Embed Size (px)
Citation preview

General Anatomy andOsteology of
Head and Neck
General Anatomy andOsteology of
Head & Neck
Mahdi HasanMBBS, M.S., (Honours)
Ph.D., D. Sc., FAMSFNASC, FICS, FNA
Recipient of Dr. B.C. Roy National AwardHony Professor, Dept of Anatomy
CSM Medical University, Erstwhile K.G. Medical College, Lucknow
Prashant PratapLecturer
Saraswati Dental College, Lucknow
I.K. International Publishing House Pvt. Ltd.NEW DELHI • BANGALORE
Published byI.K. International Publishing House Pvt. Ltd.S-25, Green Park ExtensionUphaar Cinema MarketNew Delhi - 110 016 (India)E-mail: [email protected]
ISBN 978-81-907770-5-6
© 2009 I.K. International Publishing House Pvt. Ltd.
All rights reserved. No part of this publication may be reproduced, storedin a retrieval system, or transmitted in any form or any means: electronic,mechanical, photocopying, recording, or otherwise, without the priorwritten permission from the publisher.
Published by Krishan Makhijani for I.K. International Publishing HousePvt. Ltd., S-25, Green Park Extension, Uphaar Cinema Market, NewDelhi - 110 016 and Printed by Rekha Printers Pvt. Ltd., Okhla IndustrialArea, Phase II, New Delhi - 110 020.

Preface
This book covers essentials of gross anatomy of head and neck leaving outminutia but highlighting aspects of clinical application. It is different fromthe books, available on this subject in India on many accounts. First, it includesnot only gross anatomy but also relevant details of osteology which is crucialfor conceptualizing anatomical relations. Also it embodies essentials ofhistology with emphasis on identification of histology slides with the help ofdifferential diagnosis tabulated for easy assimilation. Essentials of embryologyrequired for the first professional BDS has also been highlighted. Need wasfelt for inclusion of all these as well as anthrometry required by the studentsof dentistry for orthodontia. Deficiencies in the aforementioned areas werefelt by the Co-author (Prashant Pratap) as a first year student who discussedthe problem with his teacher and mentor (Mahdi Hasan) and this book is theresult of unique student-teacher collaboration. It took around five years tocomplete this project, during this period the Co-author passed all Professionalexaminations with flying colours. Inputs from his experience of later years inthe areas of oral pathology, oral surgery, prosthodontia, periodontia andorthodontia have enriched this book.
We are highly thankful to Dr. A. Halim for his permission to use somefigures from his BDS book, recently published by I.K. International PublishingHouse Pvt. Ltd.
It is our earnest hope that the unique manner in which this book hasevolved with focus on clinical applications will find favours with students ofdentistry of India and neighbouring countries.
Mahdi HasanPrashant Pratap
1. Scalp 1
2. Triangle of the Neck 7
3. Infrahyoid Muscles: Ribbon Muscles or Strap Muscles 20
4. Suprahyoid Muscles 22
5. Muscles of the Eyeball 25
6. Temporomandibular Joint: Craniomandibular Joint 29
7. Muscles of Mastication 36
8. Paranasal Air Sinuses 43
9. Tongue 48
10. Pharynx 53
11. Larynx 64
12. Parasympathetic Ganglia 69
13. Arteries of Head and Neck 74
14. Veins of Head and Neck 85
15. Craniometry: Anthropometry of the Skull 88
16. Meninges 93
17. Dural Venous Sinuses 95
18. Cavernous Sinus 100
19. Thyroid Gland 103
Contents

viii Contents
OSTEOLOGY
20. Nerve Supply of Muscles of Head & Neck at a Glance 109
21. Parotid Gland 111
22. Submandibular Gland 115
23. Articulated Skull 119
24. Maxilla 122
25. The Frontal Bone 128
26. The Parietal Bone 132
27. The Palatine Bone 136
28. Interior of the Skull 139
29. Norma Basalis 146
30. Norma Lateralis 153
31. Norma Occipitalis 160
32. Norma Verticalis 161
33. The Ethmoid Bone 163
34. The Mandible 166
35. The Nasal Bones 174
36. The Occipital Bone 175
37. The Sphenoid Bone 183
38. The Temporal Bones 192
39. The Zygomatic Bone 200
HISTOLOGY
Tables for Identification of Cells and Tissues 205
Index 217
1Scalp
DEFINITION
Scalp comprises soft tissues covering the vault of the skull.
EXTENT
Generally hair bearing area on the top of the head. More precisely, from beforebackward: eyebrows to the superior nuchal line, side to side from onezygomatic arch to another, though the epicranial aponeurosis is adherent tothe temporal lines on either side.
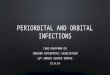
LAYERS
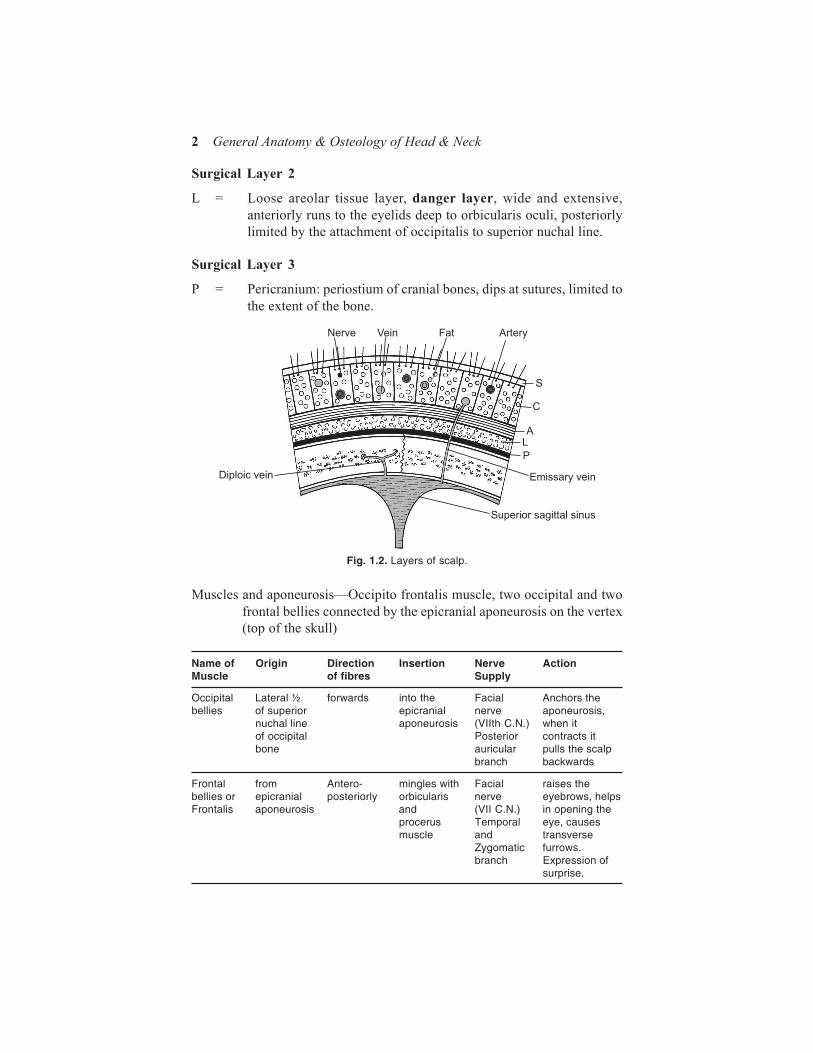
Surgical layer 1
S = skin, thick and rich in hair and sebaceous glandsC = Connective tissues, dense, interlacing criss-cross septa enclosing
small spaces occupied by blood vessels and nervesA = Aponeurosis - epicranial aponeurosis (of occipito frontalis muscle)
also called galea (helmet) aponeurotica
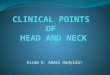
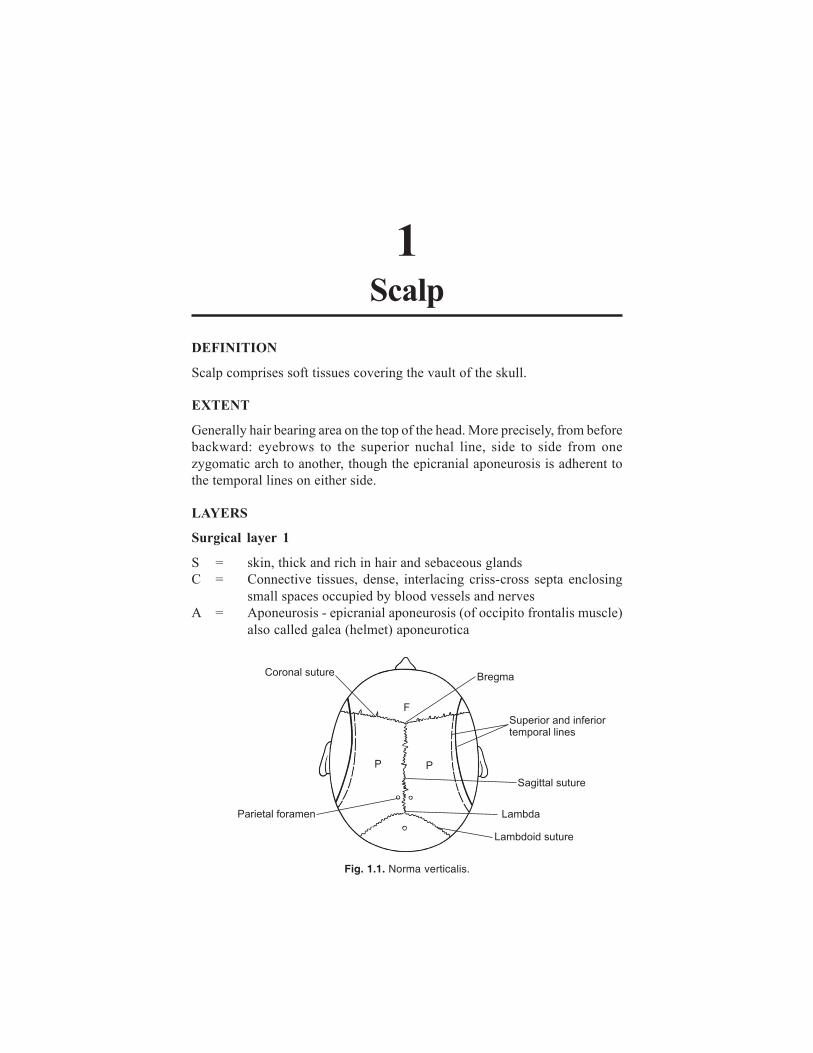
Fig. 1.1. Norma verticalis.
2 General Anatomy & Osteology of Head & Neck
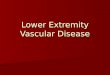
Muscles and aponeurosis—Occipito frontalis muscle, two occipital and twofrontal bellies connected by the epicranial aponeurosis on the vertex(top of the skull)
Name of Origin Direction Insertion Nerve ActionMuscle of fibres Supply
Occipital Lateral ½ forwards into the Facial Anchors thebellies of superior epicranial nerve aponeurosis,
nuchal line aponeurosis (VIIth C.N.) when itof occipital Posterior contracts itbone auricular pulls the scalp
branch backwards
Frontal from Antero- mingles with Facial raises thebellies or epicranial posteriorly orbicularis nerve eyebrows, helpsFrontalis aponeurosis and (VII C.N.) in opening the
procerus Temporal eye, causesmuscle and transverse
Zygomatic furrows.branch Expression of
surprise.
Surgical Layer 2
L = Loose areolar tissue layer, danger layer, wide and extensive,anteriorly runs to the eyelids deep to orbicularis oculi, posteriorlylimited by the attachment of occipitalis to superior nuchal line.
Surgical Layer 3
P = Pericranium: periostium of cranial bones, dips at sutures, limited tothe extent of the bone.
Fig. 1.2. Layers of scalp.
Scalp 3
APPLIED ANATOMY OF SCALP
1. Skin: Rich in hair, very strong. If caught in machinery, the first 3layers of the scalp come out (avulsion of scalp) but the hair, do notbreak. Plenty of sebaceous glands are present in the scalp, hence it isa common site for development of sebaceous cysts.
2. Dense Connective tissues: Binds skin to the galea by criss-cross septa,containing blood vessels and nerves. Blunt injury causes localisedaccumulation of blood, (haematoma) which is very painful (due to richnerve supply of scalp). If a cut or open wound occurs profuse bleedingoccurs as the cut blood vessels are not able to retract (due to theadherence to the fibrous septa). Local pressure against the bone or atourniquet (band) tied around the head (just above the level of theeyebrow is required to arrest the bleeding (as blood vessels to scalpcome from periphery-centripetally).
3. If galea aponeurotica is cut in the coronal plane, the wound gapes(margins are pulled apart by the occipital and frontal bellies in thelong axis of scalp.
4. Bleeding in loose areolar tissue layer causes a mobile haematoma (whichcan be pushed forward towards the eyes or backwards) extensivecollection of blood occurs which gravitates to eyelids, leading to blackeye after a few hours.
5. Bleeding deep to pericranium, commonly occurs in newborn babiesafter difficult childbirth (where a narrow pelvis compresses the largehead of the baby during childbirth cephalo-pelvic disproportion). This
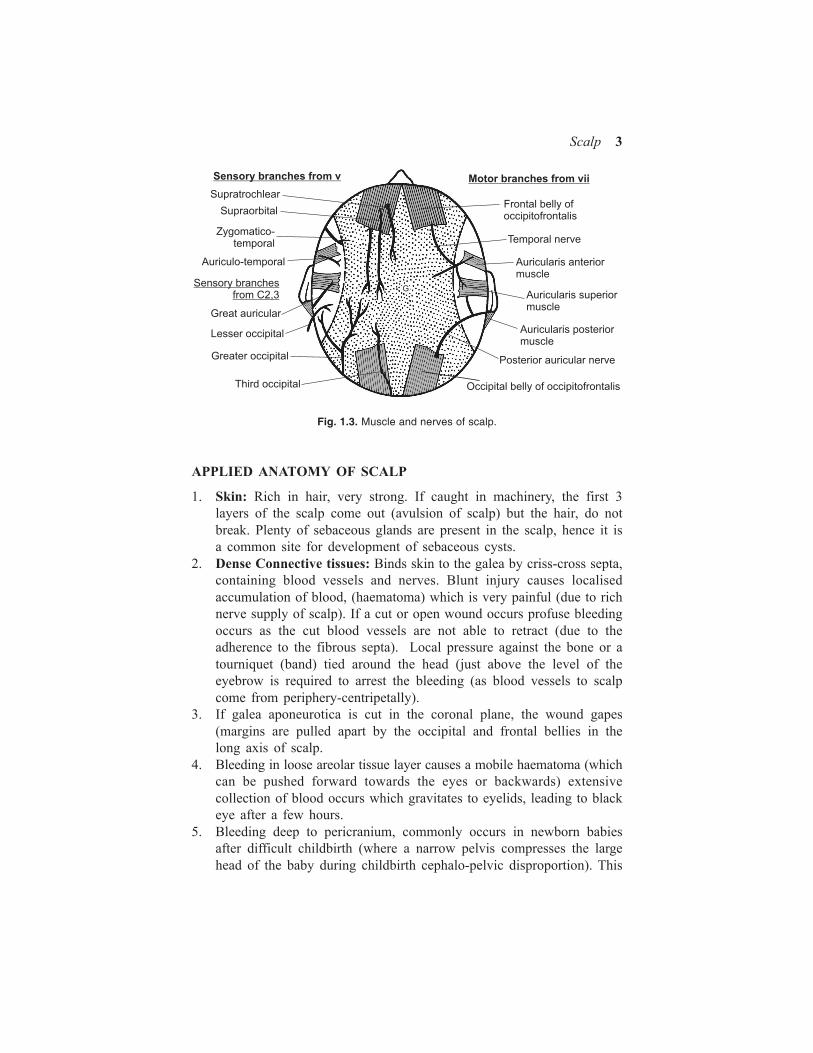
Fig. 1.3. Muscle and nerves of scalp.

General Anatomy And Osteology Of HeadAnd Neck
Publisher : IK International ISBN : 9788190777056 Author : Mahdi Hasan AndPrashant Pratap
Type the URL : http://www.kopykitab.com/product/6034
Get this eBook
30%OFF