Embed Size (px)
Citation preview

J. med. Genet. (I966). 3, I69.
Gene Effect in Carriers of AnhidroticEctodermal Dysplasia*
C. B. KERRt, R. S. WELLS, and K. E. COOPER
From the Medical Research Council Population Genetics Research Unit, Headington, Oxford, and the Department of theRegius Professor of Medicine, Radcliffe Infirmary, Oxford
Anhidrotic Ectodermal DysplasiaIn an extensive review of different forms of
hereditary ectodermal dysplasia, Cockayne (I933)recognized two types of inheritance for the varietycharacterized by anhidrosis, hypotrichosis, andcomplete or partial anodontia. He postulated anX-linked recessive gene in families where malesalone were affected and an autosomal dominant genewhere females were involved. However, as pointedout by Levit (1936), females never exhibited the fullsyndrome, and the inheritance in all familiesreviewed by Cockayne was consistent with X-linkage.Many subsequent reports of males with X-linked
anhidrotic ectodermal dysplasia have establisheda remarkably consistent phenotype. The outstand-ing feature is lack of sweating, as perceived by thepatient and on external examination of the skin.This results from a gross but not absolute deficiencyof sweat glands. Hair on the scalp and eyebrows issparse and fine and usually lacking on the bodysurfaces though adults may develop a beard. Non-eruption of teeth at either dentition may result incomplete anodontia but more frequently a few mal-formed teeth are present. Lack of teeth providesone aspect of the characteristic facies which togetherwith hypotrichosis, prominent bossing of the fore-head, and typically depressed bridge of the noserenders affected males similar in appearance.The evidence for an autosomal dominant variety
of anhidrotic ectodermal dysplasia remains incon-clusive. Some confusion with the hidrotic varietyis evident in certain reports. This latter form ischaracterized by hypotrichosis and dystrophy of thenails in association with normal sweating and
Received December 6, I965.* Requests for reprints to M.R.C. Population Genetics ResearchUnit, Old Road, Headington, Oxford.
t Present address: School of Public Health and Tropical Medicine,University of Sydney, Sydney, New South Wales, Australia.
dentition. It was clearly distinguished from theanhidrotic variety in 1929 by Weech, and numerousstudies have confirmed autosomal dominant inherit-ance (Clouston, I939; Bruno and Engelhardt, i944;White, I964; Mallmann-Muhlberger and Helwig,I964). In other reports alleged instances of auto-somal dominant anhidrotic ectodermal dysplasiawere either recorded without adequate details orwere very atypical. The father-son transmission inBattersby's (1936) pedigree was based on hearsayevidence and remote from the investigated part ofthe family where inheritance was consistent withX-linkage. Another widely-quoted example ofautosomal inheritance concerns the family reportedby Brain (1937), but mention of 'nail dystrophy' inthe father of a male with the anhidrotic form cannotbe accepted as evidence of gene effect. The samereasoning applies to the family described by Liptonand Roberts (I950), where the claim for autosomalinheritance was based on a history of one abnormaldeciduous tooth in the father. Several uniquefamilies have been described where the pattern ofinheritance suggested autosomal dominant an-hidrotic ectedermal dysplasia associated with mentalretardation (Halperin and Curtis, 1942), neuro-labyrinthitis (Helweg-Larsen and Ludvigsen, 1946),or primary hypogonadism (Mohler, 1959). Femaleswith the full syndrome and no affected male relativeshave been reported either as sporadic cases (Wagner,I952), offspring of an uncle-niece mating (Lipscomband Manonmani, I952), or in three generations ofone family (Bernard, Giraud, Rouby, and Hartung,1963). Clearly, the condition is genetically hetero-geneous, but the evidence for an X-linked formfully expressed in males is indisputable.
Phenotype in Males with X-linked Anhi-drotic Ectodermal Dysplasia. The phenotypein males results from an incomplete developmentof the epidermis and its appendages. A quantitative
I69
on 24 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.3.3.169 on 1 Septem
ber 1966. Dow
nloaded from

Kerr, Wells, and Cooper
deficiency in hair follicles due to hypoplasia orabsence of pilosebaceous structures is responsiblefor hypotrichosis. The dental defects are presumablycaused by failure of the dental lamina, an epithelialplate derived from ectoderm in the 7th week ofintrauterine life. Complete anodontia has beenrecorded (Thadani, I934; Battersby, I936; Thomaand Allen, 1940), but usually a few misshapen teethare formed, typically as conical structures in incisoror canine areas.The deficiency in epidermal sweat glands is
generally regarded as complete. However, underexperimental conditions of raised environmentaltemperature, and using a starch-iodine indicatormethod (Minor I927), slight sweating has beennoted in the axilla (Felsher, I944; Sackett, Marans,and Hursey, I956) and on the forehead (Everett,Jump, Sutherland, Savara, and Suher, I952) orchest (Felsher, I944). By contrast complete absenceof sweating has been reported under identicalconditions (Sunderman, I941; Lipton and Roberts,I950; Metson and Williams, 1952). Many skinbiopsies have been examined for sweat glandsgenerally with negative results. Most biopsies weretaken from the axilla, but negative findings havealso been recorded in serial sections of skin from theforehead (Spira, I947), palmar surfaces (Everettet al., 1952), sole of foot (Upshaw and Montgomery,1949), pubis (Clouston, I939), abdomen (Zeligs,1932), and forearm (Grant and Falls, I944). Sweatglands were demonstrated in deeper layers of thecutis by Sackett et al. (I956), whose patient alsosweated under experimental conditions. Dentalfeatures and deficiency of hair were far less markedthan usual in this patient, which raises the questionof a milder X-linked variety. Thannhauser (1936)described a similarly mild case. Sweat glands inforearm skin of a typical case were reported byRademaker (1933), but some doubt must be cast onthis finding because pilocarpine failed to producesweating which, as noted by others (Lord andWolfe, 1938), is convincing evidence for the absenceof sweat glands.
Lacrimation is generally normal but has beenrecorded as absent (Thurnam, I848; Sunderman,I94I) or diminished (Grant and Falls, I944).Scarcity of mucous glands in the nasopharynx(Upshaw and Montgomery, I949; Malagon andTaveras, I956) leads to atrophic rhinitis, and thedeficiency or absence of buccal glands in oral mucosa(Sackett et al., I956) may result in a troublesomelack of secretions. There is no deficiency ofsebaceous glands (which may undergo papulardegeneration (De Silva, 1939) ) or of apocrineglands (Upshaw and Montgomery, I949).
Mammary tissue may be defective (Clarke andMcCance, I934; Clouston, I939), presumably asa manifestation of the primary ectodermal disorder,and absent nipples were noted in an early report(Tendlau, I902). Tritsch (I963) has confirmed anormal karyotype in affected males.
Phenotype in Female Relatives. Femalerelatives of males with anhidrotic ectodermaldysplasia who were either carriers or hada 50% probability of heterozygosity have beenreported to show various manifestations of the gene.Partial anodontia was most commonly demon-strated (Battersby, I936; De Silva, 1939; Liptonand Roberts, 1950), and hypotrichosis is frequentlymentioned in older reports, though objectiveevidence is lacking (De Silva, 1939). Intolerance toheat was occasionally noted by some females(Stadler and Blackstone, 1942; Seagle, 1954), andRoberts (I929) wrote that three carriers from a largefamily 'were reported to have occasional patches onthe body which was smooth and in which the sweatglands did not function'.
Thadani (1934) mentioned hairless non-sweatingfemale relatives of males in the Hindu family firstrecorded by Darwin (I875) following a communica-tion by W. Wedderburn who noted that '. . . thedaughters are never affected though they transmitthe tendency to their sons'. Thadani's report wasentirely anecdotal and without further detailscannot be accepted as evidence of an anhidroticstate in heterozygous females. The same criticismapplies to Guilford's (I883) report of a maternalgrandmother who 'never had hair or teeth', andto a brief paper by Glass and Yost (I939) whomentioned two probably heterozygous female3 who'had never perspired and lacked mammary glands'.
Females with apparently congenital anhidrosisand ectodermal defects who were sporadic cases(Wagner, 1952) or had other similarly affectedfemale relatives (Lipscomb and Manonmani, 1952;Kline, Sidbury, and Richter, I959; Bernard et al.,I963) have been described. However, as mentionedabove, it is probable that such females are recipi-ents of other mutations.
Present InvestigationIf the assumptions of the inactive X chromosome
theory (Lyon, I96I) apply to the present locus,then a mosaic distribution of ectodermal defectswould be predicted in heterozygous females. Asearch for phenotype mosaicism was undertakenby a detailed study of two genetically proven
I70
on 24 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.3.3.169 on 1 Septem
ber 1966. Dow
nloaded from

Gene Effect in Carriers of Anhidrotic Ectodermal Dysplasia
heterozygous females, and more general examina- changes on contact with sweat were recorded photo-tion of several other proven or probable carriers. graphically on black-and-white and colour film.
Case Material and MethodsMost investigations were undertaken on members of
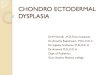
Family A (Fig. i). The family was ascertained throughan affected boy III.i, aged 4; his younger brother, III.3,was readily diagnosed at the age of 8 months by theeruption of typically pointed teeth, one in each uppercanine area. A male cousin III.5, aged 4, was alsoaffected. The heterozygous mothers II.2, aged 25, andII.4,aged 23,both daughters ofthe affected male I.i,werestudied extensively. Their daughters III.2, aged 3, andIII.4, aged 4, each with a half-chance of heterozygosity,were examined clinically.
FIG. I. Pedigree of Family A.
Two other heterozygotes were examined. One, aged3I (from Family B), was the daughter of an affected manand had a son with anhidrotic ectodermal dysplasia.The other woman, aged 26 (from Family C), had twosons with typical features of the trait, but the elder was
additionally affected with ichthyosis hystrix.The women who volunteered to act as controls for
sweat investigations were in good health and aged 24 and25 years.
Skin biopsies were obtained from the outer surface ofthe forearm. Sections were stained with haematoxylinand eosin, and with Verhoeff's and van Gieson's stain(the latter to demonstrate elastic fibres and collagen).
Studies on the distribution of sweating in heterozygousfemales and normal controls were undertaken by a
method which was basically that of Minor (1927), as
described by Kuno (1956) but using quinazarin com-
pound (quinazarin 2 : 6 disulphonic acid 28% (Gutt-mann, I940) ) instead of iodine as an indicator of skinmoisture. A colourless powder of the following com-
position: Quinazarin (Burroughs Wellcome), 35 g.;
Na2 CG3, 30 g.; starch, 6o g., was applied evenly witha fine brush over the face and entire body surface. Thesubject was then seated in an insulated and heated roomwith the feet and distal third of legs in hot water untila rectal temperature of 38-38.5o C. was reached. Colour
Results(i) Hair. No deficiency in scalp or body hair
was found. In particular, a careful examination offorearm and lower limb lanugo hair on heterozygousfemales A II.2 and II.4 failed to reveal patches ofhairless skin, though the possibility of a relativedeficiency could not be excluded in the case of II.2.
(ii) Teeth. Examination of teeth was oftenunsatisfactory because it was not possible to gain acomplete history of tooth extractions or to obtainradiographs of the jaws, and a diagnosis of partialanodontia is not reliable without information fromthese sources. Nevertheless, the following con-clusions could be drawn.
(a) Evidence suggestive of abnormal dentition.In family A the heterozygous female II.2 recalledan abnormally sharp and pointed deciduous toothin the upper canine area. At the second dentitioneach upper lateral incisor failed to erupt, and thewidely spaced central incisors were removed at9 years of age. Other teeth were subsequentlyextracted because of dental caries, but there was noevidence of absence or malformation of mandibularteeth. Her daughter appeared to have a normaldeciduous dentition. The other heterozygousfemale II.4 could not recall her deciduous teeth,but there was absence of at least three permanentteeth: left upper canine, lower lateral incisor, anda lower first premolar. Her daughter had a total ofi6 deciduous teeth. Those missing were bothupper central incisors and a left incisor and rightmolar in the lower jaw.The mother of two affected boys in family C
had absence of both upper lateral incisors and aprobable absence of a lower premolar, though thelatter may have been extracted along with severalother lower jaw teeth.
(b) Evidence of normal dentition. There was noindication of anodontia or abnormally formedteeth in the permanent dentition of the heterozygousfemale from family B.
(iii) Sweat glands.(a) Perception of sweating. With one exception
all adult females considered that they sweated in anormal manner and had not observed any regionallack of sweating, either during febrile illnesses,undergoing physical exertion, or in a hot environ-ment. The exception, A II.2, had noticed that herforearms remained dry when other areas weremoist with sweat.
I7I
on 24 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.3.3.169 on 1 Septem
ber 1966. Dow
nloaded from

Kerr, Wells, and Cooper
t=. ;' Ut ,
11 2 II 4-4ETEROZYGOUS FEMALES
f'-4
HETEROZYGSOUS -FEMAL.ES
.r}\ *Awa 1:
I,+ :L.
A BCONTRO FEMALES
.._.
CONT. FE A4A E S
2 ..S..I/"I I
I
i t 1
I' ..
yI
:.
E:2 11F.4HETEPOZYGOUS FEMALES
v;NN_
.I a-i
HETEROZYGOUS F-MAA,_-S-
!.AP,
;
('t())IA I
..... t.
B
ICOONTROL FEMALESL EALTC:iOL FEMAL E
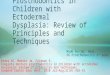
FIG. 2. Regional distribution of sweating induced by heat. Drawings made from black and white prints and colour transparencies.Dark areas represent purple change of quinazarin compound in situ. Stippling represents areas from which dye has been washed
by sweat.
\-\N I b
\-- 1--
. .'4
172
/ ---Iu
;5-- ,'A) A,1- .0.
T4
0. .0,.ft0
on 24 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.3.3.169 on 1 Septem
ber 1966. Dow
nloaded from

Gene Effect in Carriers of Anhidrotic Ectodermal Dysplasia
11.2 L.'> A 3
HETEROZYGOUS FEMALES CONTROL FEMALES
r1.2 11.4HETEROZYGOUS FEMALES
ACONTROL FEMALE
1. 2HETEROZYGOUS FEMALE
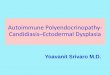
FIG. 3. Examples of photographically recorded colour changes in quinazarin compound.
(b) Distribution of sweating on the body surface.Colour changes in quinazarin compound on thebody surfaces of two heterozygous females II.2 andII.4 from family A and two normal females wererecorded photographically when the rectal tempera-ture reached 38-38-5sC. For comparative purposes,drawings were made from black-and-white printsand colour transparencies to illustrate distributionof dye on various areas of the body surface (Fig. 2).Examples of black-and-white photographs ofrepresentative areas are shown in Fig. 3. Thelatter prints provide a faithful record of areaswhere dark purple changes represented the effectsof sweating in situ. However, areas where dye hadbeen washed away by sweat could not be dis-tinguished clearly. Hence the use of colour trans-parencies in the construction of drawings becauseresidual light-red coloration or glistening andobviously moist skin could be recognized. Theselatter changes are represented by stippling on thedrawings.
As illustrated in Fig. 2, there was a differencein the extent of sweating for each class of female.The relatively localized distribution in heterozygousfemales was best demonstrated on the face, chest,and back. By contrast, much of the dye on theseareas in both controls had been washed away bysweat. Sweating localized to the left side of theforehead and neck, and more pronounced in theleft axilia, was found in heterozygote II.2. Theorder in which different regions began to sweat wassimilar for each class of female, though the onset ofcolour changes occurred after a longer period inheterozygotes. Emotional sweating, indicated bystaining in the axillae and on the palms beforethermal stimulation in both controls was not seenin either heterozygous female.
(c) Examination of skin sections for sweat glands.In order to establish the histological features in anaffected male from family A, sections were pre-pared from a biopsy specimen obtained from theouter surface of the forearm of I.i aged 6o. The
I73
on 24 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.3.3.169 on 1 Septem
ber 1966. Dow
nloaded from

Kerr, Wells, and Cooperepidermis appeared thinner than normal and theMalpighian layer was rudimentary. In all, 38 serialsections were examined for epidermal appendages.There was no evidence of glandular structures,sweat or sebaceous ducts, hair follices, and smoothmuscle. No abnormality of collagen and elasticfibres was detected in sections stained with Verhoeffand van Gieson.
Examinations were made on 48 serial sections ofskin from the forearm of each heterozygous femalein family A. The epidermis appeared entirelynormal in each case. No glandular elements, hairstructures, or smooth muscle were detected insections from II.2. By contrast, 3 sweat glands and3 sebaceous glands were found in the dermis ofII.4, together with muscle fibres of an arrectorpilae. Collagen and elastic fibres were normal ineach female.
(iv) Other Ectodermal Structures. No defectin nipples, or breast tissue (the latter primarily ofmesodermal origin) was observed in any female.
DiscussionPresent data were not sufficient to draw con-
clusions on the range of phenotypic variability inheterozygous females. However, observations onteeth suggested variation from normal dentition todegrees of partial anodontia and malformed teeth,which is in accordance with previous reports.Partial anodontia has been detected in randommembers of different normal populations with afrequency varying from 2% (Werther and Rothen-berg, I939) to about 6% (Grahnen, I962). Thesesurveys indicated that teeth were more frequentlymissing in the permanent dentition, and so theincomplete deciduous set of the female child A,III.4 (with a 50% genetical probability of heterozy-gosity) can be taken as evidence of the carrier state.The abnormally conical and pointed teeth found inaffected males and occasionally in heterozygousfemales are typical but not pathognomonic (Thomaand Allen, 1940) of the gene for anhidrotic ecto-dermal dysplasia.No obvious deficiency in the amount of scalp or
body hair was noted among females, nor were thereany apparent differences in hair distribution on eachside of the body in the heterozygous adults fromfamily A.The density of sweat glands varies considerably
over the body surface of normal people. Accordingto Kuno (I956) there are between I20 and 200active sweat glands per square centimetre of skinon the external surface of the forearm. Skin in this
area obtained from an affected male and theheterozygous female A, II.2, did not contain sweatglands, whereas 3 sweat glands and other epidermalappendages were found in the heterozygous femaleII.4. Sections obtained from the outer surface ofthe upper arm from 7 persons with normal skin(control material described elsewhere by Wells andKerr, I966) were used for comparison, becauseKuno (I956) demonstrated a similar density ofsweat glands in both areas. Sweat glands weredetected in 4 out of 7 normal skin sections (width5,u). No glandular structures were seen in 48sections (total width 0-2 mm.) of skin from theheterozygote II.2. An estimate of the probabilityof encountering a sweat gland in a given area ofskin is not justified because Kuno's work hasemphasized the irregular distribution of glands.Nevertheless, findings in heterozygote II.2 arehighly suggestive of a relative deficiency in an areaof skin where sweating was not detected subjectivelynor on experimental stimulation by heat.
Areas of thermal sweating were less extensive inheterozygous females, both by comparison withcontrol females and with data provided by Kuno(I956). The latter used a similar technique, largelyon male subjects, and demonstrated considerablevariation in the regional distribution of sweating.However, the distinct patchiness and unilateralsweating noted in the present heterozygotes hasnot been found in normal people. There was noevidence that more prolonged heat stimulationwould cause further sweating in heterozygotes. Asit was, experimental conditions were extended tothe point beyond which gross discomfort would beprovoked. The apparent delay in onset of sweatingrecorded for each heterozygote was probablydependent on the relative deficiency of active sweatglands. As Kuno has pointed out, the method isunsatisfactory for determining time of onsetbecause appearance of staining is influenced byseveral environmental factors.The results from sweat distribution tests on
heterozygous females were consistent with aquantitative defect of sweat glands. This wassupported by histological findings in one carrier,which together with the patchy distribution ofsweating is suggestive evidence of tissue mosaicism,as predicted on the inactive X chromosome theory.Superficially, relatively large areas of sweating andnon-sweating skin indicate a small number ofprecursor cells in existence at time of inactivation.Confirmation of this assumption requires moreprecise quantitation of active sweat glands, and itwas hoped to obtain such data by using the methodof Sutarman and Thomson (I952) for enumerating
174
on 24 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.3.3.169 on 1 Septem
ber 1966. Dow
nloaded from

Gene Effect in Carriers of Anhidrotic Ectodermal Dysplasia
individual sweat glands by impressions obtained inplastic media. However, estimates would bemeaningful only by comparison with a considerablebody of control information, and it was not possibleto amass sufficient data from normal females.The observed variation in dentition is also in
keeping with the assumptions of the inactiveX chromosome theory, but it is difficult to explainlack of gene effect on hair. Possibly, the gene
products controlled at the X-linked locus exert a
more generalized influence on hair formation. Inthis case, the presence of an active locus in a fewcells of the heterozygous female may be sufficientto maintain normal control, and hypotrichosiswould occur only if all normal allele-bearing Xchromosomes were inactive at the appropriate stage
in development.
SummaryPartial anodontia and diminished activity of
sweat glands were demonstrated in females hetero-zygous for anhidrotic ectodermal dysplasia.Results of thermally-induced sweating and his-tological examination of skin sections in carriersand controls indicated a quantitative deficiency ofsweat glands in the carriers. Together with thepatchy distribution of sweating these findings were
consistent with the inactive X chromosome theory.There was no obvious gene effect on the hair ofcarrier females.
REFERENCES
Battersby, J. (I936). Ectodermal dysplasia with complete anodontia.Dent. Mag. (Lond.), 53, 427.
Bernard, R., Giraud, F., Rouby, M., and Hartung, M. (i963).A propos de sept observations de dysplasie ectodermique chez dessujets de sexe feminin dont six dans la meme famille. Discussiongenetique. Arch. fran;. Pediat., 20, I051.
Brain, R. T. (I937). Familial ectodermal defect. Proc. roy. Soc. Med.,3I, 69.
Bruno, F. E., and Engelhardt, H. T. (I944). Hereditary ectodermaldysplasia. Ann. intern. Med., 20, I40.
Clarke, R. E., and McCance, R. A. (I 934). Familial sex-linkedectodermal dysplasia with incomplete forms. Arch. Dis. Childh.,
9, 39-Clouston, H. R. (I939). The major forms of hereditary ectodermal
dysplasia (with an autopsy and biopsies on the anhydrotic type).
Canad. med. Ass. J., 40, I.Cockayne, E. A. (I933). Inherited Abnormalities of the Skin and its
Appendages. Oxford University Press, London.Darwin, C. (i875). The Va-istion of Animals and Plants under
Domestication, 2nd ed., Vol. 2, p. 3I9. Murray, London.De Silva, P. C. C. (1939). Hereditary ectodermal dysplasia of
anhydrotic type. Quart. J. Med., 8, 97.
Everett, F. G., Jump, E. B., Sutherland, W. F., Savara, B. S., and
Suher, T. (I952). Anhidrotic ectodermal dysplasia withanodontia: a study of 2 families. Amer. dent. Ass., 44, 173.
Felsher, Z. (I944). Hereditary ectodermal dysplasia: report of a case
with experimental study. Arch. Derm. Syph. (Chic.), 49, 4IO.
Glass, L. C., and Yost, D. H. (I939). Inherited inability to sweat.Hered., 30, 477.
Grahnen, H. (I962). Hereditary factors in relation to dental cariesand congenitally missing teeth. In Genetics and Dental Health,ed. C. J. Witkop, p. I94. McGraw Hill, New York.
Grant, R., and Falls, H. F. (i944). Anodontia. Report of case
associated with ectodermal dysplasia of anhidrotic type. Amer.J. Orthodont., 30, 66i.
Guilford, S. H. (I883). A dental anomaly. Dent. Cosmos, 25, II3.Guttmann, L. (I940). Topographic studies of disturbances of sweat
secretion after complete lesions of peripheral nerves. Neurol.Psychiat., 3, 197.
Halperin, S. L., and Curtis, G. M. (1942). Anhidrotic ectodermaldysplasia associated with mental deficiency. Amer. ment. Defic.,46, 459.
Helweg-Larsen, H. F., and Ludvigsen, K. (1946). Congenitalfamilial anhidrosis and neurolabyrinthitis. Acta derm.-venereol.(Stockh.), 26, 489.
Kline, A. H., Sidbury, J. B., Jr., and Richter, C. P. (1959). Theoccurrence of ectodermal dysplasia and corneal dysplasia in one
family. J. Pediat., 55, 355.
Kuno, Y. (I956). Human Perspiration. Thomas, Springfield, Illinois.Levit, S. G. (I936). The problem of dominance in man. Genet.,
33, 4II.Lipscomb, L. L., and Manonmani, H. (1952). Hereditary ecto-
dermal dysplasia with report of 3 cases of the anhydrotic variety.Indian med. Ass., 21, 359.
Lipton, I., and Roberts, M. H. (I950). Hereditary ectodermaldysplasia of the anhidrotic type. Amer. Dis. Child., 79, 504.
Lord, L. W., and Wolfe, W. D. (1938). Hereditary ectodermaldysplasia of the anhidrotic type. Arch. Derm. Syph. (Chic.), 38,893.
Lyon, M. F. (I96I). Gene action in the X-chromosome of the mouse
(Mus musculus L.). Nature (Lond.), I90, 372.
Malagon, V., and Taveras, J. E. (I956). Congenital anhidroticectodermal and mesodermal dysplasia: report of 2 cases withatrichia and amastia. Arch. Derm., 74, 253.
Mallmann-Muhlberger, E., and Helwig, H. (I964). Familiare
ektodermale Dysplasie vom hidrotischen Typ. Ann. paediat.(Basel), 202, 358.
Metson, B. F., and Williams, B. K. (1952). Hereditary ectodermaldysplasia of the anhidrotic type: report of a case in a negro.
Pediat., 40, 303.
Minor, V. (1927). Cited by Kuno (I956).Mohler, D. N. (I959). Hereditary ectodermal dysplasia of the
anhidrotic type associated with primary hypogonadism. Amer.
J. Med., 27, 682.Rademaker, G. A. (I933). Congenital (hereditary) dysplasia of the
ectoderma. Acta paediat. (Uppsala), I5, 57.
Roberts, E. (I929). The inheritance of anhidrosis associated withanadontia. 7. Amer. med. Ass., 93, 277.
Sackett, L. M., Marans, A. E., and Hursey, R. J. (1956). Congenitalectodermal dysplasia of the anhidrotic type. Oral Surg., 9, 659.
Seagle, J. B. (I954). Anhidrotic hereditary ectodermal dysplasia:report of 2 cases in a brother and sister. Pediat., 45, 688.
Spira, L. (1947). Congenital ectodermal dysplasia. Acta med. scand.,127, 570-
Stadler, H., and Blackstone, C. H. (1942). Hereditary ectodermal
dysplasia of the anhidrotic type. A report of 2 cases. 7. Pediat.,
21, 229.
Sunderman, F. W. (I941). Persons lacking sweat glands: hereditaryectodermal dysplasia of the anhidrotic type. Arch. intern. Med.,
67, 846.Sutarman, a-id Thomson, M. L. (I952). A new technique for
enumerating active sweat glands in man. 7. Physiol. (Lond.), 117,
5'.Tendlau, B. (19n2). Ueber angeborene und erworbene Atrophia cutis
idiopathica. Virchows Arch. path. Anat., 167, 465.
Thadani, K. I. (I934). The toothless man of Sind. 7. Hered., 25, 483.
Thannhauser, S. J. (1936). Hereditary ectodermal dysplasia of the
"anhidrotic type" with symptoms of adrenal medulla insufficiency
and with abnormalities of the bones of the skull. Amer. med.
Ass., Io6, 9D8.Thoma, K. H., and Allen, F. W. (1940). Anodontia with ectodermal
dysplasia. Amer. Orthodont., 26, 503.
Thurnam, J. (I848). Two cases in which the skin, hair and teeth
were very imperfectly developed. Med.-chir. Trans., 31, 71.
I75
on 24 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.3.3.169 on 1 Septem
ber 1966. Dow
nloaded from

Kerr, Wells, and Cooper
Tritsch, H. (I963). Cytogenetische Untersuchungen bei versch-iedenen dermatologischen und andrologischen Krantheitsbildern.Z. Haut-u. Geschl. Kr., 34, 329.
Upshaw, B. Y., and Montgomery, H. (I949). Hereditary anhidroticectodermal dysplasia: a clinical and pathologic study. Arch.Derm. Syph. (Chic.), 60, II70.
Wagner, H. N., Jr. (1952). Electrical skin resistance studies in twopersons with congenital absence of sweat glands. ibid., 65, 543.
Weech, A. A. (1929). Hereditary ectodermal dysplasia (congenital
ectodermal defect). Amer. J. Dis. Child., 37, 766.Wells, R. S., and Kerr, C. B. (I966). The histology of ichthyosis.
J. invest. Derm. In the press.Werther, R., and Rothenberg, F. (1939). Anodontia. Amer.
Orthodont., 25, 6I.White, A. G. (I964). Hereditary ectodermal dysplasia with
megaloblastic anaemia. Brit. J. clin. Pract., I8, 54I.Zeligs, M. (1932). Hereditary ectodermal dysplasia, anhidrotic type.Amer. J. Dis. Child., 44, 394.
I76
on 24 May 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.3.3.169 on 1 Septem
ber 1966. Dow
nloaded from