Embed Size (px)
Citation preview

Gastrointestinal Disease in The Older Patient
Karen E. Hall, M.D., Ph.D.
Clinical Assistant ProfessorDepartment of Internal Medicine
University of Michigan Health System
Geriatric Research, Education and Care CenterAnn Arbor VA Health System
DDW New OrleansMay 18, 2004

1. Review of common gastrointestinal problems in older patients
2. Address controversies in treatment
3. Use questions from the 5th Edition of the American Geriatric Society Review
Syllabus
Objectives

Handouts
Handouts on my website:
http://sitemaker.umich.edu/khallinfo

Aging sets the stage for clinical impairment
Physiologic effects of aging
+
Superimposed disease
Effects of medications
=
“Clinical impairment in areas already at risk due to normal aging”

Question 1: Effect of aging on GI function
Which finding is more likely due to DISEASE rather than normal AGING?
1.Colonic diverticulosis
2.Dysphagia
3.Decreased small bowel motility
4.Decreased splanchnic blood flow
5.Decreased lower esophageal pressure

Answer: 3
Which finding is more likely due to DISEASE rather than normal AGING?
1.Colonic diverticulosis
2.Dysphagia
3.Decreased small bowel motility
4.Decreased splanchnic blood flow
5.Decreased lower esophageal pressure

Small bowel “resistant” to aging
In healthy older people there is minimal change in small bowel:
Motility
Secretion
Absorption
“Proximal and distal GI tract at greatest risk for dysfunction in aging”

Aging-associated changes in GI function
Studies in healthy older people have documented significant changes in:
Swallowing: slow bolus transit and airway closure
Splanchnic blood flow: decreased

Decreased blood supply to GI tract
Age > 70: Splanchnic Blood flow decreased by 30%
Atherosclerosis: IMA occluded in 20% autopsies
Esophagus, stomach, and proximal small bowel protected due to rich anastomotic supply
~ 20% decrease in blood flow to liverImpaired metabolism: drugs, bilirubinImpairs recovery from liver damage
“Watershed” areas: splenic flexure of colon (ischemic colitis)

Aging-associated changes in GI function
Colonic motility:
Slow transit:loss of myenteric neurons, sarcopeniadecreased prokinetic signaling: 5-HT3, 5-HT4, calcium, motilin
Increased intraluminal pressures:Loss of inhibitory nitric oxide signaling

Aging and Swallowing
Shaker and Staff. Gastroenterol Clin North Am 30:335, 2001
Proximal GI tract: Aspiration risk increases with age
Swallowing studies:40% of asymptomatic 80+ year olds have significant abnormalities
Asymptomatic aspiration in 10%

Aging and Swallowing
Kern et al. Ann Otol Rhinol Layngol 108: 982, 1999
1. No teeth: Impaired mastication
2. Impaired oropharyngeal co-ordination:Slow transit of food bolus, pooling at larynx
3. Delayed relaxation of upper esophageal sphincter (UES):
Food goes where it shouldn’t!

Reflux risk increases with age
Mean lower esophageal sphincter (LES ) pressure decreases with age:
Gastroesophageal reflux disease (GERD)
Prevalence:12-15% age <60
5-10% age >60 **underestimate
asymptomatic or atypical symptoms in 30% of elderly

Atypical reflux symptoms in elderly
Older patients:
esophageal: dyspepsia, nausea, dysphagia
aspiration: cough, hoarse voice, laryngitis, asthma, recurrent pneumonia
“Unexplained respiratory problems - GERD”

Question 2: Dysphagia
74 yo man has 1 yr trouble swallowing, nausea, no weight loss, chronic cough. No alcohol, stopped smoking. Meds: ACE, iron, diuretic, K+, vitaminPhysical “normal”. Hematocrit 34.
Which would you do next?1. Upper endoscopy (EGD)2. Esophageal Manometry3. pH monitoring4. Discontinue K+5. Trial of H2 antagonist

Answer: 1- Upper Endoscopy
74yo man has 1 yr trouble swallowing, nausea, no weight loss, chronic cough. No alcohol, stopped smoking. Meds: ACE, iron, diuretic, K+, vitaminPhysical “normal”. Hematocrit 34.
Which would you do next?1. Upper endoscopy (EGD)2. Esophageal Manometry3. pH monitoring4. Discontinue K+5. Trial of H2 antagonist

Investigation of dysphagia in older patients
Endoscopy indicated
Older patients: Higher risk of complicated GERD
UlcerationStricture Anemia Barrett’s esophagus
Increased incidence of esophageal cancer

Barrett’s Esophagus
Mucosa: Squamous to intestinal
Pre-malignant:Biopsy required to detect dysplastic epithelium
High grade dysplasia (HGD) has significant risk of progression to adenocarcinoma

Barrett’s Esophagus
Earlier studies: 7-10% risk of adenocarcinoma per year
Up to 1998-99:Screening EGD for patients with GERD history
2. +Barrett’s: biopsy HGD: surgical referral3. Low-Moderate Grade Dysplasia: high dose PPI4. Follow-up EGD every ? 6 months – 1 year?

Should we treat Barrett’s Esophagus?
Recent RCTs of PPI treatment of Barrett’s:
No significant effect on: Rate of progression of low-moderate dysplasia to HGD
Rate of esophageal adenocarcinoma
Screening EDG: esophageal cancer in 0.8%(10x expected population rate)

Why didn’t PPI treatment work?
? Not long enough (6 mo – 2 years)
? Genetic mutation already present
? Acid exposure not the only cause
? Biopsy error

Treatment of Barrett’s Esophagus
Current recommendations:
Screening EGD for patients with GERD history+Barrett’s: biopsy
+for HGD: surgical referral+for M-LGD: ?PPI + Follow-up EGD ?timing
“Future developments” - p53 antigen,cytometry
Dong Wang et al. Dis of the Esophagus, 15:80-4, 2002Conio M et al. Am J Gastroenterol. 98:1931-9, 2003.

GERD: Diagnosis and Treatment
Younger patients: “treat then scope”
if benign symptoms - acid blockade with antacids, H2 antagonist or PPI**
**GERD treatment $10 billion in 200070% medication costs
Sandler et al. Gastroenterol 122: 1500, 2002

GERD: Diagnosis and Treatment
Older patients:
“scope then treat”
Higher risk of neoplasia and complications of GERD

Back to Question 2: GERD
What about the other options?
Manometry, pH monitoring: may confirm esophageal spasm or acid but will not diagnose dysplasia or cancer
Discontinuing K+: EGD first - If ulceration and/or stricture observed with EGD then discontinue
H2 antagonist: Acid reduction sub-optimal for treatment of GERD, side effects (cimetidine)

Achalasia: Is a tight LES a good thing?
Subset of patients have pathologic increase in LES pressure termed Achalasia
0.5% prevalenceFemale: Male 4:1
Often “pretty old”: 75-85 years
“Progressive dysphagia to both liquids and solids occurring simultaneously”

Achalasia
LES: Extreme narrowing - “bird’s beak”
Swallow: LES relaxation poor or absent: inhibitory neurons absent or dysfunctional
Investigation: Barium swallow and esophagoscopy

Achalasia Treatment
1. Forcible balloon distensionRupture, mediastinitis, sepsis
2. Botulinum toxin injectionRelief x weeks-months (50% re-treat in 9 months vs 10% balloon)Risks/benefit better in frail pts?
3. Laparoscopic LES myotomy?similar risk/benefit as balloonLimited availability

Question 3: Aspiration pneumonia
69 yo male Nursing Home resident with dementia, GERD, tardive dyskinesia has productive cough, fever, hypoxia. CXR: right LL pneumonia.
After treatment of pneumonia, what you do next?1. Cervical xray to check for cervical spurs2. Discontinue antipsychotic medication3. Start metoclopramide4. Perform swallowing evaluation5. Place feeding tube

Answer: 4. Swallowing evaluation
69yo male NH resident with dementia, GERD, psychosis, tardive dyskinesia has productive cough, fever, hypoxia. CXR: right LL pneumonia.
After treatment of pneumonia, what you do next?1. Cervical xray to check for cervical spurs2. Discontinue antipsychotic medication3. Start metoclopramide4. Perform swallowing evaluation5. Place feeding tube

Aspiration pneumonia
Major risks for aspiration pneumonia in this patient:
Tardive dyskinesia (medication)GERD Impaired bolus transit: age, anticholinergic medications
Triple phase Swallowing study: fluoroscopyDiagnostic (severity; complications)Guide therapy

What about the other options?
Cervical spurs common, rarely cause dysphagia
Discontinuing antipsychotic or adding metoclopramide may worsen dyskinesia
Titrate antipsychotic down gradually to lower dose

Are feeding tubes indicated in dementia?
“Controversial topic”
Demented patients may live longer with a tubeIncreased calories
Cost: Poor quality of lifePain; restraints; ER visits; infection; bleeding
Aspiration and pneumonia risk not decreasedBacteria in saliva; reflux liquid diet

Feeding tubes in Dementia
Short-term mortality increased with feeding tubes50% mortality in 1 monthInfection, peritonitis, complications of re-insertionSanders et al. Am J Gastroenterol 95:1472-5, 2000.
Hand-feeding: Mortality and morbidity same as tube feeding
Nursing home costs much higher if patients fed by hand

Why not place a Feeding Tube?
Significant complications and ethical issues
Swallow study, adjust diet, medication first

Question 4: A constipated patient?86 yr man Nursing Home resident - has fever, emesis x 36 hours. History of HTN, CAD, diabetes, moderate dementia, acute MI 1 mo ago.
Temp 99.5; HR 112; BP 105/66; abdomen not tender; no guarding/rigidity; WBC 8; rest of lab tests normal; EKG: nonspecific ST changes.
Advance directives on file: wants hospital management of “reversible conditions”, no CPR

Question 4
What would you do next?
1. Serial abdominal exams and xrays in NH2. Serial EKGs and cardiac enzymes in NH3. Bowel regimen for constipation4. Fluids and antibiotics in NH5. To ER for urgent surgical evaluation

Answer: 5. Surgical Evaluation
What would you do next?
1. Serial abdominal exams and xrays in NH2. Serial EKGs and cardiac enzymes in NH3. Bowel regimen for constipation4. Fluids and antibiotics in NH5. To ER for urgent surgical evaluation

Acute Abdomen in the Older Patient
Morbidity and mortality: higher in geriatric patientsDue to delay in diagnosis
Symptoms vague/atypical:Rebound and guarding absent in 50-70%WBC: “normal” but may have left shiftConfusion, anorexia
“High index of suspicion needed”

Autonomic sensation impaired in aging
Age-associated decrease in visceral sensation
Peritonitis: tenderness and guarding often reduced or absent
Hall Am J Physiol 283: G827, 2002

Acute Abdomen in the Older Patient
Acute abdomen: potentially treatableappendicitis; diverticular abcess; ischemic colitis; cholecystitis
Patient’s Advance Directives: indicated desire for treatment of potentially reversible conditions

Question 4: the other options?
Patient already too ill for serial abdominal exams or cardiac enzymes in nursing home
Bowel regimen contraindicated if acute abdomen suspected – may cause perforation
Fluids and antibiotics in nursing home:Unlikely to prevent deterioration if surgical disease
If patient/family want “trial of therapy” rather than comfort care: NH treatment may not be feasible

Appendicitis in the Older Patient
Diagnosis at surgery: AppendicitisIncreased incidence: men aged 80+
70-90% have rupture at time of surgerydelay in diagnosis a major factor
6-10% mortality vs 0.5% in young
50% of deaths from appendicitis occur in aged

Diverticular Disease
> 70 % geriatric patients have diverticuli
Circular muscle: fewer fibers; larger spaces between fibersIncreased collagen between muscle bundles
Prolongation of muscle contractionIncreased intraluminal pressure
Mucosa/submucosa protrudes through wall =
Diverticulum

Diverticular disease
Caused 5000 deaths in 1998 (1/10 colon cancer rate)
Most deaths occurred in patients aged >75 years
Delay of diagnosis with perforation and abcess
Mortality rate: women 2.4 x higher than men
(more older women)

Diverticular disease
Presentation: usually some pelvic localization of symptoms, diarrhea or constipation, chills, (bleeding)
Rectal exam: localized tenderness or mass
CT scan may be helpful
Avoid flexible sigmoidoscopy!
Patient stable: trial of antibiotics, see again within a week
“Needs close observation”

Question 5: “The Bottom End”
89 yr woman NH resident with abdominal distension, mild confusion; Parkinson’s disease; hypertension; CHF; hypothyroidism; immobility. No pain, weight loss, appetite change.
Meds: Ca antagonist, digoxin, diuretic, levothyroxine, carbidopa/levodopa
Px: afebrile, abdomen distended, not tender, hard stool in rectum, no occult blood, CBC normal, abdominal films + CXR: no free air

Question 5
What should you do next?
1. Abdominal ultrasound2. Colonoscopy3. Discontinue Ca antagonist4. Administer enema5. Start prokinetic medication

Answer: 4 - Enema
What should you do next?
1. Abdominal ultrasound2. Colonoscopy3. Discontinue Ca antagonist4. Administer enema5. Start prokinetic medication

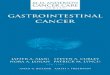
Constipation
0
5
10
15
20
25
30
Prevalence of
symptoms (%)
Pai
n
Con
stip
atio
n
Dia
rrhe
a
Fec
al in
cont
IBS
age 30-64age 65-93
Camilleri et al. JAGS 48:1142, 2000
*

Constipation in the elderly
Schiller Gastroent Clin North Am 30: 497, 2001
Multifactorial:
Aging-related colonic slowing
Immobile
Superimposed disease (Parkinson’s)
Medications (Ca antagonist, diuretic, levodopa)

Medications that cause constipation:The “Anti’s”
Schiller Gastroent Clin North Am 30: 497, 2001
Antihistamines: diphenhydramine, “Tylenol PM”Antihypertensives: atenolol, diltiazemAntidepressants: tricyclic - amitriptylineAntilipemics: cholestyramine, colestipolAntiparkinsonian: L-dopa/carbidopaAntipsychotics: haloperidol, resperidoneAntacids: aluminum-containing, sucralfateAnticonvulsants: phenytoinAnalgesics: opiates

Constipation
Initiate a bowel regimen1.“Get things moving from below first”
SuppositoryEnema: phospho-soda
tap water (not soapsuds –colitis) Dis-impaction (by your assistant!)
2. Optimize hydration and mobility
3. Maintenance: cathartic/osmotic laxative (Milk of magnesia; Dulcolax; senna; PEG solution)

Constipation
Avoid:1. Initial oral cathartics: potentially dangerous if
severely constipated“Use when bowels are moving”
2. Mineral oil by mouth: lipoid pneumonia
3. Fiber alone: unlikely to work and may cause impaction
4. Antispasmodics: anticholinergic and serotonin antagonists associated with fatal ischemic colitis

What about Tegaserod maleate (Zelnormc)?
5-HT4 agonistconstipation-predominant IBSOnly effective in women
Limited data - safe in older patientsContraindications: severe renal failure, hepatic disease, symptomatic gallbladder, previous bowel adhesions
2 mg bid – increase to 6 mg bid if toleratedNo adjustment for mild-moderate renal failure

Diarrhea
Less common than constipation, more socially debilitating
Infectious: older patients higher riskHistory of travel or problem foodsCheck hydration statusStool cultures, fecal occult bloodRectal: impaction with overflowDiverticulitis

Diarrhea in Aging population
Acute: Outpatient vs Inpatient management:
Bleeding, fever, chills (enteroinvasive)
Live alone, poor hydration/nutrition, disabled
Avoid endoscopy until infection and/or acute abdomen ruled out

Diarrhea in Aging population
Chronic: If stable: recommend colonoscopyMicroscopic/lymphocytic colitisCollagenous colitisIBD (inflammatory)Structural: pelvic laxity, fissureIrritable bowel syndrome
Treatment: antidiarrheals (Imodium)soluble fiber, cholestyramine5-ASA or steroids for severe colitisREVIEW MEDs – antiarrhythmics, Aricept©

What about Alosetron (Lotronex©)?
5-HT3 antagonistDiarrhea-predominant irritable bowel syndromeOnly effective in women
No Pre-market studies performed > age 457/1000 incidence of hospitalization for:Severe constipation, colitis, death – older patients
Withdrawn in 2000, re-released in 20021 mg/day – 1 mg bidDISCONTINUE IF CONSTIPATION OCCURS

Colon Cancer: a disease of Aging
1.7 million office visits, 45,000 deaths in 2000

Colon Cancer: a disease of Aging
80-90% of tumors arise from colon polyps
70% of age >65 have polyps, those who don’t by age 75 are probably never going to
Colonoscopy is screening method of choiceIncreased prevalence of right-sided tumorsPolypectomy decreases cancer incidence
Medicare - once every 10 years

Colon Cancer
Recommendations for screening:
Colonoscopy age 55-60 then q 10 years to age 85
Continue yearly FOB
Barium enema if colonoscopy fails

Colon Cancer: What if patient is over 85?
Use your best judgement:
Functional status/cognition
Expected life span > 5 years
Patient’s wishes
Gastroenterologist’s wishes

Colon Cancer – new tests
Virtual colonoscopySensitivity/specificity 85-90% for polyps >1cmCannot remove or biopsy tissue
Stool DNA testing“Not ready for prime time”Lot of candidate genes: p53, Apc, K-ras, BAT-26Variable expression (40-80% of Dukes A-D)Longer DNA fragments may indicate neoplasm

Colon Cancer
Recommended follow-up of polyps:
Yearly FOB
Colonoscopy:at 1 year for high grade lesions (villous, polyps >2 cm, HGD). then q 3-5 years
at 3-5 years for low grade lesions

Colon CancerWhat about primary prevention?
NSAIDs, calcium, Vitamin D may decrease risk of polyps
Fiber: controversial + and – studies May be better with Vitamin D
Pignone M, Levin B. Am Fam Physician. 2002 Jul 15;66(2):297-302.Lieberman et al. JAMA 290:2959-2967, 2003.

Handouts
Reviews:Physiology: Am J Physiol 283:G827-832, 2002Gastro Clinics North America 30, 2001Geriatric Review Syllabus 5th Editionhttp://www.americangeriatrics.org/products/grs5.shtml
Handouts on my website:
http://sitemaker.umich.edu/khallinfo