalt cardiomyopathy. A report of two cases from mineralassay laboratories and a review of the literature. Journal ofOccupational Medicine, 34, 620–626.
Kafiluddi, R., Kennedy, R. H. and Seifen, E. (1989). Extracel-lular magnesium and cardiotonic steroid toxicity in isolatedmyocardial preparations. The Journal of Pharmacology andExperimental Therapeutics , 251, 1120–1127.
Kemmerer, D. A. (2008). Devious digoxin: a case review.Journal of Emergency Nursing , 34, 487–489.
Kesteloot, H., Roelandt, J., Willems, J., Claes, J. H. andJoossens, J. V. (1968). An enquiry into the role of cobaltin the heart disease of chronic beer drinkers. Circulation ,37, 854–864.
Kindler, C. H., Yost, C. S. and Gray, A. T. (1999). Localanesthetic inhibition of baseline potassium channels with twopore domains in tandem. Anesthesiology , 90, 1092–1102.
Kobayashi, M., Furukawa, Y. and Chiba, S. (1979). Effectsof ethanol and acetaldehyde on the isolated blood-perfusedcanine atrium. Archives Internationales de Pharmacody-namie et de Therapie, 239, 109–120.
Kusuoka, H., Futaki, S., Koretsune, Y., Kitabatake, A., Suga,H. and Kamada, T. (1991). Alterations of intracellular
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

20 General, Applied and Systems Toxicology
calcium homeostasis and myocardial energetics in acuteadriamycin-induced heart failure. Journal of CardiovascularPharmacology , 18, 437–444.
Lange, L. G. (1991). Mechanism of fatty acid ethyl esterformation and biological significance. Annals of the New YorkAcademy of Sciences , 625, 802–805.
Lanki, T., Pekkanen, J., Aalto, P., Elosua, R., Berglind, N.,D’Ippoliti, D., Kulmala, M., Nyberg, F., Peters, A., Picciotto,S., Salomaa, V., Sunyer, J., Tiittanen, P., von Klot, S. andForastiere, F. (2006). Associations of traffic related air pollu-tants with hospitalisation for first acute myocardial infarc-tion: the HEAPSS study. Occupational and EnvironmentalMedicine, 63, 844–851.
Lawrence, K. (1987). Ethyl Browning’s Toxicity andMetabolism of Industrial Solvents , 2nd edn, Hydrocarbons,vol. 1, Elsevier Science Publishers, BV, Amsterdam.
Lee, A. M. and Fraumeni, J. F. Jr. (1969). Arsenic andrespiratory cancer in man: an occupational study. Journalof the National Cancer Institute, 42, 1045–1052.
Lenaz, L. and Page, J. A. (1976). Cardiotoxicity of adriamycinand related anthracyclines. Cancer Treatment Reviews , 3,111–120.
Lessard, Y. and Paulet, G. (1985). Mechanism of liposolubledrugs and general anesthetic’s membrane action: action ofdifluoromethane (FC 12) on different types of cardiac fibersisolated from sheep hearts. Cardiovascular Research , 19,465–473.
Lessard, Y. and Paulet, G. (1986). A proposed mechanism forcardiac sensitisation: Electrophysiological study of effects ofdifluorodichloromethane and adrenaline on different types ofcardiac preparations isolated from sheep hearts. Cardiovas-cular Research , 20, 807–815.
Linden, C. H. (1990). Volatile substance abuse. EmergencyMedicine Clinics of North America , 8, 559–578.
Little, R. E., Kay, G. N., Cavender, J. B., Epstein, A. E. andPlumb, V. J. (1990). Torsade de pointes and T-U wavealternans associated with arsenic poisoning. Pacing andClinical Electrophysiology , 13, 164–170.
Lustberg, M. and Silbergeld, E. (2002). Blood lead levels andmortality. Archives of Internal Medicine, 162, 2443–2449.
MacMahon, S., Collins, R. and Peto, R. (1988). Effects ofprophylactic lidocaine in suspected acute myocardial infarc-tion. An overview of results from the randomized, controlledtrials. The Journal of the American Medical Association , 260,1910–1916.
Manifold, I. H., Platts, M. M. and Kennedy, A. (1978). Cobaltcardiomyopathy in a patient on maintenance haemodialysis.British Medical Journal , 2, 1609.
Marques, M., Millas, I., Jimenez, A., Garcia-Colis, E.,Rodriguez-Foe, J. A., Velasco, S., Barrientos, A., Casado, S.and Lopez-Farre, A. (2001). Alteration of the soluble guany-late cyclase system in the vascular wall of lead-inducedhypertension in rats. Journal of the American Society ofNephrology , 12, 2594–2600.
McGarry, S. J. and Williams, A. J. (1993). Digoxin activatessarcoplasmic reticulum calcium-release channels: a possiblerole in cardiac inotropy. British Journal of Pharmacology ,108, 1043–1050.
Mendoza, L. C., Helberg, K., Rickart, A., Tilllich, G. and Bing,R. J. (1971). The effect of intravenous ethyl alcohol onthe coronary circulation and myocardial contractility of the
human and canine heart. Journal of Clinical Pharmacology ,11, 165–176.
Menke, A., Muntner, P., Batuman, V., Silbergeld, E. K. andGuallar, E. (2006). Blood lead below 0.48 micromol/L (10microg/dL) and mortality among US adults. Circulation ,114, 1388–1394.
Mest, H. J., Taube, C., Forster, W., Metsa-Ketela, T. andVapaatalo, H. (1981). Influence of cardiac rhythm distur-bances and antiarrhythmic drugs on the efflux of PGE,PGF2alpha, cyclic AMP, and cyclic GMP in canine coronarysinus blood. Prostaglandins and Medicine, 7, 1–13.
Mest, H. J., Thomsen, P. and Raap, A. (1995). Antiarrhythmiceffect of the selective I1-imidazoline receptor modulatormoxonidine on ouabain-induced cardiac arrhythmia in guineapigs. Annals of the New York Academy of Sciences , 763,620–633.
Moffat, M. P., Ferrier, G. R. and Karmazyn, M. (1986).A possible role for endogenous prostaglandins in theelectrophysiological effects of acetylstrophanthidin onisolated canine ventricular tissue. Circulation Research , 58,486–494.
Moffat, M. P., Karmazyn, M. and Ferrier, G. R. (1987).Role of prostaglandins in the arrhythmogenic effects ofouabain on isolated guinea pig hearts. European Journal ofPharmacology , 141, 383–393.
Morin, Y. and Daniel, P. (1967). Quebec beer-drinkers’cardiomyopathy: etiological considerations. CanadianMedical Association Journal , 97, 926–928.
Nakanishi, H., Ono, T., Shirasaka, M. and Yoshida, H. (1992).Suppressive effect of prostaglandin E1, but not prostacyclin,on ouabain-induced ventricular fibrillation in guinea pigs.Fukushima Journal of Medical Science, 38, 105–110.
Nakanishi, O., Yokota, Y. and Fukuzaki, H. (1990).Comparative study of dilated cardiomyopathy andspecific heart muscle diseases from pathophysiolog-ical aspects–echocardiographic observation. JapaneseCirculation Journal , 54, 1147–1157.
Navas-Acien, A., Selvin, E., Sharrett, A. R., Calderon-Aranda,E., Silbergeld, E. and Guallar, E. (2004). Lead, cadmium,smoking, and increased risk of peripheral arterial disease.Circulation , 109, 3196–3201.
Olson, H. M., Young, D. M., Prieur, D. J., LeRoy, A. F.and Reagan, R. L. (1974). Electrolyte and morphologicalterations of myocardium in adriamycin-treated rabbits.American Journal of Pathology , 77, 439–454.
O’Toole, T. E., Conklin, D. J. and Bhatnagar, A. (2008).Environmental risk factors for heart disease. Reviews onEnvironmental Health , 23, 167–202.
Paakkari, I. (2002). Cardiotoxicity of new antihistamines andcisapride. Toxicology Letters , 127, 279–284.
Patel, V. B., Why, H. J., Richardson, P. J. and Preedy, V. R.(1997). The effects of alcohol on the heart. Adverse DrugReactions and Toxicological Reviews , 16, 15–43.
Patrick, L. (2006). Lead toxicity, a review of the literature. Part1: exposure, evaluation and treatment. Alternative MedicineReview , 11, 2–22.
Peters, A., Dockery, D. W., Muller, J. E. and Mittleman, M. A.(2001). Increased particulate air pollution and the triggeringof myocardial infarction. Circulation , 103, 2810–2815.
Praga, C., Beretta, G., Vigo, P. L., Lenaz, G. R., Polini, C. andBonadonna, G. (1979). Adriamycin cardiotoxicity: a surveyof 1273 patients. Cancer Treatment Reports , 63, 827–834.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

Cardiac Toxicology 21
Puett, R. C., Schwartz, J., Hart, J. E., Yanosky, J. D., Speizer,F. E., Suh, H., Paciorek, C. J., Neas, L. M. and Laden, F.(2008). Chronic particulate exposure, mortality and coronaryheart disease in the nurses’ health study. American Journalof Epidemiology , 168, 1161–1168.
Rajagopalan, S., Politi, P. M., Sinha, B. K. and Myers, C. E.(1988). Adriamycin-induced free radical formation in theperfused rat heart: implications for cardiotoxicity. CancerResearch , 48, 4766–4769.
Rasmussen, J. (1965). Amitriptyline and imipramine poisoning.Lancet , 2, 850–851.
Revis, N. W., Zinsmeister, A. R. and Bull, R. (1981).Atherosclerosis and hypertension induction by lead andcadmium ions: an effect prevented by calcium ions. Proceed-ings of the National Academy of Sciences of the United Statesof America , 78, 6494–6498.
Richards, T. S., Kulkarni, A., Brooks, S. M., Lathrop, D. A.,Bremner, W. F. and Sperelakis, N. (1989). A moderateconcentration of ethanol alters cellular membrane potentialand decreases contractile force of human fetal heart. Devel-opmental Pharmacology and Therapeutics , 13, 51–56.
Richardson, P. J., Wodak, A. D. and Atkinson, L. (1986). Rela-tion between alcohol intake, myocardial enzyme activity, andmyocardial function in dilated cardiomyopathy. Evidence forthe concept of alcohol induced heart muscle disease. BritishHeart Journal , 56, 165–170.
Regan, T. J. (1978). Arrhythmias and the “holiday heart”:alcohol-associated cardiac rhythm disorders. American HeartJournal , 95, 555–562.
Reinhardt, C. F., Azar, A., Maxfield, M. E., Smith, P. E. Jr.and Mullin, L. S. (1971). Cardiac arrhythmias and aerosol“sniffing”. Archives of Environmental Health , 22, 265–279.
Reinhardt, C. F., Mullin, L. S. and Maxfield, M. E. (1973).Epinephrine-induced cardiac arrhythmia potential of somecommon industrial solvents. Journal of OccupationalMedicine, 15, 953–955.
Robinson, W. M. (1965). ECG changes in amitriptylinepoisoning. Lancet , 2, 850–851.
Robison, T. W. and Giri, S. N. (1986). Effects of chronicadministration of doxorubicin on myocardial ß -adrenergicreceptors. Life Sciences , 39, 731–736.
Rosenbaum, M. B., Elizari, M. V. and Lazzari, J. O. (1969). Thesyndrome of right bundle branch block with intermittent leftanterior and posterior hemiblock. American Heart Journal ,78, 306–317.
Rossi, E. (2008). Low level environmental lead a continuingchallenge. Clinical Biochemistry Reviews , 29, 63–70.
Sacks, M. H., Bonforte, R. J., Lasser, R. P. and Dimich, I.(1968). Cardiovascular complications of imipramine intox-ication. The Journal of the American Medical Association ,205, 588–590.
Sanderson, S. C., Waller, J., Jarvis, M. J., Humphries, S. E. andWardle, J. (2009). Awareness of Lifestyle Risk Factors forCancer and Heart Disease Among Adults in the UK.
Sandusky, G. E., Henk, W. G. and Roberts, E. D. (1981a).Histochemistry and ultrastructure of the heart in experimentalcobalt cardiomyopathy in the dog. Toxicology and AppliedPharmacology , 61, 89–98.
Sandusky, G. E., Crawford, M. P. and Roberts, E. D. (1981b).Experimental cobalt cardiomyopathy in the dog: a model forcardiomyopathy in dogs and man. Toxicology and AppliedPharmacology , 60, 263–278.
Schlieper, P. and Tawfik, H. (1987). Antiarrhythmic activityof alpha-tocopherol nicotinate and related compounds andtheir physio-chemical properties. Arzneimittelforschung , 37,920–923.
Schober, S. E., Mirel, L. B., Graubard, B. I., Brody, D. J.and Flegal, K. M. (2006). Blood lead levels and deathfrom all causes, cardiovascular disease, and cancer: resultsfrom the NHANES III mortality study. Environmental HealthPerspectives , 114, 1538–1541.
Schwartz, J. (1991). Lead, blood pressure, and cardiovasculardisease in men and women. Environmental Health Perspec-tives , 91, 71–75.
Schwartz, R. G., McKenzie, W. B., Alexander, J., Sager,P., D’Souza, A. and Manatunga, A. (1987). Congestiveheart failure and left ventricular dysfunction complicatingdoxorubicin therapy. Seven-year experience using serialradionuclide angiocardiography. The American Journal ofMedicine, 82, 1109–1118.
Seaton, A., MacNee, W., Donaldson, K. and Godden, D. (1995).Particulate air pollution and acute health effects. Lancet , 345,176–178.
Segel, L. D., Rendig, S. V., Choquet, Y., Chacko, K.,Amsterdam, E. A. and Mason, D. T. (1975). Effects ofchronic graded ethanol consumption on the metabolism,ultrastructural and mechanical function of the rat’s heart.Cardiovascular Research , 9, 649–663.
Simkhovick, B. Z., Kleinman, M. T. and Kloner, R. A. (2008).Air pollution and cardiovascular injury epidemiology, toxi-cology and mechanisms. Journal of the American College ofCardiology , 52, 719–726.
Shan, K., Lincoff, M. and Young, J. B. (1996). Anthracyclin-induced cardiotoxicity. Annals of Internal Medicine, 125,47–58.
Shepard, T. (1989). Mechanism of sudden death associated withvolatile substance abuse. Human Toxicology , 8, 287–292.
Shi, F., MacEwen, E. G. and Kurzman, I. D. (1993). Invitro and in vivo effect of doxorubicin combined withliposome-encapsulated muramyl tripeptide on canine mono-cyte activation. Cancer Research , 53, 3986–3991.
Soldovieri, M. V., Mideli, F. and Taglialetela, M. (2008).Cardiotoxic effects of antihistamines: from basics to clinics( . . . and back). Chemical Research in Toxicology , 21,997–1004.
Sorrell, M. F. and Tuma, D. J. (1987). The functional implica-tions of acetaldehyde binding to cell constituents. Annals ofthe New York Academy of Sciences , 493, 50–62.
Steinberg, J. S., Cohen, A. J., Wasserman, A. G., Cohen, P. andRoss, A. M. (1987). Acute arrhythmogenicity of doxorubicinadministration. Cancer , 60, 1213–1218.
Subramanyam, G., Bhaskar, M. and Govindapp, S. (1992).The role of cadmium induction of atherosclerosis in rabbits.Indian Heart Journal , 44, 177–180.
Sullivan, J. F., George, R., Bluvas, R. and Egan, J. D. (1969).Myocardiopathy of beer drinkers: subsequent course. Annalsof Internal Medicine, 70, 277–282.
Taglialatela, M., Timmerman, H. and Annunziato, L. (2000).Cardiotoxic potential and CNS effects of first generationantihistamines. Trends in Pharmacological Sciences , 21,52–56.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.

22 General, Applied and Systems Toxicology
Taylor, G. J., Harris, W. S. and Bogdonoff, M. D. (1971).Ventricular arrhythmias induced in monkeys by the inhala-tion of aerosol propellants. The Journal of Clinical Investi-gation , 50, 1546–1550.
Teragaki, M., Takeuchi, K. and Takeda, T. (1993). Clinical andhistologic features of alcohol drinkers with congestive heartfailure. American Heart Journal , 125, 808–817.
The Digitalis Investigation Group (1997). The effect of digoxinon mortality and morbidity in patients with heart failure. TheNew England Journal of Medicine, 336, 525–533.
Thomas, G., Haider, B., Oldewurtel, H. A., Lyons, M. M., Yeh,C. K. and Regan, T. J. (1980). Progression of myocardialabnormalities in experimental alcoholism. The AmericanJournal of Cardiology , 46, 233–241.
Thomas, A. P., Rozanski, D. J., Renard, D. C. and Rubin,E. (1994). Effects of ethanol on the contractile function ofthe heart: a review. Clinical and Experimental Research , 18,1221–1131.
Thomas, G. P. and Stephen, P. M. (1991). Protective actionof clonidine against the arrhythmogenic and lethal effectsof ouabain in guinea-pigs. British Journal of Pharmacology ,104, 995–999.
Thomas, A. P., Steward, G., Bolton, M. M., Conahan, S. T.and Renard, D. C. (1991). Effects of ethanol and cocaineon electrically-triggered calcium transients in cardiac musclecells. Annals of the New York Academy of Sciences , 625,395–408.
Tian, J., Liu, J., Garlid, K. D., Shapiro, J. I. and Xie, Z.(2003). Involvement of mitogen-activated protein kinasesand reactive oxygen species in the inotropic action of ouabainon cardiac myocytes. A potential role for mitochondrialKATP channels. Molecular and Cellular Biochemistry , 242,181–187.
Tong, J., Ganguly, P. K. and Singal, P. K. (1991). Myocar-dial adrenergic changes at two stages of heart failure dueto adriamycin treatment in rats. The American Journal ofPhysiology , 260, H909–H916.
Tovey, S. C., Longland, C. L., Mezna, M. and Michelangeli,F. (1998). 2-Hydroxycarbazole induces Ca2+ release fromsarcoplasmic reticulum by activating the ryanodine receptor.European Journal of Pharmacology , 354, 245–251.
Urbano-Marquez, A., Estruch, R. and Navarro-Lopez, F.(1989). The effects of alcoholism on skeletal and cardiacmuscle. The New England Journal of Medicine, 320,409–415.
Von Hoff, D. D., Layard, M. W., Basa, P., Davis, H. L.,Von Hoff, A. L. and Rozencweig, M. (1979). Risk factorsfor doxorubicin-induced congestive heart failure. Annals ofInternal Medicine, 91, 710–717.
Von Hoff, D. D., Rozencweig, M., Layard, M., Slavik, M. andMuggia, F. M. (1977). Daunomycin-induced cardiotoxicityin children and adults. A review of 110 cases. The AmericanJournal of Medicine, 62, 200–208.
Watanabe, T. and Aviado, D. M. (1975). Toxicity of aerosolpropellants in the respiratory and circulatory systems. IV.
Influence of pulmonary emphysema and anesthesia in therat. Toxicology , 3, 225–236.
Watanabe, C., Kawata, A., Sudo, N., Sekiyama, M., Inaoka, T.,Bae, M. and Ohtsuka, R. (2004). Water intake in an Asianpopulation living in arsenic-contaminated area. Toxicologyand Applied Pharmacology , 198, 272–282.
Wakasugi, S., Wada, A., Hasegawa, Y., Nakano, S. andShibata, N. (1992). Detection of abnormal cardiac adrenergicneuron activity in adriamycin-induced cardiomyopathy withiodine-125-metaiodobenzylguanidine. Journal of NuclearMedicine, 33, 208–214.
Westervelt, P., Brown, R. A., Adkins, D. R., Khoury, H., Curtin,P., Hurd, D., Luger, S. M., Ma, M. K., Ley, T. J. andDipersio, J. F. (2001). Sudden death among patients withacute promyelocytic leukemia treated with arsenic trioxide.Blood , 98, 266–271.
World Health Organization (2002). The World Health Report2002. Reducing Risks, Promoting Healthy Life. WorldHealth Organization, Geneva.
Williams, R. B. and Sherter, C. (1971). Cardiac complica-tions of tricyclic antidepressant therapy. Annals of InternalMedicine, 74, 395–398.
Wills, J. H. (1972). Sensitization of the Heart toCatecholamine-Induced Arrhythmia. Proceedings ofthe 3rd Annual Conference on Environmental Toxicology,Fairborn, Ohio, 25–27 October Springfield, NationalTechnical Information Service, Virginia, p. 249. (NTIS ADReport No. 773766).
Wu, A. H. (2008). Cardiotoxic drugs: clinical monitoring anddecision making. Heart , 94, 1503–1509.
Yang, W. and Omaye, S. T. (2009). Air pollutants, oxidativestress and human health. Mutation Research , 674, 45–54.
FURTHER READING
Bristow, M. R., Thompson, P. D., Martin, R. P., Mason,J. W., Billingham, M. E. and Harrison, D. C. (1978b).Early anthracycline cardiotoxicity. The American Journal ofMedicine, 65, 823–832.
Bristow, M. R., Mason, J. W., Billingham, M. E. and Daniels,J. R. (1978c). Doxorubicin cardiomyopathy: evaluation byphonocardiography, endomyocardial biopsy, and cardiaccatheterization. Annals of Internal Medicine, 88, 168–175.
Flanagan, R. J., Ruprah, M., Meredith, T. J. and Ramsev, J. D.(1990). An introduction to the clinical toxicology of volatilesubstances. Drug Safety , 5, 359–383.
Viado, D. M. and Smith, D. G. (1975). Toxicity of aerosolpropellants in the respiratory and circulatory systems. VIII.Respiration and circulation in primates. Toxicology , 3,241–252.
General and Applied Toxicology, Online 2009 John Wiley & Sons, Ltd.This article is 2009 John Wiley & Sons, Ltd.DOI: 10.1002/9780470744307.gat067General and Applied Toxicology was renamed as General, Applied and Systems Toxicology in 2011 2011 John Wiley & Sons, Ltd.