Embed Size (px)
Citation preview

18 Mich. St. U. J. Med. & L. 1
Michigan State University Journal of Medicine & Law
Spring, 2014
GAUGING THE HEARTBEAT OF E-PRESCRIPTIONS? - A RETROSPECTIVE ANALYSIS
Samuel D. Hodge, Jr.1 Allison Kilcourse2
Copyright © 2014 Michigan State University Journal of Medicine & Law; Samuel D. Hodge, Jr. and Allison Kilcourse
The desire to take medicine is perhaps the greatest feature which distinguishes man from animals.
---Sir William Osler
(1849 -1919) I. Statistical Overview 3
II. Medication Errors 4
III. Pharmacist Liability 5
IV. Physician Liability 6
V. The E-Prescription Process 7
VI. E-Prescriptions and the Government 9
VII. Electronic Prescriptions and the Private Sector 11
VIII. The Disadvantages of E-Prescriptions 12
A. State Responses to Electronic Prescriptions 16
1. General E-Prescription Laws 16
2. Controlled Substances 20
IX. Cases Involving E-Prescriptions 22
A. Administrative Rulings 22
B. Criminal Cases 23
C. Malpractice 25
X. Conclusion 26
Medicine has undergone a major transformation in the way routine business is transacted. This metamorphous is primarily the result of
converting paper charts into electronic medical records.3 The government has invested *2 heavily in this digital conversion by providing
financial incentives and imposing penalties to encourage its implementation.4 This incentive program included the conversion to digital
prescriptions.5 “[A] record 788 million prescriptions were routed electronically in 2012,” and this number will only increase with time.6
E-prescription7 is a computer generated system that allows physicians to electronically transmit medication orders “directly to a pharmacy
from the point-of-care.”8 The inclusion of electronic prescribing9 in the Medicare Modernization Act of 2003 provided the impetus for this
change, and the Institute of Medicine's report in 2006 on the role of e-prescribing in reducing medication mistakes received much publicity,
helping to promote awareness of e-prescribing's role in improving patient safety.10
*3 Compared to paper or fax prescriptions, e-prescribing improves medication safety, improve[s] prescribing accuracy and efficiency,
increase[s] practice effectiveness while improving health care quality and reducing health care costs.11
This article will explore the issues involving e-prescriptions and will examine whether the touted benefits of the system have come to fruition.
I. Statistical Overview
There has been a significant increase in the issuance of medication recently because of the development of new drugs and the need to care
for the elderly.12 One merely has to look at the growth of pharmacies in local neighborhoods to appreciate this fact. Whether these
businesses are stand-alone stores or branches in supermarkets, pharmacies are dominate fixtures in the landscape. This development is not
surprising because the vast majority of individuals take at least one pill on a daily basis, and more than one quarter of the population ingests
five pills or more.13 Those over 65 are the biggest consumers of drugs, and the use of multiple medications has risen during the past
decade.14 “In any given week 56% of children are taking at least one medication and 27% take two or more; 21% use at least one
prescription drug.”15 Therefore, it is not surprising that there are a number of problems associated with the issuance and consumption of
drugs.
According to the Department of Heath and Human Services, a study commissioned by the National Association of Chain Drug Stores
concluded that employees of drug stores place over 150 million calls to physicians each year to discuss perceived medication mistakes or to
obtain an explanation of prescription orders.16
Handwriting medication orders can be unproductive because of the frequent need to contact heath care providers over poor penmanship,
and having to re-enter the information required to satisfy federal and state reporting requirements. *4 17 An ancillary problem is that the sick
are inconvenienced by wasting time while their prescriptions are filled.18
II. Medication Errors
Medication is an amazing supplement for improving health. It can be utilized to “cure infectious diseases, prevent problems from chronic
diseases, and ease pain. But medicines can also cause harmful reactions if not used properly. Errors can happen in the hospital, at the
doctor's office, at the pharmacy, or at home.”19
A medication error is defined as follows:
Any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the
health care professional, patient, or consumer. Such events may be related to professional practice, health care products, procedures, and
systems, including prescribing order communication, product labeling, packaging, and nomenclature; compounding; dispensing; distribution;
administration; education; monitoring; and use.20
It is not surprising, therefore, that medication errors injure “at least 1.5 million people every year.”21 In fact, it is estimated that “at least one
medication error per hospital patient, per day occurs,” and “400,000 preventable drug-related injuries happen each year.”22 Further, “800,000
medication errors also occur in long-term care settings and about 530,000 occur among Medicare patients.”23
The National Academy of Sciences has enumerated several ways to decrease mistakes. The first recommendation calls for improving
patient-provider partnerships while encouraging consumers to become active partners in their own care.24 New and improved drug
information resources are called for as well, with improved web sites to “serve as a centralized source of comprehensive, objective, and
easy-to-understand information about drugs for consumers” and improved “drug naming, labeling, and packaging.”25
The most prominent of these recommendations, however, is the implementation of e-prescriptions. “Studies indicate that paper-based
prescribing is *5 associated with high rates of error.”26 “Electronic prescribing is safer because it eliminates problems with handwriting
legibility and, when combined with decision-support tools, automatically alerts prescribers to possible drug interactions, allergies, and other
potential problems.”27
III. Pharmacist Liability
Pharmacists are not immune from lawsuits over medication errors even though a health care provider issues the prescription. “Generally, a
pharmacist does not generally have a duty to question a judgment made by a physician as to the propriety of a prescription,” but “a
pharmacist does have a duty to be alert for clear errors28 and mistakes with a prescription.”29 Clear errors include, “obvious lethal doses;
inadequacies in the instructions; known contraindications; or incompatible prescriptions.”30 The extent to which particular jurisdictions hold a
pharmacist liable varies.31 For instance, “[s]ome courts have recognized the duty of a pharmacy to read prescriptions and be aware of patent
inadequacies in the instructions as to the maximum safe dosage of known toxic drugs and medicines”; however, other courts have noted that
“a pharmacist has no common law or statutory duty to refuse a prescription simply because it is for a quantity beyond that normally
prescribed or to warn the patient's physician of that fact.”32Additionally, “[t]he Omnibus Budget Reconciliation Act (OBRA) of 1990 expanded
the pharmacist's role in reducing the risks of prescribed drugs by requiring that they counsel Medicaid recipients.”33
*6 If a claim is brought against a pharmacist, three approaches can be used by the plaintiff:
first, they can request the claim to assert that a reasonable pharmacist concerned about the safety and efficacy of the prescribed drug has a
duty to communicate with the prescribing doctor Second, if the state has passed a statute or regulation specifically imposing a duty on
pharmacists to warn or counsel, plaintiffs can invoke that law as defining a new standard of care for pharmacists Third, plaintiffs can argue
that these earlier decisions present[[[] a standard-of-care question for the jury, one that turns on the facts of particular cases.34
Regardless of specific case law, it is widely accepted that a pharmacist has a duty to accurately fill a prescription.35 While this requirement
has been upheld in a number of cases,36 other courts have held that “the pharmacist has no duty to caution the patient of the possible
undesirable effects of the drug, absent special circumstances or neglect.”37
IV. Physician Liability
Medication errors by physicians can occur in a variety of ways, ranging from the writing of the initial prescription to the administration of the
drug. Obviously, a person may be injured if the physician prescribes the wrong medication or the doctor misdiagnosis the medical issue and
prescribes the wrong medicine.
The list of possible mistakes and errors seems endless; however, the most common error involves the dosage - the patient is provided with
either too little or too much of a drug.38Prescriptions mistakes can be fatal and are *7 traditionally caused by a doctor's inadequate
understanding of a drug's use, prescriptions that are hard to read, or medication errors attributable to drugs that have similar sounding
names.39
V. The E-Prescription Process
The high incidence of an adverse drug event is not surprising considering the complexity of medical care.40 Because of the claimed ability to
reduce medication orders that are hard to read, e-prescriptions are advocated as a method to eliminate this problem. After all, this new
electronic system is able to provide the doctor with an automated warning system at the time the prescription is issued while the doctor is
able to view the medical records of the patient.41 The pharmacy is aided by the smaller number of medication errors that require clarification
and the elimination of paper prescriptions. These benefits allow the druggist to spend more time with the customer.42
The e-prescription system relies upon computers and their data entry abilities.43 A basic system will include the necessary e-prescribing
software and internet connection between the heath care provider and pharmacy.44 The American College of Rheumatology notes that the
system has the advantage of allowing a doctor to electronically review the patient's health insurance coverage and medication history and
sending the prescription over the internet directly to the patient's pharmacy.45 It also allows the pharmacy to electronically notify the physician
when the medication has to be renewed.46
The digital transmission process starts when the patient and doctor discuss the current problems and treatment options. As the electronic
prescription *8 is typed, the e-prescribing system links electronically to a hub to ascertain whether the person is eligible for payment of the
medication.47 The patient's up-to-date medication history is then displayed to the doctor at the point-of-care.48 This is reviewed along with
clinical alerts, prescription history, eligibility, and prior authorization information, followed by the physician choosing the therapy and verifying
the patient's pharmacy of choice.49 Once the prescription is completed, the e-script is sent to the pharmacy. The druggist then fills the
prescription and sends a fill acknowledgment to the physician.50
Converting to an electronic prescription system, however, is not without its financial costs.51 The first step requires a choice between a stand-
alone or e-prescribing within an electronic medical records system or EMR.52 A stand-alone system is cheaper and easier to install. However,
it may not have the full performance abilities of an electronic medical records system.53 Additional factors that go into the selection process
include the cost of a wireless network, the price of the hardware, licensing fees for the software and the conversion cost of transferring the
existing records to the electronic system. Other considerations include networking costs, such as Internet connectivity, wireless network,
practice management system integration into the new system; hardware costs such as desktops, laptops, servers, and printers; software
licensing costs and future upgrades; yearly fees, such as subscription or licensing costs; training and support; transferring records from the
existing system to the new one; and creating communication procedures between the current office equipment and the e-prescribing
system.54
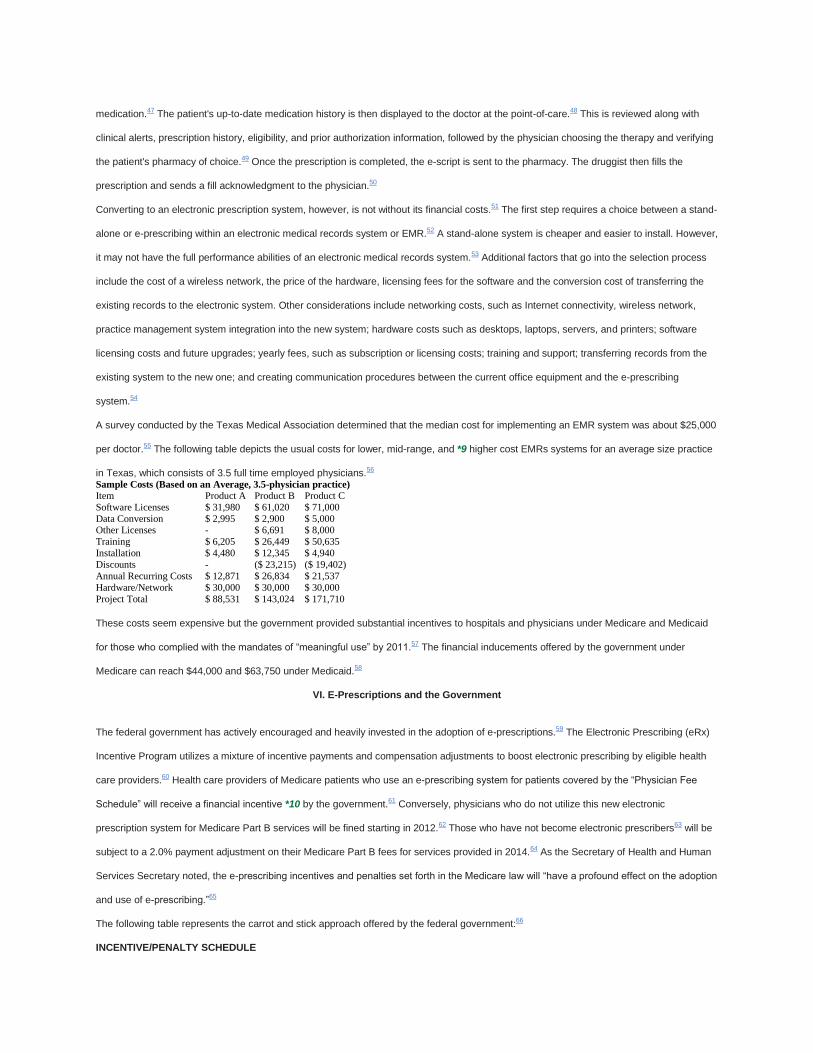
A survey conducted by the Texas Medical Association determined that the median cost for implementing an EMR system was about $25,000
per doctor.55 The following table depicts the usual costs for lower, mid-range, and *9 higher cost EMRs systems for an average size practice
in Texas, which consists of 3.5 full time employed physicians.56 Sample Costs (Based on an Average, 3.5-physician practice)
Item Product A Product B Product C
Software Licenses $ 31,980 $ 61,020 $ 71,000
Data Conversion $ 2,995 $ 2,900 $ 5,000 Other Licenses - $ 6,691 $ 8,000
Training $ 6,205 $ 26,449 $ 50,635
Installation $ 4,480 $ 12,345 $ 4,940
Discounts - ($ 23,215) ($ 19,402)
Annual Recurring Costs $ 12,871 $ 26,834 $ 21,537
Hardware/Network $ 30,000 $ 30,000 $ 30,000
Project Total $ 88,531 $ 143,024 $ 171,710
These costs seem expensive but the government provided substantial incentives to hospitals and physicians under Medicare and Medicaid
for those who complied with the mandates of “meaningful use” by 2011.57 The financial inducements offered by the government under
Medicare can reach $44,000 and $63,750 under Medicaid.58
VI. E-Prescriptions and the Government
The federal government has actively encouraged and heavily invested in the adoption of e-prescriptions.59 The Electronic Prescribing (eRx)
Incentive Program utilizes a mixture of incentive payments and compensation adjustments to boost electronic prescribing by eligible health
care providers.60 Health care providers of Medicare patients who use an e-prescribing system for patients covered by the “Physician Fee
Schedule” will receive a financial incentive *10 by the government.61 Conversely, physicians who do not utilize this new electronic
prescription system for Medicare Part B services will be fined starting in 2012.62 Those who have not become electronic prescribers63 will be
subject to a 2.0% payment adjustment on their Medicare Part B fees for services provided in 2014.64 As the Secretary of Health and Human
Services Secretary noted, the e-prescribing incentives and penalties set forth in the Medicare law will “have a profound effect on the adoption
and use of e-prescribing.”65
The following table represents the carrot and stick approach offered by the federal government:66
INCENTIVE/PENALTY SCHEDULE
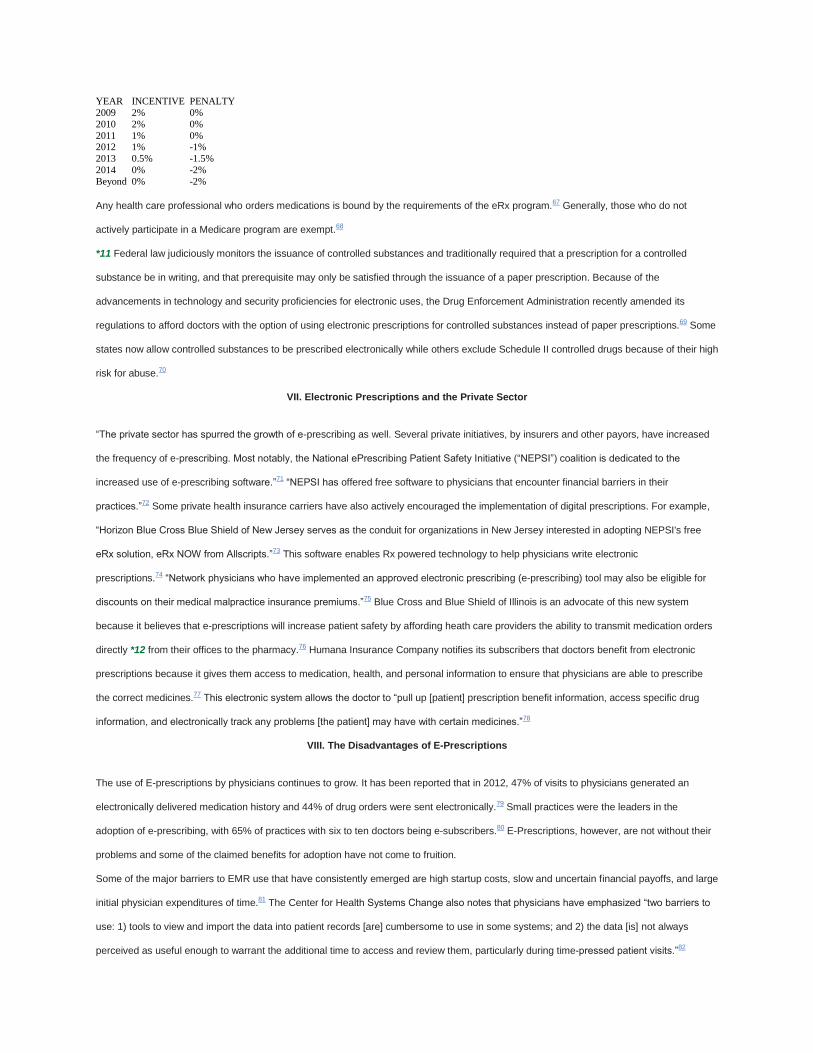
YEAR INCENTIVE PENALTY
2009 2% 0%
2010 2% 0%
2011 1% 0% 2012 1% -1%
2013 0.5% -1.5%
2014 0% -2%
Beyond 0% -2%
Any health care professional who orders medications is bound by the requirements of the eRx program.67 Generally, those who do not
actively participate in a Medicare program are exempt.68
*11 Federal law judiciously monitors the issuance of controlled substances and traditionally required that a prescription for a controlled
substance be in writing, and that prerequisite may only be satisfied through the issuance of a paper prescription. Because of the
advancements in technology and security proficiencies for electronic uses, the Drug Enforcement Administration recently amended its
regulations to afford doctors with the option of using electronic prescriptions for controlled substances instead of paper prescriptions.69 Some
states now allow controlled substances to be prescribed electronically while others exclude Schedule II controlled drugs because of their high
risk for abuse.70
VII. Electronic Prescriptions and the Private Sector
“The private sector has spurred the growth of e-prescribing as well. Several private initiatives, by insurers and other payors, have increased
the frequency of e-prescribing. Most notably, the National ePrescribing Patient Safety Initiative (“NEPSI”) coalition is dedicated to the
increased use of e-prescribing software.”71 “NEPSI has offered free software to physicians that encounter financial barriers in their
practices.”72 Some private health insurance carriers have also actively encouraged the implementation of digital prescriptions. For example,
“Horizon Blue Cross Blue Shield of New Jersey serves as the conduit for organizations in New Jersey interested in adopting NEPSI's free
eRx solution, eRx NOW from Allscripts.”73 This software enables Rx powered technology to help physicians write electronic
prescriptions.74 “Network physicians who have implemented an approved electronic prescribing (e-prescribing) tool may also be eligible for
discounts on their medical malpractice insurance premiums.”75 Blue Cross and Blue Shield of Illinois is an advocate of this new system
because it believes that e-prescriptions will increase patient safety by affording heath care providers the ability to transmit medication orders
directly *12 from their offices to the pharmacy.76 Humana Insurance Company notifies its subscribers that doctors benefit from electronic
prescriptions because it gives them access to medication, health, and personal information to ensure that physicians are able to prescribe
the correct medicines.77 This electronic system allows the doctor to “pull up [patient] prescription benefit information, access specific drug
information, and electronically track any problems [the patient] may have with certain medicines.”78
VIII. The Disadvantages of E-Prescriptions
The use of E-prescriptions by physicians continues to grow. It has been reported that in 2012, 47% of visits to physicians generated an
electronically delivered medication history and 44% of drug orders were sent electronically.79 Small practices were the leaders in the
adoption of e-prescribing, with 65% of practices with six to ten doctors being e-subscribers.80 E-Prescriptions, however, are not without their
problems and some of the claimed benefits for adoption have not come to fruition.
Some of the major barriers to EMR use that have consistently emerged are high startup costs, slow and uncertain financial payoffs, and large
initial physician expenditures of time.81 The Center for Health Systems Change also notes that physicians have emphasized “two barriers to
use: 1) tools to view and import the data into patient records [are] cumbersome to use in some systems; and 2) the data [is] not always
perceived as useful enough to warrant the additional time to access and review them, particularly during time-pressed patient visits.”82
While these are understandable issues and most likely represent short term problems, prescription errors persist with the digital systems.
Surprisingly, e-prescriptions are not error free with a mistake rate that is comparable to the traditional handwritten order.83 For instance, an
error rate of more than sixty *13 percent was found in electronic medication orders for failing to provide such things as drug usage or
dose.84 Error rates also varied by computerized prescribing system, from 5.1% to 37.5%;85 one-third of those mistakes had the potential for
harm.86 “A breakdown of the errors by category showed that the four most common classes of drugs containing medication errors were anti-
infectives (40.3%), nervous-system drugs (13.9%), and respiratory-system drugs (8.6%). The most common drug classes associated with
potential [adverse drug events] were nervous-system drugs (27.0%), cardiovascular drugs (13.5%), and anti-infectives (12.3%).”87 One
expert explained that many of the errors or miscommunications that happen with digitally sent prescriptions occur because physicians are not
providing all of the necessary information concerning the medication that needs to be issued such as the complete product name, strength
and dosage.88 The e-prescription may also be transmitted to the pharmacy with the correct drug name, but not the correct strength and/or
dosage.89 Common abbreviations used on handwritten prescriptions may also “get lost in translation” if they are entered into the e-
prescription platform.90 There have even been cases where physicians have added notes concerning a patient's use of the medication, but
this practice has resulted in additional confusion on occasion because there may be a discrepancy between the pharmacy records and the
instructions by the physician.91
The error rates and their severity also varied by computerized prescribing system, implying that some systems may be better suited for
preventing mistakes than others.92 Therefore, merely implementing a computer system for dispensing medication is not the answer.93Instead,
the prescribing system must have comprehensive functionality and processes in place to guarantee meaningful system use in order to
decrease medication errors.94 A different study supported these findings and noted that “[b]asic computerized prescribing systems may not
be adequate to reduce errors. More advanced systems with *14 dose and frequency checking are likely needed to prevent potentially harmful
errors.”95
Another analysis of users of electronic transmission of new prescriptions reported that about one-third of patients arrived to pick up their
medication before the pharmacy had received the orders.96 Some doctors blame this development on the failure of pharmacy workers to be
adequately trained to appreciate new e-prescriptions.97 This problem, however, should disappear once workers gain more familiarity with this
new system.98Pharmacist counter by blaming the doctor for the failure to promptly send the prescription or by transmitting the medication
orders to the wrong drug store.99
All parties noted that the electronic renewal process was not as successful on a consistent basis.100 New prescription routing and renewals
proved to be more challenging to assimilate into organization workflows.101 Physicians who received e-renewal requests identified several
ways in which this process broke down causing inefficiencies.102 They complained that pharmacy did not also request electronic renewals of
medication orders or make duplicative requests for a particular medication by different means even though the physician had responded to
the initial request electronically.103 Nevertheless, those who answered the survey emphasized the time-saving benefits of the electronic
renewal procedure when working correctly.104
A number of physicians also use e-prescriptions just enough to avoid the financial penalties imposed by the federal government, but “‘they
don't make e-prescribing part of their routine”’ practices.105 Part of this resistance is because their staffs are not doing their part in the
process.106 For example, “[t]he nurses or medical assistants may not have entered the medication lists for patients who haven't [been] seen
since the doctor started e-prescribing. In some cases, they haven't asked patients about their preferred pharmacies and put those in the
system.”107
*15 Even with the benefits of e-prescriptions some physician are simply reticent to convert to this digital system.108 Reasons vary and include
not wanting to use a computer, not wanting to incur the cost of the program, and being afraid that their employees won't use the
system.109 Some physicians have experienced problems with the drop down menu screens where the doctor is requested to enter the correct
dosage.110 Some systems don't confirm the dosage, and in other cases, the doctor incorrectly selects the value above or below the proper
dosage. Another criticism is “alert fatigue” where so many cautions appear that physicians start to ignore them.111 In fact, it was found that
few physicians alter their prescriptions in response to a drug allergy or interaction notice, and there are a few systems that the threshold for
alerting was fixed too low.112 The recommendation was that “[c]omputerized physician order entry systems should suppress alerts for
renewals of medication combinations that patients currently tolerate” without harm.113
The Health Insurance and Accountability and Portability Act of 1996 (HIPAA) also plays a role in the adoption of digital system with the
enactment of regulations on security and privacy.114 Several mandates must be followed, including: “secure point-to-point electronic
transmission of the prescription at each [connection] in the chain, entity authentication, audit trails and data authentication to ensure that data
have not been changed or altered during transmission.”115 Each doctor who is allowed to use the e-Rx software is provided with a name and
unique password that must be protected and learned.116 This has raised the concern that the busy doctor must remember yet a different
password.117Nevertheless, use of a password to enter the electronic prescription system is necessary for security purposes.118 Perhaps in
the future, entry may be obtained by using iris patterns, fingerprints or proximity badges.119
*16 E-prescriptions may subject physicians to special malpractice concerns.120 Doctors now have the ability to review the medication history
of a patient through this new electronic system, so they may be held accountable for an adverse drug reaction with medication ordered by
another doctor.121 For example, the e-prescribing system has the ability to notify a doctor of an adverse drug reaction with another pill that
the patient is taking.122 Even though the physician did not order that other medication, a duty may be imposed on the doctor to investigate
that possible drug interaction.123
A. State Responses to Electronic Prescriptions
States have enacted legislation or adopted regulations to address e-prescribing of non-controlled substances but these laws are of recent
vintage which is a reflection of digital medication orders being in their infancy stage.124 As a general rule, these directives regulate the
prescribing and filling of e-prescriptions by healthcare professions and pharmacies.125
An analysis demonstrates that these laws are not uniform. Some states set up detailed requirements for the use of e-prescriptions and others
impose privacy of information safeguards. Several states require pharmacists to exercise professional judgment regarding the accuracy,
validity, and authenticity of these digital prescriptions. The difficulty is that some of the state laws meant to implement electronic prescriptions
may actually complicate its use. Some of the problems include: contradictory prescription mandates among varying sets of statutes and
regulations; requiring pharmacies to keep e-prescription records in hard copy; and patient consent mandates for the digital transmission of
their prescription orders.126
1. General E-Prescription Laws
The following are sample statutes to provide a flavor of the different approaches taken by the states. Oregon was an earlier adopter of a law
on electronic *17 prescription when it enacted legislation in 2003.127 That state provides that prescription drug orders may be sent
electronically from a practitioner authorized to prescribe drugs directly to the dispensing pharmacist of the patient's choice with no intervening
person having access to the drug order.128 The form must contain the doctor's telephone number for verbal confirmation, the time and date of
transmission, the identity of the pharmacy intended to obtain the order and all other information required for a prescription by federal or state
law; and the transmission must be traceable to the prescribing practitioner by a digital signature or other secure method of validation.129 A
duty is imposed upon the dispensing pharmacist to exercise professional judgment regarding the accuracy, validity and authenticity of drug
order.130 Finally, no additional charge may be made to the patient because the drug order was transmitted electronically.131
Michigan amended its law in 2012 to provide that a prescription may be transmitted electronically as long as the order form is transmitted in
compliance with the Health Insurance Portability and Accountability Act of 1996.132 The electronically transmitted prescription must include
the name, address and telephone of the ordering doctor, the name of the patient, an electronic signature or other identifier that identifies and
authenticates the prescriber, the time and date of the transmission, the identity of the pharmacy intended to obtain the order and any other
information required by federal or state law.133 Michigan also imposes a duty on the pharmacist to “exercise professional judgment regarding
the accuracy, validity, and authenticity of the transmitted prescription.”134
South Carolina provides that a practitioner “may electronically transmit a prescription to a pharmacy” under very rigorous conditions.135 South
Carolina further requires that a doctor/patient relationship exist; “the prescription must identify the [doctor's] phone number, the time and date
of transmission, and the pharmacy intended to receive the transmission.”136 Additionally,
[t]he prescription must be transmitted by the authorized practitioner or the practitioner's designated agent to the pharmacy of the patient's
choice, and the prescription must be received only by a pharmacy, with no intervening person or entity having access to view, read,
manipulate, alter, store, or delete the electronic prescription prior to its receipt at the pharmacy.137
*18 The prescription must also contain the doctor's electronic or digital signature or key code.138 Nothing, however, may be construed to
prohibit a physician from utilizing a routing firm to transmit a prescription, except that a routing company shall provide its tax identification
number to the Board of Pharmacy before offering its services.139
Washington provides that a prescription may be sent electronically to a pharmacy of the patient's choice if the electronic transmission
“compl[ies] with all applicable statutes and rules regarding the form, content, recordkeeping, and processing of a prescription for a legend
drug;” the systems sending and receiving the electronic drug request must be approved by the board, but these requirements do “not apply
to facsimile equipment transmitting an exact visual image of the prescription.”140 Medication orders are to be treated as “confidential health
information, and may be released only to the patient or the patient's authorized representative, the prescriber or other authorized practitioner
then caring for the patient, or other persons specifically authorized by law to receive such information.”141 Like a number of other jurisdictions,
a duty is imposed upon the pharmacist to “exercise professional judgment regarding the accuracy, validity, and authenticity of the
prescription drug order received [electronically], consistent with federal and state laws.”142
Alabama has a regulation that is directed to electronic prescriptions for non-controlled legend drugs and mandates that “the prescription must
include the patient's name and address, the drug prescribed, strength per dosage unit, directions for use, and the name of the prescriber or
authorized agent.”143 Prescriptions
transmitted over an e-prescription network approved by the Board [and] all transmissions must ensure appropriate security and authenticity
to include the following: An electronic signature process enabling the pharmacy to ensure the identity of the prescriber; [the] [d]ate and time
stamp; [a] transmitting system identifier; [a] prescriber internal sender identification; and a pharmacy internal receiver identification.144
California's law is contained in its Administrative Code and provides that “prescriptions may be transmitted by electronic means from the
prescriber to the pharmacy.”145 “An electronically transmitted prescription order shall include the name and address of the prescriber, a
telephone number for oral confirmation, date of transmission and the identity of the recipient, as well as any other information required by
federal or state law or regulations.”146 “A *19 pharmacy receiving an electronic image transmission prescription shall either receive the
prescription in hard copy form or have the capacity to retrieve a hard copy facsimile of the prescription from the pharmacy's computer
memory.”147 Also, its law provides that “[a]n electronically transmitted prescription shall be transmitted only to the pharmacy of the patient's
choice.”148 “This requirement shall not apply to orders for medications to be administered in an acute care hospital.”149
Minnesota's law, which became effective on January 1, 2011, is very detailed and requires that “all providers, group purchasers, prescribers,
and dispensers must establish, maintain, and use an electronic prescription drug program.”150 All transactions “must use either HL7
messages or the NCPDP SCRIPT Standard to transmit prescriptions or prescription-related information internally when the sender and the
recipient are part of the same legal entity.”151 “If an entity sends prescriptions outside the entity, it must use the NCPDP SCRIPT Standard or
other applicable standards required by this section.”152 “[A]ny clinic with two or fewer practicing physicians, [however,] is exempt if the clinic is
making a good-faith effort to meet the electronic health records system requirement that includes an electronic prescribing
component.”153 The statute then enumerates twelve transactions that must use the NCPDP SCRIPT Standard including transactions such as
new prescription transactions, prescription change request transactions and prescription change response transactions.154
Pennsylvania law defines an electronically transmitted prescription as an original prescription or refill authorization sent by electronic means,
and includes computer-to-computer, computer-to-facsimile machine or e-mail transmission.155 That prescription must be sent directly to a
pharmacy of the patient's choice and include the prescriber's telephone number, the date of the transmission, the name of the pharmacy
intended to receive the transmission and the prescription must be electronically encrypted or transmitted by technological means designed to
protect and prevent access, alteration, manipulation or use by any unauthorized person.156 A hard copy or a readily retrievable image of the
prescription information must be stored for at least two years.157
*20 2. Controlled Substances
Since the federal government only recently granted physicians the right to electronically dispense controlled substances, a number of states
have not yet addressed this issue. Pennsylvania, however, has considered the issue and noted that “a prescription for a Schedule II, III, IV or
V controlled substance is considered a written prescription order on a prescription blank and may be accepted by a pharmacist provided that
the transmission complies with this chapter and other requirements....”158 Minnesota provides that Schedule II controlled substances may
only be issued through a written prescription or, in an emergency situation, may be dispensed at the oral prescription of a practitioner so long
as it is reduced promptly to writing and filed by the pharmacist.159 West Virginia also restricts the issuances of Schedule II substances to an
emergency but the statute does not include Minnesota's rule that the prescription must then be reduced to writing.160 Kentucky law
specifically notes a Schedule II substance may only be issued through a written prescription while Schedules III, IV, and V drugs may be
dispensed following a written, electronic, or oral prescription.161
Kansas provides that, in emergency situations, a controlled substance in Schedule II “may be dispensed upon oral prescription of a
prescriber [as long as the order is] reduced promptly to writing or transmitted electronically and filed by the pharmacy.”162 However, no refills
are allowed for a Schedule II substance.163 California allows physicians to only prescribe Schedule II, III, or IV drugs pursuant to § 4170 of
California's Business and Professions Code, which requires that prior to dispensing, the prescriber must offer to provide a written prescription
to the patient that the patient may elect to have filled by the prescriber or by any pharmacy.164 Electronic prescriptions for Schedule II drugs
in Alabama and Montana cannot be issued without an accompanying hard-copy prescription while e-prescriptions for controlled substances
classified as III-V are prohibited.165
New York's law is very specific when it comes to issuing controlled substances.166 That state's law provides that “[n]o controlled substance
may be [issued] except on an official New York state prescription or on an electronic prescription, and in good faith and in the course of [the
doctor's] professional *21 practice only.”167 The prescription must contain the name, address, and age of the ultimate user; the name,
address, Federal registration number, telephone number, and digital signature of the prescribing practitioner; and it must contain specific
directions for use, including but not limited to the dosage and frequency of amount and the maximum daily dosage.168 “No such prescription
shall be made for a quantity of controlled substances which would exceed a thirty day supply....”169 New York, however, permits a physician
to order as much as three months of a controlled substance as long as it is given to treat a medical condition that has been specifically
identified by the commissioner as allowing the issuance of more than a thirty day supply.170
Texas law was amended in 2012 and appears to be one of the most detailed in the United States involving controlled substances.171 Texas
allows a doctor to e-prescribe a controlled substance listed in Schedule II as long as it sequentially numbered.172Prescriptions dealing with
controlled substances must contain the date the prescription is issued; the controlled substance prescribed; the quantity of controlled
substance prescribed, shown numerically if the prescription is electronic; the intended use of the controlled substance or the diagnosis for
which it is prescribed with the instructions for use of the substance; the practitioner's name, address, and Federal Drug Enforcement
Administration number issued for prescribing a controlled substance in Texas; the name, address, and date of birth or age of the person for
whom the controlled substance is prescribed; and, the earliest date on which a pharmacy may fill the prescription.173 Each dispensing
pharmacist is also mandated to fill in on the official prescription form in the electronic prescription record, each item of information given
orally to the dispensing pharmacy and the date the order is filled.174 Electronic prescription shall appropriately note the identity of the
dispensing pharmacist; retain with the records of the pharmacy for at least two years the electronic prescription, the name of the patient and
send all information required by the director, including any information required to complete an electronic prescription record, to the director
by electronic transfer not later than the seventh day after the date the prescription is filled.175
*22 IX. Cases Involving E-Prescriptions
There have not been many reported cases concerning e-prescriptions, presumably because the technology and its widespread use are fairly
new. Most of the published litigation involves criminal prosecutions.
A. Administrative Rulings
One of the earliest cases dealing with the electronic transmission of a prescription occurred in 1998.176 Walgreen Company was charged with
violating “various regulatory statutes and administrative rules relating to pharmacies when, as part of a test program, it [received]
prescriptions orders from [doctors] through [e-mail], and provided used computers for some of the physicians participating in the test.”177 In
Walgreen Co. v. Wisconsin Pharmacy Examining Bd., the Wisconsin Pharmacy Examining Board “concluded that the use of computer-
transmitted prescriptions violated [the law] which require[d] written prescription orders to be signed by the prescribing physician.”178Although
this was a case of first impression “involving computer transmission of prescriptions from physician to pharmacy,” the court found in favor of
Walgreens.179 It used as precedent a case in which a facsimile prescription transmission was equivalent to telephone orders.180
Logan v. St. Charles Health Council, Inc. involved a claim for a violation of a state privacy statute.181 The plaintiff, a physician, filed suit as the
result “of her employment by a federally-assisted health care center.”182 She “became credentialed to provide certain medical services to
veterans at [a clinic] [and] was provided an identification code that allowed her to electronically [send] prescriptions to the VA hospital
pharmacy, and access VA patient files.”183 The plaintiff claimed that while on vacation, others “began using [her] name and identification
code to write prescriptions to be filled at the VA pharmacy” without her knowledge.184 Additionally, the physician-plaintiff asserted that upon
her return, the defendants refused to take remedial action to correct the records related to those medication orders.185 The defense argued
that “[t]he Federal Tort Claims Act provides the exclusive remedy for damages resulting *23 from ‘the performance of medical, surgical,
dental, or related functions' by Public Health Service employees acting within the scope of their employment.”186 The plaintiff, however,
maintained that this federal law should not extend to her claim because her suit did not sound in medical malpractice.187 The court agreed
and remanded the matter to state court to proceed on the privacy statute violation.188
In Brighton Pharmacy, Inc. v. Colorado State Pharmacy Bd., a pharmacy and pharmacist appealed a challenge to the Colorado State
Pharmacy Board ruling that:
A pharmacist shall make every reasonable effort to ensure that any order, regardless of the means of transmission, has been issued for a
legitimate medical purpose by an authorized practitioner. A pharmacist shall not dispense a prescription drug if the pharmacist knows or
should have known that the order for such drug was issued on the basis of an internet-based questionnaire, an internet-based consultation,
or a telephonic consultation, all without a valid preexisting patient-practitioner relationship.189
“[A] typical scenario addressed by this Rule involves websites to which a consumer can go and request a prescription for a particular
pharmaceutical.”190 “Requests for Viagra and hydrocodone constitute a significant portion of the business.”191 The purchaser then responds
to a variety of set questions exclusive to the requested drug.192 The person's responses are sent to a doctor who then issues the electronic
prescription through a participating pharmacy.193 Often, the parties are from varying states and have never met.194 Although the court
acknowledged that there are many legitimate scenarios in which this type of transaction could occur, it was in the bounds of the Board to
create and uphold the rule prohibiting prescriptions based on internet questionnaires.195
B. Criminal Cases
United States v. Hanny involved the sale of prescription drugs over the Internet.196 The defendant was a retired surgeon who received an
offer to work for “a company that sold prescription drugs over the Internet.”197 The company *24 wanted the physician “to authorize
prescriptions to its Internet customers.”198 Even though he “questioned the legality [[[of the business] and consulted an attorney,” the
defendant went to work for the company.199 “To authorize the sale, the physician would [affix] his electronic signature to the order.”200 The
doctor was not required to see the patient, and the electronic order was sent to a participating pharmacy to fill.201 The defendant authorized
over 2,400 medication orders and kept a portion of each sale.202 Eventually, the Missouri Board of Medicine informed the physician that his
actions were illegal, but he continued to prescribe medication.203 He was then charged with conspiring to distribute a controlled substance
outside the normal medical practice.204 The defendant pleaded guilty, and on sentencing, the judge determined that the physician was
involved in selling drugs through mass-marketing by means of an interactive computer service and received an enhancement penalty. This
decision was upheld on appeal.205
United States ex rel. Ciaschini v. Ahold USA Inc. involved a qui tam realtor claim by a whistle blower against a pharmacy alleging it had
submitted false claims to the government in order to obtain Medicare and Medicaid payments for prescription drugs provided to customers in
violation of the False Claims Act.206 The plaintiff was a licensed pharmacist at The Stop & Shop Supermarket Company in
Massachusetts.207 It was practice for the pharmacists employed by the business “‘to electronically submit prescriptions of a Beneficiary of a
Federal Health Care Program to Corporate Headquarters, which, in turn, electronically submitted the claim for payment to the Federal Health
Care Program through the [firm's] electronic billing system.”’208 The plaintiff alleged that these submissions were false for a number of
reasons.209 The court dismissed the suit because the plaintiff failed to provide sufficient details connecting the entry of the information in the
computer system to planned claims filed with the government.210
United States v. Ghassan Haj-Hamed, involved a physician who was “indicted on twenty-two counts of distributing prescription drugs without
a legitimate medical purpose.”211
*25 An investigation revealed that Dr. Haj-Hamed routinely spoke to patients for a minute or so without conducting any meaningful physical
examination. He then prescribed frequently abused controlled substances to the patients in exchange for cash payments. A confidential
source told agents that Dr. Haj-Hamed referred to himself as ‘Dr. Feel Good.’ Others considered him an easy source for obtaining Oxycontin
and other controlled substances. It was noteworthy is that he told patients to ‘fill their prescriptions in Ohio or Indiana to avoid Kentucky's
electronic prescription-tracking system.212
The government eventually dismissed twenty-one counts in exchange for the defendant pleading guilty to one count.213
Thacker v. Kentucky dealt with a person arrested for driving under the influence.214 During the traffic stop, a police officer found prescription
drug containers for controlled medications and learned that defendant had been charged with prescription forgery.215 A detective then
requested a KASPER report, which described the defendant's prescription activity in Kentucky and showed that suspect had been issued
overlapping prescriptions.216 The detective then questioned defendant's pharmacies about the prescriptions.217 The appellate court held that
the detective's use of the KASPER-derived information system was not an unreasonable search and seizure.218 Instead, the search
exception to an arrest warrant applied because the State had a substantial interest in tracing drug distributions, and the KASPER system
reasonably advanced that interest.219
C. Malpractice
In Washington v. United States, a claim was filed under the Federal Tort Claims Act as the result of an amputation of a leg and subsequent
patient death.220 The facts show that the decedent was an insulin dependent diabetic. He “stepped on a nail, causing a puncture wound to
his left foot[[[,]” developed an abscess, and was given a prescription which was ordered electronically by the doctor at the VA.221 To obtain
the medication after the doctor's visit, the patient presented himself “at the pharmacy located in the VA.”222Following his visit, the patient went
to the nurse whose notes show that he was sent to *26the pharmacy for medication and instructions.223 The decedent's wife, however, said
that the nurse told them that the medicine would be mailed, so they went home.224 The patient's name appeared on a list of those who failed
to pick up ordered prescriptions.225Two days later, he returned to the VA and his foot was much worse.226 He was finally given the medication
and the pharmacist noted that it was about to be mailed to him.227Two days later, the patient was seen at the VA Emergency Room with an
abscess and cellulitis.228 He was admitted to the hospital and his blood sugar count was highly elevated.229 Eventually, his leg was
amputated because the infection was not controlled.230 After a prolonged hospitalization, he died.231 Multiple counts of negligence were
advanced including that he was initially sent home with conflicting instructions relating to his medication so he was delayed in starting his
antibiotics.232 The court agreed and found in the decedent's favor.233
X. Conclusion
The issuance and consumption of medication has a number of problems. Historically, the staffs of pharmacies make millions of calls to
physicians in an effort to clarify prescriptions or to inquire about possible medication errors. Doctors and their staff also spend valuable time
each day answering these inquires. Electronic prescribing of medication has been heavily promoted as the solution to these problems, and
the federal government has spent millions of dollars to encourage physicians to adopt these digital systems. Unfortunately, errors persist with
electronic prescribing and healthcare providers question whether the time needed to view and import the information into patient records
merits the extra time needed to access and review them.
Regardless of the existing issues, so much time and money has been expended with this conversion process that digital prescriptions are not
about to disappear. Most of the experienced difficulties relate to the growing pains of new technology and the reluctance of people to adopt
and learn a new system. It is anticipated that these problems will be resolved in the coming years so the prognosis of electronic prescriptions
is robust. More and more healthcare providers will adopt this electronic method of prescribing medication especially in *27 view of the
financial penalties being imposed by the federal government for those who do not use this technology.
Footnotes
1
Samuel D. Hodge, Jr. is a professor and chair of the Legal Studies Department at Temple University where he teaches both law and
anatomy. He lectures nationally on anatomy and trauma and is considered one of the most popular speakers of continuing legal education
courses in the country. Professor Hodge is a graduate of Temple University Beasley School of Law and is a member of the American College
of Legal Medicine.
2
Allison Kilcourse currently works for the law firm of Galerman and Tabakin, LLP in Jenkintown, Pennsylvania. She is a graduate of Temple
University Beasley School of Law and completed her undergraduate studies at Saint Joseph's University, receiving a B.A. in International
Affairs and Political Science.
3
The American Recovery and Reinvestment Act deals with the conversion of paper charts into electronic medical records. It is believed that
there are many benefits for this conversion including streamlining patient care and providing long-term savings in the health field. The
electronic medical records stimulus also offers financial incentives and penalties to entice physicians to convert to the paperless electronic
medical record systems. See generally What are the Benefits of Electronic Medical Records?, MEDICALRECORDS.COM, http://
www.medicalrecords.com/physicians/what-are-the-benefits-of-working-with-emr (last updated May 21, 2013).
4
Charles S. Hartig, Regulatory Barriers When Implementing E-Prescribing of Controlled Substances: Could Model Language Be The
Solution?, 5 ST. LOUIS U. J. HEALTH L. & POL'Y 213, 217 (2011). As President George Bush noted in his State of the Union Address on
January 20, 2004: “By computerizing health records, we can avoid dangerous medical mistakes, reduce costs, and improve care.” He also
believes that innovations in electronic health records and the secure exchange of medical data will assist in transforming health care by
improving health care quality, reducing paperwork, preventing medical errors, reducing health care costs, improving administrative
efficiencies, and increasing access to affordable health care. See generally Transforming Health Care: The President's Health Information
Technology Plan, THE WHITE HOUSE, http://georgewbush-whitehouse.archives.gov/infocus/technology/economic_
policy200404/chap3.html (last visited June 21, 2013).
5
VIST-A was the first major initiative into the world of electronic health records and e-prescribing, with the Veteran Affairs' computerization of
health records. Douglas Goldstein et al., Case Studies of VistA Implementation — United States and International, in MEDICAL
INFORMATICS 20/20, 223, 226, 263 (2007), available at http:// www.jblearning.com/samples/0763739251/39251_ CH09&uscore;
223_284.pdf; see also Charles S. Hartig, Regulatory Barriers When Implementing E-Prescribing of Controlled Substances: Could Model
Language Be The Solution?, 5 ST. LOUIS U. J. HEALTH L. & POL'Y 213, 213-214 (2011).
6
The National Progress Report on E Prescribing and Safe Rx Rankings, SURESRCIPTS, http://www.surescripts.com/about-e-
prescribing/progress-reports/national-progress-reports (last visited June 26, 2013).
7
The court in Brody v. Zix Corp., No. 3:04-CV1931-K, 2006 WL 2739352, at *1 (N.D. Tex., 2006) noted that electronic prescriptions were
“intended to alleviate problems with illegible physician handwriting on prescriptions and help doctors streamline the process of dealing with
insurance companies and pharmacies.”
8
E-Prescribing, CENTERS FOR MEDICARE AND MEDICAID SERVICES, http:// www.cms.gov/Medicare/E-
Health/Eprescribing/index.html?redirect=/eprescribing/ (last visited June 21, 2013).
9
The use and benefits of e-prescriptions was noted as early as 1986. John Donald noted in the British Medical Journal that “[a] computer is
used to produce all prescriptions for patients.... This method of prescribing improves safety, saves time, decrease prescribing cost, and
provides an instant audit of all important prescribing parameters.”). John B. Donald, On Line Prescribing by Computer, 292 BR. MED. J. 937,
937 (1986).
10
See id.
11
What Are Some of The Benefits of E-Prescribing?, U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, http://
www.hrsa.gov/healthit/toolbox/HealthITAdoptiontoolbox/ElectronicPrescribing/benefitsepres.html (last visited June 21, 2013).
12
Bo Hovstadius, Bengt Astrand, and Goran Petersson, Dispensed Drugs and Multiple Medications in the Swedish Population: An Individual-
Based Register Study, BMC CLINICAL PHARMACOLOGY (2009), http:// www.biomedcentral.com/1472-6904/9/11 (last visited February 16,
2012).
13
Medication Safety Basics, CENTER FOR DISEASES CONTROL AND PREVENTION, http://www.cdc.gov/medicationsafety/basics.html (last
visited February 16, 2012).
14
Patterns of Medication Use in the United States, SLONE EPIDEMIOLOGY CENTER AT BOSTON UNIVERSITY at *1 (2006), available at
http:// www.bu.edu/slone/research/studies/slone-survey/.
15
Id. at 14.
16
What Are Some of The Benefits of E-Prescribing?, supra note 11.
17
Jeff Todd, E-Prescribing In A Changing Legal Environment, 12 RICH. J.L. & TECH. 12, 5 (2006).
18
Id.
19
Medication Errors, FDA, http:// www.fda.gov/drugs/drugsafety/medicationerrors/default.htm (last updated Aug. 08, 2013).
20
Id.
21
Christine Stencel & Chris Dobbins, Medication Errors Injure 1.5 Million People and Cost Billions of Dollars Annually, NEWS FROM THE
NATIONAL ACADEMIES, (July 20, 2006), http:// www8.nationalacademies.org/onpinews/newsitem.aspx?RecordID=11623.
22
Id.
23
Id.
24
Id.
25
Id.
26
Stencel & Dobbins, supra note 21, at 1.
27
Id.
28
In Springhill Hospitals, Inc. v. Larrimore, the court noted that a hospital's policy to its druggist is that “the prescribing physician shall be called
for consultation whenever the pharmacist deems it necessary upon reviewing a medication order to prevent any unwanted outcome,” did not
impose liability separate and apart from doctor if the druggist contacted the physician as required. Springhill Hospitals, Inc. v. Larrimore, 5
So.3d 513, 521 (Ala. 2008).
29
LAURA DIETZ ET AL., 25 AM. JUR. 2D DRUGS AND CONTROLLED SUBSTANCES § 249 (2013).
30
Id.
31
“When the condition worsens after a prescription error, pharmacies often are quick to claim that this would have happened anyway and that
the plaintiff cannot prove that the error made a difference. For example, pharmacies have claimed that a person's infection would not have
improved even if an antibiotic—instead of a decongestant—had been dispensed; that ulcerative colitis would have necessitated removal of
the large intestine even if an incorrect and ineffective steroid dose had been filed; that no studies show that getting diabetes medication
instead of a muscle relaxant causes kidney damage.” Trent B. Speckhals, Not What The Doctor Ordered: prescription errors—when a patient
gets the wrong drug, at the wrong strength, or with the wrong directions—can be serious and even deadly. With thorough preparation, you
can show that the pharmacy committed malpractice, TRIAL Dec. 1, 2010, at 34.
32
DEITZ, supra note 29.
33
Frank M. McCLellan, Reading the RX Right is not Enough: millions of Americans rely on prescribed drugs to stay healthy—and on their
pharmacists to protect them from medication errors. Some courts are beginning to recognize that pharmacists must do more than fill
prescriptions accurately, TRIAL, May 1, 2002, at 26. “Alabama codified Omnibus Budget Reconciliation Act in 1991” and noted:
“Pharmacists, because of their strategic position in the health care system, have traditionally provided drug information to their patients and
to other health care professionals.” “Pharmacists are also required to review prescriptions for contraindications, drug interactions, and
incorrect dosages. Pharmacists may also discuss side effects, adverse interactions, and contraindications. Pharmacies are required to keep
patient medication profiles that incorporate the patient's name, age, sex, patient history, and a list of prescription medications.” Julie L.
Doughty,Walls v. Alpharma: Is the Learned Intermediary Doctrine the Right Cure for Pharmacists in Alabama?, 9 JONES L. REV. 37, 45
(2005).
34
Id. at 28.
35
Thomas William Arbon & S. Craig Smith, Prescription for Error, TRIAL, Oct. 1999, at 66. In Simmons v. Apex Drug Stores, Inc., plaintiff sued
defendant-pharmacist after receiving an antidepressant, for which he suffered an adverse reaction, instead of a prescription for an appetite
suppressant. While the claim was dismissed under a statute of limitations defense, the court held the pharmacist's actions to be a breach of
duty and the proximate cause.Simmons v. Apex Drug Stores, Inc., 506 N.W.2d 562, 564-65 (Mich. App. 1993), modified by Patterson v.
Kleiman, 526 N.W. 2d 879 (Mich. 1994).
36
Walter v. Wal-Mart Stores, Inc., 748 A.2d 961, 968 (Me. 2000), see alsoHarco Drugs, Inc. v. Holloway, 669 So. 2d 878, 880-81 (Ala. 1995).
37
Morgan v. Wal-Mart Stores, Inc., 30 S.W.3d 455, 466-67 (Tex. App. 2000).
38
Kathleen Michon, Medical Malpractice: Common Errors by Doctors and Hospitals, NOLO, http://www.nolo.com/legal-encyclopedia/medical-
malpractice-common-errors-doctors-hospitals-32289.html (last visited June 20, 2013).
39
Mary A. Fischer, When Bad Medicine Happens to Good People, OPRAH MAG. (May 2005), http://www.oprah.com/health/What-Happens-
When-Doctors-Make-Medical-Mistakes-Misdiagnosis.
40
What Are Some of The Benefits of E-Prescribing?, U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, http://
www.hrsa.gov/healthit/toolbox/HealthITAdoptiontoolbox/ElectronicPrescribing/benefitsepres.html (last visited June 21, 2013).
41
Id.
42
Benefits of E-Prescribing for Pharmacists, SURESCRIPTS, http:// www.surescripts.com/about-e-prescribing/benefits-of-e-prescribing_for-
pharmacies (last visited June 20, 2013). Unlike faxes or paper prescriptions, e-prescriptions go directly into the pharmacist's computer.
Authorizations for medication renewals can be serviced with just a few keystrokes. When compared with the paper form of prescriptions,
electronic prescriptions decrease the amount of employee time needed to finish dispensing activities by 27% for new prescriptions and 10%
for renewals (valued at $1.07 and $0.41 per prescription respectively). Id
43
Shawn Riley, The Benefits of E-prescribing for Today's Physician, HEALTHTECHNICA.COM, (Nov. 12, 2010), http://
www.healthtechnica.com/blogsphere/2010/11/12/the-benefits-of-e-prescribing-for-todays-physician/#sthash.botCbGFd.dpuf.
44
Id.
45
What is E-Prescribing?, AM. COLL. OF RHEUMATOLOGY, http:// www.rheumatology.org/Practice/Office/Hit/E-Prescribing/ (last visited June
20, 2013).
46
Id.
47
Id.
48
Id.
49
Id.
50
Id.
51
The power of the government to influence the practice of medicine is demonstrated by the fact that the number of prescriptions that were
sent to drug stores electronically increased by 181% in 2009 compared with 2008. Robert Lowes, Use of Electronic Prescribing Nearly
Tripled in 2009, MEDSCAPE (Mar. 5, 2010), http://www.medscape.com/viewarticle/718039. Despite these statistics, only about 36% of all
prescriptions were sent electronically in the United States in 2011. Randall Stross, Chicken Scratches vs. Electronic Prescriptions, N.Y.
TIMES (Apr. 28, 2012), http://www.nytimes.com/2012/04/29/business/e-prescriptions-reduce-errors-but-their-adoption-is-slow.html?_r=0.
52
How Much Does An E-Prescribing System Cost?, HEALTH RES. AND SERVS. ADMIN., http://
www.hrsa.gov/healthit/toolbox/HealthITAdoptiontoolbox/ElectronicPrescribing/costofepres.html (last visited June 20, 2013).
53
Considerations in Choosing an E-Prescribing System, AM. COLL. OF PHYSICIANS, http://www.acponline.org/running_
practice/technology/eprescribing/medicare_program_choosing.pdf (last visited June 20, 2013).
54
HEALTH RES. AND SERVS. ADMIN., supra note 52.
55
Id. See also Crystal Conde, RECs to the Rescue: Regional Centers Help Physicians Use HIT, Tex Med. 2010; 106(4):61-67, http://
www.texmed.org/Template.aspx?id =16095#sthash.ITC09mUI.dpuf (last visited February 10, 2014).
56
Id.
57
Id.
58
Clinician's Guide to E-Prescriptions, CTR. FOR IMPROVING MEDICATION MGMT.,
http://www.surescripts.com/media/800052/cliniciansguidee-prescribing_ 2011.pdf (last visited June 20, 2013).
59
Electronic Prescribing (eRx) Incentive Program, Centers for Medicare and Medicaid Services, CMS.GOV,
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ERxIncentive/index.html?redirect=/ erxincentive (last
modified July, 17, 2013).
60
Id.
61
Id.
62
Id.
63
It is anticipated that this incentive program will increase those using electronic prescribing from 15% to 95% in just a decade. Amanda
Baltazar, Electronic Prescribing, ABOUT.COM PHARMACY, http:// pharmacy.about.com/od/Technology/a/Electronic-Prescribing.htm (last
visited June 20, 2013).
64
Centers for Medicare and Medicaid Services, CMS.gov, supra note 59.
65
Law Will Boost E-Prescribing, HHS Secretary Says, GOVERNMENT HEALTH IT (July 21, 2008), http://www.govhealthit.com/news/law-will-
boost-e-prescribing-hhs-secretary-says.
66
Electronic Prescribing (eRx) Incentive Program, AM. OSTEOPATH ASS'N, http://www.osteopathic.org/inside-aoa/development/practice-
mgt/Pages/erx-incentive-program.aspx (last visited June 20, 2013).
67
As of Spring 2013, “more than 291,000 providers and 3,800 hospitals have received incentive payments.” Kelly Kennedy, Incentives Push
Doctors To Electronic Medical Records, USA Today (May 22, 2013), http:// www.usatoday.com/story/news/health/2013/05/22/more-doctors-
hospitals-using-electronic-medical-records/2350811/.
68
Electronic Prescribing (eRx) Incentive Program, supra note 66, at 1.
69
Electronic Prescriptions for Controlled Substances Notice of Approved Certification Process, FED. REGISTER (Mar. 26, 2013), https://
www.federalregister.gov/articles/2013/03/26/2013-06918/electronic-prescriptions-for-controlled-substances-notice-of-approved-certification-
process.
70
Electronic Prescriptions for Controlled Substances Clarification, FED. REGISTER (Oct. 11, 2011), http://www.deadiversion.usdoj.gov/fed_
regs/notices/2011/fr1019.htm.
71
Charles Hartig, Regulatory Barriers When Implementing E-Prescribing of Controlled Substances: Could Model Language Be The Solution? 5
ST. LOUIS UNIV. J. HEALTH LAW & POLICY 213, 218 (2011).
72
Id. at 218-19.
73
E-Prescribing & Incentives, HORIZON BLUE CROSS AND BLUE SHIELD OF N.J., http://www.horizonblue.com/providers/services-
programs/pharmacy-programs/e-prescribing-incentives (last visited Jan. 8, 2014).
74
Id.
75
Id.

76
E-Prescribing Collaborative Program, BLUECROSS BLUESHIELD OF ILLINOIS, http://www.bcbsil.com/provider/pharmacy/eprescribing.html
(last visited Jan. 8, 2014).
77
Electronic Prescribing, HUMANA, https://www.humana.com/insurance-through-employer/pharmacy/rx-tools/eprescribe.
78
Id.
79
The National Progress Report on E-Prescribing and Safe-Rx Rankings for 2012, SURESCRIPTS,
http://www.surescripts.com/downloads/npr/National%20Progress%CC20Report%CC20on%CC20E%CC20Prescribing%CC20Year%C̈̈̈̈ 12.pdf
.
80
Id.
81
Robert H. Miller & Ida Sim, Physicians' Use of Electronic Medical Records: Barriers and Solutions, 23 HEALTH AFFAIRS 116, 119 (2004),
available at http://www.mariaskachko.com/healthcare/articles/physician_use_EMR.pdf.
82
Joy M. Grossman et al., Physician Practices, E-Prescribing and Accessing Information to Improve Prescribing Decisions, 20 CENTER FOR
STUDYING HEALTH SYSTEM CHANGE 1, 1 (2011), http://www.hschange.com/CONTENT/1202/.
83
Ed Silverman, E-Prescribing & Handwritten Error Rates Are Similar, PHARMOLAT, (July 5, 2011), http://www.pharmalive.com/e-prescribing-
handwritten-error-rates-are-similar.
84
Id.
85
Id.
86
Karen Nanji et al., Errors Associated With Outpatient Computerized Prescribing Systems, 18 J. AM. MED. INFORM. ASSOC. 767, 767
(2011), http:// jamia.bmj.com/content/early/2011/06/09/amiajnl-2011-000205.abstract.
87
Id.
88
Melissa Krause and Fred Hamlin, E-Prescribing: Expectations and Limitations, Computer Talk, November/December 2010 at 41,
http://phsirx.com/wp-content/uploads/2011/12/ViewPoints_Nov-Dec2010.pdf (last visited June 26, 2013).
89
Id.

90
Id.
91
Id.
92
Nanji et al., supra note 86, at 772.
93
Id.
94
Id.
95
Tejal K. Gandhi et al., Outpatient Prescribing Errors and The Impact of Computerized Prescribing, 9 J. GEN. INTERN. MED. 837, 837
(2005), http:// www.ncbi.nlm.nih.gov/pmc/articles/PMC1490201/pdf/jgi_05414.pdf.
96
Joy M. Grossman et al., Transmitting and Processing Electronic Prescriptions: Experiences of Physician Practices and Pharmacies, 19 J.
AM. MED. INFORM. ASSOC. 353, 356 (2011), http:// www.ncbi.nlm.nih.gov/pubmed/22101907.
97
Id.
98
Id.
99
Id.
100
Id.
101
Id.
102
Id.
103
Id.
104
Id.
105
Kenneth Terry, Be Warned: e-Prescribing's 6 Big Challenges for Doctors, MEDSCAPE TODAY,
http://www.medscape.com/viewarticle/773404_2 (last visited June 20, 2013).
106
Id.
107
Id.
108
Marrisa Torrieri, Safe E-Prescribing: A Primer for Practices, PHYSICIAN PRACTICE, http://
www.capitaldigestivecare.com/sites/default/files/Kaufman_PhysiciansPractice.e-prescribe.pdf (last visited June 21, 2013).
109
Id.
110
Id. at 2.
111
Id.
112
Saul N. Weingart et al., Physicians' Decisions to Override Computerized Drug Alerts in Primary Care, ARCH INTERN MED. 2625, 2625
(2003).
113
Id.
114
Richard H. Schwartz & Michael Martin, Electronic Prescribing Holds Both Promises and Problems, HEALIO PEDIATRICS: INFECTIOUS
DISEASES IN CHILDREN, http://www.healio.com/pediatrics/practice-management/news/print/infectious-diseases-in-children/#b16e5b4d-
c817-4b13-a14c-79e155d4a5e9'/electronic-prescribing-holds-both-promises-and-problems (last visited June 21, 2013).
115
Id.
116
Id.
117
Id.
118
Id.
119
Id.
120
See generally David B. Towel, E-prescribing Malpractice Risks, THE DOCTORS COMPANY, http://
www.thedoctors.com/KnowledgeCenter/PatientSafety/articles/CON_ID_004728 (last visited June 25, 2013).
121
Id.
122
Id.
123
Id.
124
Id.
125
Jon White, Report on State Prescribing Laws - Implications for E-Prescribing, PRIVACY AND SECURITY SOLUTIONS FOR
INTEROPERABLE HEALER INFORMATION EXCHANGE, ES-1, August 2009, http:// www.healthit.gov/sites/default/files/290-05-0015-state-
rx-law-report-2.pdf (last visited June 25, 2013).
126
Id. at 3-1. According to an article published by the American Academy of Orthopedic Surgeons, all 50 states and the District of Columbia
have rules or statutes dealing with e-prescriptions. See Jackie Ryan, Nuts and Bolts of E-Prescribing, AAOS NOW, Vol. 7, No. 6, June 2013,
http:// www.aaos.org/news/aaosnow/oct08/managing6.asp (last visited June 25, 2013).
127
OR. REV. STATE. ANN. § 475.188(2)(a)-(b) (West 2013).
128
Id.
129
§ 475.188(2)(c)-(d).
130
§ 475.188(4).
131
§ 475.188(8).
132
See generally MICH. COMP. LAWS ANN. § 333.17754 (West 2013).
133
§ 333.17754(1)(a)-(f).
134
§ 333.17754(3).
135
S.C. CODE ANN. § 44-117-320(A) (2013).
136
§ 44-117-320(A)(1)-(2).
137
§ 44-117-320(A)(3).
138
§ 44-117-320(A)(5).
139
§ 44-117-320(C)(1).
140
WASH. REV. CODE ANN. § 69.50.312(1)(a)-(b) (West 2013).
141
§ 69.50.312(1)(d).
142
§ 69.50.312(1)(f).
143
ALA. ADMIN CODE r. § 680-X-2-32(a) (2013).
144
§ 680-X-2-32(b).
145
CAL. CODE REGS. TIT. 16, § 1717.4(a) (2013).
146
§ 1717.4(c).
147
§ 1717.4(e).
148
§ 1717.4(f).
149
Id.
150
MINN. STAT. ANN. § 62J.497(Subd. 2.)(a) (West 2013).
151
§ 62J.497(Subd. 2.)(c).
152
Id.
153
§ 62J.497(Subd. 2.)(d).
154
§ 62J.497(Subd. 3.)(4)-(6).
155
49 PA. CODE § 27.201(a) (2013).
156
§ 27.201(b)-(b)(iv).
157
§ 27.201(b)(4).
158
§ 27.201(b)(5).
159
MINN. STAT. ANN. § 152.11 (West 2013).
160
W. VA. CODE § 60A-3-308 (2013).
161
KY. REV. STAT. § 218A.110 (West 2013).
162
KAN. STAT. ANN. § 65-4123(b) (West 2013).
163
Id.
164
CAL. BUS. & PROF. CODE § 4170(a)(6) (West 2013).
165
Jeff Byers, POCP: States' E-Prescribing Rules For Controlled Substances Vary, Health Imaging,
http://www.healthimaging.com/topics/oncology-imaging/pocp-states-e-prescribing-rules-controlled-substances-vary (last visted February 13,
2014).
166
See generally N.Y. PUB. HEALTH LAW § 33321 (McKinney 2013).
167
§ 3332(1).
168
§ 3332(2)(a)-(c).
169
§ 3332(3).
170
Id.
171
See generally TEX. HEALTH & SAFETY CODE ANN. § 481.075 (West 2013).
172
§ 481.075(a)-(b).
173
§ 481.075(e)-(g).
174
§ 481.075(g)(1).
175
White, supra note 125, at A-1.
176
See generally Walgreen Co. v. Wis. Pharmacy Examining Bd., No. 97-1513, 217 WL 65551 at *1 (Wis. App., Feb. 19, 1998).
177
Id.
178
Id.
179
Id. at 3.
180
Id.
181
Logan v. St. Charles Health Council, No. 1:06CV00039, 2006 WL 1149214 at *1 (W.D. Va., May 1, 2006).
182
Id.
183
Id.
184
Id.
185
Id.
186
Id.
187
Id.
188
Id.
189
Brighton Pharmacy Inc. v. Colo. State Pharmacy Examining Bd., 160 P.3d 412, 415 (2007).
190
Id.
191
Id.
192
Id.
193
Id. at 415.
194
Id.
195
Id. at 414.
196
United States v. Hanny, 509 F.3d 916, 917 (2007).
197
Id.
198
Id.
199
Id.
200
Id. at 917.
201
Id.
202
Id.
203
Id.
204
Id. at 918.
205
Id. at 920.
206
See generally United States ex rel. Ciaschini v. Ahold USA Inc., 282 F.R.D. 27 (2012).
207
Id. at 29.
208
Id. at n. 40.
209
Id. at n. 41.
210
Id. at 35-36.
211
United States v. Haj-Hamad, 549 F.3d 1020, 1022 (2008).
212
Id.
213
Id.
214
Thacker v. Kentucky, 80 S.W.3d 451, 453 (2002).
215
Id.
216
Id.
217
Id.
218
Id. at 456.
219
Id. at 455.
220
Washington v. United States, No. 1:04 CV 007 TCM, 2005 WL 1799737 at *1 (E.D. Mo., July 27, 2005).
221
Id.
222
Id. at 3.
223
Id.
224
Id.
225
Id.
226
Id. at 4.
227
Id.
228
Id.
229
Id.
230
Id. at 5.
231
Id. at 6.
232
Id. at 8.
233
Id. at 12.
18 MSUJMEDL 1
End of Document © 2016 Thomson Reuters. No claim to original U.S.
Government Works. SELECTED TOPICS
Products Liability
o Particular Products
o
Manufacturer Warning of Prescription Drug Inherent Risks
1. Secondary Sources
Construction and application of learned-intermediary doctrine
57 A.L.R.5th 1 (Originally published in 1998)
...This annotation collects and analyzes those state and federal cases in which the courts have applied the learned-intermediary doctrine, or invoked an exception thereto, in
determining whether, and unde...
2. ¶180 FDA AND STATE AND LOCAL AGENCIES
FDA Enforcement Man. ¶180
...Forty-six states have adopted the Uniform Food and Drug Law, which was patterned on the Federal Food, Drug and Cosmetic Act (FD&C Act). As a result, state laws
generally define adulteration and misbran...
3. Drug Products Liability and Malpractice Cases
17 Am. Jur. Trials 1 (Originally published in 1970)
...This article examines the special techniques to be employed by counsel representing either the plaintiff or defendant in the trial of a products liability action brought against the
manufacturer of a d...
4. See More Secondary Sources
5. Briefs
Brief for Respondents Gladys Mensing and Julie Demahy
2011 WL 686400
Pliva, Inc. v. Mensing
Supreme Court of the United States.
February 23, 2011
...FN* Cou e failure-to-warn claim brought against a
prescription-drug manufactu...
6. Brief of Petitioners PLIVA, Inc.; Teva Pharms. USA, Inc.; and UDL Labs, Inc.
2011 WL 219554
PLIVA, Inc. v. Mensing
Supreme Court of the United States.
January 24, 2011
...FN1. Available at http://www.gphaonline.org/about-gpha/about-generics/case/generics-providing-savings-americans (last visited January 23, 2011). The Eighth Circuit's
decision in Nos. 09-993 and 09-1039...
7. Brief for Respondent
2008 WL 3285388
Wyeth v. Levine
Supreme Court of the United States.
August 07, 2008
...1. In the nineteenth and early twentieth centuries, centralized markets for food and drugs developed to serve growing urban centers. See Peter Barton Hutt et al., Food and
Drug Law 7 (3d ed. 2007) (“Fo...
8. See More Briefs
9. Trial Court Documents
Rodger v. Ford Motor Co.
2006 WL 5779145
Rodger v. Ford Motor Co.
Circuit Court of Michigan, Wayne County
October 30, 2006
...Plaintiff, Sylvania Roger, through counsel, respectfully moves for reconsideration. 1. On October 17, 2006 the Court granted summary disposition to Defendants against
Plaintiff for reasons stated on th...
10. Mary KRAFT, individually and in a representative capacity, Plaintiff, v. DETROIT ENTERTAINMENT, LLC, d/b/a Motor City Casino, Greektown Casino, MGM Grand Detroit, LLC, d/b/a MGM Grand
Detroit Casino, International Game Technology, Inc., and Anchor Gaming, Inc., Defendants, IGT and Anchor Coin, Intervenor Defendants.
2002 WL 34110085
Mary KRAFT, individually and in a representative capacity, Plaintiff, v. DETROIT ENTERTAINMENT, LLC, d/b/a Motor City Casino, Greektown Casino, MGM Grand Detroit,
LLC, d/b/a MGM Grand Detroit Casino, International Game Technology, Inc., and Anchor Gaming, Inc., Defendants, IGT and Anchor Coin, Intervenor Defendants.
Circuit Court of Michigan, Wayne County
April 26, 2002
...In this case the plaintiff, Mary Kraft, seeks a money judgment against the defendants, who are the owners of gaming casinos in the City of Detroit, Michigan (the casino
defendants) or are the manufactu...
11. Fjolla v. Nacco Materials Handling Group, Inc.
2007 WL 6197429
Fjolla v. Nacco Materials Handling Group, Inc.
Circuit Court of Michigan, Oakland County
October 05, 2007
...At a session of said Court, held in the Court House, in the City of Pontiac, Oakland County, Michigan, this 4 day of October, 2007 PRESENT: THE HONORABLE STEVEN N.
ANDREWS, Circuit Judge This matter is...
12. See More Trial Court Documents
Preferences
My ContactsGlobal
Help
Live Chat
Sign Off
Westlaw. © 2016 Thomson Reuters
Privacy Statement
Accessibility
Su





























