Embed Size (px)
Citation preview

Gastroenterology: top tips for on calls
Dr Laura Hopkins BM BSc MRCP
Gastroenterology SpR
Clinical teaching fellow
West Middlesex University Hospital

Discuss clinical scenarios within gastroenterology that you will be exposed to in FY1 doctor
acute presentations
procedures
Identify potential challenges in the clinical scenarios and formulate plans on how to manage them
Learning objectives

27 year old male
Know IBD (UC)
Current Rx: Asacol 2.4g OD
Presents with: bowels opening 8/day with blood, abdominal discomfort
Observations: BP 120/65, HR 102, Temp 36.7, sats 98%, RR 18
On examination: tender in LIF, no guarding, soft abdo
Clinical scenario 1

Question 1:
What next investigation would help assess the severity of this patients presentation?
a) Abdominal XR
b) Stool culture
c) CXR
d) Haemoglobin
e) Flexible sigmoidoscopy
Investigations

Mild Moderate Severe
Bloody stools/day <4 4 more if ≥6 AND 1 of
Pulse <90 ≤ 90 bpm > 90 bpm
temperature < 37.5 ≤ 37.8 > 37.8
Hb > 11.5 ≥10.5 g/dl < 10.5 g/dl
ESR/CRP ESR <20 ≤ 30 > 30
Truelove and Witt
ADMISSION

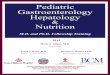
Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org, rID: 29399

Question 2: Which of the following meets the criteria for a diagnosis of toxic megacolon?
a) Transverse colon dilated to 6 cm
b) Small bowel dilated to 2.5 cm
c) Severe abdominal pain with guarding
d) Caecum dilated to 7 cm
e) Absence of bowel sounds
Abdominal XR

Question 3:
What treatment below should NOT be given to this patient?
a) Phosphate enema prior to flexible sigmoidoscopy
b) Prophylactic LMWH
c) IV hydrocortisone
d) IV fluids
e) Ensure (nutritional drinks)
Management

IV steroids (hydrocortisone 100mg QDS) Stool cultures X 3 (c.diff and bacterial)
VTE prophylaxis IV fluids +/- KCl
Unprepared flexible sigmoidoscopy + biopsy (CMV)
Ensure gastro team are aware of patient
Severe colitis: IP management

57 year old female
Known Alcoholic liver disease
Current Rx: spironolactone 100 mg OD, thiamine, vit B co-strong, omeprazole 40 mg
Presents with: jaundice, swollen abdomen
Observations: BP 100/50, HR 95, Temp 36.2, sats 95% OA, RR 20
Examination: yellow sclera, distended abdomen with shifting dullness, palmer erytherma, spider naevi
Clinical scenario 2

Question 4:
Which of the following information is needed to calculate the Child-Pugh score?
a) Presence of varices on OGD
b) UEs
c) Albumin
d) Cause of liver disease
e) ALT
Decompensated liver disease

Used to assess the severity of liver disease
Includes grade A-C (C=most severe)
C = only 45% chance of survival at one year
To calculate need: Alb/INR/bili
Ascites
Encephalopathy grade
Child-Pugh score

Infection
Chest/urine
SBP
GI bleed
Decompensated liver disease Jaundice, ascites, encephalopathy
Why have they decompensated?
Bloods Urine dipstick/culture Blood cultures Ascitic tap
Bloods: Hb, Plts, INR Reverse coagulopathy (vit K) PR examination Postural BPs Hx of Varices?

Question 5:
Which of the following confirms a diagnosis of spontaneous bacterial peritonitis?
a) Abdominal tenderness
b) PMN count > 250 cells/mm2
c) Positive ascitic culture
d) Lymphocytes > 300 cells/mm2
e) Serum ascites-albumin gradient (SAAG) > 11g/dl
Decompensated liver disease Jaundice, ascites, encephalopathy

Question 6: When performing an ascitic tap it is important to send the ascitic fluid for the following (can select multiple options and please rank in order of importance): a) WCC and gram stain b) Protein c) Ascitic culture d) Cytology e) CRP f) Amylase
Decompensated liver disease Jaundice, ascites, encephalopathy

Electrolyte/metabolic abnormality
Hepatocellular carcinoma
Alcohol consumption
Decompensated liver disease Jaundice, ascites, encephalopathy
UEs (Na/K) Bone profile BM
AFP Abdominal US
Signs of withdrawal (6-48hrs) Recent consumption

Detox regime Chlordiazepoxide (CIWA) PRN/regular
Nutrition Ensures/NG feeding
Pabrinex (48 hours) (I+II pairs TDS)
Bowels Lactulose (aim for bowels opening 2-3/day)
Review nephrotoxics (spironolactone)
Other management

80 year old male
Presents with black stool for 24 hours, dizzyness
PMHx: AF, IHD, Diabetes, HTN, high cholesterol, Right THR, OA
Medications: warfarin, ramipril, amlodipine, bisoprolol, simvastatin, novomix 30 BD, PRN paracetamol
Observations: BP 82/60, HR 120, Temp 36, RR 28, sats 95%OA
Examination: pale, mild epigastric tenderness, meleana on PR
Clinical scenario 3

Question 7:
What is the next most important step in his management?
a) OGD
b) Giving vitamin k
c) Speaking to haematology
d) Organising a blood transfusion
e) Abdominal XR
Clinical scenario 3

Bloods:
FBC (Hb 7.5, plts 122)
UEs (urea 15, creat 80)
INR (6.2)
Resuscitation (stage 3 shock: 1.5L)
Fluids
blood
Upper GI bleed

Question 8:
What is the best antidote we can give to reverse the effects warfarin when someone is actively bleeding?
a) Vitamin K
b) FFP
c) Stop warfarin
d) Unit of RBC
e) Prothrombin complex concentrate (PCC)
Upper GI bleed

Bloods:
FBC (Hb 7.5, plts 122)
UEs (urea 15, creat 80)
INR (6.2)
Resuscitation
Fluids (crystalloid)
Blood (XM BUT consider O neg)
Blood products (PCC- beriplex/octaplex) Important to involve haematology team
Upper GI bleed

Whilst on ward cover you are bleeped to see the 57F with decompensated ALD because she has become drowsy:
What do you want to know?
On arrival to ward what will you do?
Clinical case 2 cont…

Question 9:
The nurse on the phone is able to tell you she open her eyes when they tried to check a BM but that she seemed confused as she thought she was at the dentist. When they took the BM she withdrew her arm away.
What is her GCS?
a) 6
b) 10
c) 8
d) 15
e) 3
Clinical case 2 cont…

What is there GCS? This patient was 10 (E2, V4, M4)
< 8 may not be able to maintain airway AVPU
Encephalopathic
Bowels Nutrition
Intracrebral event
Any hx of fall Clotting and plts CT head
Blood sugar
Drowsiness in liver patient

Question 10:
A patient under your care requires an ERCP. They presented with cholangitis and a scan showed they have a gallstone stuck in their CBD. Which of the following do you need to do:
a) Let the patient know they are having the procedure
b) Put a form into endoscopy for them to organise it
c) Speak to the gastro consultant doing the procedure
d) Review the drug chart for any anti-coagulants
e) All of the above
Procedures

ERCP
Review drug chart (antiplt/heparin): 7 days off clopidogrel Hold heparin night before (if prophylactic)
OGD
Fasted for at least 6 hours Am list: from midnight Pm list: from 6 am
Colonoscopy
Try to avoid as IP procedure requires bowel preparation Have to be mobile!
Applicable to all IV access for sedation and analgesics Are they a diabetic? do they need a form 4 completing
Procedures

Any questions?

Discuss clinical scenarios within gastroenterology that you will be exposed to in FY1 doctor
acute presentations
procedures
Identify potential challenges in the clinical scenarios and formulate plans on how to manage them
Learning objectives