Embed Size (px)
Citation preview

Personalized Genetic Testing
12855 SW 132 Street Suite 101, Miami, FL 33196
Phone: (786) 732-4679 • Fax: (305) 978-8590
Web: www.pgenetic.com
Laboratory Director: Ana Margarita Espina Hernandez, Ph.D
Patient: Doe, John
Date of Birth: Jan 01, 1955
Gender: Male
Sample ID: 1000.99999
Physician: Test
Practice: Test
Anytown, NJ
Phone: Test
Date Collected: Feb 25, 2016
Date Received: Jan 29, 2016
Date Reported: Apr 11, 2016
Specimen type: Buccal Swab
GeneDose LIVE
Individualized, additional therapeutic decision support
information based on John Doe's genetics, drug regimen,
indications, demographics, and lifestyle indicators are available at
GeneDose™ LIVE via this secured URL:
http://checkdru.gs/
GeneDose Key: dXXHXXF54
Table of Contents
Pg. 1Genetic Summary
Pg. 2Current Regimen Risk Chart
Pg. 3Current Regimen Risk Detail (by severity)
Pg. 10Thrombosis Profile
Pg. 11ApoE Genotype Information
Pg. 12Medications Summary
Pg. 15Medication Report Details (by therapeutic class)
Pg. 27Clinical Evidence Levels
Pg. 28Patient Information Card
AppendixSNP Report
Genetic Summary Information
† When multiple activities are listed, check information in Medication
Report Details (Pg. 15) for specific medication of interest.
Uncertain = No known diplotype/result (name) or activity for this
combination of genetic variants; Uninterpretable Genotype.
Genetic Summary
Gene Result Activity †
ApoE ɛ3|ɛ3 See ApoE Genotype Info.
CYP2C19 *1|*1 Extensive metabolizer
CYP2C9 *1|*1 Extensive metabolizer
CYP2D6 *5|*41 Intermediate metabolizer
CYP3A4 *1A|*1A Extensive metabolizer
CYP3A5 *3|*3 Poor metabolizer
Factor V Leiden Normal See thrombosis profile
MTHFR (A1298C) Normal See thrombosis profile
MTHFR (C677T) Variant See thrombosis profile
Prothrombin (F2) Normal See thrombosis profile
SLCO1B1 *1|*1 Normal liver uptake
activity
VKORC1 *1|*1 Normal (with respect to
Warfarin)
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 1 of 28
Powered by:
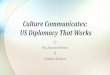
Current Regimen Risk Chart
This chart shows each medication input into GeneDose LIVE for John Doe. The longer a bar is in this chart, the more risky the medication may be.
0 to 5 - Few risks; 6 to 20 - Moderate risk; 20+ - Significant risk
Genetic Drug interaction Anticholinergic burdenLifestyle ADR (Black box) Beers criteria
DUTOPROL (Metoprolol…
Kazano (Alogliptin)
Adderall (Amphetamin…
Aspirin
Delone, Lasix (Furosem…
Coumadin, Jantoven (W…
BuSpar (Buspirone)
0 10025 50 75 125
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 2 of 28
Powered by:

Current Regimen Risk Detail
Beers criteriaAnticholinergic burdenADRDrug InteractionLifestyleGeneticSevere Risks
Genetic warning for DUTOPROL (Metoprolol Succinate)
Individuals with intermediate metabolizer status have increased risk of adverse drug reactions. For heart failure (indication):
select alternative drug (e.g. bisoprolol, carvedilol) or reduce dose by 50%. For other indications: be alert to adverse drug
events (e.g. bradycardia, cold extremities) or select alternative drug (e.g. atenolol, bisoprolol).
Kazano (Alogliptin) has its pharmacodynamic parameters altered by DUTOPROL (Metoprolol Succinate)
• use combination with caution
• monitor blood glucose concentration and for changes in glycemic control
Patients receiving beta-blockers and antidiabetic agents concomitantly should be closely monitored for an inappropriate
response. While beta-blockers may have negative effects on glycemic control, they reduce the risk of cardiovascular disease
and stroke.
American Geriatric Society guidelines
The following products appear on the American Geriatric Society's Beers Criteria for Potentially Inappropriate Medication
Use in Older Adults:
• Amphetamine Aspartate 7.5mg, Amphetamine Sulfate 7.5mg, Dextroamphetamine Saccharate 7.5mg, Dextroamphetamine Sulfate 7.5mg Oral
tablet
• Aspirin 325mg Oral tablet
• Buspirone Hydrochloride 10mg Oral tablet
• Furosemide 20mg Oral tablet
• Metoprolol Succinate 100mg, Hydrochlorothiazide 12.5mg Oral tablet, extended release
Strong regimen anticholinergic burden
The cumulative effect of taking multiple medicines with anticholinergic properties termed as anticholinergic burden can
adversely impact cognition, physical function and increase the risk of mortality.
Beers criteriaAnticholinergic burdenADRDrug InteractionLifestyleGeneticMajor Risks
Aspirin with Alcohol
• avoid combination unless benefit outweighs potential risk
Concomitant ingestion of ethanol with salicylates, especially aspirin, ASA, increases the risk of developing gastric irritation
and GI mucosal bleeding. Ethanol and salicylates are mucosal irritants and aspirin decreases platelet aggregation. Routine
ingestion of ethanol and aspirin can cause significant GI bleeding, which may or may not be overt. Even occasional
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 3 of 28
Powered by:
concomitant use of salicylates and ethanol should be avoided. Chronic alcoholism is often associated with
hypoprothrombinemia and this condition increases the risk of salicylate-induced bleeding. Patients should be warned
regarding the potential for increased risk of GI bleeding if alcohol-containing beverages are taken concurrently with
salicylates
Adderall (Amphetamine Aspartate) with Alcohol
• avoid combination unless benefit outweighs potential risk
Amphetamines do not change the pharmacokinetics of ethanol nor do they relieve cognitive impairment that results from
ethanol intoxication, even though subjective improvements in motor performance have been noted on concomitant ingestion
by patients. Ethanol containing beverages generally should be avoided.
BuSpar (Buspirone) with Alcohol
• avoid combination unless benefit outweighs potential risk
• warn against driving or operating machinery or performing other hazardous tasks until drug effects are known
• monitor for an increase in CNS/respiratory depression
Alcohol is associated with CNS depression. The combined use of alcohol and CNS depressants can lead to additive CNS
depression, which could be dangerous in tasks requiring mental alertness and fatal in overdose. Alcohol taken with other CNS
depressants can lead to additive respiratory depression, hypotension, profound sedation, or coma. Consider the patient's use
of alcohol or illicit drugs when prescribing CNS depressant medications. In many cases, the patient should receive a lower
dose of the CNS depressant initially if the patient is not likely to be compliant with avoiding alcohol.
DUTOPROL (Metoprolol Succinate) effectiveness may be reduced due to aggravation of underlying condition by Adderall(Amphetamine Aspartate)
• use combination with caution
• consider alternative drug therapy
• monitor for altered clinical response to drug therapy
• monitor blood pressure
Amphetamines increase both systolic and diastolic blood pressure and may counteract the activity of some antihypertensive
agents. Close monitoring of blood pressure or the selection of alternative therapeutic agents may be needed.
Adderall (Amphetamine Aspartate) aggravate underlying condition, thus reducing effectiveness of Delone, Lasix(Furosemide)
• use combination with caution
• monitor blood pressure
• monitor heart rate
Amphetamines increase both systolic and diastolic blood pressure and may counteract the activity of some antihypertensive
agents, such as loop diuretics.
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 4 of 28
Powered by:
DUTOPROL (Metoprolol Succinate) may have a mutually antagonistic effect with Adderall (Amphetamine Aspartate)
• use combination with caution
• monitor for altered clinical response to drug therapy
• monitor blood pressure
Concurrent use of beta-blocking agents with sympathomimetics can result in mutual antagonism of desired therapeutic
effects of either agent and/or can cause unopposed alpha pharmacodynamic effects.
Coumadin, Jantoven (Warfarin) causes additive effects that may result in increased risk of bleeding with Aspirin
• avoid combination unless benefit outweighs potential risk
• monitor for evidence of bleeding
Co-use may increased the risk of bleeding.
Beers criteriaAnticholinergic burdenADRDrug InteractionLifestyleGeneticModerate Risks
Delone, Lasix (Furosemide) with Alcohol
• use combination with caution
• monitor blood pressure
Ethanol, since it also possesses diuretic properties, should be taken in small quantities in patients receiving loop diuretics. The
diuretic properties may be additive, leading to dehydration in some patients. In addition, ethanol has hypotensive properties
which can enhance the antihypertensive effects of diuretics.
Coumadin, Jantoven (Warfarin) with Alcohol
• monitor for evidence of bleeding
• monitor international normalized ratio (INR) or prothrombin time
In controlled studies of patients or healthy subjects anticoagulated with warfarin, small to moderate amounts of wine do not
alter INR values or warfarin levels. However, acute intoxication resulting from large amounts of ethanol may enhance the
hypoprothrombinemic response to oral anticoagulants due to inhibition of warfarin's metabolism.
DUTOPROL (Metoprolol Succinate) with Alcohol
• use combination with caution
Ethanol interacts with antihypertensive agents by potentiating their hypotensive effect.
Kazano (Alogliptin) with Alcohol
• use combination with caution
• monitor blood glucose concentration and for changes in glycemic control
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 5 of 28
Powered by:
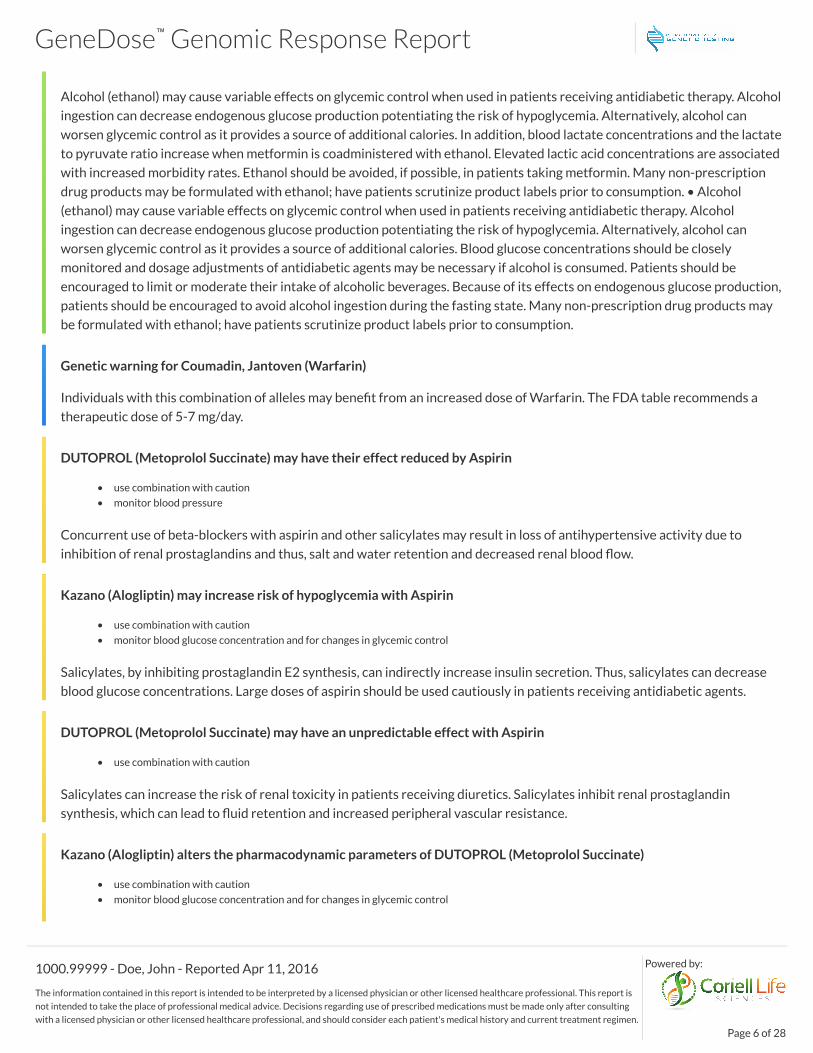
Alcohol (ethanol) may cause variable effects on glycemic control when used in patients receiving antidiabetic therapy. Alcohol
ingestion can decrease endogenous glucose production potentiating the risk of hypoglycemia. Alternatively, alcohol can
worsen glycemic control as it provides a source of additional calories. In addition, blood lactate concentrations and the lactate
to pyruvate ratio increase when metformin is coadministered with ethanol. Elevated lactic acid concentrations are associated
with increased morbidity rates. Ethanol should be avoided, if possible, in patients taking metformin. Many non-prescription
drug products may be formulated with ethanol; have patients scrutinize product labels prior to consumption. • Alcohol
(ethanol) may cause variable effects on glycemic control when used in patients receiving antidiabetic therapy. Alcohol
ingestion can decrease endogenous glucose production potentiating the risk of hypoglycemia. Alternatively, alcohol can
worsen glycemic control as it provides a source of additional calories. Blood glucose concentrations should be closely
monitored and dosage adjustments of antidiabetic agents may be necessary if alcohol is consumed. Patients should be
encouraged to limit or moderate their intake of alcoholic beverages. Because of its effects on endogenous glucose production,
patients should be encouraged to avoid alcohol ingestion during the fasting state. Many non-prescription drug products may
be formulated with ethanol; have patients scrutinize product labels prior to consumption.
Genetic warning for Coumadin, Jantoven (Warfarin)
Individuals with this combination of alleles may benefit from an increased dose of Warfarin. The FDA table recommends a
therapeutic dose of 5-7 mg/day.
DUTOPROL (Metoprolol Succinate) may have their effect reduced by Aspirin
• use combination with caution
• monitor blood pressure
Concurrent use of beta-blockers with aspirin and other salicylates may result in loss of antihypertensive activity due to
inhibition of renal prostaglandins and thus, salt and water retention and decreased renal blood flow.
Kazano (Alogliptin) may increase risk of hypoglycemia with Aspirin
• use combination with caution
• monitor blood glucose concentration and for changes in glycemic control
Salicylates, by inhibiting prostaglandin E2 synthesis, can indirectly increase insulin secretion. Thus, salicylates can decrease
blood glucose concentrations. Large doses of aspirin should be used cautiously in patients receiving antidiabetic agents.
DUTOPROL (Metoprolol Succinate) may have an unpredictable effect with Aspirin
• use combination with caution
Salicylates can increase the risk of renal toxicity in patients receiving diuretics. Salicylates inhibit renal prostaglandin
synthesis, which can lead to fluid retention and increased peripheral vascular resistance.
Kazano (Alogliptin) alters the pharmacodynamic parameters of DUTOPROL (Metoprolol Succinate)
• use combination with caution
• monitor blood glucose concentration and for changes in glycemic control
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 6 of 28
Powered by:

Thiazide diuretics can decrease insulin sensitivity thereby leading to glucose intolerance and hyperglycemia. Because of this,
a potential pharmacodynamic interaction exists between thiazide diuretics and antidiabetic agents.
Kazano (Alogliptin) has its effect increased by Adderall (Amphetamine Aspartate)
• use combination with caution
• monitor blood pressure
Amphetamines may potentiate the actions of some antidiabetic agents. As long as blood glucose is carefully monitored to
avoid hypoglycemia, it appears that amphetamines can be used concurrently.
DUTOPROL (Metoprolol Succinate) may have an additive effect with Delone, Lasix (Furosemide)
• monitor renal function
• monitor blood pressure
• monitor heart rate
• monitor serum potassium
• monitor serum electrolytes
Use cautiously and with monitoring of renal function, blood pressure, cardiac status, electrolytes (especially potassium), and
monitor the clinical response for the condition treated.
Kazano (Alogliptin) has its pharmacodynamic parameters altered by Aspirin
• use combination with caution
• monitor blood glucose concentration and for changes in glycemic control
Large doses of salicylates may enhance hypoglycemia in diabetic patients. If these agents are administered or discontinued in
patients receiving oral antidiabetic agents, patients should be monitored for hypoglycemia or loss of blood glucose control.
Aspirin may reduce effect of Delone, Lasix (Furosemide)
• use combination with caution
• monitor for altered clinical response to drug therapy
• monitor patient clinically
Salicylates may decrease the diuretic, natriuretic, and antihypertensive actions of diuretics, possibly through inhibition of
renal prostaglandin synthesis. Patients receiving loop diuretics and salicylates should be monitored.
Kazano (Alogliptin) has its pharmacodynamic parameters altered by DUTOPROL (Metoprolol Succinate)
• use combination with caution
• monitor blood glucose concentration and for changes in glycemic control
Thiazide diuretics can decrease insulin sensitivity thereby leading to glucose intolerance and hyperglycemia.Diuretic-induced
hypokalemia may also lead to hyperglycemia. Because of this, a potential pharmacodynamic interaction exists. Monitor
closely.
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 7 of 28
Powered by:

Kazano (Alogliptin) effectiveness may be reduced due to aggravation of underlying condition by Adderall (AmphetamineAspartate)
• use combination with caution
• monitor blood glucose concentration and for changes in glycemic control
Patients receiving alogliptin should be closely monitored for loss of diabetic control when therapy with sympathomimetic
agents is instituted.
Kazano (Alogliptin) has its pharmacodynamic parameters altered by DUTOPROL (Metoprolol Succinate)
• use combination with caution
• monitor patient clinically
• monitor blood glucose concentration and for changes in glycemic control
Beta-blockers can prolong hypoglycemia by interfering with the mobilization of glycogen stores or can promote
hyperglycemia. Also, beta-blockers can blunt some of the physiologic symptoms of hypoglycemia, such as tremors and
tachycardia.
Beers criteriaAnticholinergic burdenADRDrug InteractionLifestyleGeneticMinor Risks
Kazano (Alogliptin) has its effect reduced by Delone, Lasix (Furosemide)
• use combination with caution
• monitor patient clinically
• monitor blood glucose concentration and for changes in glycemic control
Furosemide may cause hyperglycemia and glycosuria in patients with diabetes mellitus, probably due to diuretic-induced
hypokalemia.
DUTOPROL (Metoprolol Succinate) has an unpredictable effect with Coumadin, Jantoven (Warfarin)
• monitor patient clinically
• monitor international normalized ratio (INR) or prothrombin time
Per the prescribing information for warfarin sodium (Coumadin), use of diuretics (e.g., hydrochlorothiazide) with warfarin
may increase or decrease PT/INR response. Monitor accordingly with drug initation, adjustment, or discontinuation.
Coumadin, Jantoven (Warfarin) has an unpredictable effect with Delone, Lasix (Furosemide)
• monitor patient clinically
• monitor international normalized ratio (INR) or prothrombin time
Per the prescribing information for warfarin sodium (Coumadin), the use of diuretics (e.g., furosemide) with warfarin is
associated with increases and decreases in PT/INR response. Monitor accordingly with drug initation, adjustment, or
discontinuation.
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 8 of 28
Powered by:

Kazano (Alogliptin) has its effect reduced by Delone, Lasix (Furosemide)
• use combination with caution
• monitor blood glucose concentration and for changes in glycemic control
Furosemide may cause hyperglycemia and glycosuria in patients with diabetes mellitus. Because of this, a potential
pharmacodynamic interaction exists between furosemide and all antidiabetic agents, including alogliptin.
BuSpar (Buspirone) may have its serum concentration increased by Aspirin
• use combination with caution
• monitor for signs of drug toxicity
In vitro studies showed that therapeutic levels of aspirin, ASA increased the plasma concentrations of free buspirone by 23%
through plasma protein binding displacement. In vivo interaction studies with these drugs have not been performed.
DUTOPROL (Metoprolol Succinate) increases effect of Coumadin, Jantoven (Warfarin)
• monitor patient clinically
• monitor international normalized ratio (INR) or prothrombin time
Concomitant use of beta-blockers and warfarin may result in elevations in PT/INR response; patients receiving warfarin
should be monitored for changes in the INR when beta-blockers are initiated or discontinued, or if the dosage is changed.
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 9 of 28
Powered by:

Thrombosis Profile
Tested Genes (Alleles) Genotype Predicted Phenotype Clinical Guidance
Prothrombin (F2) Normal
Factor V Leiden Normal
MTHFR (A1298C) Normal
MTHFR (C677T) Homozygous
variant
Normal risk expected based on the
patient’s genotype.
The absence of these variant alleles of
Prothrombin (Factor II) and Factor V
Leiden suggests that the patient does not
have the elevated risk of thrombosis
associated with these genetic markers.
General Description
Genetic analyses of three genes (four alleles) considered to increase the risk for venous thrombosis were performed using molecular genetic
techniques. The presence of the Prothrombin (Factor 2) gene allele 20210A and Factor V Leiden allele 1691A are risk factors for venous
thrombosis. This risk may be further increased by the use of estrogen therapy, oral contraceptives, pregnancy, and surgery.
Patients who are homozygous for MTHFR 677T or MTHFR 1298C may have a further increased risk for venous thrombosis if they also possess
the Factor V Leiden 1691A allele. However the MTHFR alleles alone do not predict a significant risk for venous thrombosis.
References and Useful Information:
• Factor V Leiden Working Group; ACMG Laboratory Quality Assurance Molecular Subcommittee of the ACMG Laboratory Quality Assurance
Committee AMERICAN COLLEGE OF MEDICAL GENETICS; Standards and Guidelines for Clinical Genetics Laboratories; 2006 Edition
◦ Middeldorp S, Henkens CM, Koopman MM, van Pampus ECM,Hamulyák K, van der Meer J, Prins MH, Büller HR. The incidence of venous
thromboembolism in family members of patients with factor V Leiden mutation and venous thrombosis. Ann Intern Med 1998;128:15-20.
◦ Vandenbroucke JP, Koster T, Briet E, Reitsma PH, Bertina RM, Rosendaal FR. Increased risk of venous thrombosis in oral contraceptive users
who are carriers of factor V Leiden mutation. Lancet 1994;344:1453-1457.
◦ Rosendaal FR, Koster T, Vandenbroucke JP, Reitsma PH. High risk of thrombosis in patients homozygous for factor V Leiden (activated
protein C resistance). Blood 1995;85(6):1504-1508.
◦ Reich LM, Bower M, Key NS. Role of the geneticist in testing and counseling for inherited thrombophilia. Genet Med 2003;5:133-143.
◦ Tosetto A, Rodeghiero F, Martinelli I, De Stefano V, Missiaglia E, Chiusolo P, Mannucci PM. Additional genetic risk factors for venous
thromboembolism in carriers of the factor V Leiden mutation. Br J Haematol 1998;103:871-876.
◦ De Stefano V, Martinelli I, Mannucci PM, Paciaroni K, Chiusolo P, Casorelli I, Rossi E, Leone G. The risk of recurrent deep venous thrombosis
among heterozygous carriers of both factor V Leiden and the G20210A prothrombin mutation. N Engl J Med 1999;341:801-806.
• M. Adams, P.D. Smith, D. Martin, J.R. Thompson, D. Lodwick, N.J. Samani. Genetic analysis of thermolabile methylenetetrahydrofolate reductase as a risk
factor for myocardial infarction. QJM. 1996 Jun;89(6):437-44.
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 10 of 28
Powered by:
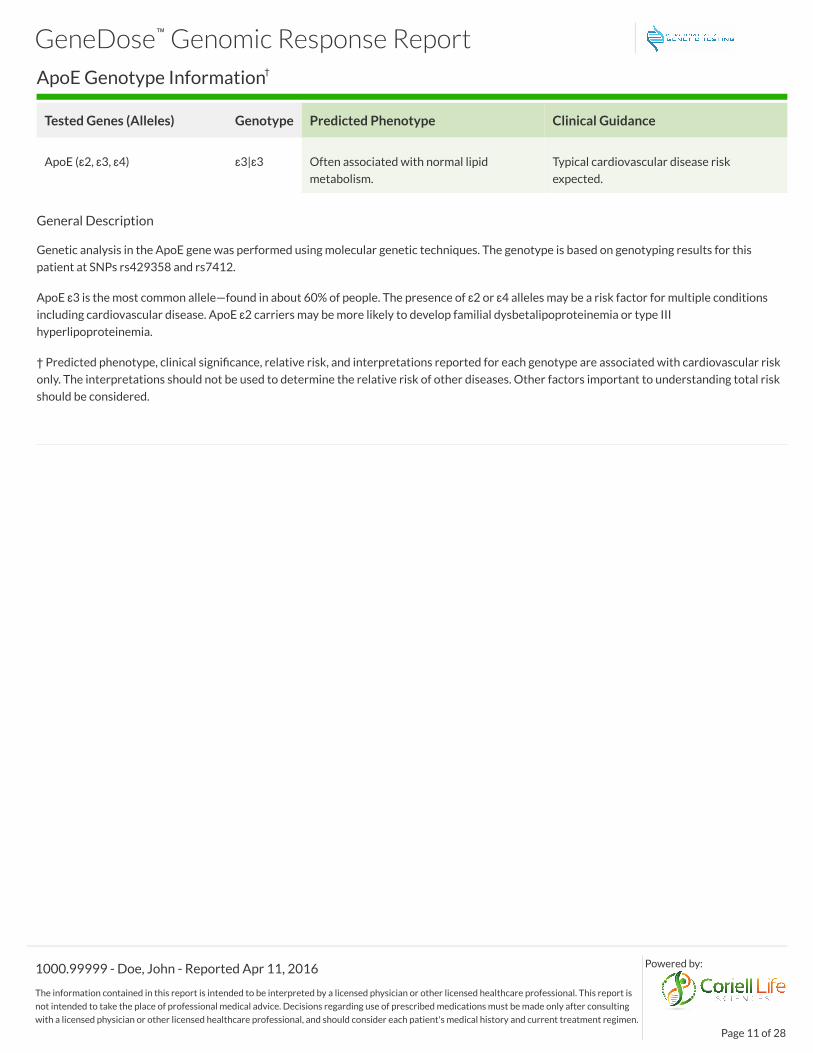
ApoE Genotype Information†
Tested Genes (Alleles) Genotype Predicted Phenotype Clinical Guidance
ApoE (ɛ2, ɛ3, ɛ4) ɛ3|ɛ3 Often associated with normal lipid
metabolism.
Typical cardiovascular disease risk
expected.
General Description
Genetic analysis in the ApoE gene was performed using molecular genetic techniques. The genotype is based on genotyping results for this
patient at SNPs rs429358 and rs7412.
ApoE ɛ3 is the most common allele—found in about 60% of people. The presence of ɛ2 or ɛ4 alleles may be a risk factor for multiple conditions
including cardiovascular disease. ApoE ɛ2 carriers may be more likely to develop familial dysbetalipoproteinemia or type III
hyperlipoproteinemia.
† Predicted phenotype, clinical significance, relative risk, and interpretations reported for each genotype are associated with cardiovascular risk
only. The interpretations should not be used to determine the relative risk of other diseases. Other factors important to understanding total risk
should be considered.
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 11 of 28
Powered by:

Medication Summary (more alternatives discoverable at GeneDose™ LIVE)Secured URL: https://app.genedose.com/?token=dXXHXXF54
Cardiac
Therapeutic Class Standard Precautions Caution / Info Change recommended
Antiarrhythmics Flecainide
Propafenone
Anticoagulants Acenocoumarol Warfarin
Anticonvulsants Phenytoin
Antiplatelet Agents Clopidogrel Ticagrelor
Beta Blockers Carvedilol Metoprolol
Statins Atorvastatin
Simvastatin
Gastroenterology
Therapeutic Class Standard Precautions Caution / Info Change recommended
Antidepressants Mirtazapine
Trazodone
Amitriptyline
Clomipramine
Desipramine
Doxepin
Nortriptyline
Immunosuppressants Cyclosporine
Nonsteroidal Anti-
Inflamatory Drugs
(NSAIDs)
Celecoxib
Proton Pump
Inhibitors (PPIs)
Dexlansoprazole
Esomeprazole
Lansoprazole
Omeprazole
Pantoprazole
Rabeprazole
Selective Serotonin
Reuptake Inhibitors
(SSRIs)
Citalopram / Escitalopram Paroxetine
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 12 of 28
Powered by:

Infectious Disease
Therapeutic Class Standard Precautions Caution / Info Change recommended
Antifungals Ketoconazole
Voriconazole
Pain
Therapeutic Class Standard Precautions Caution / Info Change recommended
Anticonvulsants Clobazam
Phenytoin
Antidepressants Duloxetine
Flupenthixol
Mirtazapine
Moclobemide
Trazodone
Amitriptyline
Clomipramine
Desipramine
Doxepin
Nortriptyline
Protriptyline
Venlafaxine
Vortioxetine
Antipsychotics Olanzapine
Immunosuppressants Cyclosporine Tacrolimus
Muscle Relaxants Carisoprodol
Nonsteroidal Anti-
Inflamatory Drugs
(NSAIDs)
Celecoxib
Diclofenac
Flurbiprofen
Meloxicam
Opioids Buprenorphine Codeine
Oxycodone
Tramadol
Selective Serotonin
Reuptake Inhibitors
(SSRIs)
Citalopram / Escitalopram
Sertraline
Fluoxetine
Paroxetine
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 13 of 28
Powered by:
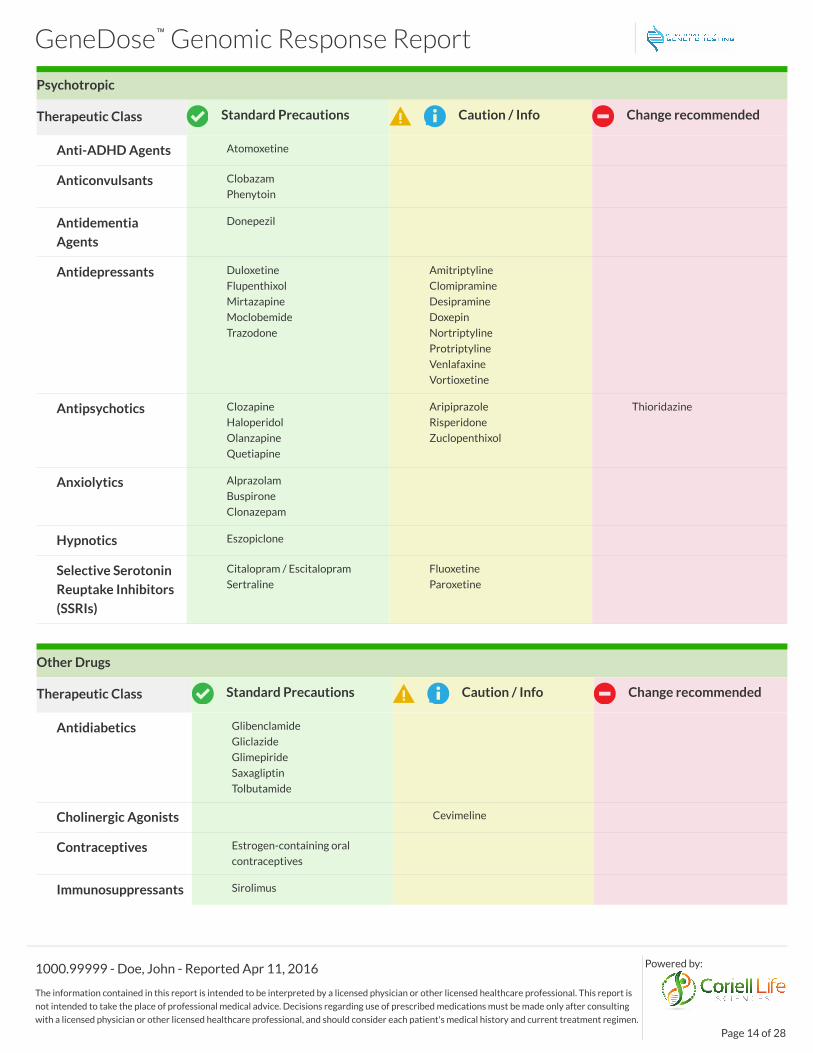
Psychotropic
Therapeutic Class Standard Precautions Caution / Info Change recommended
Anti-ADHD Agents Atomoxetine
Anticonvulsants Clobazam
Phenytoin
Antidementia
Agents
Donepezil
Antidepressants Duloxetine
Flupenthixol
Mirtazapine
Moclobemide
Trazodone
Amitriptyline
Clomipramine
Desipramine
Doxepin
Nortriptyline
Protriptyline
Venlafaxine
Vortioxetine
Antipsychotics Clozapine
Haloperidol
Olanzapine
Quetiapine
Aripiprazole
Risperidone
Zuclopenthixol
Thioridazine
Anxiolytics Alprazolam
Buspirone
Clonazepam
Hypnotics Eszopiclone
Selective Serotonin
Reuptake Inhibitors
(SSRIs)
Citalopram / Escitalopram
Sertraline
Fluoxetine
Paroxetine
Other Drugs
Therapeutic Class Standard Precautions Caution / Info Change recommended
Antidiabetics Glibenclamide
Gliclazide
Glimepiride
Saxagliptin
Tolbutamide
Cholinergic Agonists Cevimeline
Contraceptives Estrogen-containing oral
contraceptives
Immunosuppressants Sirolimus
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 14 of 28
Powered by:

Legend Clinical Evidence Level
Typical response is expected Additional information available Strong
Change recommended Response is uncertain Moderate
Consider alternative therapy Emerging
Medication Report Details (by therapeutic class)
Drug Finding Recommendation Concern Evidence Reference
Anti-ADHD Agents
Atomoxetine
(Strattera)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
8, 22
Antiarrhythmics
Flecainide
(Tambocor)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have the potential for decreased
elimination. Consider reducing dose by
25%; record ECG; monitor plasma
concentration.
ADR 8
Propafenone
(Rythmol)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have decreased metabolism to less
active compounds; the resultant increased
plasma concentrations may increase the
risk proarrhythmia, exaggerated beta-
adrenergic blocking activity, and other
adverse events. Adjust dose in response to
plasma concentration and record ECG or
select alternative drug (e.g. sotalol,
disopyramide, quinidine, amiodarone).
ADR 8, 27
Anticoagulants
Acenocoumarol
(Sintrom, Acitrom)
CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Warfarin
(Coumadin)
Multigenic:
VKORC1, CYP2C9:
Two alleles showing normal
activity.; Extensive
metabolizer. Two alleles
showing normal activity.
Individuals with this combination of alleles
may benefit from an increased dose of
Warfarin. The FDA table recommends a
therapeutic dose of 5-7 mg/day.
74
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 15 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Anticonvulsants
Clobazam
(Onfi)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
37
Phenytoin
(Dilantin)
CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Antidementia Agents
Donepezil CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
38
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 16 of 28
Powered by:
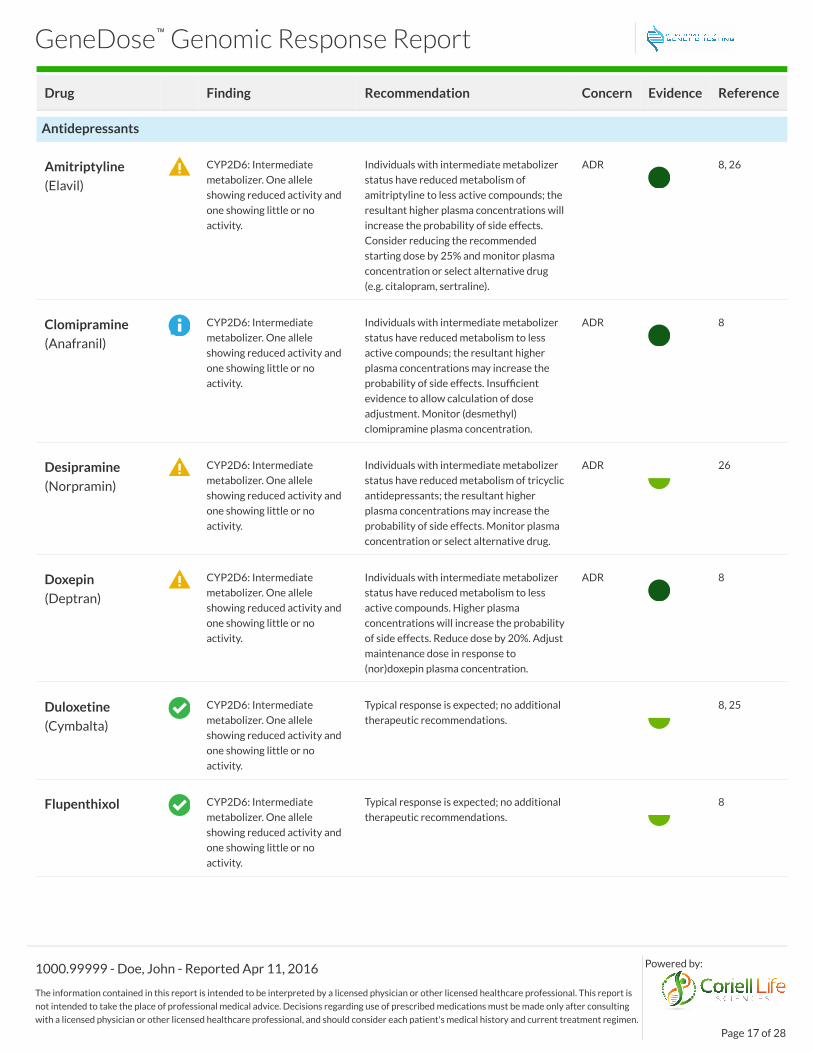
Drug Finding Recommendation Concern Evidence Reference
Antidepressants
Amitriptyline
(Elavil)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have reduced metabolism of
amitriptyline to less active compounds; the
resultant higher plasma concentrations will
increase the probability of side effects.
Consider reducing the recommended
starting dose by 25% and monitor plasma
concentration or select alternative drug
(e.g. citalopram, sertraline).
ADR 8, 26
Clomipramine
(Anafranil)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have reduced metabolism to less
active compounds; the resultant higher
plasma concentrations may increase the
probability of side effects. Insufficient
evidence to allow calculation of dose
adjustment. Monitor (desmethyl)
clomipramine plasma concentration.
ADR 8
Desipramine
(Norpramin)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have reduced metabolism of tricyclic
antidepressants; the resultant higher
plasma concentrations may increase the
probability of side effects. Monitor plasma
concentration or select alternative drug.
ADR 26
Doxepin
(Deptran)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have reduced metabolism to less
active compounds. Higher plasma
concentrations will increase the probability
of side effects. Reduce dose by 20%. Adjust
maintenance dose in response to
(nor)doxepin plasma concentration.
ADR 8
Duloxetine
(Cymbalta)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
8, 25
Flupenthixol CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
8
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 17 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Imipramine
(Tofranil)
Multigenic:
CYP2C19, CYP2D6:
Extensive metabolizer. Two
alleles showing normal
activity. Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Multiple results from uncorrelated genes.
CYP2C19: Typical response is expected; no
additional therapeutic recommendations.
CYP2D6: Recommended dosage
adjustment and additional monitoring
suggested
8
Mirtazapine CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Moclobemide CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Nortriptyline
(Pamelor)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have reduced metabolism of
tricyclics to less active compounds when
compared to extensive metabolizers; the
resultant higher plasma concentrations will
increase the probability of side effects.
Consider reducing the dose by 40% and
monitor nortriptyline
10-hydroxynortriptyline plasma
concentrations.
ADR 8, 26
Protriptyline
(Vivactil)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have reduced metabolism of tricyclic
antidepressants; the resultant higher
plasma concentrations may increase the
probability of side effects. Monitor plasma
concentration or select alternative drug.
ADR 52
Trazodone
(Oleptro, Desyrel)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
67
Venlafaxine
(Effexor)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Insufficient evidence to allow calculation of
dose adjustment. Consider selecting
alternative drug (e.g. citalopram, sertraline)
or adjust dose to clinical response and
monitor (O-desmethyl) venlafaxine plasma
concentration.
8
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 18 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Vortioxetine
(Brintellix)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status may be at an increased risk of
adverse drug reactions due to reduced
metabolic clearance and high plasma
concentrations of the active compound.
Consider reducing the dose.
ADR 73
Antidiabetics
Glibenclamide
(Glyburide)
CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Gliclazide CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Glimepiride CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Saxagliptin
(Onglyza)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
71
Tolbutamide
(Orinase)
CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Antifungals
Ketoconazole
(Nizoral)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
72
Voriconazole CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8, 21
Antiplatelet Agents
Clopidogrel
(Plavix)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Ticagrelor
(Brilinta)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
ADR &
Efficacy
51
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 19 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Antipsychotics
Aripiprazole
(Abilify)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Intermediate metabolizers are at uncertain
risk of adverse drug reaction. However,
note that for individuals with poor
metabolizer status it is recommended to
reduce the maximum dose to 10 mg/day
(67% of the maximum recommended daily
dose).
ADR 8, 58
Clozapine CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
8, 24
Haloperidol
(Haldol)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Olanzapine
(Zalasta, Zyprexa)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Quetiapine
(Seroquel)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
61
Risperidone
(Risperdal)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Insufficient evidence to allow calculation of
dose adjustment. Consider selecting
alternative drug (e.g. quetiapine,
olanzapine, clozapine) or being extra alert
to adverse drug events and adjusting dose
to clinical response.
ADR 8, 28
Thioridazine CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status are at an increased risk of serious
adverse drug reactions due to elevated
levels of thioridazine. Select alternative
drug.
ADR 35
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 20 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Zuclopenthixol CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with poor metabolizer status
have decreased metabolism to less active
compounds; the resultant increased plasma
concentrations may increase the risk of
adverse drug reactions. Reduce the
standard dose by 25% or select an
alternative drug (flupenthixol, quetiapine,
olanzapine, clozapine).
ADR 8
Anxiolytics
Alprazolam
(Xanax, Niravam)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
68
Buspirone
(Buspar)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
69
Clonazepam
(Klonopin)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
70
Beta Blockers
Carvedilol
(Coreg)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Typical response is expected; no additional
therapeutic recommendations.
8, 23
Metoprolol
(Lopressor)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have increased risk of adverse drug
reactions. For heart failure (indication):
select alternative drug (e.g. bisoprolol,
carvedilol) or reduce dose by 50%. For
other indications: be alert to adverse drug
events (e.g. bradycardia, cold extremities)
or select alternative drug (e.g. atenolol,
bisoprolol).
ADR 8
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 21 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Cholinergic Agonists
Cevimeline
(Evoxac)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status may be at an increased risk of
adverse drug reactions due to reduced
metabolic clearance and abnormally high
plasma concentrations of the active
compound. Insufficient evidence to allow
calculation of dose adjustment. Cevimeline
should be administered with caution.
ADR 60
Contraceptives
Estrogen-
containing oral
contraceptives
F5: Two wild-type alleles. Typical response is expected; no additional
therapeutic recommendations.
8
Hypnotics
Eszopiclone
(Lunesta)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
66
Immunosuppressants
Cyclosporine
(Gengraf, Neoral)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
63
Sirolimus
(Rapamune)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
64
Tacrolimus
(Prograf, Hecoria)
CYP3A5: *3|*3 Individuals with poor metabolizer status
have higher dose-adjusted trough
concentrations of tacrolimus; the resultant
increased concentrations may increase the
probability of pharmacotherapy success.
Consider initiating therapy with the
recommended starting dose. In liver
transplant patients, donor genotype should
be considered as well as the recipient's.
76
Muscle Relaxants
Carisoprodol
(Soma)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
33, 78
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 22 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Non-drug
ApoE ApoE: Often associated with
normal lipid metabolism.
Typical cardiovascular disease risk
expected.
Nonsteroidal Anti-Inflamatory Drugs (NSAIDs)
Celecoxib
(Celebrex)
CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
1, 19
Diclofenac
(Cataflam)
CYP2C9:rs1057910: Two
alleles showing normal
activity.
Typical response is expected; no additional
therapeutic recommendations.
29
Flurbiprofen
(Ocufen)
CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
30
Meloxicam
(Mobic)
CYP2C9: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
32
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 23 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Opioids
Buprenorphine
(Butrans,
Buprenex)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
62
Codeine CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
For analgesia, select alternative drug (e.g.
acetaminophen, NSAID, morphine; not
tramadol or oxycodone) or be alert to
symptoms of insufficient pain relief. For
cough, there are no data on the effect of
CYP2D6 genotype or phenotype on the
antitussive effect of codeine.
Efficacy 8
Oxycodone
(Oxycontin)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status are at risk of potentially reduced
efficacy; consider alternative therapy.
Insufficient evidence to allow calculation of
dose adjustment. Select alternative drug
(not tramadol or codeine) or be alert to
symptoms of insufficient pain relief.
Efficacy 8
Tramadol
(Ultracet, Ultram)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status have decreased metabolism to more
active compounds; the resultant decreased
plasma concentrations may increase the
probability of pharmacotherapy failure.
Consider dose increase. If response is still
inadequate; select alternative drug (not
oxycodone or codeine) or be alert to
symptoms of insufficient pain relief.
Efficacy 8
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 24 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Proton Pump Inhibitors (PPIs)
Dexlansoprazole
(Kapidex,
Dexilant)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
11
Esomeprazole
(Nexium)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
12
Lansoprazole
(Prevacid)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
5
Omeprazole
(Prilosec, Zegerid)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
4
Pantoprazole
(Protonix)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
6
Rabeprazole
(Aciphex)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
7
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 25 of 28
Powered by:

Drug Finding Recommendation Concern Evidence Reference
Selective Serotonin Reuptake Inhibitors (SSRIs)
Citalopram /
Escitalopram
(Celexa, Lexapro)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8, 20
Fluoxetine
(Prozac)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals taking fluoxetine should be alert
to concomitant use of drugs metabolized by
CYP2D6. For a more in-depth
recommendation for individuals taking
fluoxetine, please visit this individual's
GeneDose Live profile. Briefly, fluoxetine is
a potent inhibitor of CYP2D6 enzyme
pathway. Fluoxetine inhibits the activity of
CYP2D6, and may make individuals with
normal CYP2D6 metabolic activity
resemble a poor metabolizer.
Coadministration of fluoxetine with other
drugs that are metabolized by CYP2D6,
including certain antidepressants (e.g.
TCAs), antipsychotics (e.g. phenothiazines
and most atypicals), and antiarrhythmics
(e.g. propafenone, flecainide, and others)
should be approached with caution.
ADR &
Efficacy
39
Paroxetine
(Paxil)
CYP2D6: Intermediate
metabolizer. One allele
showing reduced activity and
one showing little or no
activity.
Individuals with intermediate metabolizer
status may have increased plasma
concentrations/ decreased clearance of
paroxetine. However, an association with
treatment response or severity of side
effects is not conclusive.
ADR 8
Sertraline
(Zoloft)
CYP2C19: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
8
Statins
Atorvastatin
(Lipitor, Caduet)
CYP3A4: Extensive
metabolizer. Two alleles
showing normal activity.
Typical response is expected; no additional
therapeutic recommendations.
54, 55
Simvastatin
(Zocor)
SLCO1B1: Normal liver
uptake activity.
Individuals with normal SLCO1B1 liver
uptake activity are expected to have a
typical response to a standard dose of
simvastatin.
3
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 26 of 28
Powered by:

References
Available at GeneDose.com or by request.
Clinical Evidence Levels
Strong
• Includes gene-drug pairs approved by the Coriell Institute for Medical Research Pharmacogenomics Advisory Group.
• Includes gene-drug pairs supported by multiple studies documenting consistent effects of specific genetic variant(s) on clinical outcomes.
• Includes gene-drug pairs approved by the Dutch Pharmacogenetics Working Group (DPWG) and/or guidelines published in Clinical Pharmacology and
Therapeutics by the Clinical Pharmacogenetics Implementation Consortium (CPIC).
Moderate
• Includes gene-drug pairs supported by pharmacokinetic, pharmacodynamic, or molecular/cellular functional studies showing consistent effects of
genetic variant(s).
• Includes Drug product information (e.g. This interpretation is based on guidance available in the FDA (Food and Drug Administration) drug label for
ABILIFY® (10/2013).
• Includes gene-drug pairs for which potential clinical outcomes are inferred from similar gene-drug interactions approved by the Dutch
Pharmacogenetics Working Group (DPWG), and/or guidelines published in Clinical Pharmacology and Therapeutics by the Clinical Pharmacogenetics
Implementation Consortium (CPIC), and/or pharmacogenomic reports and submission from the Coriell Institute for Medical Research.
Emerging
• Includes gene-drug pairs supported by published studies of the drug, related drug, or a probing compound of interest involving limited data and/or
inconsistent findings.
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 27 of 28
Powered by:
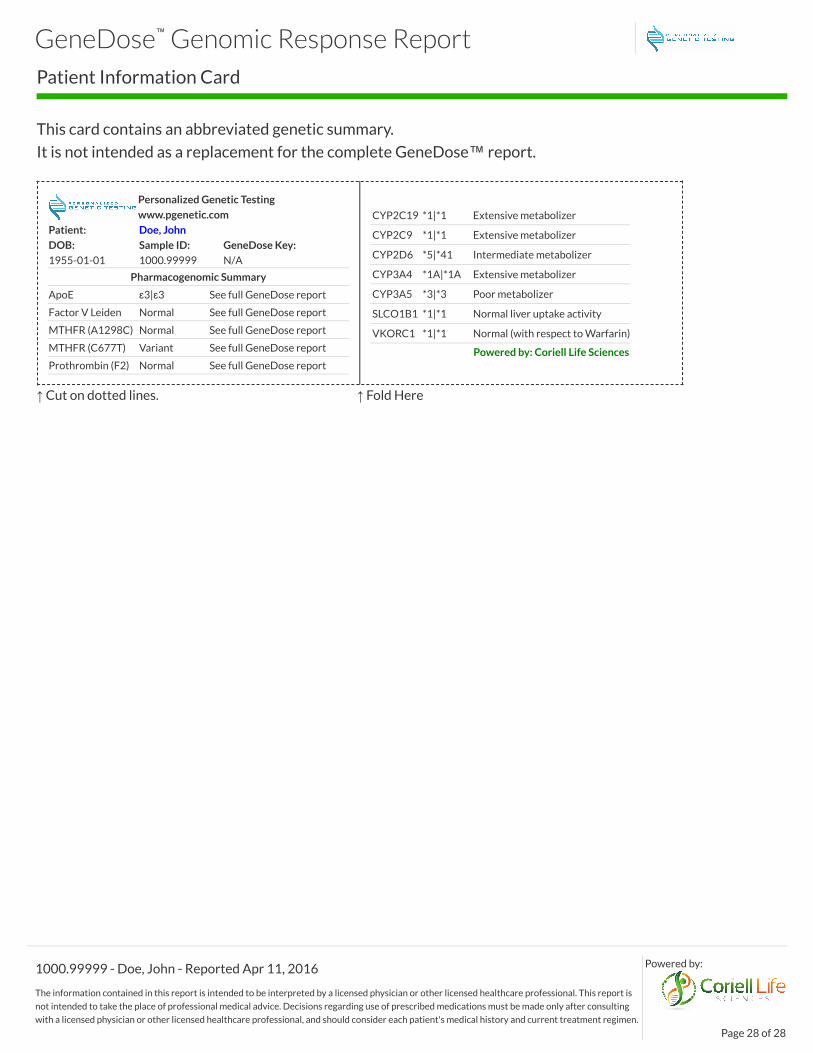
Patient Information Card
This card contains an abbreviated genetic summary.
It is not intended as a replacement for the complete GeneDose™ report.
Personalized Genetic Testing
www.pgenetic.com
Patient: Doe, John
DOB: Sample ID: GeneDose Key:
1955-01-01 1000.99999 N/A
Pharmacogenomic Summary
ApoE ɛ3|ɛ3 See full GeneDose report
Factor V Leiden Normal See full GeneDose report
MTHFR (A1298C) Normal See full GeneDose report
MTHFR (C677T) Variant See full GeneDose report
Prothrombin (F2) Normal See full GeneDose report
CYP2C19 *1|*1 Extensive metabolizer
CYP2C9 *1|*1 Extensive metabolizer
CYP2D6 *5|*41 Intermediate metabolizer
CYP3A4 *1A|*1A Extensive metabolizer
CYP3A5 *3|*3 Poor metabolizer
SLCO1B1 *1|*1 Normal liver uptake activity
VKORC1 *1|*1 Normal (with respect to Warfarin)
Powered by: Coriell Life Sciences
↑ Cut on dotted lines. ↑ Fold Here
GeneDose™ Genomic Response Report
1000.99999 - Doe, John - Reported Apr 11, 2016
The information contained in this report is intended to be interpreted by a licensed physician or other licensed healthcare professional. This report is
not intended to take the place of professional medical advice. Decisions regarding use of prescribed medications must be made only after consulting
with a licensed physician or other licensed healthcare professional, and should consider each patient's medical history and current treatment regimen.
Page 28 of 28
Powered by:




















![[1992] [DeLone _ McLean] Information Systems Success - The Quest for a Dependent Variable](https://img.pdfslide.us/doc/110x75/5695d1fa1a28ab9b0298ab07/1992-delone-mclean-information-systems-success-the-quest-for-a-dependent.jpg)