Embed Size (px)
Citation preview

Gender and Place of Death from Coronary ArteryDisease in Washington State
Charles Maynard, PhD
Men may be more likely than women to die outsidethe hospital from coronary artery disease, whereaswomen may be as likely as men to die inside thehospital. This study used Washington State deathrecords to compare death rates from coronary arterydisease inside and outside the hospital for womenand men from 1980 to 2001. For in-hospital deaths,the men:women ratio of deaths was 1.6 in 1980and 2001; for out-of-hospital deaths, the ratio de-creased slightly from 2.6 in 1980 to 2.3 in 2001.These findings support the contention that, despitesignificant decreases in mortality, men continue tohave higher rates of death outside and inside thehospital than do women, although there has been aslight decrease in male:female mortality for deathsoutside the hospital. �2004 by Excerpta Medica,Inc.
(Am J Cardiol 2004;93:1286–1288)
Even with significant decreases in death rates, car-diovascular disease remains the current leading
cause of death for women and men in the UnitedStates.1 Coronary artery disease (CAD) also continuesto be an important cause of death for women and men,although men are more likely to die outside the hos-pital and women are as likely or more likely to dieinside the hospital.2 This study compared CAD deathrates inside and outside the hospital for women andmen in Washington State from 1980 to 2001. It washypothesized that death rates outside the hospitalwould be lower for women and that death rates insidethe hospital would be similar between men andwomen.
• • •This report is based on death records obtained in
electronic form from the Washington State Depart-ment of Health. From 1980 to 2001, there were857,440 deaths in Washington State; in 203,009 ofthese deaths (24%), CAD was the underlying cause.From 1980 to 1998, CAD as the underlying cause ofdeath was defined by the International Classificationof Diseases-Ninth Revision codes 410 to 414 and429.2; from 1999 to the present, the InternationalClassification of Diseases-Tenth Revision codes I21to I25 and I51.6 were definitive of CAD. Evidence has
suggested that diagnosis of CAD as the underlyingcause of death is comparable in the 2 systems.3
From the electronic death record, year of death,type of facility where death occurred, decedent age,gender, race, education, marital status, and whetherthe patient smoked in the past 15 years were obtained.Age was classified as �50, 50 to 64, 65 to 74, 75 to84, and �85 years old. Race was categorized as whiteor nonwhite, and education was defined as whether thedecedent graduated from high school. The type offacility where death occurred was classified as home(n � 55,571), other place (n � 9,101), in transport (n� 416), emergency department (n � 11,618), hospital(n � 76,704), or nursing home including hospice (n �49,507). For purposes of this study, place of death wasdefined as inside the hospital (i.e., hospital or nursinghome) or outside the hospital (i.e., all other locations).There were 92 patients whose place of death wasunknown. This report includes 203,009 patients �20years of age.
Baseline characteristics of women and men werecompared with the 2-sample t test for continuous ageand the chi-square statistic for categorical variables,such as race. Age-specific death rates were calculatedby dividing the number of deaths in given age andgender categories by the population number in Wash-ington State in those categories. Washington Statepopulation estimates by age and gender for the years1980 to 2001 were provided by the Washington StateDepartment of Health. Age-adjusted death rates werecalculated using the direct method of standardization,with the 2000 United States population as the stan-dard. Annual death rates for women and men werecompared with the Wilcoxon rank-sum test. Poisson’sregression was used to examine the effects of age,gender, and year of death on 440 separate death ratesconstructed from 22 years of data, 5 age categories,gender (women vs men), and death outside the hospi-tal (yes vs no). Analyses were conducted separatelyfor deaths inside and outside the hospital.
Overall, 45% of deaths occurred in women and38% were outside the hospital. Among women, 31%died outside the hospital as opposed to 44% of men (p�0.0001). As presented in Table 1, women wereolder, less likely to be married, and less likely to havesmoked in the 15 years before death.
Age-adjusted death rates for women and men ac-cording to place of death are shown in Figures 1 and2. For deaths inside the hospital, rates for women andmen decreased over time; overall rates decreased 56%for both men and women (Figure 1). The difference indeath rates over the 22-year period was statisticallysignificant (p �0.0001 by Wilcoxon rank-sum test),and the male:female death rate was 1.6 in 1980 and
From the Department of Veterans Affairs Puget Sound HealthcareSystem and the Department of Health Services, University of Wash-ington, Seattle, Washington. Dr. Maynard’s address is: Department ofVeterans Affairs, Health Services Research and Development (152),1660 S. Columbian Way, Seattle, Washington 98108. E-mail:[email protected]. Manuscript received November 13,2003; revised manuscript received and accepted February 3, 2004.
1286 ©2004 by Excerpta Medica, Inc. All rights reserved. 0002-9149/04/$–see front matterThe American Journal of Cardiology Vol. 93 May 15, 2004 doi:10.1016/j.amjcard.2004.02.016
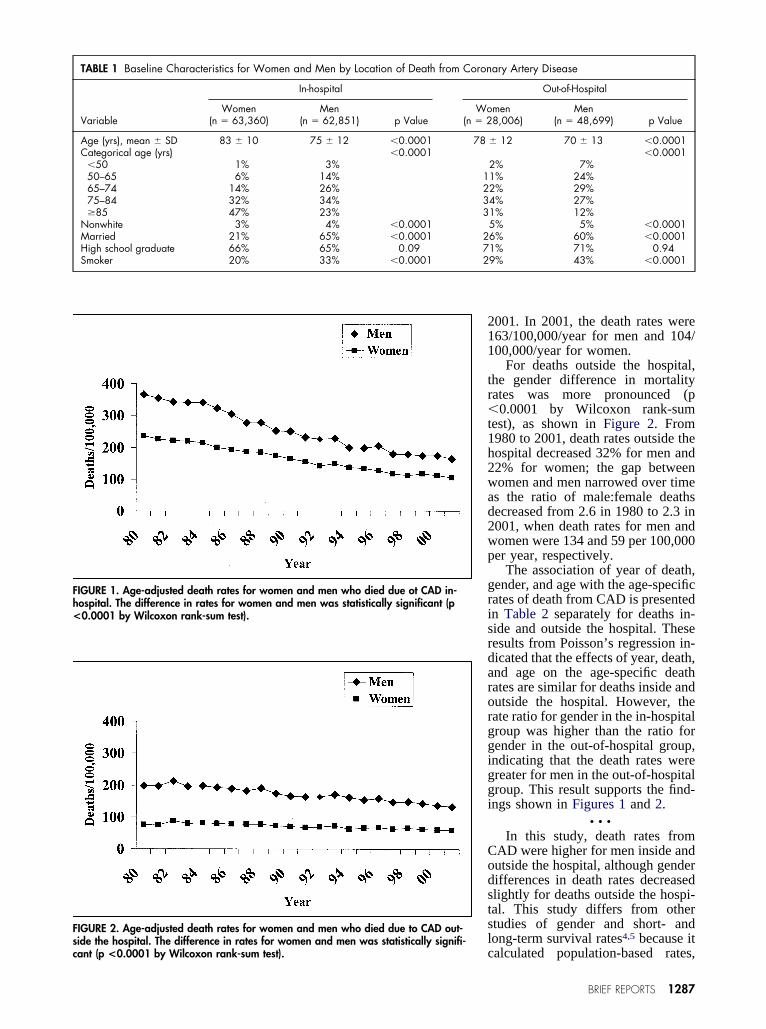
2001. In 2001, the death rates were163/100,000/year for men and 104/100,000/year for women.
For deaths outside the hospital,the gender difference in mortalityrates was more pronounced (p�0.0001 by Wilcoxon rank-sumtest), as shown in Figure 2. From1980 to 2001, death rates outside thehospital decreased 32% for men and22% for women; the gap betweenwomen and men narrowed over timeas the ratio of male:female deathsdecreased from 2.6 in 1980 to 2.3 in2001, when death rates for men andwomen were 134 and 59 per 100,000per year, respectively.
The association of year of death,gender, and age with the age-specificrates of death from CAD is presentedin Table 2 separately for deaths in-side and outside the hospital. Theseresults from Poisson’s regression in-dicated that the effects of year, death,and age on the age-specific deathrates are similar for deaths inside andoutside the hospital. However, therate ratio for gender in the in-hospitalgroup was higher than the ratio forgender in the out-of-hospital group,indicating that the death rates weregreater for men in the out-of-hospitalgroup. This result supports the find-ings shown in Figures 1 and 2.
• • •In this study, death rates from
CAD were higher for men inside andoutside the hospital, although genderdifferences in death rates decreasedslightly for deaths outside the hospi-tal. This study differs from otherstudies of gender and short- andlong-term survival rates4,5 because itcalculated population-based rates,
TABLE 1 Baseline Characteristics for Women and Men by Location of Death from Coronary Artery Disease
Variable
In-hospital Out-of-Hospital
Women(n � 63,360)
Men(n � 62,851) p Value
Women(n � 28,006)
Men(n � 48,699) p Value
Age (yrs), mean � SD 83 � 10 75 � 12 �0.0001 78 � 12 70 � 13 �0.0001Categorical age (yrs) �0.0001 �0.0001
�50 1% 3% 2% 7%50–65 6% 14% 11% 24%65–74 14% 26% 22% 29%75–84 32% 34% 34% 27%�85 47% 23% 31% 12%
Nonwhite 3% 4% �0.0001 5% 5% �0.0001Married 21% 65% �0.0001 26% 60% �0.0001High school graduate 66% 65% 0.09 71% 71% 0.94Smoker 20% 33% �0.0001 29% 43% �0.0001
FIGURE 1. Age-adjusted death rates for women and men who died due ot CAD in-hospital. The difference in rates for women and men was statistically significant (p<0.0001 by Wilcoxon rank-sum test).
FIGURE 2. Age-adjusted death rates for women and men who died due to CAD out-side the hospital. The difference in rates for women and men was statistically signifi-cant (p <0.0001 by Wilcoxon rank-sum test).
BRIEF REPORTS 1287

whereas most investigations have used populations ofpatients hospitalized with CAD and have not includedthose who died outside the hospital. The study byTunstall-Pedoe et al2 is an exception because it ascer-tained mortality before and during hospitalization formyocardial infarction. These results are consistentwith those from the Atherosclerosis Risk in Commu-nities study,6 which reported greater decreases fordeath rates due to CAD inside than outside the hospital inpatients hospitalized with acute myocardial infarction.However, death rates outside the hospital were higherthan those inside the hospital in that study.6
This study reports an observation and does notexplain why death rates outside the hospital werehigher in men or why gender differences in mortalityoutside the hospital have attenuated over the years.Moreover, it relies on death records that may notalways be accurate in assigning the underlying causeof death or the location of death, although reliabilityfor the latter was 88% in 1 study.7 The validity ofdeath records can change over time and may be sub-ject to changes in medical practice, such as shorter
lengths of hospital stay. Neverthe-less, the electronic death record is arepresentation of the death certifi-cate, the official document that ex-plains the circumstances of death.Also, this study is from a single statewith a predominantly white popula-tion, leading to the question of howapplicable these findings are. How-ever, the large number of deaths re-ported in this study lends credence tothese findings and supports the con-
tention that the gender difference is particularly evi-dent in deaths due to CAD outside the hospital.
1. American Heart Association. Heart Disease and Stroke Statistics—2004 Up-date. Dallas: American Heart Association, 2003:8.2. Tunstall-Pedoe H, Morrison C, Woodward M, Fitzpatrick B, Watt G. Sexdifferences in myocardial infarction and coronary death in the Scottish MONICApopulation of Glasgow 1985 to 1991: presentation, diagnosis, treatment, and28-day case fatality of 3991 events in men and 1551 events in women. Circula-tion 1996;93:1981–1992.3. Anderson RN, Minino AM, Hoyert DL, Rosenberg HM. Comparability ofcause of death between ICD-9 and ICD-10: preliminary estimates. Natl Vital StatRep 2003;49:6.4. Vaccarino V, Parsons L, Every NR, Barron HV, Krumholz HM. Sex-baseddifferences in early mortality after myocardial infarction. N Engl J Med 1999;341:217–225.5. Maynard C, Litwin PE, Martin JS, Weaver WD. Association of gender andsurvival in patients with acute myocardial infarction. Arch Intern Med 1997;157:1379–1384.6. Rosamond WD, Chambliss LE, Folsom AR, Cooper LS, Conwill DE, Clegg L,Wang CH, Heiss G. Trends in the incidence of myocardial infarction and inmortality due to coronary heart disease, 1987 to 1994. N Engl J Med 1998;339:861–867.7. Poe GS, Powell-Griner E, McLaughlin JK, Placek PJ, Thompson GB, Robin-son K. Comparability of the death certificate and the 1986 National MortalityFollowback Survey. National Center for Health Statistics. Vital Health Stat1993;2:10–12.
Educational Attainment and Myocardial Infarct-Related Congestive Heart Failure (The Determinants of
Myocardial Infarction Onset Study)
Kenneth J. Mukamal, MD, MPH, MA, Malcolm Maclure, ScD, James E. Muller, MD,Jane B. Sherwood, RN, and Murray A. Mittleman, MD, DrPH
We assessed educational attainment and complica-tions during hospitalization in 3,882 patients with
acute myocardial infarction for the Determinants ofMyocardial Infarction Onset Study. Educational at-tainment had a graded, inverse association withprevalence of congestive heart failure (CHF) duringhospitalization, with the lowest prevalence amongpatients who attended college (odds ratio 0.75; 95%confidence interval, 0.57 to 0.99; p for trend 0.02),with similar findings among men, women, whites,and blacks. �2004 by Excerpta Medica, Inc.
(Am J Cardiol 2004;93:1288–1291)
To determine the association of educational attain-ment with congestive heart failure (CHF) compli-
cating acute myocardial infarction (AMI), we studiedpatients enrolled in the Determinants of Myocardial
From the Divisions of General Medicine and Primary Care and Car-diology, Department of Medicine, Beth Israel Deaconess MedicalCenter; Departments of Epidemiology and Health and Social Behav-ior, Harvard School of Public Health; and Division of Cardiology,Department of Medicine, Massachusetts General Hospital, Boston,Massachusetts. This study was supported by Grant HL41016 from theNational Heart, Lung, and Blood Institute, Bethesda, Maryland; GrantK23AA00299 from the National Institute on Alcohol Abuse andAlcoholism, Bethesda, Maryland; and Grant 9630115N from theAmerican Heart Association, Dallas, Texas. Dr. Mukamal’s address is:Beth Israel Deaconess Medical Center, 330 Brookline Avenue,RO-114, Boston, Massachusetts 02215. E-mail: [email protected]. Manuscript received November 19, 2003; re-vised manuscript received and accepted February 2, 2004.
TABLE 2 Association of Year of Death, Gender, and Age With Age-specific DeathRates for Coronary Artery Disease: Results from Poisson Regression*
Variable
Rate-Ratio (95% confidence interval)
In-hospital Out-of-Hospital
Yr of death (/yr) 0.9586 (0.9577–0.9594) 0.9797 (0.9786–0.9808)Women 0.6157 (0.6089–0.6226) 0.3949 (0.3891–0.4008)Age (/10 yr increase) 1.1366 (1.1361–1.1371) 1.1037 (1.1032–1.1043)
1288 ©2004 by Excerpta Medica, Inc. All rights reserved. 0002-9149/04/$–see front matterThe American Journal of Cardiology Vol. 93 May 15, 2004 doi:10.1016/j.amjcard.2004.02.017


















