Embed Size (px)
Citation preview
Gastro-intesinal assessment
DR---NOHA ELSAYED 2015---2016
Gastro-intesinal assessment
Inspection(DCAP-BTLS)
Auscultation(not included)
Palpation
Percussion
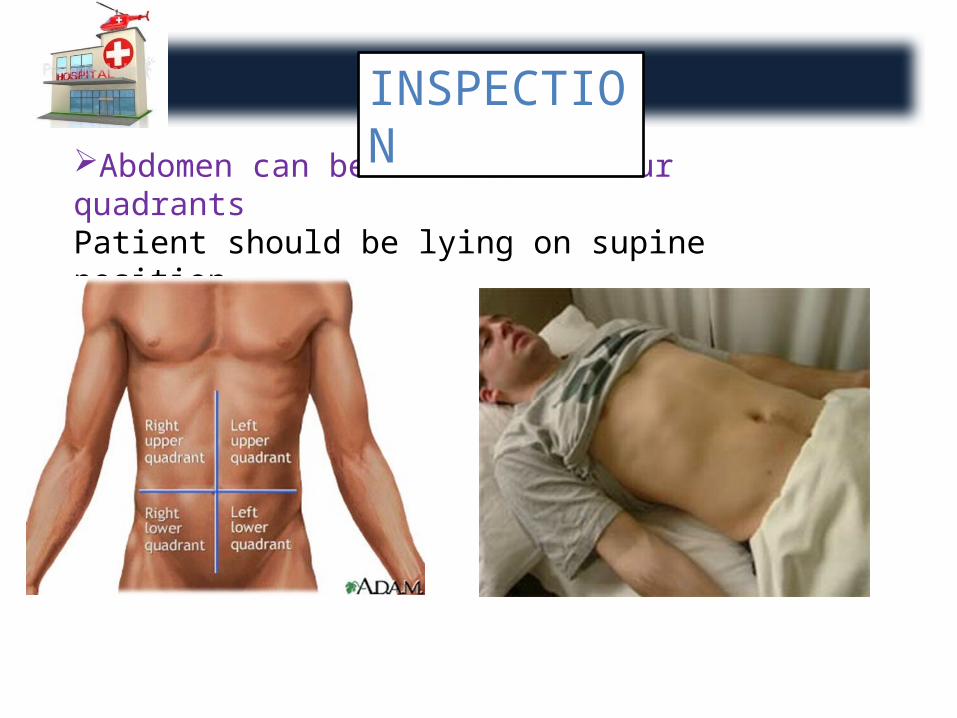
Abdomen can be divided in four quadrantsPatient should be lying on supine position
INSPECTION
Inspect oral mucosa For example:1. Lips & mucous membranes should be moist & without lesions
(If dry …. Indicates dehydration)2. Large abdomen …. Indicates Ascitis (Abdominal veins may be
seen)3. Bruising …. Indicates trauma or bleeding in the abdominal
cavity4. Abdominal girth …. Used to document enlarging of organs or
swelling from internal bleeding5. Stools should be assessed for color, consistency & a foul odour
Dark melena stools(Upper GIT bleeding)
Bright red blood(Lower GIT bleeding)
Deformities & Discolorations D
Contusions C
Abrasions A
Penetrations & Punctures P
Burns B
Tenderness T
Lacerations L
Swelling & Symmetry S
DCAP-BTLS
+Visible peristalsis
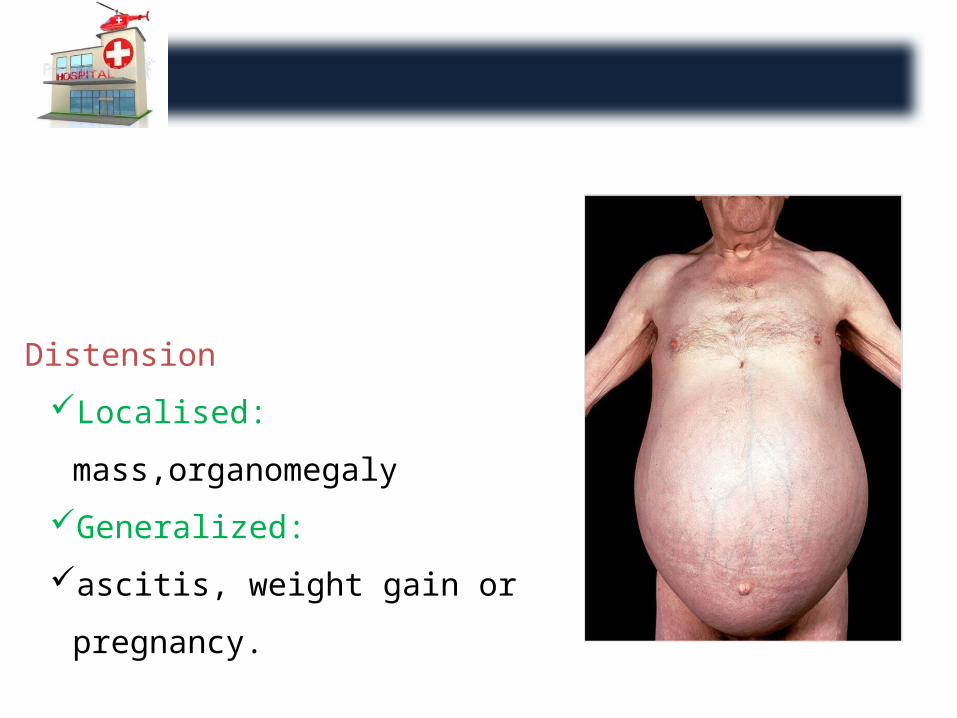
Distension
Localised: mass,organomegaly
Generalized:
ascitis, weight gain or pregnancy.
Palpate the abdomen
Begin farthest away from the pain.
First superficial (for tenderness or rebound tenderness) rebound
tenderness means pain as pressure of palpation removed ……..suggest
peritoneal inflammation and then
deep palpation(for organs)
liver(palpate for nodules=malignancy)
Spleen not palpable
Kidney also not palpable only if there is a history of polycystic kidney
Assess for discomfort, rigidity, and masses.
If a pelvic fracture is suspected .the pelvis should not be assessed for
stability ………….that any hematoma that has formed to maintain
homeostasis may be disrupted causing internal hemorrhage.
Murphy’s sign severe right upper quadrant pain on deep palpation
exacerbated by deep inspiration this is associated with cholecysitis
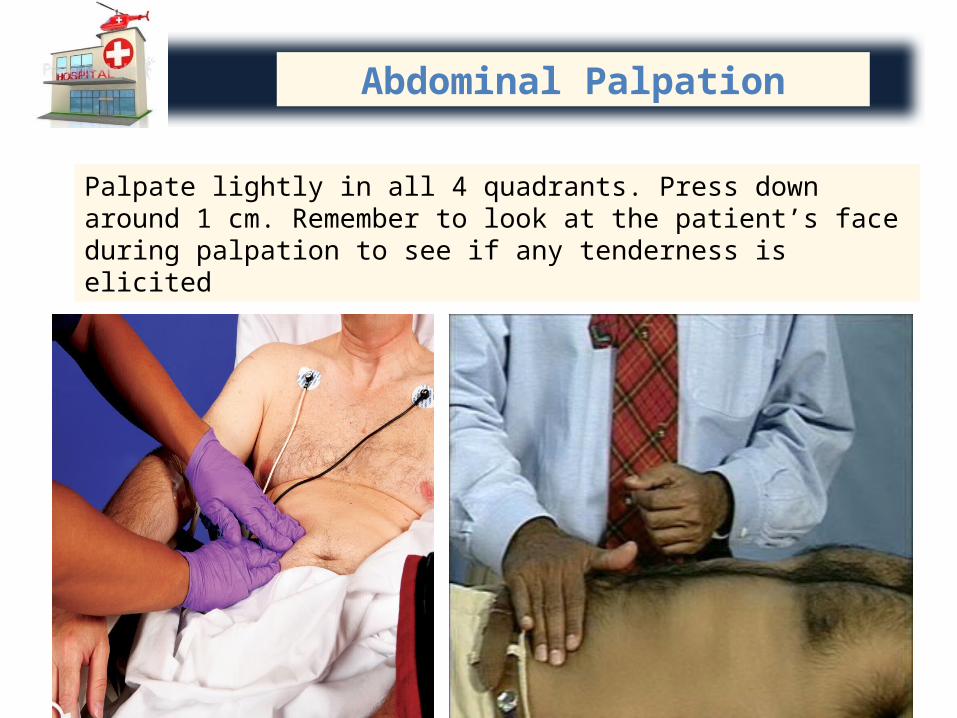
Abdominal Palpation
Palpate lightly in all 4 quadrants. Press down around 1 cm. Remember to look at the patient’s face during palpation to see if any tenderness is elicited
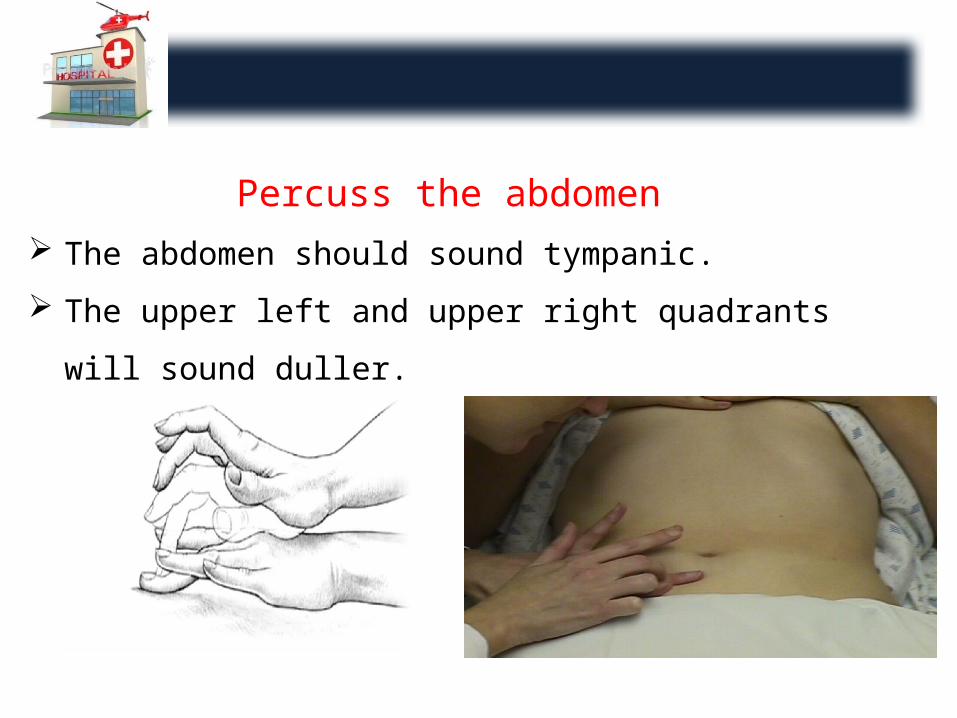
Percuss the abdomen The abdomen should sound tympanic.
The upper left and upper right quadrants will sound duller.
Genito-urinal assessment:
Assessment of genitalia includes: Mammary, Testicular, Prostate glands
Limited to patients with specific needs, such as: Those with spinal cord injuries or trauma
Proper kidney function is vital because kidney excretes the majority of toxins from human body
The best indicator for kidney function …. Serum Creatinine (Normal: 0.6 – 1.2 mg/dl)
The more nephrons that have been destroyed, the higher the creatinine level
Take care: Blood urea nitrogen (BUN) is more indicator for hydration than
for renal function (Normal: 8 – 23 mg/dl) BUN/Creatinine ratio is the best method to determine whether
the patient has any type of renal failure (Normal: 10:1 to 20:1)
75% of nephrons can be destroyed before signs & symptoms of renal failure occur
Renal failure (RF) leads to
Monitored by: Arterial blood gases, Urine output Causes of RF: Burn, Crush, Injuries Release of large protein molecules from damaged tissue
destroys the nephrons End stage renal disease …. Requires Peritoneal dialysis (PD) or
Hemodialysis (HD)
•Metabolic acidosis•Congestive heart failure
•Electrolytes imbalance•Anemia
Peritoneal dialysis (PD) Hemodialysis (HD)
Catheter is placed in the peritoneum that serves as the filter to remove wastes from the peritoneal cavity using dialyzing solution
Will have arterio-venous (AV)shunt placed in the arm that is attached to machine acts as a mechanical kidney to remove wastes from the body.
This AV site should be assessed for a thrill (Palpate) & a bruit (Audible) which indicates patent & normally functioning shunt …. Absence of one or both of those indicates clotting of the shunt
• CCTP main concern is maintaining stability of joints by splints or soft and hard casts and assessing for neurovascular compromise of distal extremities.
• Assessment should be completed bilaterally and also assessment of distal skin color ,nail bed colour ,skin temperature ,mobility of distal joints ,pulses and pain sensation
Muscloskeletal assessment
Psychological & Emotional assessment
If a patient is hospitalized for more than 24 hours …. Complete psychological, emotional assessment should be transferred with the patient as it may be helpful to the staff at the receiving facility.
Previously diagnosed psychiatric disorders & Level of anxiety the patient is experiencing must be known.
Psychiatric disorders may be unsafe requiring physical & chemical restraint during transportation or administration of anxiolytics or benzodiazepines
Communication should be with the transferring hospital which is responsible for care of the patients until the arrival .
Changes, Orders & Response of patient should be called immediately to the staff at receiving hospital … To become aware of events occurring enroute so they are prepared to receive the patient.
Communication, Documentation
Documentation of assessment findings to provide continuity of care & patient safety & to protect themselves in case of legal issues.