Embed Size (px)
Citation preview

Clinical Science (1997) 92,321 -330 (Printed in Great Britain) 32 I
Editorial Review
Gene therapy for diabetes mellitus
Kevin DOCHERTY Department of Molecular and Cell Biology, University of Aberdeen, Institute of Medical Sciences, Foresterhill, Aberdeen, U. K.
1. This review describes experimental approaches to test the feasibility of using gene therapy to administer insulin to type 1 and type 2 diabetic patients. -0 approaches, i.e. en vivo and in vivo transfer of the insulin gene, are described. 2. Substantial progress has been made in recent years in engineering glucose-responsive P-cell lines that have been genetically engineered to proliferate or differentiate in response to appropriate extra- cellular signals. 3. Non-P-cell lines have been engineered to consti- tutively secrete insulin at a constant rate. These cells may improve glycaemic control in patients over longer periods when used in combination with insulin injections. Engineering glucose-stimulated insulin secretion in such cells has proved extremely difficult and several genes may be required. 4. In vivo transfer of the insulin gene to animals results in improved control of diabetes. However, for safety reasons this approach may have limited use in the treatment of diabetes in humans.
INTRODUCTION
In recent years gene therapy has been considered for a growing number of diseases. A certain amount of progress has been made towards gene therapy for single gene defects, such as adenosine deaminase deficiency, cystic fibrosis and some inherited meta- bolic disorders. If the defective gene has been iden- tified and mapped, attempts can be made to replace it with a functional copy, or have a functional copy of the gene expressed in the patient either by modi- fying cells in vivo or implanting cells that have been modified ex vivo. However, many of these genetic disorders are rare, and recently attention has been given to gene therapy for more common disorders, many of which are not inherited. At least two approaches have been adopted for the treatment of infectious diseases by gene therapy: (1) rendering cells resistant to viral infection, thus limiting the
spread of virus in infected individuals; or (2) enhancing antiviral immunity by genetically modify- ing cells so that they express viral gene products to induce an antiviral immune response [l]. In the case of cancer, gene therapy may work by: (1) replacing defective tumour suppresser genes; (2) inactivating overexpressed oncogenes by antisense technology; or (3) delivering genetic pro-drugs that are activated only within cancer cells [2]. Neurological disorders are also seen as targets for gene therapy, either by direct injection of naked DNA into the brain or implanting cells that have been modified ex vivo close to the site of lesion [3]. Gene therapy is attrac- tive in these disorders, which are characterized by considerable morbidity and mortality with little or no effective therapy. The benefits to the patient far outweigh the risks associated with the delivery of genetic material or the aberrant overexpression of the gene product.
It has also been suggested that gene therapy may be applied to the treatment of diabetes mellitus [4-61. However, in this case there is a reliable form of treatment that has stood the test of time (since 1921), and there are potentially real risks to the patient through attempting to use genetic manipula- tion to reinstate blood insulin levels within the extremely narrow physiological limits. Nevertheless, there are strong arguments, outlined below, in favour of new therapeutic approaches to diabetes that are based on recent advances in gene tech- nology.
Diabetes rnellitus
There are two forms of diabetes mellitus, type 1 or insulin-dependent diabetes mellitus (IDDM), and type 2 or non-insulin-dependent diabetes mellitus (NIDDM). IDDM is an autoimmune disorder in which activated T-cells infiltrate the islets of Langer- hans and completely destroy the insulin-producing p-cells. The causes of IDDM are unknown: environ- mental factors such as previous infection by rubella
Keywords: j-cells, cell engineering, insulin gene, insulin replacement, islets of Langerhans. Abbreviations: HLH, helix-loop-helix; IDDM, insulindependent diabetes mellitus; NIDDM, non-insulin-dependent diabetes mellitus; RB, retinoblastoma; RIP, rat insulin promoter: Tag, simian virus 40 large T antigen; tet, tetracycline operon regulatory system; TGN, trans-Golgi network; SV40, simian virus 40; VNTR, vatiable number of tandem repeats. Correspondence: Professor K. Docherty, Department of Molecular and Cell Biology, University of Aberdeen, Institute of Medical Sciences, Foresterhill, Aberdeen AB25 Z D , U.K.
322 K. Docherty
or other infectious agents contribute along with genetic factors to the risk of developing the disease. At least ten different genes are linked to IDDM, of which the HLA region on the short arm of chromo- some 6 and the insulin gene on the short arm of chromosome 11 are most important [7]. IDDM patients are dependent on daily injections of insulin for their survival.
NIDDM is a more common disorder than IDDM (up to 3% in the British population versus about 0.3% for IDDM). It is a relatively heterogeneous metabolic disorder caused by a defect in insulin action and p-cell function [S]. Genetic factors and poor nutrition in utero are associated with the disease, while obesity and lack of exercise in adults are major contributory factors. NIDDM can be con- trolled by diet and exercise, but many patients require concomitant treatment with drugs that stimulate P-cell activity or enhance insulin action. These drugs, however, have limited long-term effi- cacy and ultimately there may be progression to insulin therapy.
There are a number of ways in which gene therapy can be applied to diabetes mellitus. One potential strategy is to target the immune system and prevent the autoimmune destruction of p-cells. An alternative strategy might be to use genetic tech- nology to replace the insulin-secreting capacity of the patient. This could be done by introducing an active insulin gene into tissue in vivo, or by engineering cells ex vivo that could be implanted into the patient. Until we know much more about the nature of the immune destruction of p-cells, there is little prospect of targeting gene therapy to- wards the immune system. On the other hand there has been some progress towards, and a growing literature addressing, the problem of insulin replace- ment by ex vivo and in vivo gene transfer and this will be the main topic of this review. First, one should ask whether there is a requirement for novel methods of administering insulin.
Current regimes for insulin replacement in either IDDM or NIDDM fail to reinstate the normal regu- lation of glucose metabolism, and a large proportion of diabetic patients develop complications such as nephropathy, retinopathy, neuropathy and cardio- vascular disease. The results of the Diabetes Control and Complications Trial have clearly demonstrated that strict glycaemic control can significantly reduce
U P B C
the appearance of these long-term complications in IDDM 1191. Alternative forms of insulin administra- tion have been attempted. Open-loop and closed- loop insulin-infusion devices have not been particularly successful; they require a high patient motivation, are subject to clogging or breakdown and do not provide a physiological replacement of normal amounts of insulin. The development of insulin analogues, with varied pharmaco-kinetic or dynamic properties, that can more closely mimic normal insulin control of glycaemia, have proved disappointing [lo]. Gene therapy on the other hand may provide better day-to-day control of blood glucose with expected improvements in the pros- pects for developing diabetic complications in later life.
Before describing how in vivo or ex vivo transfer of the insulin gene to diabetic patients might be achieved, it is important to understand how insulin- gene expression, biosynthesis, post-translational pro- cessing and secretion are regulated in normal p-cells.
INSULIN EXPRESSION BIOSYNTHESIS AND
Insulin-gene transcription
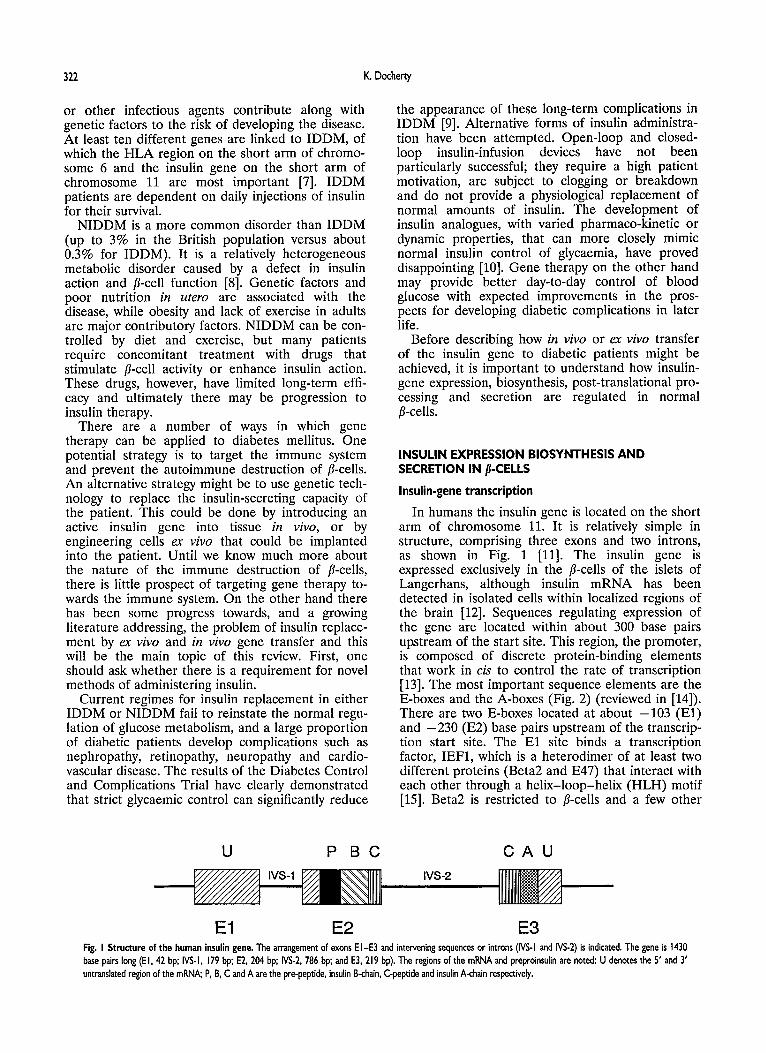
In humans the insulin gene is located on the short arm of chromosome 11. It is relatively simple in structure, comprising three exons and two introns, as shown in Fig. 1 [ll]. The insulin gene is expressed exclusively in the p-cells of the islets of Langerhans, although insulin mRNA has been detected in isolated cells within localized regions of the brain [12]. Sequences regulating expression of the gene are located within about 300 base pairs upstream of the start site. This region, the promoter, is composed of discrete protein-binding elements that work in cis to control the rate of transcription [13]. The most important sequence elements are the E-boxes and the A-boxes (Fig. 2) (reviewed in [14]). There are two E-boxes located at about -103 (El ) and -230 (E2) base pairs upstream of the transcrip- tion start site. The El site binds a transcription factor, IEF1, which is a heterodimer of at least two different proteins (Beta2 and E47) that interact with each other through a helix-loop-helix (HLH) motif [15]. Beta2 is restricted to p-cells and a few other
SECRETION IN /?-CELLS
C A U
E l E2 E3 Fig. I Structure of the human insulin gene. The arrangement of exons EI-E3 and intervening sequences or introns (IVS-I and NS-2) is indicated. The gene is 1430 base pairs long ( E l , 4 2 bp; IVS-I, 179 bp; E2, 204 bp; IVS-2. 786 bp; and E3, 219 bp). The regions of the mRNA and preproinsulin are noted: U denotes the 5' and 3' untranslated region of the rnRNA; P, B, C and A are the pre-peptide, insulin B-chain, C-peptide and insulin A-chain respectively.

Gene therapy for diabetes mellitus 323
SPl lUFl Od-1 USF lUFl CREB lUFl lEFl lUFl Pur-1
I I I I I I I L 350 300 -250 -200 -1 50 -1 00 50 +1
Fig. 2 The human insulin gene promoter. The boxes on the line represent discrete regulatory sequences with their position relative to the transcription start site indicated by the negative numbers underneath. Proteins that bind to these sites are shown above each box. The homoeodomain protein IUFl (IPFIIIDXIISTFI) that binds to the Al, A2, A3 and A5 sites (the A4 site is present in the rat insulin I gene promoter but is absent from the human insulin gene promoter), and the helix-loop-helix heterodimer IEFl, are particularly important.
neuroendocrine cells, whereas E47 (and other related HLH proteins that can heterodimerize with Beta2) are widely distributed. Deletion of the El site has a marked effect on transcription of the gene. The E2 site is much more complex, binding at least three different proteins including the ubiqui- tous HLH factor USF [16]. The E2 site also appears to be important for transcription of the gene.
There are four A-boxes in the human insulin pro- moter (Al, A2, A3 and A5). These sequences bind a homoeodomain factor called IUFl [17] (also known as IPF1, IDXl and STF1) [18-201. IUFl is restricted to @-cells and possibly also somatostatin- secreting cells of the gut. It plays an important role in cell-lineage determination in the developing islets [21]. The endocrine pancreas originates from endo- dermal cells in the gut of embryos of about 20 somites [22, 231. All four islet cell types (p, 01, 6 and PP) arise from a common pluripotent precursor. IUFl is expressed at the earliest stages and is essen- tial for pancreatic development [24]. Co-localization studies show that the endocrine cells pass through various stages where IUFl is co-expressed with com- binations of other hormones. IUFl is subsequently extinguished in 01, 6 and PP cells, remaining co-ex- pressed with insulin in p-cells [25]. IUFl is also important in linking glucose metabolism in the p-cell to the regulation of insulin-gene transcription [26, 271.
Other sequences and their binding proteins are shown in Fig. 2. The role of these other factors and their relative importance are unclear. A VNTR (variable number of tandem repeats) region is located upstream of the promoter, and approxima- tely 200 base pairs beyond this is a hormone response element [28]. The IDDM2 locus that is associated with the inheritance of IDDM has been mapped to the VNTR region [29]. The VNTR binds a transcription factor (Pur-1) and it may also have transcriptional regulatory properties [30].
Despite the marked progress that has been made in describing in detail the insulin promoter and in characterizing the associated DNA-binding proteins,
it is still too early to present models as to how exactly these proteins interact with each other, and with the promoter, to control transcription of the insulin gene. The P-cell factor IUFl (IPFl/IDXl/ STF1) is undoubtedly important.
Proinsulin biosynthesis and processing
Insulin is synthesized as a precursor preproinsulin, that undergoes post-translational processing during its transit through the secretory pathway. The pre- sequence, or signal peptide, is removed cotransla- tionally as the nascent polypeptide chain is transferred into the endoplasmic reticulum. Within the endoplasmic reticulum, proinsulin is folded and disulphide bond formation occurs. Proinsulin is then transferred through the Golgi cisternae, to the trans- Golgi network (TGN), where it is packaged into immature secretory granules. There are two path- ways of secretion in the p-cell (and in neuroendo- crine cells in general): the regulated secretory pathway where proinsulin is packaged into storage granules and secreted in response to appropriate stimuli, i.e. an increase in intracellular calcium con- centration, and the constitutive pathway, which is present in all cell types [31]. The constitutive path- way is used to transfer membrane proteins, viral glycoproteins and other rapidly secreted proteins to the cell surface.
Two endoproteases, PC2 and PC3 (also known as PC1) are involved in the processing of proinsulin to insulin. They operate sequentially, PC3 cleaving at the Arg-Arg sequence at the B-chain-C-peptide junction followed by PC2 cleavage at the Lys-Arg sequence at the C-peptide-A-chain junction (see Fig. 4) [32]. The final stage in proinsulin processing, removal of the newly exposed Arg-Arg residues on the C-terminus of the B-chain, is catalysed by car- boxypeptidase H, which is present in a wide variety of cell types.
PC2 and PC3 are members of a subtilisin-like family of calcium-dependent mammalian proteases

324 K. Docherty
[33]. Their expression is restricted to neuroendo- crine cells where they are involved in the processing of a large number of prohormones, including pro- opiomelanocortin and prosomatostatin. Other mem- bers of the family include PC4 (restricted to testes), PC5, PC6, PC7, PACE4 and furin. Of particular relevance to the present discussion on engineering cell lines to secrete insulin is furin. A type I trans- membrane protein, furin, is present in a wide variety of cell types, where it is located within the TGN. It is involved in the cleavage of membrane-protein precursors (e.g. the insulin proreceptor), a number of growth factors, e.g. transforming growth factor-p, and viral glycoproteins. It specifically recognizes sequences containing the motif Arg-Xaa-Lys/Arg- Arg [W.
Insulin secretion
The major insulin secretagogue is glucose. It is now well established that glucose metabolism is required to stimulate insulin secretion, and the essential details of the glucose sensing mechanism have been described in outline [35]. Glucose uptake into the p-cell is facilitated by a high K, glucose transporter (GLUT2), which allows the intracellular glucose concentration to equilibrate with that in the circulation. Glucose is then phosphorylated by gluco- kinase, which with a high Km (11 mmol/l) is the key enzyme regulating flux through the glycolytic path- way. Increased P-cell glucose metabolism leads to an increase in the ATP/ADP ratio, resulting in closure of the ATP-dependent K+ channel on the cell sur- face. The resultant membrane depolarization acti- vates a voltage-dependent Ca2+ channel; calcium enters the cell and stimulates exocytosis of pre- formed insulin storage granules.
Under normal conditions insulin is secreted in equimolar amounts with C-peptide. However, in patients with NIDDM not all the secreted insulin- like material is fully processed, and substantial quantities of proinsulin and split intermediates, which exhibit only a small percentage of the biologi- cal activity of insulin, are secreted.
CELL ENGINEERING IN THE TREATMENT OF DIABETES MELLITUS
Because of the complex interplay between insulin, other peptide hormones and the sympathetic ner- vous system in glucose homoeostasis, the ultimate objective in administering insulin using implants of genetically engineered cells may be limited. The therapeutic benefits should be regarded as a spec- trum. At one end, the engineered cells would sense changes in circulating glucose levels and secrete appropriate amounts of insulin into the blood stream. These patients would no longer be dependent on injections of insulin. At the other end of the spectrum the cells would not be glucose
responsive; insulin would be released at a constant trickle. The amount of insulin in the circulation in this latter situation would be determined by the number of cells in the initial implant. This low back- ground level would provide basal, between-meal (and night time) control of hepatic glucose output. The patient would continue with insulin injections, the benefit being in the provision of improved gly- caemia and better long-term control of the disease. Between these two ends of the spectrum, cells could be engineered which exhibit some degree of glucose sensitivity, perhaps at the level of the gene, or per- haps even responsiveness to post-prandial increases in gut hormones. Such cells would be particularly important in the treatment of NIDDM.
Having described the objectives of cell engineer- ing for the treatment of diabetes, the next sections will describe in detail how these objectives might be achieved. Three main strategies will be covered: (1) engineering p-cell lines; (2) engineering islet stem cells; and (3) engineering non-p-cell lines. The advantage of engineering Q-cell lines and islet stem cells is that they contain a p-cell phenotype, includ- ing the glucose-sensing mechanism and related insulin secretory response. The disadvantage is that when implanted they may be subject to attack by the immune system, involving mechanisms related to the initial destruction to the patient’s own p-cells. This might be overcome by microencapsulation. The advantage of engineering non-p-cells is that they would not be recognized as p-cells by the immune system. The disadvantage of engineering non-p-cells is that they would not express an endogenous glucose sensor and engineering the various gene products required for this process would present for- midable hurdles.
Engineering /?-cell lines
/&Cells in the form of human islets of Langerhans have been used in the treatment of diabetes for several years [36]. However, islet transplantation has failed to have a major impact on the treatment of diabetes for three principal reasons: (1) following donor transplantation immunosuppression is required, making it most applicable to patients undergoing simultaneous renal transplantation for end-stage complications; (2) the poor availability of donor material for transplantation; and (3) the poor yield of pure islets during the isolation procedure. Several approaches have been taken to avoid the need for immunosuppression, including altering the immune properties of the islet by, for example, expressing adenovirus early region 3 (E3) genes [37], eliminating non-endocrine cells that are responsible for triggering islet rejection, and induction of graft tolerance by, for example, targeting CD4+ T-cells [38, 391. In addition, the graft may be encapsulated within microcapsules or hollow fibres that protect the islets from immune attack but provide access to

Gene therapy for diabetes rnellitus 325
nutrients and allow insulin to escape into the cir- culation [40-441. However, even if these advances led to successful grafting of islets, the lack of donor material would still limit this approach. This could be overcome if xenotransplantation was proven to work. Studies to date have concentrated on pig islet xenografts [45]; however the pig islet is particularly difficult to isolate and purify because of the nature of the pig islet capsule and its tendency to fragment easily. Engineering /?-cell lines may provide a method which avoids the problems associated with islet isolation and purification.
Adult islets of Langerhans are for the most part terminally differentiated cells that will not grow and divide in culture. However, a number of immortal- ized p-cell lines have been generated. This has been achieved by simian virus 40 (SV40) transformation or X-ray irradiation of isolated islets, by cell fusion between islets and immortalized cells or by expres- sion of oncogenes in transgenic mice. The problem with these cells is that they tend to lose glucose responsiveness after short periods in culture. This may be related to a process of ongoing dediffer- entiation which is associated with a variety of marker proteins. This process has been extensively investigated and has been shown to be related pre- dominantly to a decrease in the levels of both GLUT-2 and glucokinase.
One approach has been to stably transfect immor- talized /.?-cell lines with genes encoding GLUT-2 or glucokinase. When RIN cells (an immortalized rat /.?-cell line) were stably transfected with GLUT-2, glucose-stimulated insulin secretion was observed at both physiological and subphysiological concentra- tions of glucose [46]. Cells over-expressing glucoki- nase alone did not show an enhanced insulin secretory response to glucose. Interestingly, the levels of glucokinase enzymic activity were elevated in cells stably transfected with GLUT-2. The reason for this is unclear, but it suggests that GLUT-2 and glucokinase are essential for the insulin response to glucose. Further support for a role for glucokinase comes from the observation that pre-incubation of RIN cells in 2-deoxyglucose (which inhibits hexoki- nase) for 24 h shifted the glucose dose that maxi- mally stimulated insulin from 50 pmol/l to 5 mmol/l (i.e. close to the physiological range) [46]. Clearly, knocking out hexokinase in p-cells stably transfected with GLUT-2 may well shift the glucose response to within the physiological range.
An alternative strategy is to generate conditionally transformed p-cell lines that contain a genetic switch which determines whether they grow and divide in culture or remain within a non-dividing differen- tiated state. Immortalization of cells can be achieved by introducing into the cell the viral oncogene SV40 large T antigen (Tag). SV40 Tag acts by sequester- ing the p53 and retinoblastoma (RB) gene products which act together as 'gatekeepers' to the cell cycle [47]. To generate immortalized p-cell lines, the insulin-gene promoter, which is usually designated
RIP for rat insulin promoter, is joined to the gene encoding SV40 Tag. This DNA construct, RIP-Tag, is microinjected into mouse embryos, which are then implanted into pseudopregnant female mice. In the resultant offspring the SV40 Tag is expressed exclu- sively in the p-cells, which grow into a tumour. The p-cell tumour is removed and cell-lines are gener- ated [48]. The problem is that SV40 Tag retains some transforming activity and the resulting cell- lines tend to dedifferentiate. This problem associ- ated with the use of Tag has been surmounted to some extent by using temperature-sensitive mutants of SV40 Tag. At raised temperatures (39°C) the mutant (SV40TS Tag) loses its ability to bind p53 and RB, whereas at lower temperatures (33°C) it binds p53 and RB [49]. Thus rat hepatocytes trans- formed with SV4OTS Tag grew as an immortalized cell line at 37"C, but secreted only very low levels of the liver-cell markers albumin and transferrin, i.e. they were dedifferentiated. On switching to the non- permissive temperature (39°C) the secretion of albu- min and transferrin increased between 10- and 20-fold [50]. These experiments showed that condi- tionally transformed cell-lines could be generated by switching Tag activity on and off.
Deuschle et al. [51] took this further by placing SV40 Tag under the control of a genetic switch involving the bacterial tetracycline operon regulatory system (tet) from TNlO of Escherischia coli. Using this system, Tag activity could be regulated in vivo [51]. Efrat et al. [52] used the tet regulatory system to generate p-cell lines that were conditionally trans- formed. In one strain of transgenic mice a fusion protein containing the tet repressor joined to the activating domain of the herpes simplex virus pro- tein VP16 (TETR-VP16), which converts the repressor into an activator, was produced in p-cells under the control of the insulin promoter (RIP). In another strain of transgenic mice the Tag gene was introduced under the control of a tandem array of the tet operator sequences and a minimal promoter. This construct was not expressed since it lacked the functional promoter. Mice from the two resultant lineages were crossed to generate double-transgenic mice. The expressed TETR-VP16 fusion protein bound to the tet operator sequences and activated Tag in p-cells, thus generating /I-cell tumours. Cells derived from these tumours grew in culture, but in the presence of a tetracycline analogue, which sequestered the TETR-VP16 protein, the cells stopped growing. When these cells were implanted into mice rendered diabetic by treatment with strep- tozotocin the blood glucose levels normalized within 2 weeks. However, the cells continued to proliferate, resulting in hypoglycaemia and premature death. When the cells were implanted along with a slow- release tetracycline pellet, the cells no longer pro- liferated and normal glycaemia was maintained for up to 4 months. These exciting results indicate that proliferating cells containing a genetic switch may have uses in the treatment of diabetes. They main-

326 K. Docherty
tain the cell within a differentiated state and they prevent problems associated with increased insulin levels due to cell proliferation continuing post- implantation. It will be interesting to see whether these cells adjust their activity to coincide with fluc- tuations in blood glucose, as seen during overnight fasting or during glucose infusion. As regards their use in the treatment of diabetes, it is unlikely that mouse cells will be used. A better source of cells would be the pig (see Fig. 3). Pig physiology is more similar to human than is mouse; pig insulin has been used in the treatment of diabetes for many years, and the pig transgenic technology is now available.
Engineering islet stem cells
From the previous description of mechanisms regulating insulin-gene transcription, the question arises as to whether introduction of appropriate transcription factors into non-p-cells will switch on transcription of the endogenous insulin gene. Such experiments should be encouraged; however, our understanding of transcription suggests that regula- tion involves a subtle interplay, dependent on the relative concentrations of a number of proteins most of which are present in a wide variety of cell types. Under different conditions, e.g. post-translational modification or different partnerships, these pro- teins can act in either a positive or negative manner [53]. Conceptually, switching on a non-p-cell endo- genous insulin gene, in for example liver or other major organs, is difficult to imagine.
On the other hand, it may be possible to target islet stem cells. As described previously there have been major breakthroughs in our understanding of islet cell ontogeny and the role of transcription factors such as IUFl in lineage determination. There is, however, a large gap in our knowledge as to how islet cells are replaced in the adult. It is likely that there is a continuous slow turnover of cells, fed from a stem-cell population in the pan- creatic duct [23]. The stimuli for these cells to mature may be local rather than systemic, possible candidates including vascular endothelial growth factor [54]. If residual islet stem cells could be iso- lated from the pancreatic duct of IDDM patients, it might be possible to induce growth and differentia- tion of a p-cell phenotype by stably transfecting them with appropriate p-cell transcription factors, or even oncogenes [55]. The induction of the endogen- ous insulin gene in a-like cells transfected with IUFl is particularly encouraging [56]. However, to test the feasibility of this approach we need much more data on the properties of such stem cells and methods for their isolation and culture.
Engineering non-$cells
There are two potential approaches to engineer- ing non-p-cells. The first involves introducing the insulin gene (and other genes as necessary) into primary cultures of cells taken from a diabetic patient. The cells would have to come from an accessible site (e.g. skin or muscle), grow well in cul-
I tet-operator Tag I
Tag in all cells
I RIP tet-act I
Tet-act protein expressed but not expressed $. in Beta cells
Tet-act switches on Tag in Beta cells.
When Beta cells are treated with Tet, Tag is switched off. Fig. 3 Generation of tansgenic pigs containing a genetic switch controlling proliferation and differentiation. One transgenic line contains a tet activator protein (fusion protein combining the tet repressor with the activator domain of VP16) under the control of the insulin promoter (RIP). The tet activator is expressed in fi-cells. A second transgenic line contains the large T antigen (Tag) downstream of a minimal promoter and repeat sequences from the tet operator. This DNA is present in all cells but because it has a minimal promoter it is not expressed. These pigs are mated so that in the resultant offspring the tet activator promoter binds to the tet operator sequences in the !-cells and switches on expression of Tag. When the !-cells are treated with a tetracycline analogue, expression of Tag is switched off. Other variations of this model exist. For example, mutations in the tet repressor-W 16 fusion protein will cause it to act as a repressor in the absence of tetracycline and an activator in the presence of tetracycline.

Gene therapy for diabetes mellitus 327
ture and be amenable to genetic manipulation. They would be characterized for insulin production in vitro, and having passed various levels of quality control [4] they would be transplanted back into the donor patient. Such syngeneic transplantation would conceivably avoid problems associated with tissue rejection. The second approach would be to trans- fect a non-p-cell line with the insulin gene (cDNA). In this case the cells would be grown in culture, characterized, cryopreserved and implanted into patients as required. The cells would be encapsu- lated into matrix gel or hollow fibres to protect them from rejection. The overall strategy is the same for both approaches and the technical problems similar. However, introducing DNA into primary cell cul- tures is more difficult, or more technically demand- ing, than into established cell lines, and would probably involve the use of high titre retroviral or adenovirus vectors.
Most of the work to date has focused on engineering immortalized non-p-cell lines. Neuro- endocrine cells have been used because they contain a regulated secretory pathway with the relevant endoproteases to support processing of proinsulin to insulin. Thus over 10years ago the mouse cortico- trophic cell line, AtT20, stably transfected with an insulin gene (cDNA) was shown to efficiently pro- cess proinsulin to insulin [57]. Insulin was secreted by way of the regulated pathway, i.e. secretion was stimulated by membrane depolarization in the presence of calcium. However, this cell line (AtT20ins) did not release insulin in response to glucose. It did, however, express an endogenous glu- cokinase gene, and so attempts were made to engineer AtT20ins cells that would respond to glucose by stably transfecting them with a cDNA encoding GLUT2 [58]. The experiment was partially successful in that the cells responded to glucose, but not in the physiological range. Maximal insulin secretion was recorded over the range 50,umolfl to 20 mmol/l. This insulin secretory response was not observed in AtT20ins cells transfected with the high- affinity glucose transporter GLUT1, suggesting that the effects were specific to GLUT2 [59]. Obviously, components in addition to GLUT2 and glucokinase are required to engineer glucose responsiveness in non-p-cell lines. It will be of interest to determine how many of these components can be expressed simultaneously in a transfected cell.
In a separate study, AtT20 cells were stably trans- fected with a human insulin cDNA under the con- trol of a metallothionein promoter [60-621. Peritoneal implantation of these cells (AtT20Mtins) in nude mice resulted in plasma human C-peptide levels of 0.1 pmol/ml, which is about 25% of the values in normally fed non-diabetic human subjects. Subsequent administration of streptozotocin pro- duced severe and fatal hyperglycaemia in mice implanted with non-transfected AtT2O cells. The implanted AtT20Mtins cells delayed the develop- ment of hyperglycaemia by about 2weeks. The
animals then developed hyperglycaemia despite the maintenance of human C-peptide levels. Injection of insulin into these animals failed to correct the hyperglycaemia, suggesting that they had become insulin resistant as a consequence of increased glucocorticoids resulting from the ACTH that was co-secreted with insulin from the cell implant. These experiments suggested that AtT20, and possibly other neuroendocrine cells, may have limited use in the delivery of insulin to diabetic patients, unless efforts are made to knock-out the gene for co-se- creted peptides which may have an antagonistic effect on the action of insulin or otherwise upset the metabolic balance of the patient.
Non-neuroendocrine cell engineering may there- fore prove more beneficial in the long term. The problem with these cells is that they lack a regulated secretory pathway and the enzymes (PC2 and PC3) involved in converting proinsulin to insulin. Thus stable transfection of fibroblasts with an insulin cDNA results in secretion of intact proinsulin with very little of the split intermediates (des 64, 65 proinsulin and des 31, 32 proinsulin) and fully pro- cessed insulin. The cells, however, contain the related protease furin in their TGN. Therefore to allow conversion of proinsulin to insulin to occur in a wide variety of cells, site-directed mutagenesis was used to change the cleavage sites within human proinsulin to a furin consensus cleavage site (Fig. 4) [63]. In cells transfected with the mutant insulin cDNA (minigene) the extent of processing of proin- sulin to insulin correlated with the levels of furin in NIH3T3 (fibroblast), HeG2 (liver), COS (kidney epithelial) and CHO (ovary epithelial) cells [64]. In cells with low levels of endogenous furin, complete conversion of proinsulin could be achieved by cotransfecting the mutant insulin cDNA along with a cDNA encoding furin. Of major importance was the observation that myoblasts transfected with the mutant insulin cDNA could secrete fully processed insulin [65]. The major advantage of using myoblasts to deliver insulin to diabetic patients is that they contain a built-in switch that controls proliferation and differentiation. That is, they can be induced to form myotubes that no longer grow and divide. If stably transfected myotubes can be shown to secrete insulin then this may provide an excellent system for delivering a constitutive background level of insulin in patients.
As mentioned above, transplantation of non- neuroendocrine cells, engineered to secrete fully processed insulin as a trickle, may have some bene- ficial effects on the progress of the disease. The assembly of a full glucose secretory response in such cells presents formidable problems. It may, however, be possible to regulate the gene at the level of trans- cription by co-transfecting the mutant minigene, under the control of a glucose-responsive element from the insulin or other appropriate promoters (e.g. the L-type pyruvate kinase promoter), along with appropriate transcription factors, e.g. IUF1.

K. Docherty
KTRREA LQKRGI
Insulin B chain C-Peptide + Insulin A chain
PC3 PC2
KTRRKR RRKRGI
Insulin B chain C-Peptide Insulin A chain
Furin Furin Fig. 4 Construction of an insulin minigene that will support processing of proinsulin to insulin in non-neuroendocrine cells. Processing of human proinsulin to insulin involves the sequential action of two endoproteases, PC3 which cleaves at the sequence RR (Arg-Arg) between the insulin B-chain and the C-peptide, and PC2 which cleaves at the sequence KR (Lys-Arg ) between the C-peptide and the insulin A-chain. Sitedirected mutagensis was used to mutate both cleavage sites to recognition sites for the endoprotease furin. When transfected into non-endocrine cells, e.g. HepG2 (liver) or C2C12 (muscle), the mutant proinsulin, but not wild-type proinsulin, was efficiently processed to insulin. In xlme cells, however, complete processing could only be achieved by co-transfecting the mutant insulin minigene along with a [DNA encoding furin (K. Docherty, H.M. Docherty, H. Crag, k Hart, JA Shaw and K.I.J. Shennan, unpublished work).
The response to changes in glucose levels would be sluggish, but at least some post-prandial increase in circulating insulin levels might be achieved.
IN VlVO DELIVERY OF THE INSULIN GENE
Genetic material can be delivered to tissues in vivo by direct administration of naked DNA, or more usually by entrapping the DNA in liposomes or by using retroviral or adenoviral vectors. A number of studies have addressed the feasibility of in vivo gene therapy for the administration of insulin to diabetic patients. Thus a rat insulin I gene frag- ment containing the insulin gene regulatory sequences was entrapped in liposomes and intro- duced intravenously into rats [66, 671. The liposomes were taken up by the liver where the insulin gene was expressed for a relatively short time (10 h). The secreted insulin-like material (which was not fully characterized) reduced blood glucose levels by about 30% [66]. More recent studies have shown that injection into the portal vein of a retroviral vector harbouring an insulin cDNA under the control of a viral long terminal repeat region resulted in uptake and expression of insulin in the liver [68]. When these animals were subsequently made diabetic by treatment with streptozotocin, ectopic expression of insulin in the liver prevented ketoacidosis and death. Normoglycaemia was achieved during a 24 h fast, while no adverse effects on the animals were observed for up to 20days after the onset of dia- betes. Ectopic expression of insulin in the liver has also been achieved in transgenic mice using a DNA construct in which the insulin gene is driven by the phosphoenolpyruvate carboxykinase promoter [69].
Again, the background level of insulin had a bene- ficial effect on glycaemia when the animals were treated with streptozotocin. Taken together, these studies support the view that a constant trickle of insulin can have beneficial effects on diabetes.
In vivo delivery of insulin genes in diabetic patients must however be viewed with some caution. There is no fail safe method of ensuring a set rate of insulin release from ectopic tissues. Among the many variables that might affect the rate of insulin secretion, the random manner in which the gene integrates within the genome and the effect that this might have on expression may be the most import- ant. The same could be said of implanted cells, but as long as they were encapsulated and implanted in a suitable way so that they could be readily removed (or destroyed by the host immune system if released accidentally from the capsule), then the procedure could be reversed if necessary. On the other hand, the risk versus benefit for in vivo gene transfer may not be sufficiently favourable.
CONCLUSION
The application of gene therapy to diabetes presents formidable problems that have yet to be encountered in its application to other diseases. Advances in gene therapy have been made in the treatment of single-gene disorders, such as acquired immune deficiency syndrome and cystic fibrosis, where the genes involved (adenosine deaminase or cystic fibrosis transmembrane regulator) have been isolated and the pathology is well known. In these cases the patients are extremely ill and presently available forms of therapy do not prolong life

Gene therapy for diabetes mellitus 329
beyond a certain period. There is an available route of administration of the gene: in the blood stream or nasal or lung airways. The same is true of cancer and some neurological disorders where low-level expression of the gene will provide benefits while high-level expression will not cause additional prob- lems. On the other hand, administration of insulin by engineered cells presents new problems. Insulin is a potentially lethal protein that at high doses will cause hypoglycaemia and death. Its activity levels must be restricted within very narrow limits. Developing a strategy for cell engineering for dia- betes is very different from that in the above examples where the benefits far outweigh the risks. Any form of gene therapy which involves the expres- sion of an exogenous insulin gene in patients must be reversible, so that if high-level expression occurs then the implant can be removed.
Engineering insulin-secreting cell lines has received a great deal of interest and some exciting advances have been made. The development of cell lines that contain a genetic switch controlling pro- liferation and differentiation of the cells is seen as being of particular importance, and one can expect substantial investment in the development of more refined switches, e.g. based on the cre/lox system. We now know more about the subtle interplay between GLUT-2 and glucokinase in glucose-stimu- lated insulin secretion in immortalized p-cells. Reducing hexokinase levels by antisense techniques may go some way towards solving some of the present problems. The use of residual stem cells is appealing but we need more research in this area. Engineering glucose-responsive non-p-cell lines is proving much more difficult and many of the prob- lems have yet to be resolved. In the meantime, the constitutive release of insulin from engineered cells may show clear improvements in long-term glucose control, particularly in NIDDM.
ACKNOWLEDGMENTS
Related work from this laboratory was funded by the British Diabetic Association and the Medical Research Council and was performed in collabora- tion with Dr. C.J. Bailey of the University of Aston, Birmingham, U.K.
REFERENCES I. Gilboa E, Smith C. Gene therapy for infectious diseases: the AIDS model. Trends
2. Culver Kw, Blaese RM. Gene therapy for cancer. Trends Genet 1994; 1 0
3. Friedman T. Gene therapy for neurological disorders. Trends Genet 1994; 10
4. Selden RF, Skoskiewia MJ, Russel PS, Goodman HM. Regulation of insulin-gene expression. New Engl J Med 1987; 3 17: 1067-76.
5. Docherty K. Gene therapy and cellular engineering in diabetes. In: Pickup JC, ed. Biotechnology of insulin therapy. Oxford Blackwell Scientific, 1991: 154-82.
6. Newgard CB. Cellular engineering and gene therapy strategies for insulin replacement in diabetes. Diabetes 1994; 43: 341-50.
Genet 1994; 10 139-44.
174-8.
210-4.
7. Todd ]A Genetic analysis of type I diabetes using whole genome approaches. Proc Natl Acad Sci USA 1995; 9 2 8560-5.
8. Gray H, OMilly S. B-Cell dysfunction in non-insulin dependent diabetes mellitus. Transplant Proc 1994; 2 6 366-70.
9. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long- term complications in insulin-dependent diabetes mellitus. New Engl J Med 1993;
10. Galloway ]A, Chance RE. Improving insulin therapy achievements and challenges.
I I. Bell GI, Pictet RL, Rutter WJ. Cordell B, Tixher E, and Goodman, HM. Sequence
12. Devaskar SU, Giddings SJ, Rajakumar PA, Carnaghi LR, Menon RK, Zahm DS.
329: 977-86.
Horm Metab Res 1994; 2 6 59 1-8.
of the human insulin gene. Nature (London) 1980; 284: 26-32.
Insulin gene expression and insulin synthesis in mammalian neuronal cells. J Biol Chem 1994; 269 8445-54.
13. Walker MD, Edlund T, Boulet AM, Rutter w]. Cell-specific expression controlled by the 5' flanking region of insulin and chymotrypsin genes. Nature (London)
14. Docherty, K. Clark, kR The regulation of insulin gene expression. In: Leslie RDG, Robbins D, eds. Diabetes: clinical science in practice. Cambridge: Cambridge University Press, 1995: 15-31.
15. Naya FJ, Stellrecht CMM, Tsai M-J. Tissue-specific regulation of the insulin gene by a novel basic helix-loop-helix transcription factor. Genes Dev 1995; 9:
16. Read ML, Clark AR, Docherty K. The helix-loop-helix transcription factor USF
1983; 306 557-61.
1009- 19.
binds to a regulatory sequence in the human insulin gene enhancer. Biochem J 1993; 295: 233-7.
the human insulin gene enhancer. Biochem. J. 1989; 2 M 233-9.
of the insulin gene. EMBO 1. 1993; I2 425 1-9.
of somatostatin transactivating factor-I P: a novel homeobox factor that stimulates Somatostatin expression in pancreatic islet cells. Mol Endocrinol 1993;
17. Boam DSW, Docherty K. A tissue specific nuclear factor binds to multiple sites in
18. Ohlsson H, Karlsson K, Edlund T. IPFI, a horneodomain-containing transactivator
19. Leonard J, Peers B, Johnson T, Ferreri K, Lee S, Montminy M. Characterisation
7: 1275-83. 20. Miller CP, McGehee Jr. RE, Habener JF. IDX-I: a new homeodomain
transcription factor expressed in rat pancreatic islets and duodenum that transactivates the somatostatin gene. EMBO J 1994; 13: I 145-56.
21. Jonsson J, Carlsson L, Edlund T, Edlund H. Insulin-promoter-factor I is required for pancreas development in mice. Nature (London) 1994; 371: 606-9.
22. Pictet R, Rutter WJ. Development of the endocrine pancreas. In: Steiner DF, Frenkel, M, eds. Handbook of physiology. Washington D C American Physiological Society, 1972 25-66.
23. SlackJMW. Developmental biology of the pancreas. Development 1995; 121:
24. Jonsson J, Ahlgren U, Edlund T, Edlund H. IPFI, a homeodomain protein with a dual function in pancreas development. Int J Dev Biol 1995; 3 9 789-98.
25. GmY, Montminy MR, Stein R, Leonard J, Gamer LW, Wright CVE, Teitelman G. Expression of murine STF-I , a putative insulin gene transcription factor, in &cells of pancreas, duodenal epithelium and pancreatic exocrine and endocrine progenitors duringontogeny. Development 1995; 121: 11-18,
26. MacFarlane WM, Read ML, Gilligan M, Bujalska I, Docherty K. Glucose modulates the binding activity of the &cell transcription factor, IUFl, in a phosphorylation-dependent manner. Biochem J 1994; 303: 625-3 I .
27. Docherty K, Macfarlane WM, Read ML, Smith SB, Wilson ME, Bujalska I, Gilligan M. Regulation of insulin gene transcription by nutrients. Biochem Soc Trans 1996;
1569-80.
24: 368-72. 28. Clark AR, Wilson ME, London NJM, James RFL, Docherty K. Identification and
characterization of a thyroid hormonelretinoic acid response element upstream of the human insulin gene. Biochem. J. 1995; 309: 863-70.
29. Bennet ST, Lucassen AM, Gough SCL, et al. Susceptibility to type I diabetes at lDDM2 is determined by tandem repeat variations at the insulin gene minisatellite locus. Nature (Genetics) 1995; 9: 285-92.
susceptibility locus lDDM2 regulates insulin transcription. Nature (Genetics) 30. Kennedy GC, German MS, Rutter WJ. The minisatellite in the diabetes
1995; 9 293-8.
25-3 I . 3 I . Kelly RB. Pathways of protein secretion in eukaryotes. Science 1995; 230:
32. Bailyes EM, Shennan KIJ, Seal AJ, Srneekens SP, Steiner DF, Hutton JC. Docherty K. A member of the eukaryotic subtilisin family (PC3) has the enzymic properties of the type I proinsulin converting endopeptidase. Biochem J 1992; 285: 39 1-4.
33. Halban PA, lrminger J-C. Sorting and prxessing of secretory proteins. Biochem J 1994;299 1-18.

330 K. Docherty
34. Van de Ven WJM, Roebroek AJM, Van Duijnhoven HLP. Structure and function of eukaryotic proprotein processing enzymes of the subtilisin family of serine proteases. Crit Rev Oncogenesis 1993; 4: 115-36.
35. Ashcroft FM, khcroft SJH. Mechanisms of insulin secretion. In: Ashcroft FM, Ashcroft SJH, eds. Insulin, molecular biology to pathology. Oxford/New Yorkl Toronto: Oxford University Press, I992 97- 150.
36. Sutherland DER Present status of pancreas transplantation alone in nonuremic diabetic patients. Transplant Pm 1994; 2 6 379-83
37. Efrat S, Fejer G, Brownlee M Horwia MS. Prolonged survival of pancreatic islet allografts mediated by adenovirus immunoregulatory transgenes. Proc Natl Acad Sci USA 1995; 92: 6947-5 I.
38. Yeo A, Lamb JR Manipulating the immune response in allergic disease: targeting CD4' T cells. Trends Biotechnol 1995; 13: 186-90.
39. Lafferty KJ, Hao L. Approaches to the prevention of immune destruction of transplanted pancreatic islets. Transplant Proc 1994; 2 6 399-400.
40. Colton CK. Engineering challenges in cell-encapsulation technology. Trends Biotechnol 1996: 14: 158-62.
41. Li RH, Altreuter DH, Gentile FT. Transport characterisation of hydrogel matrices for cell encapsulation. Biotechnol Bioeng 1996; 5 0 365-73.
42. Scharp DW, Swanson CJ, Olack BJ, et al. Protection of encapsulated human islets implanted without immunosuppression in patients with type I or type II diabetes and in nondiabetic control subjects. Diabetes 1994; 43: 1167-70.
43. Sullivan SJ, Maki T. Borland KM, et al. Biohybrid artificial pancreas: long-term implantation studies in diabetic, pancreatectomised dogs. Science 1991; 252
44. Lacy PE. Treating diabetes with transplanted cells. Scientific American 1995; 40-6.
45. Tibell A, Groth CG, Korsgren 0, Andenson A, Hellerstrom C. Pig-to-human islet transplantation in eight patients. Transplant Proc. 1994; 2 6 762-63.
46. Ferber S, Beltrande H, Johnson JH. et al. GLUT-2 gene transfer into insulinoma cells confers both low and high affinity glucose-stimulated insulin release. J Biol Chem 1994; 269 I 1523-9.
47. McLean IS. Improved techniques for immortalizing animal cells. Trends Biotechnol 1993; I I: 232-8.
48. Hanahan D. Heritable formation of pancreatic /?-cell tumours in transgenic mice expressing recombinant insulin/simian virus 40 oncogenes. Nature (London) 1985; 3 15: I 15-22.
49. Jat PS, Sharp PA Cell lines established by temperature-sensitive simian virus 40 large-T-antigen gene are growth restricted at the non-permissive temperature. Mol Cell Biol 1989; 9 1672-81.
enhancement of liver-specific gene expression. Proc Natl Acad Sci USA 1988; 85:
718-21.
50. Zaret KS, DiPersio CM, Jackson DA, Montigny WJ, Weinstat DL Conditional
9076-80. 5 I. Deuschle U, Pepperkok R Wang F, Giordano TJ, McAllister WT, Ansorge W,
Bujard H. Regulated expression of foreign genes in mammalian cells under the control of coliphage T3 RNA polymerase and lac repressor. Proc Natl Acad Sci USA 1989; 8 6 5400-4
transformation of a pancreatic jsell line derived from transgenic mice expressing a tetracycline-regulated oncogene. Proc Natl Acad Sci USA 1995; 9 2 3576-80.
52. Efrat S, Fusco-Demane D, Lemberg H. Emran OA, Wang X. Conditional
53. Clark AR, Docherty K. Negative regulation of transcription in eukaryotes. Biochem J 1993; 296 521-41.
54. Oberg C, Waltenberger J, Claesson-Welsh L, Welsh M. Expression of protein tyrosine kinases in islet cells: possible role of the Flk-l receptor for /?-cell maturation from duct cells. Growth Factors 1994; 10 I 15-26.
55. Welsh M, Welsh N, Nilsson T, Arkhamrnar P. Pepinsky RB, Steiner DF. Berggren P-0. Stimulation of pancreatic islet beta-cell replication by oncogenes. Proc Natl Acad Sci USA 1988; 85: I 16-20.
56. Serup P, Jensen J. Andersen FG, Jlergensen MC, Blume N, Holst JJ, Madsen OD. Induction of insulin and islet amyloid polypeptide production in pancreatic islet glucagonoma cells by insulin promoter factor I. Proc Natl Acad Sci USA 1996: 9 3 9015-20.
57. Moore H-P, Walker MD, Lee F, Kelly RB. Expressing a human proinsulin cDNA in a mouse ACTH-secreting cell: intracellular storage, proteolytic processing and secretion on stimulation. Cell 1983; 35: 53 1-8.
stimulated insulin secretion an biosynthesis in non-islet cells. Proc Natl Acad Sci USA 1992; 8 9 688-92.
59. Hughes SD, Quaade C, Johnson JH, Ferber S, Newgard CB. Transfedion of AtT- 20ins cells with GLUT-2 but not GLUT-I confers glucose-stimulated insulin secretion. J Biol Chem 1993; 268 15205-12.
gene therapy. J Mol Endocrinol 1993; I I: 335-41.
pituitary cells as a model for somatic cell gene therapy in diabetes mellitus. J Endocrinol 1994; 142 339-43.
62. Bailey CJ, Docherty K. Exploring the feasibility of insulin gene therapy. In: Flatt PR, Lenzen S. eds. Frontiers of insulin secretion and pancreatic B-cell research. London: Smith-Gordon, 1995: 78- 1-78-7.
constitutively processed and secreted as mature active insulin. J Biol Chem 1994;
58. Hughes SD, Johnson JH, Quaade C, Newgard CB. Engineering of glucose-
60. Stewart C, Taylor NA, Docherty K, Bailey CJ. Insulin delivery by somatic cell
6 I. Stewart C, Taylor NA, Green IC, Docherty K, Bailey CJ. Insulin-releasing
63. Groskreutz J, Sliwkowski MX, Gorman CM. Genetically engineered proinsulin
269: 6241-5. 64. Yanagita M. Hoshino H, Nakayama K, Takeuchi T. Processing of mutated
proinsulin with tetrabasic cleavage sites to mature insulin reflects the expression of furin in non-endocrine cell lines. Endocrinology 1993; 133: 639-44
processing of genetically modified human proinsulin by rat myoblast primary cultures. Human Gene Therapy 1996; 7: 7 1-8.
66. Nicolau C, Pape AL, Soriano P, Fargette F. Juhel M-F. In vivo expression of rat insulin after intravenous administration of the liposome-entrapped gene for rat insulin I. Proc Natl Acad Sci USA 1983; 8 0 1068-72.
67. Kaneda Y, lwai K. Uchia T. Introduction and expression of the human insulin gene in adult rat liver. J Biol Chem 1989; 264 I21 26-9.
68. Koloddka TM, Finegold M, Moss L, Woo SL. Gene therapy for diabetes mellitus in rats by hepatic expression of insulin. Proc Natl Acad Sci USA 1995; 9 2
65. Simonson G, Groskreua DJ. Gorman CM, Macdonald MJ. Synthesis and
3293-7. 69. Valera A, Fillat C, Costa C, Sabater J, Visa J, Pujol A, Bosch F. Regulated
expression of human insulin in the liver of transgenic mice corrects diabetic alterations. FASEB J. 1994; 8 440-7.





























