Embed Size (px)
Citation preview
Gastroenteropancreatic and Bronchopulmonary Neuroendocrine Tumors
Overview
Gastroenteropancreatic and Bronchopulmonary Neuroendocrine Tumors
Overview
Edda Gomez-Panzani, M.D.
2 EGP MD
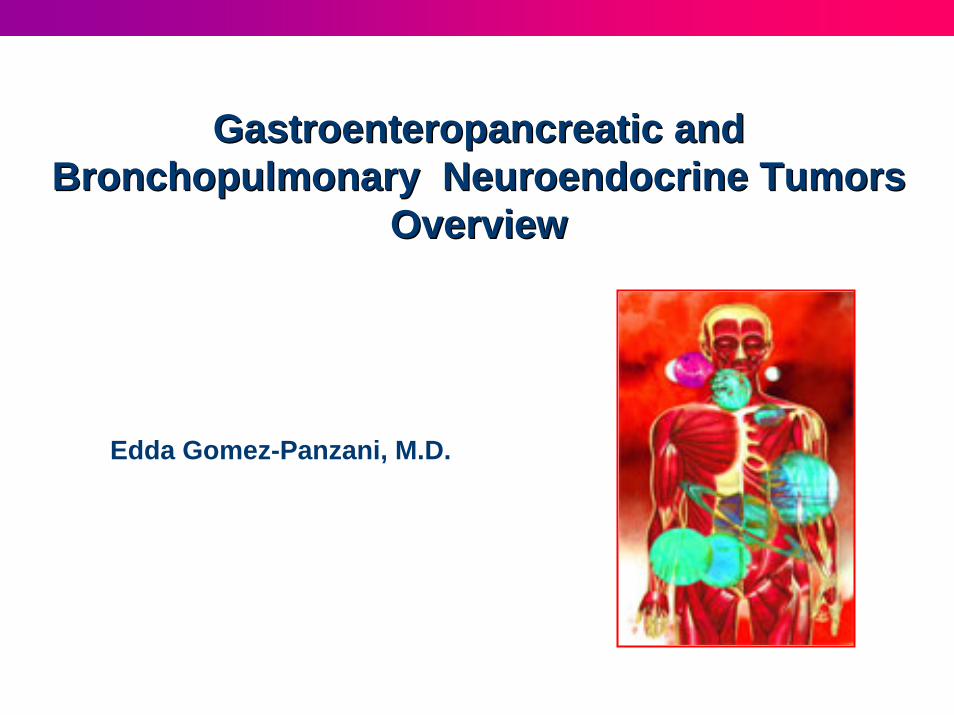
The genes are the coded messages in a cell that guide its behavior; they are packed in bundles called chromosomes
http://dels-old.nas.edu/plant_genome/images/DNA.jpg
Genes and chromosomes
Fluo
resc
ent I
n-Si
tuH
ybrid
izat
ion
(FIS
H) i
dent
ifica
tion
of H
uman
C
hrom
osom
es
3 EGP MD
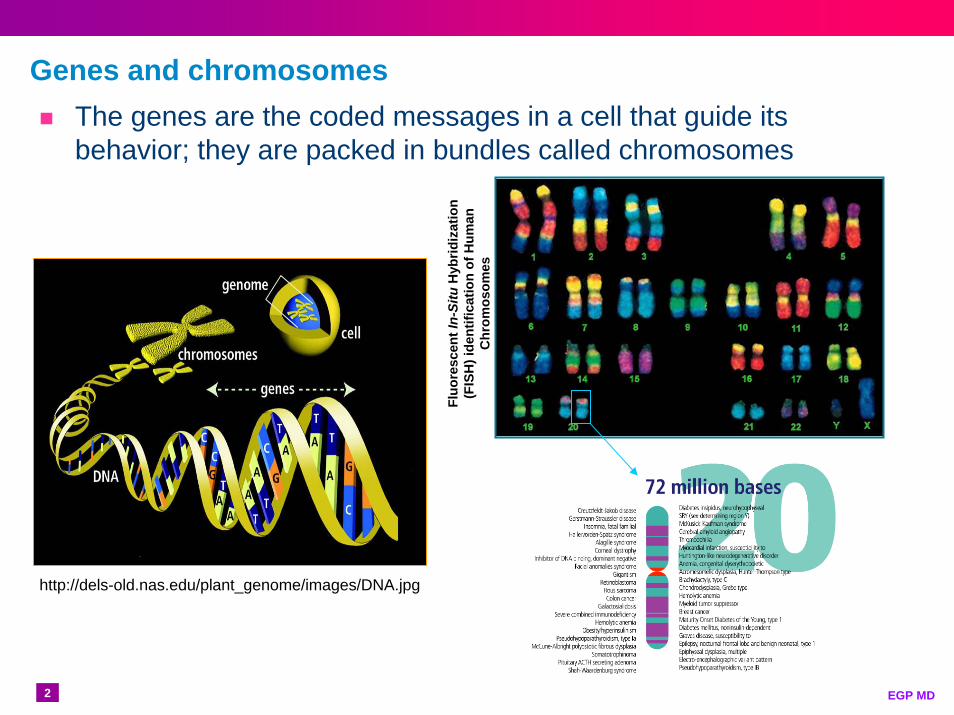
Normal cell cycle
http://www2.le.ac.uk/departments/genetics/vgec/diagrams/22-Cell-cycle.gif
http://www.cbp.pitt.edu/faculty/yong_wan/images/main_cell_cycle.jpg

4 EGP MD
Sometimes, mutations occur. Mutations are changes in the genes that result in the cells changing their behavior.
These changes can involve losses, alterations or gains in the important cell control systems related to growth, interaction with other cells and even cells’ life span
Once damage occurs, it can be:Reversed
Removed
Toleratedhttp://www.cancer.gov/PublishedContent/Images/images
/documents/2bb8687b-eb2b-4e62-ba30-a0572dee414e/cancer10.jpg
Errors during the cell cycle
5 EGP MD
Mutations
Muhammad Mahdi Karim (www.micro2macro.net)Own work by uploader, http://bjornfree.com/galleries.htmlAuthor=Bjørn Christian Tørrissen Date=2010-04-10
http://forums2.gardenweb.com/forums/load/annuals/msg070249178518.html

6 EGP MD
Apoptosis (Programmed Cell Death)Some times, when the damage is significant and it cannot be repaired or removed, the cell goes through a process of programmed cell death called apoptosisApoptosis: A normal, genetically regulated process leading to the death of cells and triggered by the presence or absence of certain stimuli, as DNA damage www.dictionary.com
http://www.microbiologybytes.com/virology/kalmakoff/baculo/pics/Apoptosis.gif
7 EGP MD
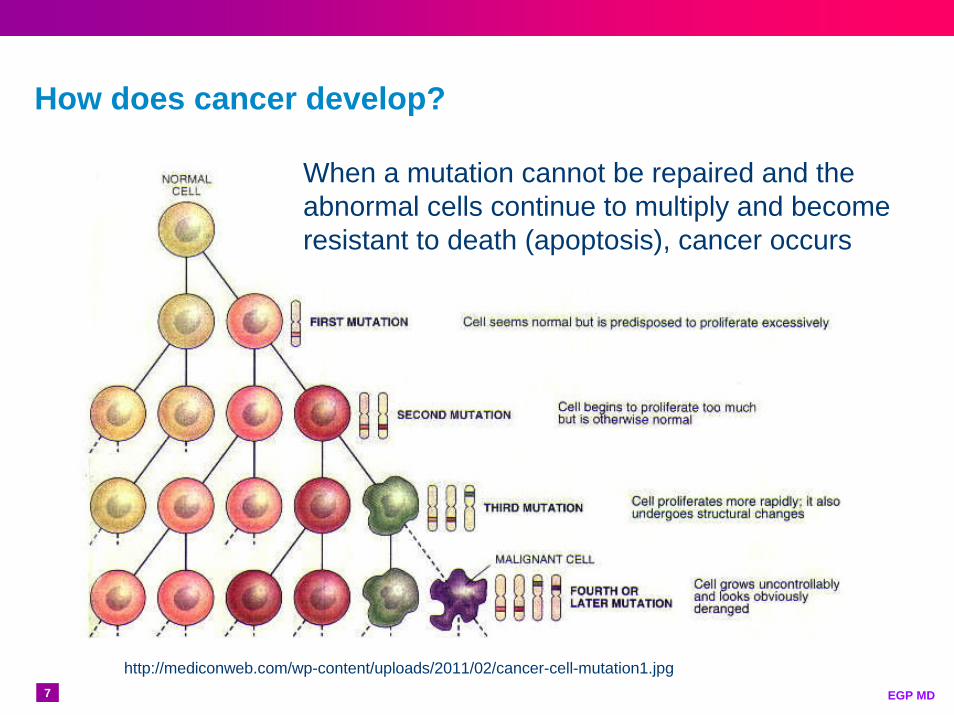
How does cancer develop?
http://mediconweb.com/wp-content/uploads/2011/02/cancer-cell-mutation1.jpg
When a mutation cannot be repaired and the abnormal cells continue to multiply and become resistant to death (apoptosis), cancer occurs
8 EGP MD
Mutations
http://msucares.com/news/print/sgnews/sg11/sg110824.htmlPhoto by Gary Bachman
http://forums2.gardenweb.com/forums/load/annuals/msg070249178518.html
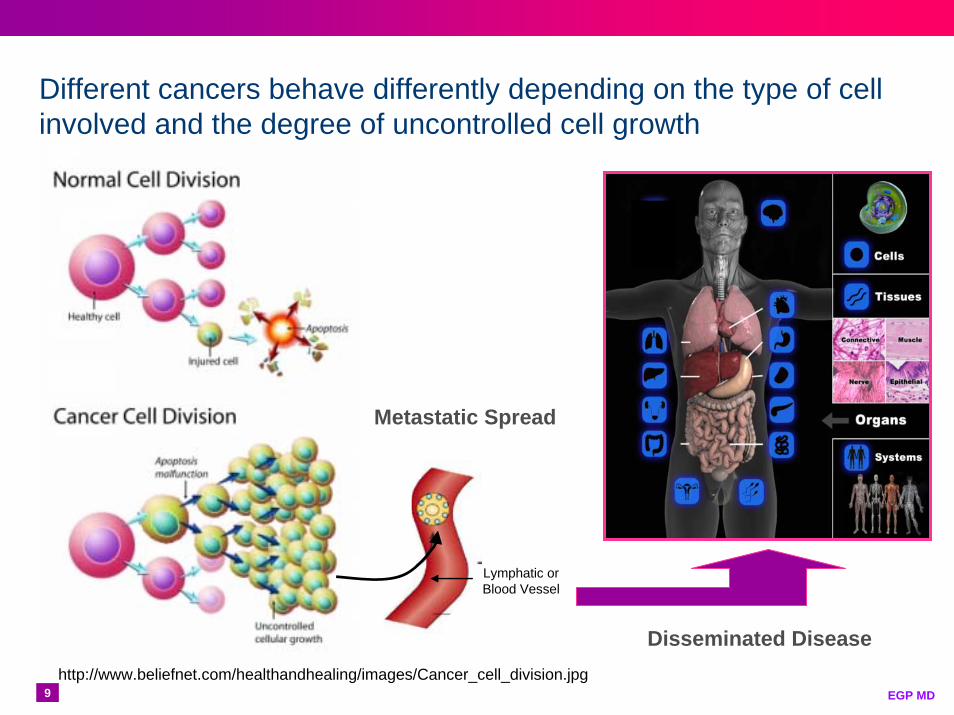
9 EGP MDhttp://www.beliefnet.com/healthandhealing/images/Cancer_cell_division.jpg
Lymphatic orBlood Vessel
Metastatic Spread
Disseminated Disease
Different cancers behave differently depending on the type of cell involved and the degree of uncontrolled cell growth
10 EGP MD
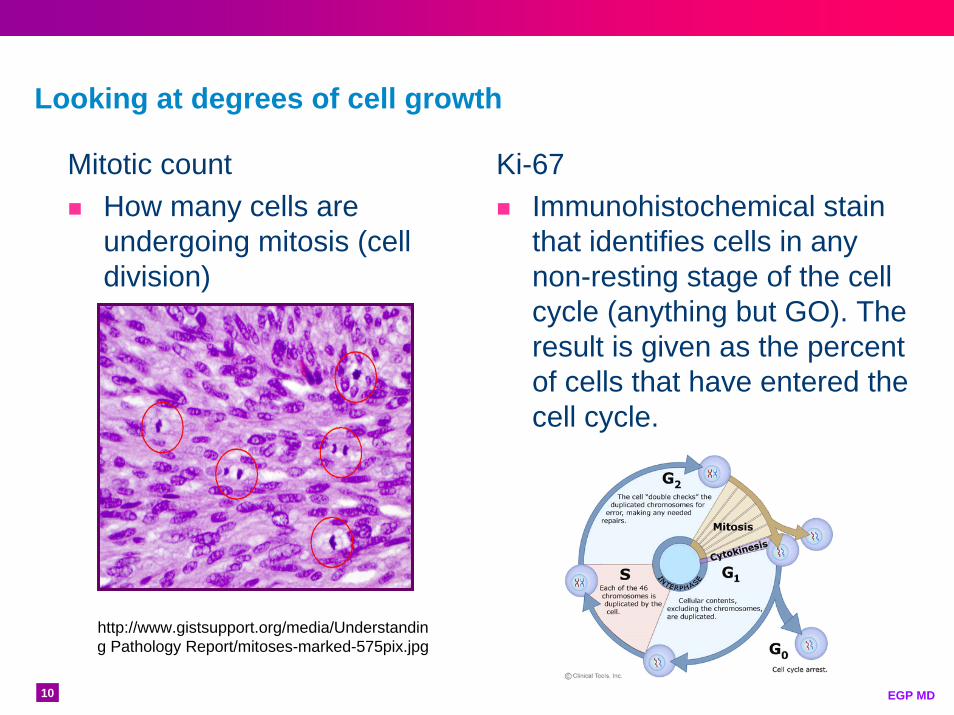
Looking at degrees of cell growth
http://www.gistsupport.org/media/Understanding Pathology Report/mitoses-marked-575pix.jpg
Ki-67Immunohistochemical stain that identifies cells in any non-resting stage of the cell cycle (anything but GO). The result is given as the percent of cells that have entered the cell cycle.
Mitotic countHow many cells are undergoing mitosis (cell division)
11 EGP MD

12 EGP MD
Merkel cell tumors (skin)
Anterior pituitary gland• Adenoma
Endocrine tumors in miscellaneous sites
• Ovary, cervix, endometrium
• Breast• Prostate• Medullary thyroid
carcinoma• Kidney• Larynx, paranasal
sinuses, salivary glands
Pheochromocytomas and
Paragangliomas
Bronchopulmonary and Thymic endocrine tumors
• Thymic carcinoid• Tumorlets• Typical and atypical lung
carcinoid • Small cell lung cancer• Large cell lung cancer
GI endocrine tumors• Carcinoid Tumors• Undifferentiated NE
carcinomas
Pancreatic endocrine tumors• Non-functional• Insulinoma• Gastrinoma• VIPoma• Glucagonoma• Somatostatinoma• ACTH-oma
Neuroendocrine Tumors (NETs)
NEUROENDOCRINE
TUMORS

13 EGP MD
Neuroendocrine Tumors (NETs) – Incidence
0
1
2
3
4
5
6
19731974197519761977197819791980198119821983198419851986198719881989199019911992199319941995199619971998199920002001200220032004
Inci
denc
e pe
r 100
,000
Year
Yao C. J. et al. J. of Clin Onc. 2008. 26;18:3063-3072.
SEER9 SEER13 SEER17

14 EGP MD
Gastro-Entero-Pancreatic (GEP) and Bronchopulmonary (BP) NETs – Incidence
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
197319751977197919811983198519871989199119931995199719992001200320052007
LungSmall IntestineRectumPancreas
Inci
denc
e pe
r 100
,000
YearYao C. J. et al. J. of Clin Onc. 2008. 26;18:3063-3072 and Age-adjusted incidences for NETs from the SEER (1973-2007) tumor registry database.
15 EGP MD
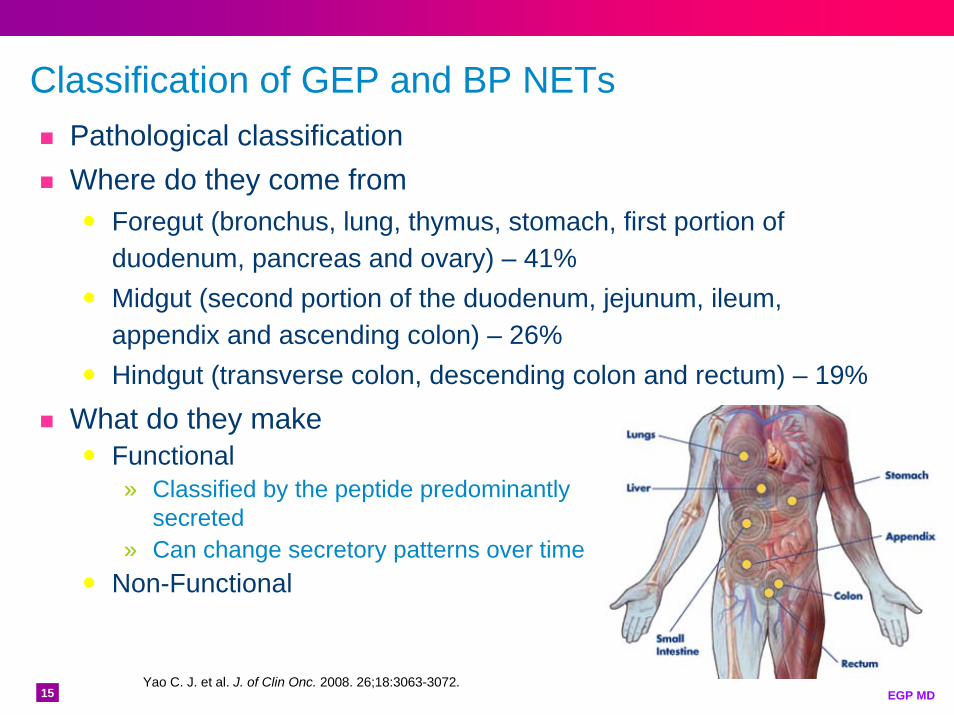
Classification of GEP and BP NETsPathological classificationWhere do they come from
Foregut (bronchus, lung, thymus, stomach, first portion of duodenum, pancreas and ovary) – 41%Midgut (second portion of the duodenum, jejunum, ileum, appendix and ascending colon) – 26%Hindgut (transverse colon, descending colon and rectum) – 19%
What do they makeFunctional» Classified by the peptide predominantly
secreted» Can change secretory patterns over time
Non-Functional
Yao C. J. et al. J. of Clin Onc. 2008. 26;18:3063-3072.
16 EGP MD
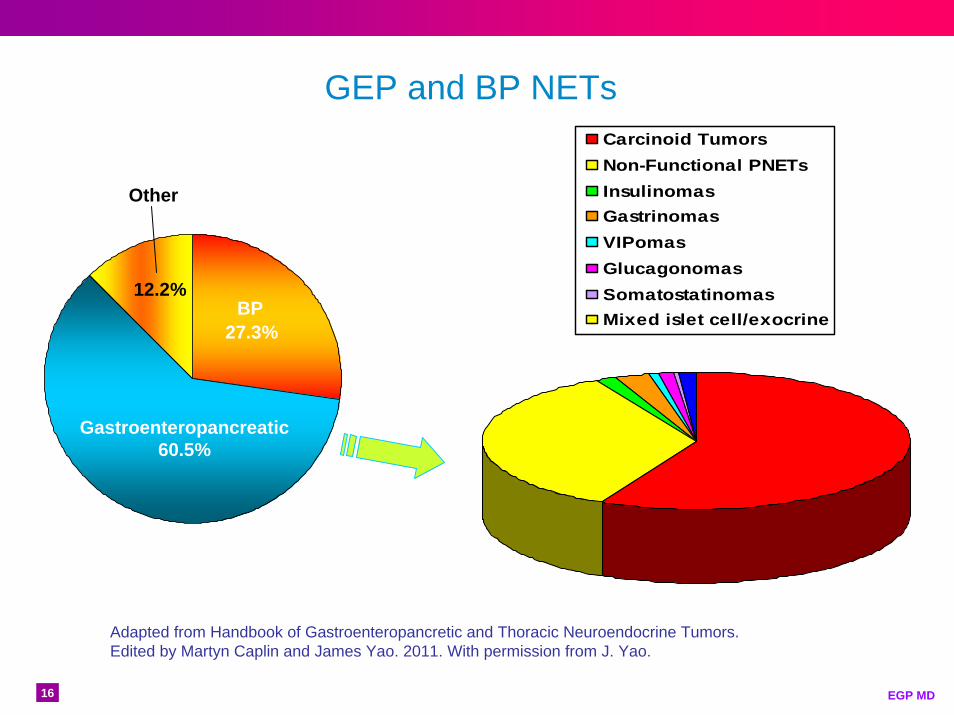
Carcinoid TumorsNon-Functional PNETsInsulinomasGastrinomasVIPomasGlucagonomasSomatostatinomasMixed islet cell/exocrine
Gastroenteropancreatic 60.5%
27.3%BP
12.2%
Other
GEP and BP NETs
Adapted from Handbook of Gastroenteropancretic and Thoracic Neuroendocrine Tumors. Edited by Martyn Caplin and James Yao. 2011. With permission from J. Yao.
17 EGP MD
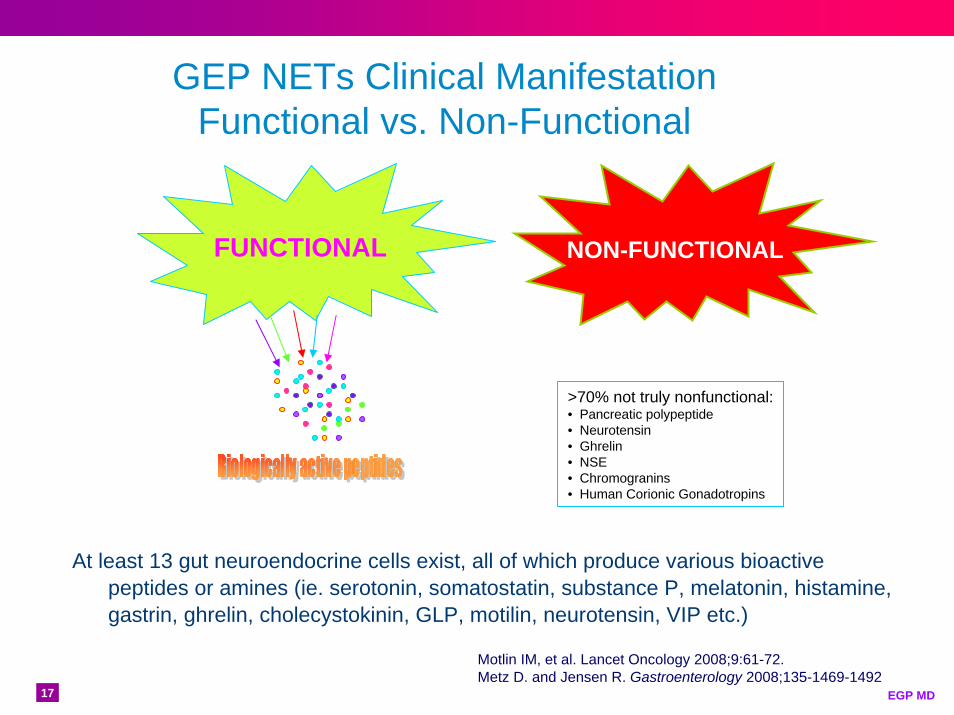
GEP NETs Clinical Manifestation Functional vs. Non-Functional
At least 13 gut neuroendocrine cells exist, all of which produce various bioactive peptides or amines (ie. serotonin, somatostatin, substance P, melatonin, histamine, gastrin, ghrelin, cholecystokinin, GLP, motilin, neurotensin, VIP etc.)
>70% not truly nonfunctional:• Pancreatic polypeptide• Neurotensin• Ghrelin• NSE• Chromogranins• Human Corionic Gonadotropins
Motlin IM, et al. Lancet Oncology 2008;9:61-72.Metz D. and Jensen R. Gastroenterology 2008;135-1469-1492
FUNCTIONAL NON-FUNCTIONAL
18 EGP MD
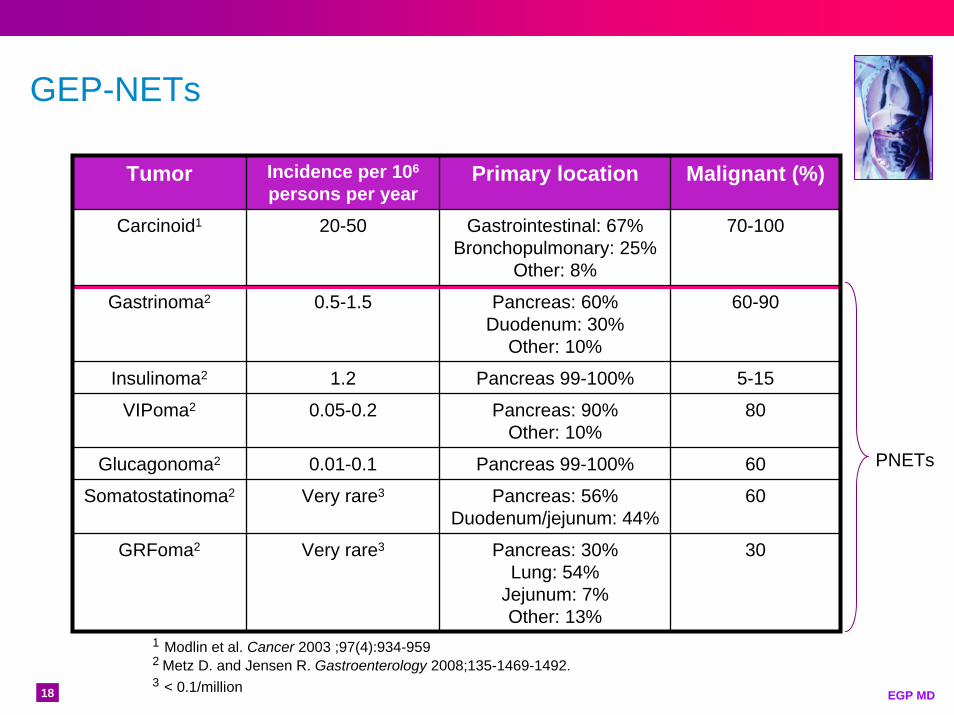
GEP-NETs
Tumor Incidence per 106
persons per yearPrimary location Malignant (%)
Carcinoid1 20-50 Gastrointestinal: 67%Bronchopulmonary: 25%
Other: 8%
70-100
0.5-1.5
1.2
0.05-0.2
0.01-0.1
Very rare3
Very rare3
Gastrinoma2 Pancreas: 60%Duodenum: 30%
Other: 10%
Insulinoma2 Pancreas 99-100% 5-15
VIPoma2 Pancreas: 90%Other: 10%
80
Glucagonoma2 Pancreas 99-100% 60
Somatostatinoma2 Pancreas: 56%Duodenum/jejunum: 44%
60
GRFoma2
60-90
Pancreas: 30%Lung: 54%
Jejunum: 7%Other: 13%
30
1 Modlin et al. Cancer 2003 ;97(4):934-9592 Metz D. and Jensen R. Gastroenterology 2008;135-1469-1492.3 < 0.1/million
PNETs
19 EGP MD
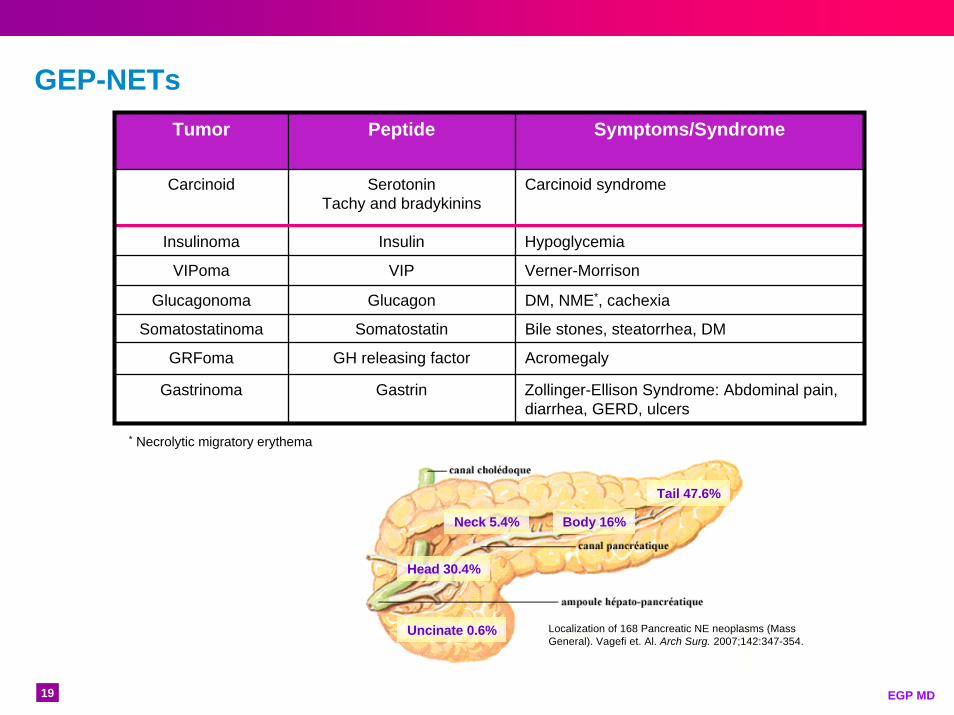
GEP-NETsTumor Peptide Symptoms/Syndrome
Carcinoid SerotoninTachy and bradykinins
Carcinoid syndrome
Insulinoma Insulin Hypoglycemia
VIPoma VIP Verner-Morrison
Glucagonoma Glucagon DM, NME*, cachexia
Somatostatinoma Somatostatin Bile stones, steatorrhea, DM
GRFoma GH releasing factor Acromegaly
Gastrinoma Gastrin Zollinger-Ellison Syndrome: Abdominal pain, diarrhea, GERD, ulcers
* Necrolytic migratory erythema
Head 30.4%
Uncinate 0.6%
Tail 47.6%
Neck 5.4% Body 16%
Localization of 168 Pancreatic NE neoplasms (Mass General). Vagefi et. Al. Arch Surg. 2007;142:347-354.
20 EGP MD©Edda Gomez-Panzani
21 EGP MD
Siegfried Obendorfer 1907
Carcinoid (Karzinoide)
Adenoma Carcinoid Carcinoma
Benign Tumors Malignant Tumors
22 EGP MD
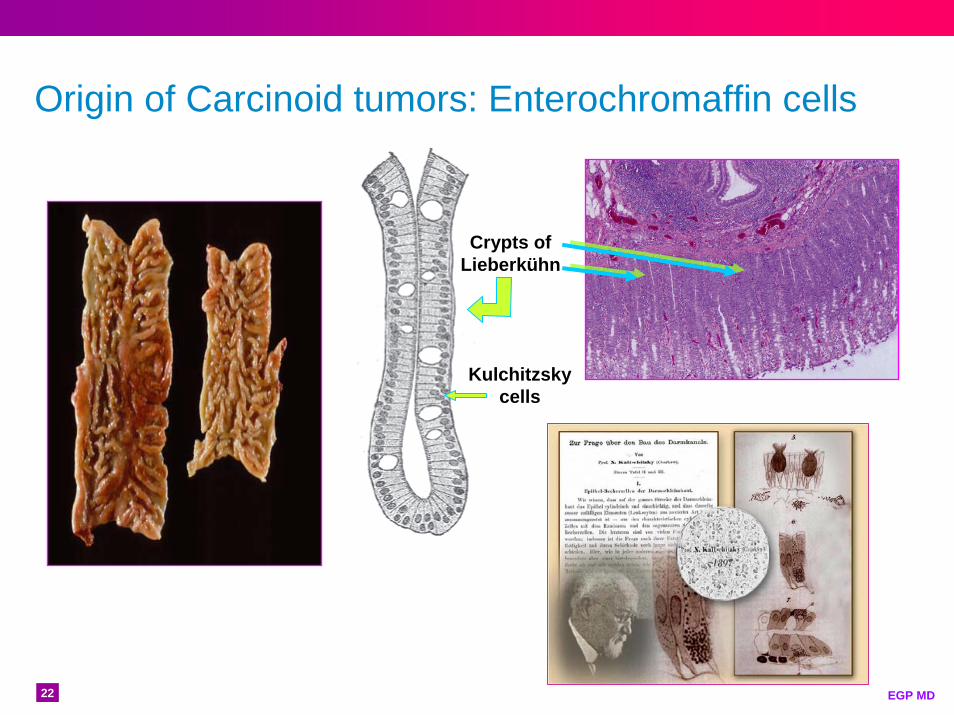
Origin of Carcinoid tumors: Enterochromaffin cells
Crypts of Lieberkühn
Kulchitzsky cells

23 EGP MD
Intestinal Carcinoid tumors
24 EGP MD
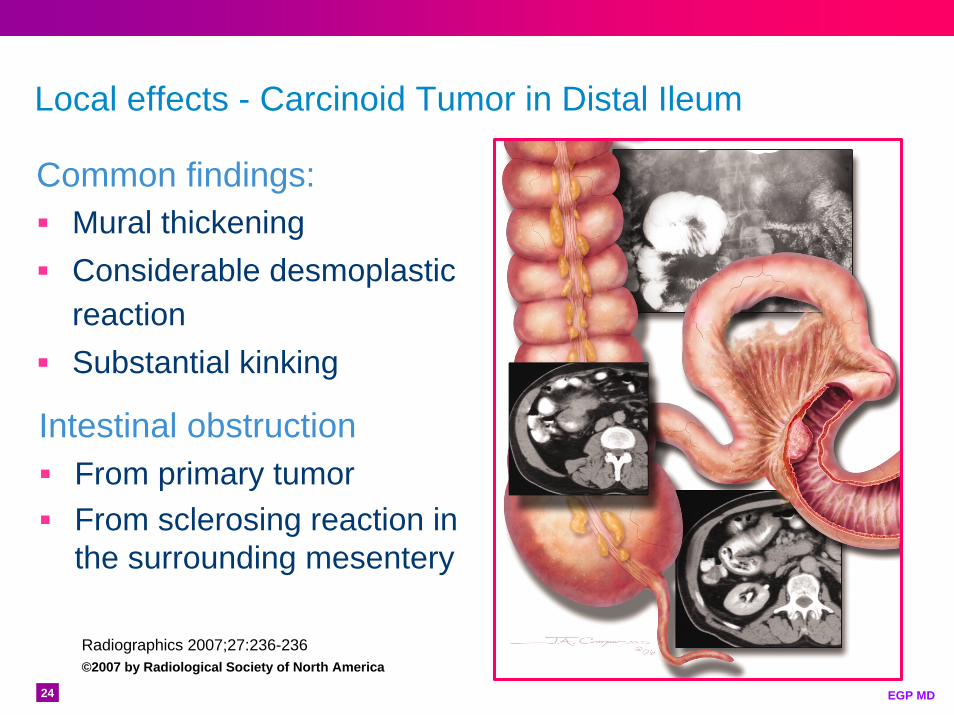
Local effects - Carcinoid Tumor in Distal Ileum
Common findings:Mural thickeningConsiderable desmoplastic reactionSubstantial kinking
Radiographics 2007;27:236-236©2007 by Radiological Society of North America
Intestinal obstructionFrom primary tumorFrom sclerosing reaction in the surrounding mesentery
25 EGP MD
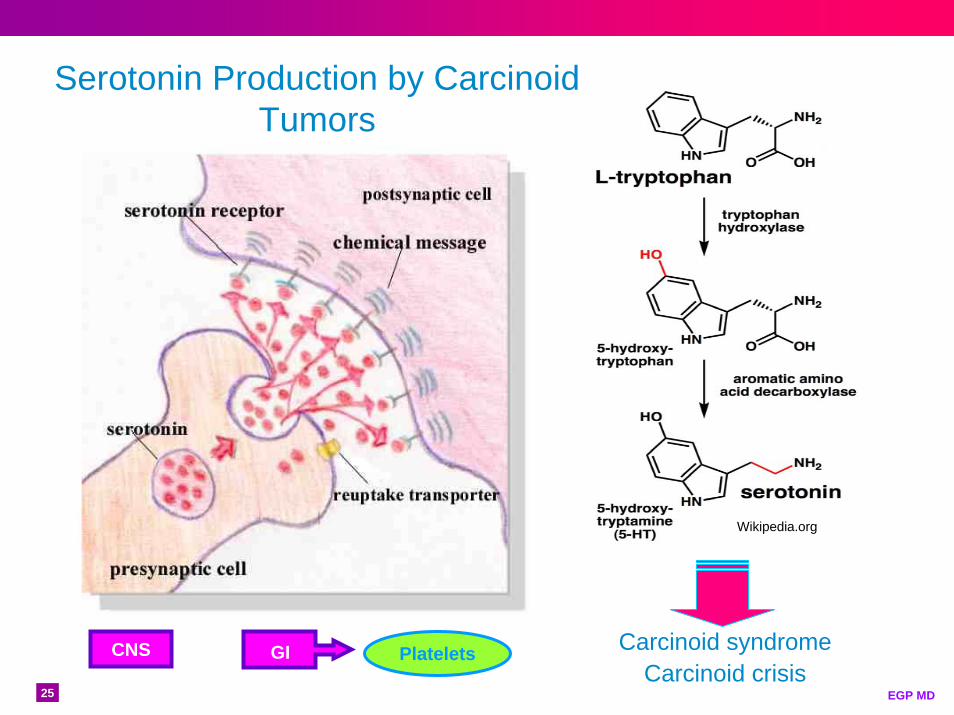
Serotonin Production by Carcinoid Tumors
Wikipedia.org
PlateletsCNS GI Carcinoid syndromeCarcinoid crisis
26 EGP MD
Functional vs. Non-Functional
What role does the liver play?

27 EGP MD
The liver
From: Biomedical CommunicationsArizona Health Sciences Center
28 EGP MD
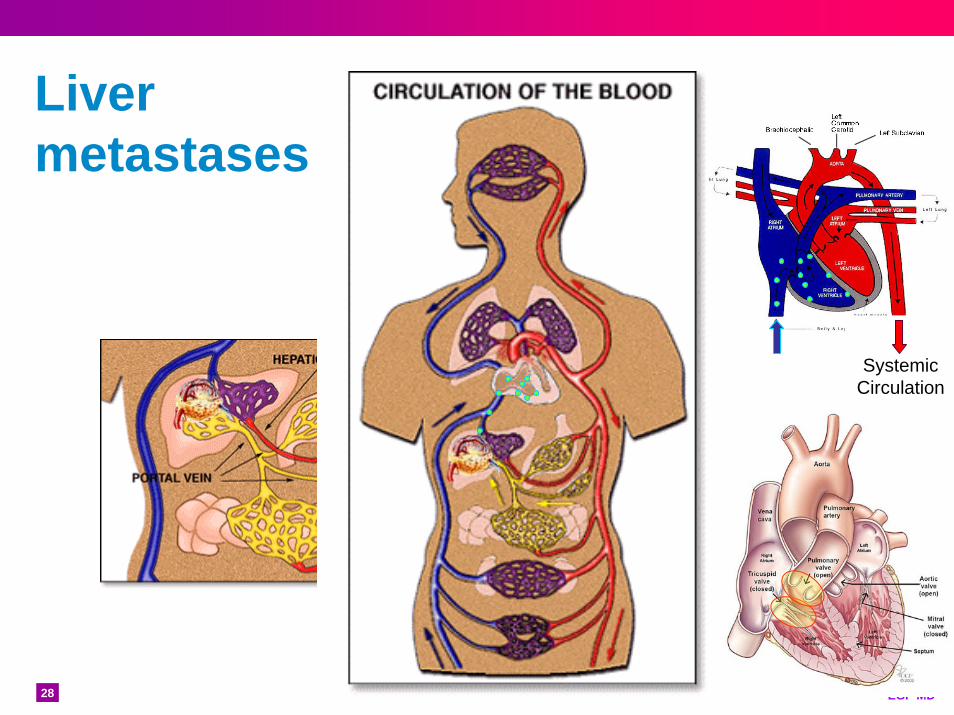
Liver metastases
Systemic Circulation

29 EGP MD
Carcinoid Syndrome
The occurrence and severity of the syndrome is directly related to tumor bulk in an area that drains into the systemic circulationIn the vast majority of cases this correlates to hepatic metastases

30 EGP MD
Syndrome without liver metastases
Exceptions include:» Peritoneal carcinomatosis» Primary ovarian carcinoids» Broncopulmonary carcinoids
Peritoneal carcinomatosis arising from appendiceal tumor
Glockzin et al. World Journal of Surgical Oncology2009 7:5 doi:10.1186/1477-7819-7-5
31 EGP MD
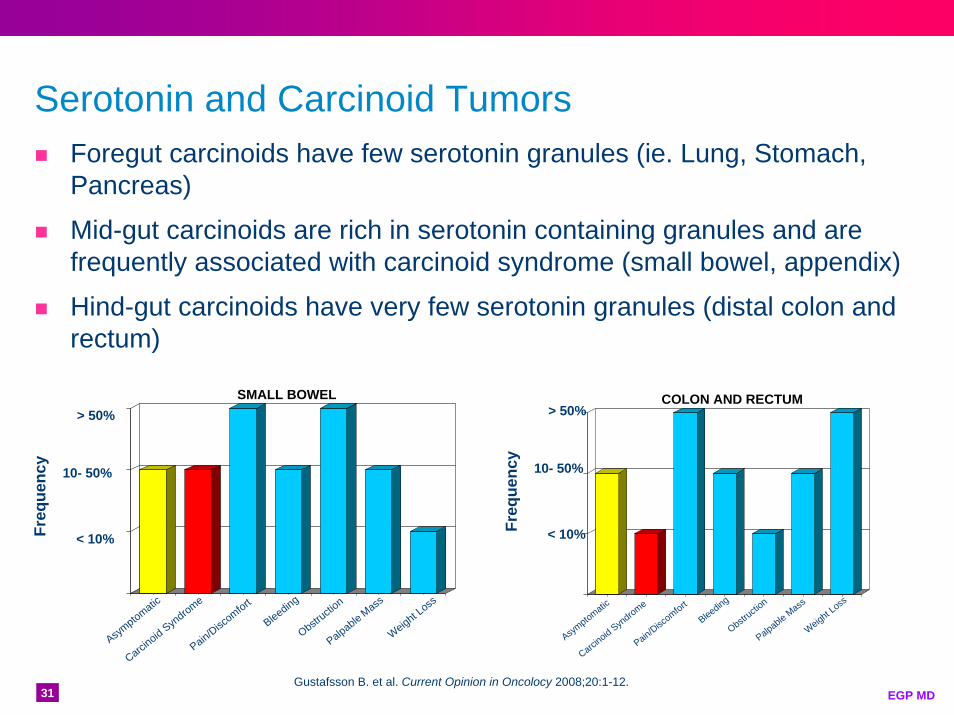
Serotonin and Carcinoid TumorsForegut carcinoids have few serotonin granules (ie. Lung, Stomach, Pancreas)
Mid-gut carcinoids are rich in serotonin containing granules and arefrequently associated with carcinoid syndrome (small bowel, appendix)
Hind-gut carcinoids have very few serotonin granules (distal colon and rectum)
Freq
uenc
y
> 50%
10- 50%
< 10%
Asymptomatic
Gustafsson B. et al. Current Opinion in Oncolocy 2008;20:1-12.
Carcinoid Syn
drome
Pain/Discomfort
Bleeding
Obstructio
n
Palpable Mass
Weight Loss
Asymptomatic
Carcinoid Syndrome
Pain/Discomfort
Bleeding
Obstructio
n
Palpable Mass
Weight Loss
Freq
uenc
y
> 50%
10- 50%
< 10%
COLON AND RECTUMSMALL BOWEL
32 EGP MD
Carcinoid Syndrome
In 10% of patients with carcinoid tumors1954 – Thorson and Waldenstrom
Malignant carcinoid of the small intestineMetastases to the liverPeripheral vasomotor symptoms (flushing)DiarrheaValvular disease of the right side of the heart (pulmonary stenosis and tricuspid regurgitation without septal defects)BronchoconstrictionAbdominal pain

33 EGP MD
Frequency of Carcinoid Syndrome by Primary Organ site location of Carcinoid Tumor
Freq
uenc
y
> 50%
10- 50%
< 10%
Stomach
Small Intestin
e
Appendix
Colon and
Rectum
Adapted from Gustafsson B. et al. Current Opinion in Oncology 2008;20:1-12.
Bronchopulm
onary
34 EGP MD
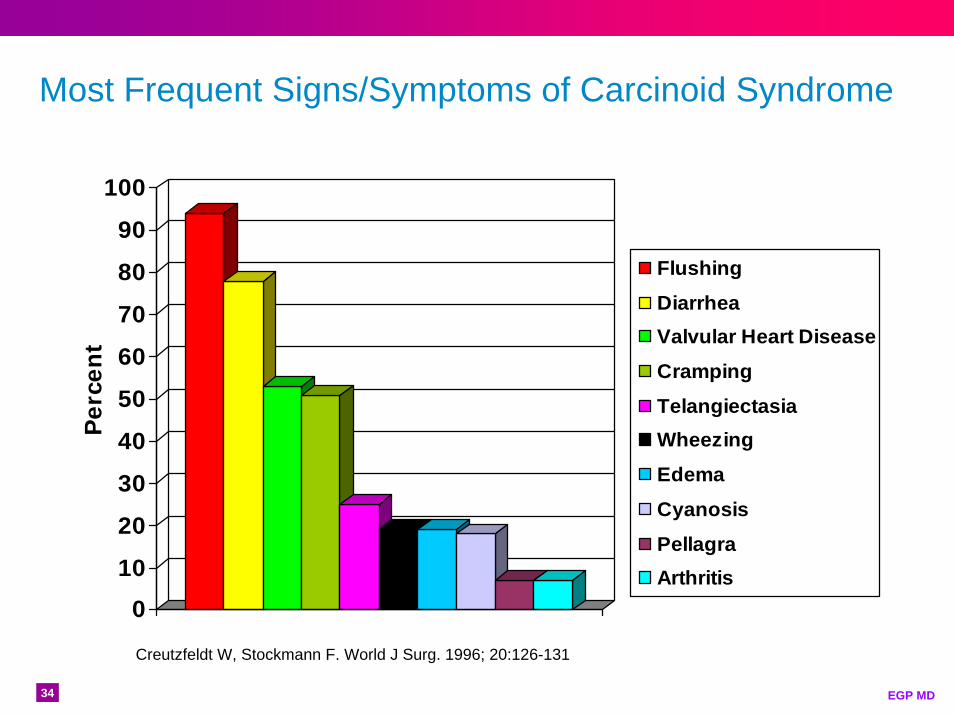
Most Frequent Signs/Symptoms of Carcinoid Syndrome
0
10
20
30
40
50
60
70
80
90
100
Flushing
DiarrheaValvular Heart Disease
Cramping
TelangiectasiaWheezing
Edema
Cyanosis
PellagraArthritis
Creutzfeldt W, Stockmann F. World J Surg. 1996; 20:126-131
Per
cen
t
35 EGP MD
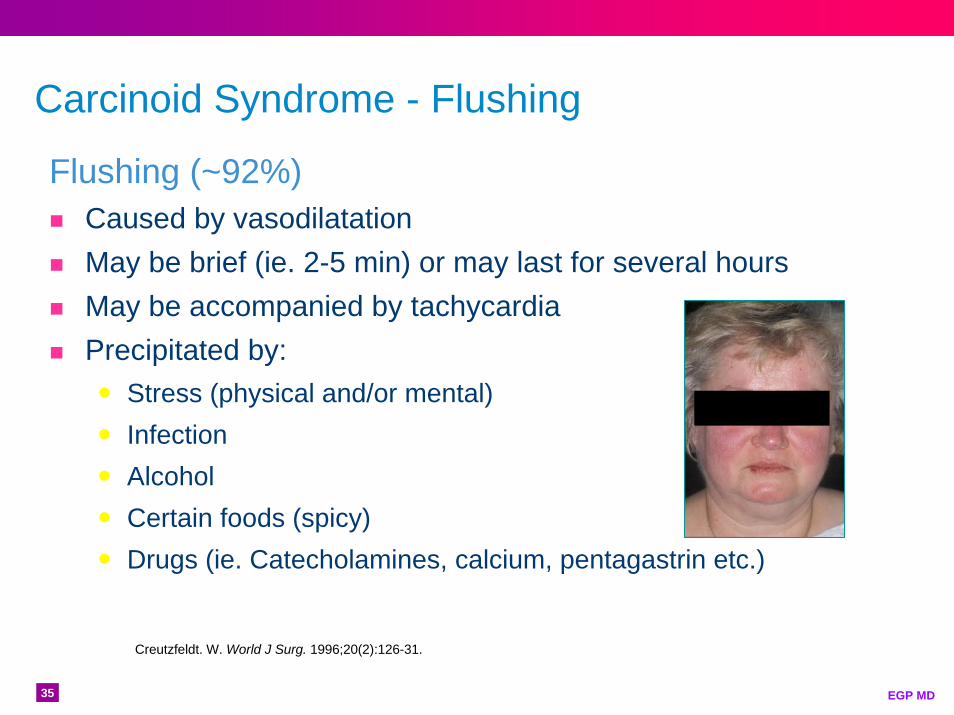
Carcinoid Syndrome - Flushing
Flushing (~92%)Caused by vasodilatationMay be brief (ie. 2-5 min) or may last for several hoursMay be accompanied by tachycardiaPrecipitated by:
Stress (physical and/or mental)InfectionAlcoholCertain foods (spicy)Drugs (ie. Catecholamines, calcium, pentagastrin etc.)
Creutzfeldt. W. World J Surg. 1996;20(2):126-31.
36 EGP MD
Carcinoid Syndrome - Diarrhea
Diarrhea (~78%)
Serotonin and Substance P stimulate small bowel and colonic motility
Post-prandial transit times in the small bowel and colon have been reported (von der Ohne et al.) to be 2 to 6 times faster in carcinoid patients than in healthy individuals. Fasting colonic times are normal.
Malabsorption can result in fluid and electrolyte imbalance, malnutrition, pellagra etc.
May be accompanied by borborygmi, cramping and or pain
Walter Sutton’s sketch of the GI system- 1905. Clendening Medical Library, Univ. of Kansas Med. Ctr.
Creutzfeldt. W. World J Surg. 1996;20(2):126-31.
37 EGP MD
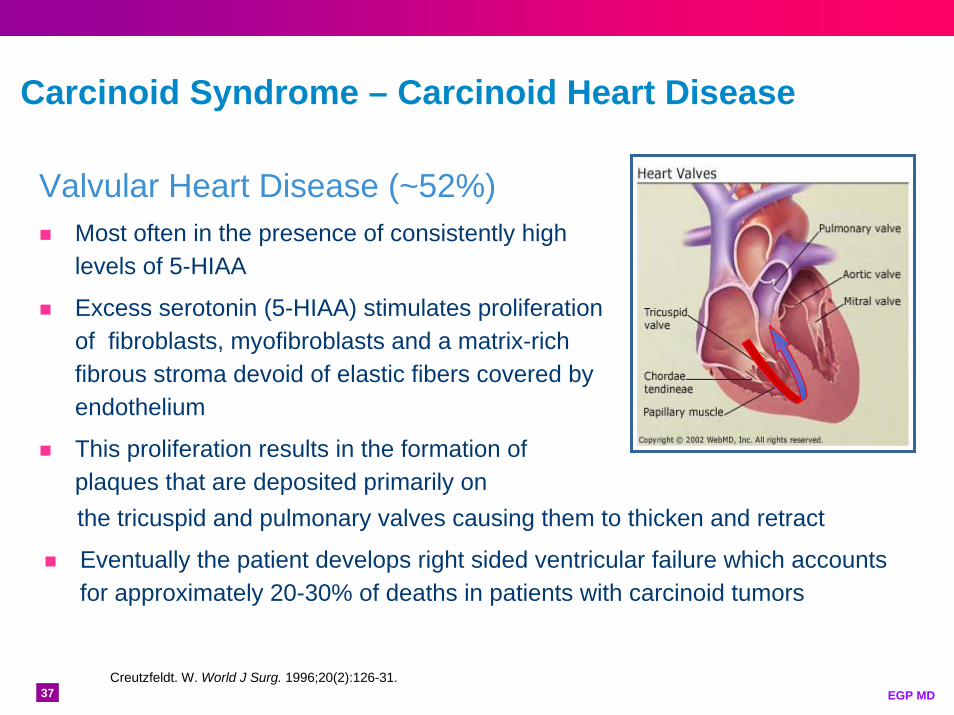
Carcinoid Syndrome – Carcinoid Heart Disease
Valvular Heart Disease (~52%)Most often in the presence of consistently high levels of 5-HIAA
Excess serotonin (5-HIAA) stimulates proliferation of fibroblasts, myofibroblasts and a matrix-rich fibrous stroma devoid of elastic fibers covered by endothelium
This proliferation results in the formation of plaques that are deposited primarily on the tricuspid and pulmonary valves causing them to thicken and retract
Eventually the patient develops right sided ventricular failure which accounts for approximately 20-30% of deaths in patients with carcinoid tumors
Creutzfeldt. W. World J Surg. 1996;20(2):126-31.
38 EGP MD
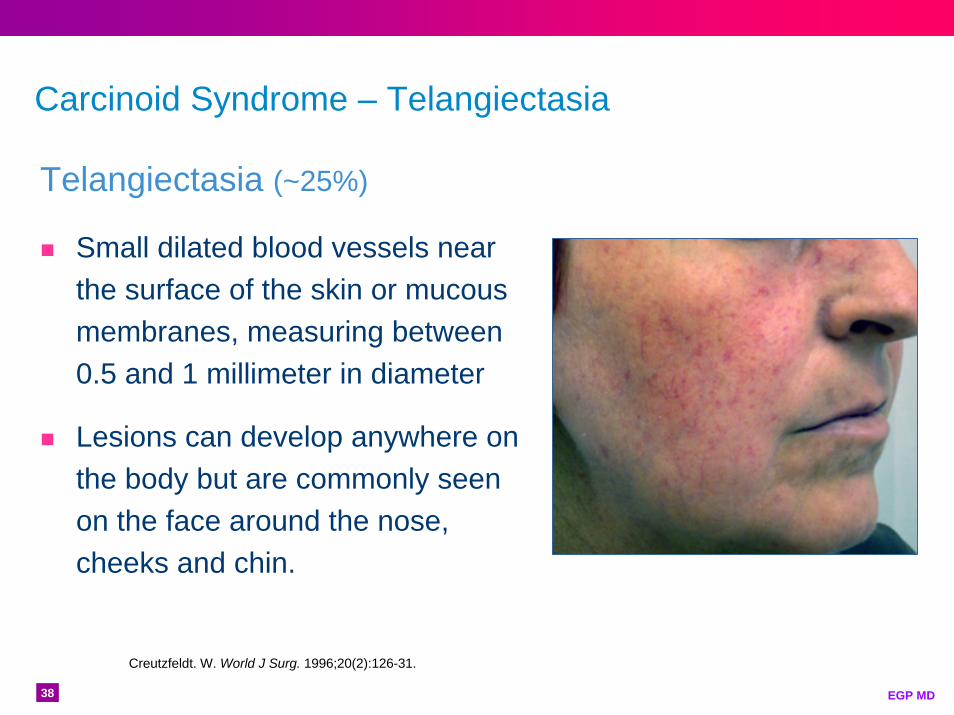
Carcinoid Syndrome – Telangiectasia
Telangiectasia (~25%)
Small dilated blood vessels near the surface of the skin or mucous membranes, measuring between 0.5 and 1 millimeter in diameter
Lesions can develop anywhere on the body but are commonly seen on the face around the nose, cheeks and chin.
Creutzfeldt. W. World J Surg. 1996;20(2):126-31.
39 EGP MDWikipedia.org
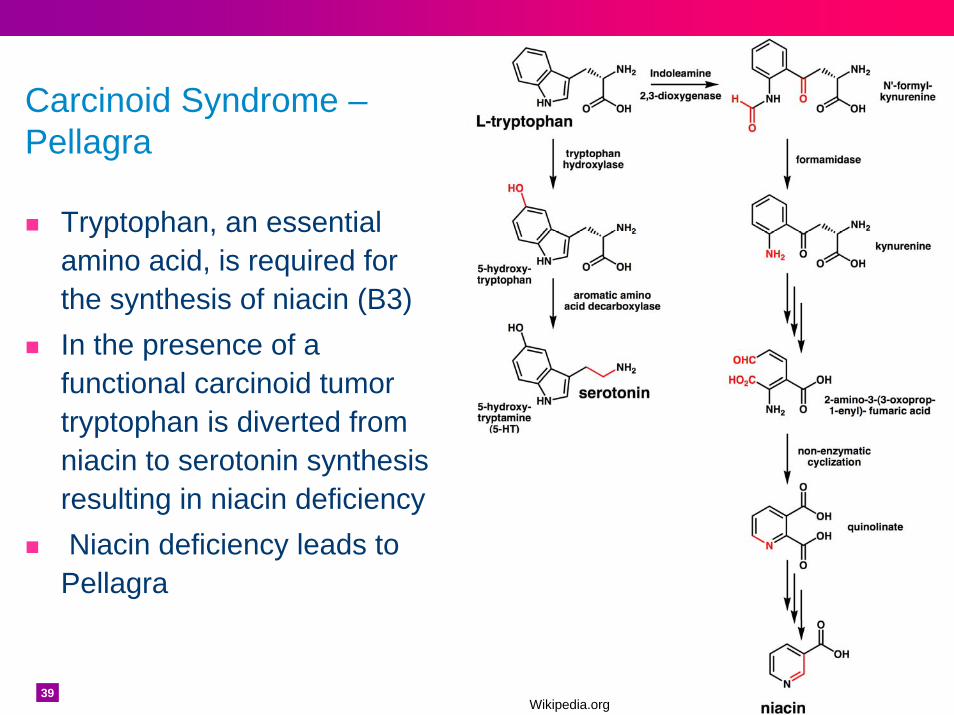
Tryptophan, an essential amino acid, is required for the synthesis of niacin (B3) In the presence of a functional carcinoid tumor tryptophan is diverted from niacin to serotonin synthesis resulting in niacin deficiencyNiacin deficiency leads to Pellagra
Carcinoid Syndrome –Pellagra
40 EGP MD
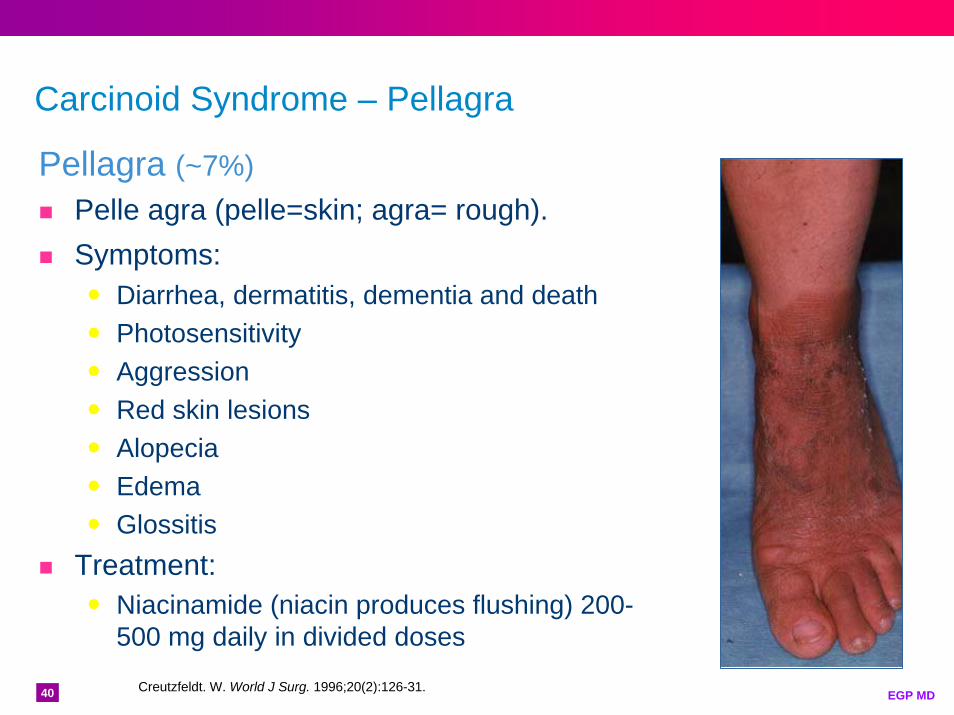
Carcinoid Syndrome – Pellagra
Pellagra (~7%)Pelle agra (pelle=skin; agra= rough).Symptoms:
Diarrhea, dermatitis, dementia and deathPhotosensitivityAggressionRed skin lesionsAlopeciaEdemaGlossitis
Treatment:Niacinamide (niacin produces flushing) 200-500 mg daily in divided doses
Creutzfeldt. W. World J Surg. 1996;20(2):126-31.
41 EGP MD
DyspneaPalpitationsLow blood pressureFatigue/AstheniaDizzinessMyopathyChanges in mental state
Other Signs/Symptoms of Carcinoid Tumors
Creutzfeldt. W. World J Surg. 1996;20(2):126-31.
42 EGP MD
Carcinoid CrisisImmediate onset of a debilitating and life-threatening condition associated with carcinoid syndrome
May occur spontaneously or may be precipitated by anesthesia, chemotherapy, infection, stress, catecholamines, tumor manipulation or embolization procedures
Symptoms include prolonged severe flushing, diarrhea, hypotension/hypertension, tachycardia, severe dyspnea, peripheral cyanosis and sometimes hemodynamic instability, hyperthermia and bronchospasm.
Most often seen with large tumor load, high levels of circulating serotonin, elevated CGA and 5-HIAA
Appropriate precautions include immediate therapy and close monitoring before, during and after surgical treatment.
Oberg K. Williams Textbook of Endocrinology; 10th Ed. Saunders; 2003;1857-1876.

43 EGP MD
Natural History of Carcinoid Tumors
0 2 4 6 8 10 12 14 16 18 20
Primary Tumor Growth
Metastases
Death
Vaguesymptoms
Diagnosis:Irritable Bowel
Menopause
NETDiagnosis
Years
Vinik A., Amer J Dig Dis. Sci., 1989;34:14-27
Flushing
Diarrhea

44 EGP MD
The problem, however, remains that diagnostic
investigation is usually initiated by
symptomatology, and in the vast majority of
patients, symptomatology is indicative of
metastasis.
Modlin IM, Kidd M, et al. Current status of gastrointestinal carcinoids. Gastroenterology 2005;128:1717-51.
45 EGP MD
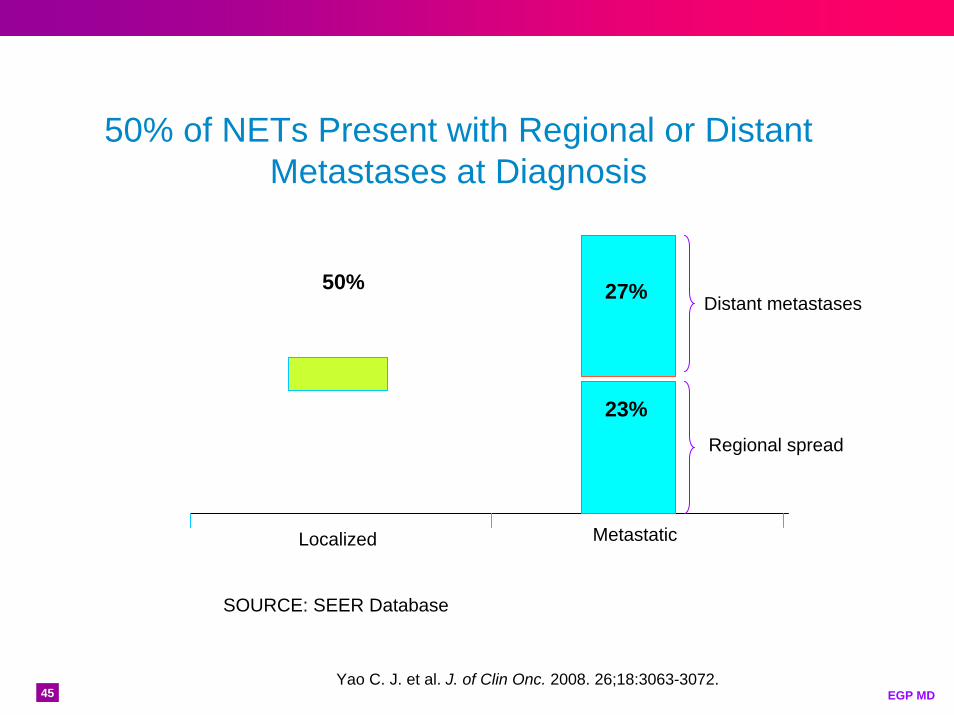
50% of NETs Present with Regional or Distant Metastases at Diagnosis
Yao C. J. et al. J. of Clin Onc. 2008. 26;18:3063-3072.
50% 27%
23%
Localized Metastatic
Distant metastases
Regional spread
SOURCE: SEER Database

46 EGP MD
Extent of Disease at Diagnosis by Site of Origin
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Rectum Lung Jejunum/Ileum
DistantRegionalLocalized
Ext
ent o
f Dis
ease
(%)
92%
8%
49%
51%71%
29%
Given the time it takes to make the diagnosis, the probability of metastatic disease, is dramatically increased
Median age at diagnosis for NETs: Rectum - 56 years, lung - 64 years and jejunum/ileum - 66 years
Yao C. J. et al. J. of Clin Onc. 2008. 26;18:3063-3072.
47 EGP MD
13335121516
343535
71
135
0
30
60
90
120
150
Liver
Mesente
ry
Retroperi
toneu
m
BonePer
itoneu
mOva
ryThor
ax
Supraclavic
ularSkin
Retro-orb
ital
Epicard
ialBrea
stBrai
n
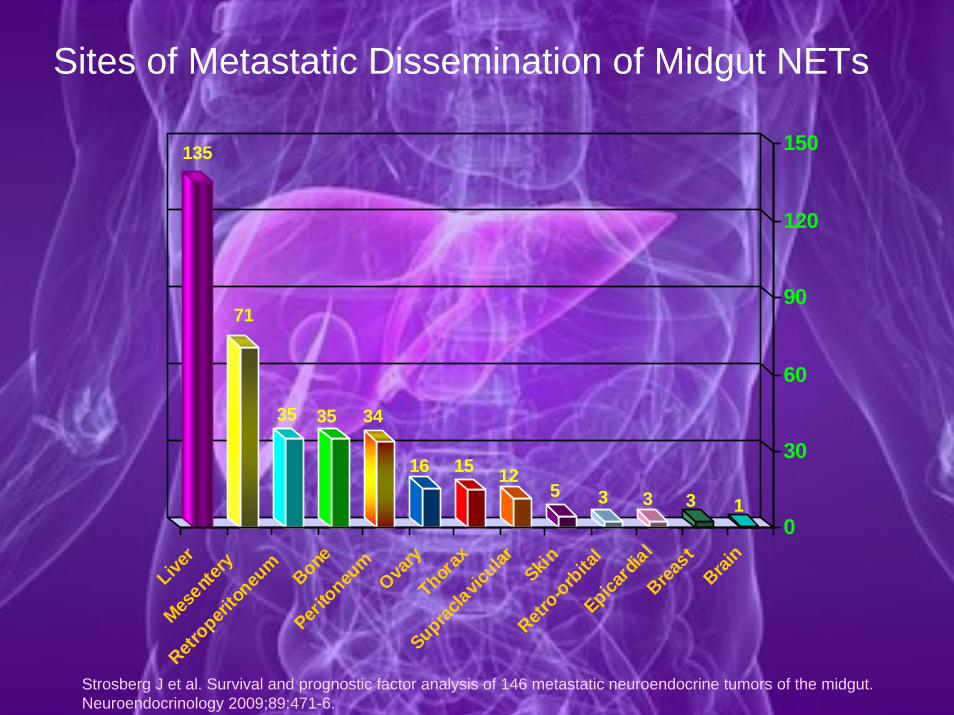
Sites of Metastatic Dissemination of Midgut NETs
Strosberg J et al. Survival and prognostic factor analysis of 146 metastatic neuroendocrine tumors of the midgut. Neuroendocrinology 2009;89:471-6.

48 EGP MD
49 EGP MD
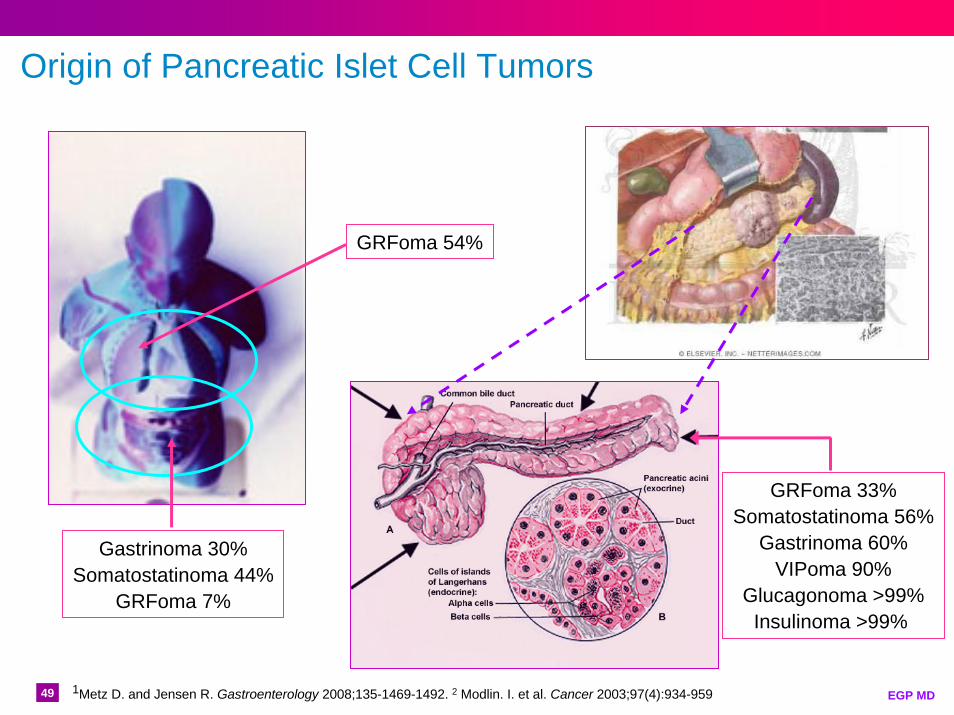
Origin of Pancreatic Islet Cell Tumors
GRFoma 54%
Gastrinoma 30%Somatostatinoma 44%
GRFoma 7%
GRFoma 33%Somatostatinoma 56%
Gastrinoma 60%VIPoma 90%
Glucagonoma >99%Insulinoma >99%
1Metz D. and Jensen R. Gastroenterology 2008;135-1469-1492. 2 Modlin. I. et al. Cancer 2003;97(4):934-959
50 EGP MD
Insulinomas – 17% of all PETs
Insulinoma Insulin
Hyperinsulinemia• Neuroglycopenia (90%)
• Amnesia or coma (47%)• Confusion (80%)• Visual changes (59%)• Convulsions (17%)• Altered consciousness (38%)
• Sympathetic overdrive (60-70%)• Weakness (56%)• Sweating (69%)• Tremors (24%)• Palpitations (12%)• Hyperphagia (14%)
• Obesity (<50%)Metz D. and Jensen R. Gastroenterology 2008;135-1469-1492
Whipple triad•Episodic (symptomatic) hypoglycemia
•CNS dysfunction temporally related to hypoglycemia (measured at the time the symptoms were present)
•Dramatic reversal of CNS abnormalities by glucose administration
51 EGP MD
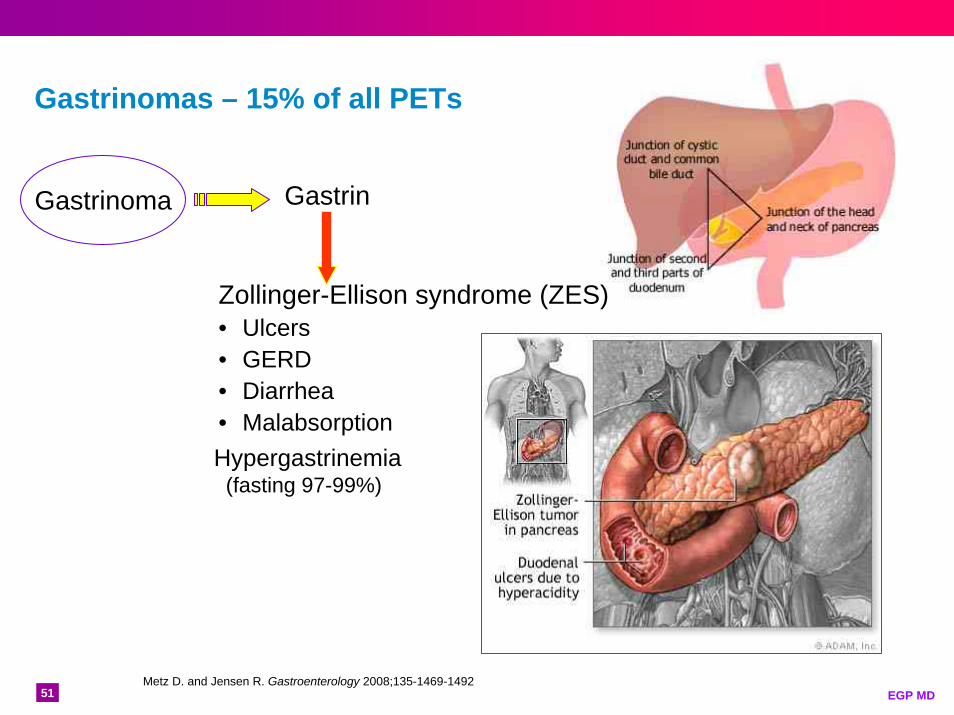
Gastrinomas – 15% of all PETs
Gastrinoma Gastrin
Zollinger-Ellison syndrome (ZES)• Ulcers• GERD• Diarrhea• MalabsorptionHypergastrinemia
(fasting 97-99%)
Metz D. and Jensen R. Gastroenterology 2008;135-1469-1492

52 EGP MD
VIPomas – 2% of all PETs
VIPomas VIP
Diarrhea• Electrolyte disturbances
• Hypokalemia (70-100%)• Dehydration (45-95%)• Hyperglycemia (20-50%)• Hypercalcemia (25-50%)• Hypochlorhydria (35-76%)• Flushing (15-30%)
Metz D. and Jensen R. Gastroenterology 2008;135-1469-1492

53 EGP MD
Glucagonoma – 1% of all PETs
Glucagon
Hyperglucagonemia• Glucose intolerance (DM)• Weight loss• Necrolytic migratory erythema
Metz D. and Jensen R. Gastroenterology 2008;135-1469-1492; Echenique-Elizondo. Pancreas 2004;5(4):179-185.
Glucagonoma
• Hypoaminoacidemia• Chelitis• Normocytic anemia• Vein thrombosis• Neuropsychiatric manifestations angularchelitis.net
Courtesy of Prof. Raimo Suhonen

54 EGP MD
Non-functional NETs – ~33%
Most secrete amines and peptides but do not result in an identifiable clinical syndromeLocal mass effects: obstruction and painRemoval of the primary tumor has been reported to prolong survival in all patients (median 1.2 vs. 8.4 years; p<0.001) and in those with metastases (1.0 vs. 4.8 years; p<0.001)
Franko J, Wentao F et al. J Gastrointest Surg; 2012; 14:541-548
Ashley S and Lauwers G. N Engl J Med 2002;347:1783-1791

55 EGP MD
56 EGP MD
Comprise ~20% of all lung cancersR. Laennec’s report (published posthumously in 1831) of an intrabronchial mass could be the first written description of a BP carcinoid
René-Théophile Hyacinthe Laënnec
Bronchopulmonary (BP) Neuroendocrine Tumors
Clinical presentationCoughHemoptysisObstructive pneumonia<5% Carcinoid syndrome
57 EGP MD
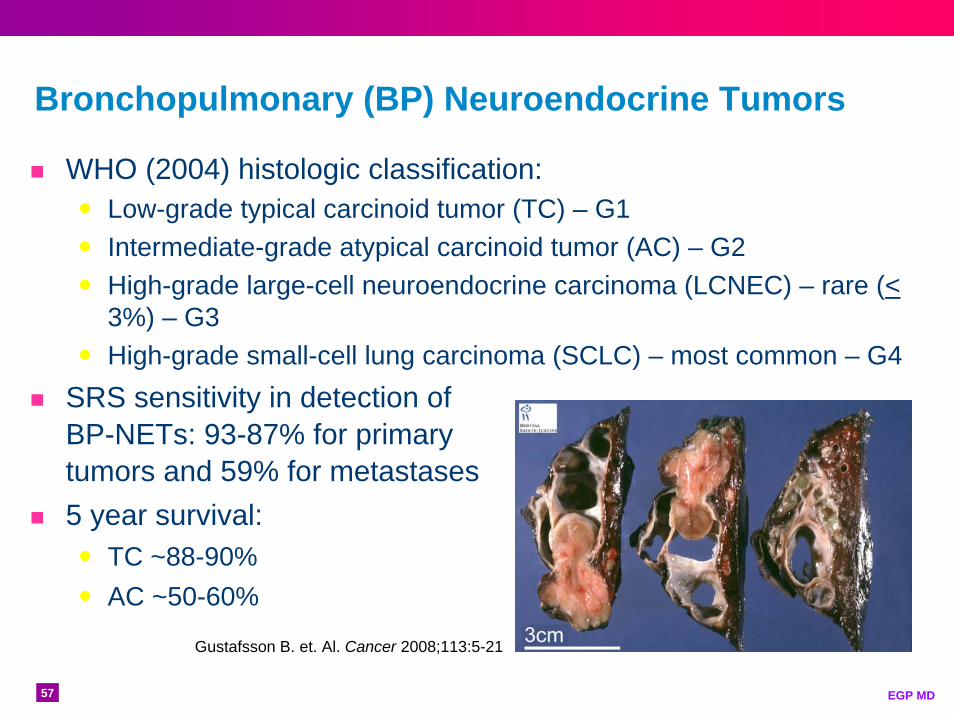
Bronchopulmonary (BP) Neuroendocrine Tumors
WHO (2004) histologic classification:Low-grade typical carcinoid tumor (TC) – G1Intermediate-grade atypical carcinoid tumor (AC) – G2High-grade large-cell neuroendocrine carcinoma (LCNEC) – rare (<3%) – G3High-grade small-cell lung carcinoma (SCLC) – most common – G4
SRS sensitivity in detection of BP-NETs: 93-87% for primary tumors and 59% for metastases
5 year survival:TC ~88-90%AC ~50-60%
Gustafsson B. et. Al. Cancer 2008;113:5-21

58 EGP MD