Embed Size (px)
DESCRIPTION
The mechanism of Gastric secretion in human GIT
Citation preview

GASTRIC ACID, CALCIUM ABSORPTION, ANDTHEIR IMPACT ON BONE HEALTHSascha Kopic and John P. Geibel
Departments of Surgery and Cellular and Molecular Physiology, Yale School of Medicine,New Haven, Connecticut
LKopic S, Geibel JP. Gastric Acid, Calcium Absorption, and Their Impact on BoneHealth. Physiol Rev 93:189–268, 2013; doi:10.1152/physrev.00015.2012.—Cal-cium balance is essential for a multitude of physiological processes, ranging from cellsignaling to maintenance of bone health. Adequate intestinal absorption of calcium is amajor factor for maintaining systemic calcium homeostasis. Recent observations indi-
cate that a reduction of gastric acidity may impair effective calcium uptake through the intestine.This article reviews the physiology of gastric acid secretion, intestinal calcium absorption, and theirrespective neuroendocrine regulation and explores the physiological basis of a potential link be-tween these individual systems.
I. INTRODUCTION 189II. GASTRIC ACID SECRETION 189III. INTESTINAL CALCIUM ABSORPTION 203IV. REGULATION OF CALCIUM HOMEOSTASIS 212V. THE STOMACH AND CALCIUM 231VI. CONCLUSIONS 238
I. INTRODUCTION
The average adult human body contains �1.6% calcium,which relates to �1,120 g in a 70-kg individual (743). Ninety-nine percent of the calcium is stored in bone and teeth andis therefore inaccessible to most physiological processes(743). Although the amount of the immediately accessible11 g (1%) of calcium may seem miniscule, this fractionrepresents a pivotal constituent of our body. It serves abroad diversity of roles, which range from intracellular sig-naling and maintenance of membrane integrity to musclecontraction and neuronal transmission.
To allow for these calcium-dependent processes to func-tion, our body undertakes extensive measures to keep theintracellular and extracellular calcium concentrations andthe gradient between these two compartments stable. Theextracellular calcium concentration is typically clamped at�1.1 mM, whereas the intracellular environment is kept ata 10,000 times lower concentration. In consequence, rela-tively small disturbances in calcium homeostasis can lead tosevere symptoms, such as cardiac arrhythmias or cognitivedysfunctions. To maintain eucalcemia, our body is there-fore tightly regulating the balance between calcium absorp-tion by the intestine and calcium excretion by the kidney. Inaddition, calcium is deposited in or extracted from bone,which serves as a dynamic calcium reservoir. These threeorgan systems, i.e., the intestine, the kidney, and bone, areprecisely controlled by a complex endocrine network,
which primarily consists of the calcitropic hormones: 1,25-dihydroxyvitamin D [1,25(OH)2-vitamin D], parathyroidhormone (PTH), and calcitonin.
This review mainly focuses on the question as to how calciumenters the body through the intestine and how this mechanismis regulated via the endocrine system. Furthermore, the processof gastric acid secretion as related to calcium homeostasis willbe reviewed in detail. This may seem surprising, as gastric acidsecretion and intestinal calcium absorption are two distinctphysiological processes, which on first examination may notseem to be interdependent. However, recent clinical studiessuggest that there may be a relationship between reduced gas-tric acid secretion and increased risk for sustaining bone frac-tures, which asks the question whether we need gastric acid toabsorb calcium efficiently through the intestine, or whether thestomach exerts endocrine functions that impact bone health.Indeed, it has been put forward several decades ago that gas-tric acid solubilizes calcium that is then complexed with otherdietary constituents, thereby allowing for a more efficient ab-sorption in the intestine (18, 520, 699, 797). Furthermore, it islong known that a partial or complete resection of the stomachresults in decreased bone density, also leading to fractures (58,305, 732, 876). The stomach, the intestine, and bone are there-fore functionally more intertwined than one may initially as-sume. This review will independently analyze the processes ofgastric acid secretion, intestinal calcium absorption, and theirrespective neuroendocrine control and will conclude with acritical attempt at illustrating where these two seemingly inde-pendent organ systems intersect in terms of calcium homeo-stasis and bone health.
II. GASTRIC ACID SECRETION
The stomach is a unique organ that fulfills multiple roles.The main function of the gastric mucosa is to secrete con-
Physiol Rev 93: 189–268, 2013doi:10.1152/physrev.00015.2012
1890031-9333/13 Copyright © 2013 the American Physiological Society
on Decem
ber 8, 2014D
ownloaded from

centrated hydrochloric acid, which provides a chemical bar-rier against ingested pathogens and aids in the digestion offoodstuffs. To achieve these functions, the gastric glandcontains specialized cells that pump protons into the gastriclumen in an effort to acidify the contents of the stomach.These cells are known as parietal cells, or oxyntic cells.Since concentrated acid is a noxious substance, the gastricmucosa has to undertake extensive measures to protect it-self from tissue injury. The protection is accomplished bysecreting mucus from mucus neck cells, but also by tightlyregulating the secretion of acid (see sect. IIB). A variety ofspecialized endocrine cells in the gastric mucosa are in-volved in the regulation of gastric acid secretion. A pertur-bation of either protective mechanism can lead to severetissue damage, resulting in gastric ulcers. This section dis-cusses the process of how gastric acid is secreted by review-ing the molecular mechanism underlying acid secretion inthe parietal cell and its neuroendocrine regulation.
A. Apical Ion Transport in the Parietal Cell
The gastric parietal cell is responsible for acidifying thestomach by secreting concentrated acid. Gastric acid secre-
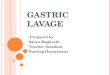
tion depends on the apical extrusion of three ions. Protonsare pumped into the gastric lumen by a proton pump, thegastric H�-K�-ATPase, to acidify the gastric content to apH of as low as 1. Chloride is secreted via apical chloridechannels to ensure formation of HCl and to provide thecounter-ion conductance to protons. Lastly, potassiumleaves the parietal cell apically in a recycling mechanism,thereby fueling reciprocal proton transport by the H�-K�-ATPase (FIGURE 1). It has been demonstrated in numerousinvestigations that disruption of one of these ion transportmechanism renders the parietal cell incapable of secretinggastric acid (705, 820, 1013, 1029).
1. H�-K�-ATPase
A) STRUCTURE. The gastric H�-K�-ATPase belongs to thefamily of P2-type ATPases, which also includes the ubiqui-tous Na�-K�-ATPase and the sarcoplasmic reticulumCa2�-ATPase (SERCA). As the name implies, it exchangesone intracellular hydrogen ion for one extracellular potas-sium ion at the expense of ATP. ATP is provided to thepump by a large network of mitochondria, which occupyup to 40% of the cell volume, making the parietal cell one ofthe most mitochondria-rich cells in the body (292). In the
K+
PPIsAPAs
Parietal cell
KCNQ1Kir
CFTRCIC-2?SLC26A9
SST
BasolateralApical
Hist
SSTR
K+
H+
Ca2+
cAMP
Cl–
Gast
ACh
CCK2
M3
H2
FIGURE 1. Parietal cell model. The gastric parietal cell is equipped with apical ion transport mechanisms thatallow for the secretion of concentrated hydrochloric acid. Activation of basolateral secretagogue receptorsmainly leads to an increase in either cAMP (histamine) or calcium (acetylcholine, gastrin), causing apicalinsertion and activation of the H�-K�-ATPase. Somatostatin reduces intracellular cAMP levels. ACh, acetyl-choline; APAs, acid pump antagonists; Gast, gastrin; Hist, histamine; PPIs, proton pump inhibitors; SST,somatostatin.
SASCHA KOPIC AND JOHN P. GEIBEL
190 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

process of proton extrusion, the H�-K�-ATPase can over-come a massive acid gradient of 6 pH units, which is nec-essary to achieve sufficient gastric acidification. The pumpitself is a heterodimer, consisting of a � subunit and a �subunit, while the individual pumps assemble as (��)4 te-tramers on the parietal cell surface (1). The � subunit con-sists of 10 transmembrane domains and contains the cata-lytic site, which mediates ion exchange. The � subunit sta-bilizes the � subunit and is heavily glycosylated (41, 1105).Mutational analysis of the glycosylated asparagine residuessuggests that these sites are critical for adequate membranedelivery of the entire pump (41, 1105). Furthermore, the �subunit prevents a reversal of ion transport by a “ratchet”-like mechanism, which allows H�-K�-ATPase to pumpagainst the imposed high proton gradient (4, 294). Bothsubunits share a significant degree of homology to Na�-K�-ATPase (697, 1012). This close relationship to other P2-type ATPase has historically been exploited for homologymodeling of H�-K�-ATPase based on the crystal structureof SERCA, which had been acquired in several conforma-tional states (762, 815, 1092, 1093). Recently, however,direct structural information on H�-K�-ATPase has beenobtained by electron crystallography, also in the presence ofthe acid pump antagonist SCH28080 (2–4).
B) TRAFFICKING. In the resting parietal cell, H�-K�-ATPase isstored in tubulovesicles throughout the cell (292). Follow-ing neuronal or hormonal stimulation (see sect. IIB), thesevesicles are postulated to fuse with the apical pole, which ischaracterized by multiple microvilli-lined membrane in-vaginations, the so-called secretory canaliculi (292). Thisdistinct apical morphology of the parietal cells maximizescell surface and thereby allows for insertion of a high num-ber of proton pumps per cell following stimulation. Thechanges in membrane morphology and insertion of H�-K�-ATPase are extremely dynamic to ensure fine regulation ofgastric acid secretion (973). H�-K�-ATPase containingtubulovesicle fusion relies on SNARE complex forma-tion. In particular, the SNARE proteins syntaxin 3/7/12/13, VAMP2/8, and SNAP-25 were implicated to be candi-dates mediating this process (548–550, 624). The func-tional significance of these proteins was, for example,demonstrated in primary rabbit parietal cell cultures ex-pressing a SNAP-25 mutation, which was shown to reducetheir capacity to secrete gastric acid (548).
Apart from SNARE proteins, the small GTPases of the rabfamily (rab2/11a/25/27b) are involved in the regulation ofH�-K�-ATPase vesicle trafficking (147, 293, 386, 387,1049, 1070). Functional data especially substantiate theimportance of rab11a and rab27b. In parallel to SNAP-25defective cells, parietal cells transfected with a rab11a andrab27b mutant secrete acid less effectively (293, 1049).
After stimulation, in the off-phase of gastric acid secretion,H�-K�-ATPase has to be retrieved from the plasma mem-
brane for recycling (336). It is plausible that the initial stepof this process relies on the formation of clathrin-coated pitsand subsequent vesicle budding. Indeed, clathrin was iden-tified fairly early on H�-K�-ATPase containing tubulo-vesicles, although a functional role was not demonstrated(813). One of the multiple clathrin binding proteins is Hun-tingtin interacting protein 1 related (Hip1r) which aids invesicle formation and membrane trafficking (309). It isstrongly expressed in parietal cells, especially in the vicinityof secretory canaliculi (522). Functionally, Hip1r-deficientanimals present with a decreased number of parietal cells,loss of tubulovesicles, and decreased acid output (522,561).
2. Chloride secretion
Apical chloride secretion provides the second componentfor the formation of concentrated HCl and maintains over-all electroneutrality during acid secretion. The importanceof chloride efflux for the process of gastric acid secretionhas been established in the 1980s. Patch-clamp measure-ments demonstrated the presence of chloride conductanceon the apical pole of the parietal cell in Necturus, the humanparietal cell line HGT-1, and rabbit parietal cells (259, 935,940). All reports demonstrated a sensitivity of the chloridecurrent to cAMP or histamine, which is a common secondmessenger promoting acid secretion or a direct acid secre-tagogue, respectively (259, 935, 940). Simple flux measure-ments in isolated parietal cell vesicles had indicated thepresence of a chloride conductance pathway even earlier(232, 895, 1169). In these early experiments, inhibition ofchloride flux with chloride channel blockers also abolishedproton transport which underlines the necessity of intactchloride secretion for acid secretion to take place (232, 895,1169). However, the molecular identity of the chloridepathway remained elusive. Today, at least three candidateshave been put forward as potential mediators of apical chlo-ride secretion in the parietal cell: the cystic fibrosis conduc-tance regulator (CFTR), chloride channel protein 2 (ClC-2),and solute carrier 26 A 9 (SLC26A9) (FIGURE 1).
A) CFTR. CFTR represents a common apical chloride conduc-tance pathway in a broad variety of epithelia, such as theairways, intestine, and pancreas. Its mutation is responsiblefor the most widespread inherited disease, namely, cysticfibrosis (CF), which results in increased mortality due tosecretory defects and concomitant infections. The presenceof CFTR has been confirmed in gastric mucosa by in situhybridization, albeit at low quantities (1044). Nevertheless,functional measurements in isolated gastric glands demon-strated a decreased acid secretory capacity in animals car-rying the most common mutation responsible for CF(�F508) (1013). Furthermore, acid secretion was reducedin wild-type animals when a specific CFTR inhibitor wasapplied (1013). Although these observations may suggest adirect involvement of CFTR in the process of chloride se-cretion, it is plausible that CFTR rather has a regulatory
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
191Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

effect on H�-K�-ATPase (1013). In other tissues, CFTRcan interact with a variety of ion transport proteins, such asNHE, forming regulatory complexes, making an interac-tion with H�-K�-ATPase plausible (1013).
B) CLC-2. ClC-2 has been proposed as an alternative chloridesecretion pathway to CFTR in other epithelia, such as thelung and intestine (207, 404, 675, 766). ClC-2 has beencloned from rabbit gastric mucosa, which led to the hypoth-esis that the channel may also be involved in acid secretion(706). However, follow-up investigations revealed that therole of ClC-2 is much less clear. The studies revealed con-troversial results regarding the channel’s expression in thegastric mucosa (488, 706, 1001). While the initial observa-tions reported mRNA and cDNA expression in rabbit gas-tric mucosa, no protein could be detected in human and ratgastric glands (488, 706, 1001). The importance of ClC-2 inthe stomach has further been severely challenged by thecreation of a ClC-2 (�/�) animal model. Although ClC-2-deficient animals present with a distinct phenotype charac-terized by testicular and retinal abnormalities, no defect inacid secretion was observed (118).
C) SLC26A9. Lastly, evidence suggests that chloride may leavethe apical pole via SLC26A9, a chloride-bicarbonate anti-porter. Both SLC26A9 and an antiporter from the sameanion exchanger family (SLC26A6) have been detected inthe tubulovesicles of parietal cells (845, 1179, 1180). Con-cerning the functional involvement, the authors speculateabout two potential roles SLC26A9 may play in parietal cellphysiology. Being a chloride-bicarbonate exchanger, its ac-tivation would entail alkalinization of the gastric lumenby bicarbonate efflux and simultaneous chloride uptake(1180). Since this would neutralize H�-K�-ATPase-mediated proton extrusion, it has been suggested thatSLC26A9 activates in the off-phase of acid secretion toneutralize tubulovesicular pH during vesicle retrieval(1180). Alternatively, SLC26A9 may function as a chloridesecretion pathway that contributes to acid secretion. Thishypothesis is based on the observation that SLC26A9 canalso exhibit the behavior of a bona fide chloride channel,rather than an anion antiporter (88, 281). Undoubtedly,further functional investigations are needed to delineate itsexact role in the parietal cell. Its genetic disruption, how-ever, leads to a severely altered parietal cell morphologythat is characterized by dilation of gastric glands, loss oftubulovesicles, and decreased acid output (1180). Althoughthese results do not answer whether SLC26A9 serves as anapical chloride efflux pathway, they indicate that it may benecessary for normal parietal cell function.
3. Potassium recycling
Even before the identification of H�-K�-ATPase, it hasbeen observed that potassium is necessary for acid secretionto take place (335). To prevent the luminal depletion ofpotassium, which would impair proton pumping by H�-
K�-ATPase, potassium has to leak through potassiumchannels or transporters into the gland lumen to ensureadequate supply to H�-K�-ATPase (FIGURE 1). This pro-cess is referred to as potassium recycling. Early flux mea-surements in isolated H�-K�-ATPase containing parietalcell vesicles had already indicated the presence of a largepotassium conductance during H�-K�-ATPase activity(1169). The exact molecular identity of the potassium effluxpathway is, however, under debate. The list of candidatesthat have been put forward to be responsible for potassiumrecycling during acid secretion is long and includes KCNQ1(Kv7.1), KCNJ10 (Kir4.1), KCNJ15 (Kir4.2), KCNJ2(Kir2.1.), and KCC4.
A) KCNQ1. KCNQ1 is a typical “shaker”-like six transmem-brane spanning domain voltage-gated potassium channel(1144). It was initially identified in the heart, where itsmutation can be responsible for cardiac arrhythmias(1144). Yet, studies in KCNQ1 (�/�) animals revealed noelectrocardiographical abnormalities (641). Rather thansuffering from cardiac abnormalities, these animals surpris-ingly exhibited a distinct gastric phenotype with gastric hy-perplasia, dilated gastric glands, vacuolated parietal cells,hypochlorhydria, and hypergastrinemia (641). This obser-vation led to the speculation that KCNQ1 may be the chan-nel responsible for potassium recycling. Subsequently, im-munohistochemical studies confirmed a colocalization ofthe channel with H�-K�-ATPase, and acid secretion wasshown to be inhibited by pharmacological blockade (253,391). Direct measurement of acid secretion in KCNQ1(�/�) mice with modified Ussing chambers (pH stat) laterconfirmed the initially observed hypochlorhydria (1029).Interestingly, luminal substitution of potassium could res-cue the acid secretory deficit, indicating that hypochlorhy-dria ensued from a true lack of apical potassium secretionrather than a general morphological defect of the KCNQ1(�/�) parietal cell (1029).
KCNQ1 is a peculiar channel in that it has a low conduc-tance in acidic environments. In the context of the extremeacidic milieu surrounding the parietal cell, this would im-pede its function as a potassium recycling pathway. Tocircumvent this limitation, KCNQ1 attaches to a regulatorysubunit (KCNE2), which modulates the channel’s gatingproperties and current amplitude (253, 391, 1087). Coas-sembly with KCNE2 activates KCNQ1 at acidic pH valuesand thus facilitates the process of potassium secretion intothe gland lumen (391, 436). The importance of KCNE2 forproper channel function is underlined by the observationthat KNCE2 (�/�) animals display a phenotype similar toKCNQ1 (�/�) mice, i.e., hypochlorhydria, altered parietalcell morphology, and hypergastrinemia (917).
B) KIR CHANNELS. Apart from KCNQ1, several members ofthe inward-rectifier potassium channel (Kir) family havebeen proposed to be involved in gastric acid secretion, albeit
SASCHA KOPIC AND JOHN P. GEIBEL
192 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

the amount of functional evidence supporting a role of thesechannels is smaller and the field is divided about the relativecontribution of each channel. Kir 2.1, 4.1, 4.2, and 7.1 wereall confirmed on an mRNA level in gastric mucosa (353,431, 707). On a protein level, immunohistochemistry dem-onstrated colocalization of Kir 2.1, 4.1, and 4.2 with H�-K�-ATPase (353, 431, 556, 707). Cell fractionation exper-iments further indicated trafficking of Kir 4.1 and 4.2 to thecell surface, following parietal cell stimulation (431, 556).A most recent observation monitored acid secretion in Kir
4.1 (�/�) mice (1028). Surprisingly, loss of Kir 4.1 results inaugmented rather than impaired acid secretion, accompa-nied by upregulated H�-K�-ATPase expression (1028).This makes a contribution of Kir 4.1 to potassium recyclinghighly unlikely. Instead, it has been proposed that the chan-nel may balance excessive potassium loss through KCNQ1and may be involved in membrane recycling (1028). In sum-mary, more investigations will be necessary to clarify theroles of the individual Kir channels.
C) KCC4. Apart from being secreted through channels, potas-sium and chloride may exit the parietal cell through trans-porters. This alternative hypothesis is corroborated by arecent observation of Fuji et al. (352). The group reportedthat the K-2Cl cotransporter KCC4 coimmunoprecipitateswith H�-K�-ATPase in apical membrane fractions of pari-etal cells (352). Furthermore, flux measurements in H�-K�-ATPase containing vesicles showed decreased chloride andproton transport under pharmacological blockade ofKCC4, suggesting a functional coupling of KCC4 to H�-K�-ATPase (352). Although the hypothesis that both po-tassium and chloride leave the cell via a transporter is in-triguing, the observation is, as of now, solitary and needsfurther experimental validation.
B. Control of Acid Secretion
Gastric acid secretion is subjected to precise regulation. Thecomplex regulatory machinery that orchestrates the secretionof gastric acid consists of hormonal (gastrin, somatostatin),paracrine (histamine, somatostatin), and neuronal compo-nents (FIGURE 2). The need for this tight regulation is high-lighted by conditions that lead to a hypersecretion of gastricacid, such as Zollinger-Ellisson syndrome (ZES; gastrinoma).Gastric hypersecretion can overcome the measures our bodyundertakes to protect itself from the acid and thereby lead topeptic ulcers. A fine on-demand regulation of acid secretion isthus pivotal to ensure the balance between an adequately lowintragastric pH and tissue protection.
According to the well-established model of acid secretion,the parietal cell is activated by neuronal input from thevagus nerve, endocrine input from gastrin-producing Gcells, and paracrine input from histamine-producing en-terochromaffin-like (ECL) cells (FIGURES 1 AND 2). Thedistinct substances released by these cells, i.e., acetylcho-
line, histamine, and gastrin, directly or indirectly stimulatethe parietal cell by inducing insertion of H�-K�-ATPase atthe apical membrane and are thus commonly referred to asacid secretagogues. The main inhibitor of parietal cell acidsecretion is somatostatin, which is secreted by the D-cellsof the gastric mucosa (FIGURES 1 AND 2). Because of thecomplexity of the network that controls the release ofacid into the stomach, it has been historically challengingto dissect the relative role of each individual regulatorycomponent. Without a doubt, knockout models havegreatly aided us in the last years to gain a more profoundunderstanding of this process, despite their limitations ofchronic compensation. The subsequent chapter aims tosummarize the key players in our canonical model of acidregulation.
1. Cholinergic stimulation/vagus nerve
Since the seminal experiments conducted by Pavlov ondogs, we know that the mere prospect of food ingestion orsham-feeding is sufficient to trigger the secretion of gastricacid (833). This first of three phases of acid secretion iscalled the cephalic phase and is mostly mediated throughthe vagus nerve (595, 725, 910). Hence, before the adventof pharmacological inhibitors, vagotomy has been an effec-tive surgical procedure to control acid-related disorders(301).
The parietal cell receives neuronal input from the vagus nervethat is relayed via cholinergic postganglionic enteric fibers inthe enteric nervous system (ENS) (FIGURES 1 AND 2). In ad-dition, the vagus nerve activates G-cells to release gastrin,resulting in an indirect stimulation of the parietal cell. Di-rect cholinergic activation occurs mostly via muscarinic M3
receptors, which have been identified on the surface of theparietal cell (507, 541, 846). The M3 receptor is a classicseven-transmembrane domain GPCR. Predictably, knock-out of M3 receptors leads to an impairment of gastric acidsecretion and compensatory hypergastrinemia due to nega-tive feedback (9). Following acetylcholine binding, M3 re-ceptor activation mostly causes an increase in intracellularcalcium concentrations (44, 1163). Calcium rises in re-sponse to PLC-mediated IP3 generation and subsequent mo-bilization from intracellular stores (190). The primary ki-nases activated by the M3 receptor are protein kinase C(PKC) and calcium/calmodulin-dependent protein kinase II(CaMKII) (136, 196, 314–316, 773, 774, 1095). Whileactivation of CaMKII has a clear stimulatory effect on acidsecretion, PKC has been reported to have dual effects, al-though reports of an inhibitory role predominate numeri-cally (23, 73, 136, 196, 313, 314, 316, 597, 755, 773,1095). It has been postulated that the expression of differ-ent PKC isoforms may account for this dichotomy (313,314). Current evidence suggests that the PKC-� isoform hasa suppressing effect by trans-inhibiting CaMKII activity,whereas PKC-� increases the baseline levels of intracellularcalcium, thereby sensitizing the parietal cell to subsequent
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
193Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

stimulation (313, 314). Apart from PKC and CaMKII acti-vation, cholinergic signaling activates parietal cell MAPKs,which is partially a downstream effect of PKC activation(771, 1039, 1062, 1063). MAPK activation seems to have abiphasic effect on acid secretion (acute inhibition andchronic augmentation) and also serves as a mediator oftrophic responses in the parietal cell. For example, pro-
longed MAPK activation (72h) has been shown to serve asa maturation and differentiation signal leading to a trans-formation of parietal cell morphology in vitro (1039). Thechange in morphology is accompanied by a downregulationof H�-K�-ATPase gene expression (1039). As of now, it ischallenging to put these findings into a physiological per-spective.
PPIsAPAs
Parietal cell
D-cell
D-cell
ECL-cell
SST
Somatostatin
Somatostatin
Histamine
Basolateral
Oxyntic mucosa
Lumenal
Hist
SSTR
SSTR
K+
H+
Gast
ACh
CCK2
H,K-ATPase
CCK2
M3
PAC1
H2
SST
Gast
PACAP
D-cell
G-cell
Somatostatin
Gastrin
Circulation
Basolateral
Antrum
Lumenal
LowlumenalpH
CalciumAmino acidsPolyamines
ENS
ENS
ENS
ENS
SSTR
VPAC
SST
PACAPVIP
AChGRP
CaSRCaSR
CCK1 CCK
CaSR
?
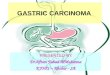
FIGURE 2. Neuroendocrine regulation of gastric acid secretion. In addition to direct neuronal regulation, theparietal cell receives paracrine signals from neighboring ECL- and D-cells. Gastrin is produced in the antralmucosa of the stomach and reaches the oxyntic mucosa via the circulation (endocrine regulation). Gastrin-mediated histamine release represents one of the major stimulatory pathways leading to the secretion ofgastric acid (gastrin-histamine axis). The secretion of gastrin is closely tied to intragastric pH (via somatosta-tin), thereby creating a negative-feedback loop. ACh, acetylcholine; APAs, acid pump antagonists; ENS, entericnervous system; Gast, gastrin; Hist, histamine; PPIs, proton pump inhibitors; SST, somatostatin.
SASCHA KOPIC AND JOHN P. GEIBEL
194 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

In addition to M3 receptors, M1 receptors have also beenimplicated to play a role in the process of acid secretion.This hypothesis was derived from the observation that theM1 receptor is expressed in gastric mucosa and that itsblocker pirenzepine can inhibit gastric acid secretion (29,466). Most evidence pointed to an expression of M1 onECL-cells, where it was speculated to regulate the release ofhistamine (437, 507). More recent findings somewhat sur-prisingly report that pirenzepine also suppresses acid secre-tion in M1-deficient animals. Furthermore, these animalsshow a normal phenotype in terms of acid output (10).These observations question both the involvement of M1
receptors in acid secretion and the specificity of pirenzepine.
Lastly, knockout studies point towards a contribution of theM5 receptor to the regulation of acid secretion, as its deletioncorrelates with decreased acid output (10). Yet, M5 receptormRNA could only be detected in whole stomach homoge-nates, but not in gastric mucosa per se, making its localizationto the submucosal enteric plexus more likely (10).
2. Gastrin/G-cell
Gastrin has been discovered in 1906 by John S. Edkins, whoinjected gastric extracts of pig and cat stomachs into thejugular vein of cats and observed a subsequent increase inacid secretion (298). Gastrin is a peptide hormone that isproduced in specialized G-cells, located in the antral sectionof the stomach (FIGURE 2) and endocrine cells in the duo-denum, small intestine, colon, pancreas, testis, and pitu-itary. It is the main mediator of the so-called gastric phase ofacid secretion, which initiates when the ingested food entersthe stomach. The gastric phase accounts for the majority ofthe acid secretory response of the stomach.
A) SYNTHESIS. The gastrin cDNA encodes a 101-amino acidpre-pro-hormone that undergoes extensive posttransla-tional processing (113, 519, 551, 552, 1161). In brief, thepre-pro-hormone is first cleaved NH2-terminally to createprogastrin and then truncated to two main core proteins,G17 and G34, which can exist in glycine extended (G17-Gly; G34-Gly) or terminally amidated (G17-NH2, G34-NH2) forms. Furthermore, a fraction of progastrin (�47%in humans) is sulfated at Tyr66 in the course of its passagethrough the Golgi apparatus, thereby giving rise to sulfatedand nonsulfated isoforms of gastrin (22). Sulfation has noinfluence on the acid secretory response, as the affinity tothe gastrin receptor remains unchanged (399, 596). G17-NH2 is the main circulating form that mediates the secre-tory effects of gastrin. Although the glycine-extended formshave a low affinity towards the gastrin receptor (CCK2) andthus play no role in gastric acid secretion (they are four tofive orders of magnitude less potent in inducing acid secre-tion), it is still important to acknowledge their existence(178, 722). First, they serve as substrates for the synthesis ofamidated gastrin and are cosecreted with gastrin by theG-cells (1040, 1051). Second, they potentiate the acid se-
cretory response to amidated gastrin, although they have nointrinsic ability to induce acid secretion (178). Third, pro-gastrin and glycine extended gastrins were shown to act asa proliferative signal, especially in the colon (20, 482, 994,1145). This is also of pathophysiological relevance as bothforms can promote cancer growth by presumably inhibitingapoptosis and inducing angiogenesis (71, 87, 900). For ex-ample, it was shown that overexpression of progastrin inmice is a predisposing factor for the development of colo-rectal or bronchoalveolar cancers (587, 1017).
B) REGULATION OF RELEASE. Gastrin is released by the G-cell inresponse to a variety of stimuli of different origin. Directneuronal stimulation of the G-cell occurs via ACh and gas-trin releasing peptide (GRP), which are released by postgan-glionic neurons of the enteric nervous system. The postgan-glionic fibers themselves receive input from the efferentfraction of the vagus nerve (86, 485). On the other hand,food-related signals, such as calcium, amino acids, andamines, can also directly trigger gastrin secretion (FIGURE 2)
(257). The secretory stimuli culminate in an increase inintracellular calcium concentrations, leading to vesiclefusion and gastrin secretion. The main inhibitory signalfor gastrin secretion is somatostatin, which reaches theG-cells in a paracrine fashion from neighboring D-cells(632, 975).
With regard to the neuronal control of gastrin secretion, it isgenerally thought that vagal stimulation increases the re-lease of gastrin, although some conflicting evidence exists(310, 694). Latest experiments that assessed local gastrinconcentrations utilizing microdialysis, however, clearlyshow an increase in gastrin levels following acute electricalvagal stimulation (310). The vagus nerve then synapses onneurons of the ENS, which are thought to release either theneurotransmitter ACh or GRP on a G-cell, leading to secre-tion of gastrin (295, 635, 694, 960, 978). It should be notedthat a recent investigation failed to observe increased gas-trin levels, following exogenous GRP administration in hu-mans (456). Yet, GRP itself serves as a clear acid secreta-gogue, although potentially not via gastrin (456). Whetherthese conflicting observations are attributable to species dif-ferences (most earlier observations utilized rodent models)remains to be elucidated. The ENS is also thought to medi-ate parietal and G-cell activation in response to mechanicaldistension of the stomach (455, 962, 977). The neurohor-monal response to gastric stretch is an integral part of thegastric phase of acid secretion. Closer examination, how-ever, reveals that the reports are very conflicting in that it isnot clear whether a pure mechanical distension stimulatesor inhibits gastrin release (455, 664, 803, 962, 977). Abiphasic model characterized by initial inhibition of gastrinsecretion under low volumes followed by stimulation underhigh volumes has been suggested, but awaits further confir-mation (977).
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
195Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

Dietary components, such as amino acids and calcium, candirectly promote the secretion of gastrin and can thus sus-tain acid secretion in the gastric and intestinal phase asdigestion progresses (652, 1074). A rise in serum calciumconcentrations evokes a similar effect. The correlation be-tween calcium and gastrin is discussed in a separate section(see sect. VD2). It has been unclear for a long time as to howthese dietary components activate the G-cell. An involve-ment of the ENS has been proposed as the most likely ex-planation in the past. More recent observations, however,strongly indicate that the calcium-sensing receptor (CaSR)represents the molecular link between luminal dietary con-stituents and G-cell activation (325). The CaSR and its rolein the stomach are discussed separately and shall only besummarized at this point (FIGURE 8) (see sect. IVD). First,the same dietary components, i.e., amino acids, amines, andcalcium, which have all been shown to trigger gastrin re-lease also function as activators of CaSR (652, 1074). Sec-ond, CaSR is expressed on the apical and basolateral side ofthe G-cell, which allows it to act as nutrient sensor both inthe gastric lumen and the circulation (142, 182, 886).Third, direct activation of the CaSR is known to stimulateacid secretion (145, 291, 373). Finally, and most impor-tantly, CaSR (�/�) animals lack the gastrin secretory re-sponse to intraluminal instillation of peptone, calcium, andphenylalanine (325). In light of this evidence, it is highlylikely that CaSR is the long elusive luminal nutrient sensorthat regulates the secretion of gastrin from the G-cell.
The plasma levels of gastrin are closely tied to the intragas-tric pH. Low intraluminal pH is a potent inhibitor of gastrinrelease, which serves as a negative-feedback mechanism toimpede an overproduction of acid. Conversely, a more al-kali intragastric pH induces the secretion of gastrin, whichaccounts for the commonly observed hypergastrinemia instates of acid suppression, such as during proton pumpinhibitor (PPI) therapy. The pH dependency of serum gas-trin levels is mainly relayed via somatostatin, as acid di-rectly stimulates somatostatin release (see sect. IIB4). Soma-tostatin, released by neighboring antral D-cells, in turn actsas the main inhibitor of gastrin secretion (FIGURE 2). Thephysical proximity to G-cells allows for a fine paracrineregulation of gastrin release. Although it is generally ac-cepted that intragastric pH mostly modulates local soma-tostatin levels, the G-cell may also directly sense intragastricpH via CaSR. CaSR is acid sensitive, and it has been shownthat isolated rat G-cells secrete less gastrin when the extra-cellular pH is dropped from 7.4 to 5.5 (569). However,more investigations are needed to substantiate this evi-dence. Furthermore, gastrin release is also inhibited by neu-ronal regulation by the ENS. The neurotransmitter galaninhas been demonstrated to exert a direct inhibitory effect onisolated G-cells (695, 961).
C) CELLULAR EFFECTS. Following secretion, gastrin enters thebloodstream and acts on its target cells in an endocrine
fashion. Its half-life is determined by its rate of eliminationfrom the plasma which mainly occurs by metabolism in thekidney, gut, and brain (419, 420). The importance of renalelimination is corroborated by the observation that patientswith renal failure present with higher plasma gastrin levels(818, 1075).
The two primary target cells of gastrin are the histamine-secreting ECL cell and the parietal cell. Gastrin exerts itsfunctions via binding to the cholecystokinin receptor type 2(CCK2), a seven transmembrane domain G protein-coupledreceptor, which is expressed on mature parietal and ECLcells, but also on gastric stem cells (560, 596, 608, 769, 772,904). On the ECL cell, gastrin binding causes the release ofhistamine, which in turn stimulates the parietal cell in aparacrine fashion (FIGURE 2) (see sect. IIB3) (412). Thisactivation cascade is commonly referred to as the gastrin-histamine axis. Evidence for a direct, i.e., nonhistamine-relayed, activation of H�-K�-ATPase in the parietal cell bygastrin exists, but is far less substantiated (459, 1024,1025). Gastrin may sensitize the parietal cell to subsequentsecretagogue stimulation, rather than acting as a bona fidesecretagogue itself. Canonically it is widely accepted thatgastrin exerts its physiological effects mostly via activationof ECL cells (24, 1131). Knock-out of gastrin leads to asevere impairment of basal and stimulated acid secretion(179, 347). Apart from stimulating acid secretion, gastrinserves as a pivotal proliferative signal for the gastric mucosain general (60, 410, 534, 631, 816). It is commonly ob-served that elevated plasma gastrin levels lead to substantialmucosal proliferation (60, 410, 534, 631, 816). This phe-nomenon has been extensively described in various knock-out animals suffering from hypochlorhydria and concomi-tant hypergastrinemia, but also in patients with ZES (39,515, 584, 1066). The source of mucosal cell proliferation isprogenitor cells located in the isthmus region of the gastricgland (545). Expression of the CCK2 has been confirmed onseveral gastric progenitor cells (560, 769). Furthermore,gastrin has been shown to stimulate cell migration from theprogenitor region along the gastric gland axis (578). Muco-sal hyperplasia thus ensues most likely via a direct activa-tion of precursor cells by gastrin. Although hypergastrine-mia causes a generalized mucosal hyperplasia, ECL cellsseem to be particularly regulated by gastrin, as their relativefraction compared with other mucosal cells increases underprolonged gastrin exposure (60, 410, 631). Conversely, theabsence of the CCK2 almost entirely eliminates matureECL-cells from the gastric mucosa (177, 622). [Somewhatsurprisingly this does not occur when gastrin itself isknocked out (179, 347).] It should be noted that the M3
receptor seems to be necessary as a cofactor mediating thetrophic effects of gastrin, as its absence is associated with anormal mucosal phenotype despite elevated serum gastrinlevels (see above) (9). The mechanism underlying this inter-dependency between gastrin and the M3 receptor is as ofnow elusive. The cholinergic and gastrin systems also seem
SASCHA KOPIC AND JOHN P. GEIBEL
196 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

to be intertwined with regard to acid secretion. In the ab-sence of the CCK2 receptor, the parietal cell’s acid secretoryresponse to the secretagogue carbachol (ACh analog) isabolished, while the response to histamine remains intact(543). Again, one can only speculate about the molecularbasis of this interaction.
In conclusion, gastrin is the most important activator ofacid secretion in the stomach. The role of gastrin, and espe-cially its glycine extended forms, has evolved beyond beinga mere acid secretagogue to being an important global reg-ulator of cell growth and differentiation. Furthermore, theregulation of gastrin by the levels of plasma calcium pro-vokes the question as to whether gastrin itself in turn has animpact on global calcium homeostasis. A subsequent sec-tion makes an attempt at addressing this question (see sect.VD2).
3. Histamine/ECL cell
Histamine has been discovered as early as 1910 by Dale,Barger and Laidlow in extracts of ergot fungi (63, 237). In1920, Popielski for the first time described its effect on thesecretion of gastric acid (866). He observed that subcutane-ous administration of histamine resulted in increased acidsecretion (866). Furthermore, he concluded that this effectwas independent of the vagus nerve, as secretion still tookplace after vagotomy and administration of atropine. Thisled Popielski to postulate that histamine exerts its effectsdirectly on the level of the gastric gland (866). The hypoth-esis that histamine acts in a paracrine fashion on parietalcells and that its release is regulated by the levels of gastrinhas been put forward for the first time by Emmelin andKahlson in 1944 (306). At this point, the cellular source ofhistamine was still obscure. It was only in the late 1960sthat histamine had been histochemically localized to theECL cells of the gastric gland (413, 1084).
A) SYNTHESIS AND REGULATION OF RELEASE. Histamine is theeffector of the gastrin-histamine axis and directly stimulatesthe parietal cell to secrete hydrochloric acid (FIGURE 2).Histamine is derived from the amino acid histidine, which isenzymatically converted to histamine by L-histidine decar-boxylase (HDC) (957). The effects of genetic HDC deletionare predictably severe: animals lacking HDC have a lowbasal acid output that does not respond to exogenous ad-ministration of gastrin (1066).
Histamine is stored in secretory granules of the ECL cell andis released into the surrounding milieu in response to stim-ulation by gastrin and neuronal signals. Stimulation by gas-trin occurs via activation of its GPCR CCK2 (772, 904).Gastrin affects the ECL cell in multiple ways. First, gastrinexposure increases the levels of HDC expression by enhanc-ing its transcription and inhibiting its degradation, to allowfor increased synthesis of histamine (268, 331). The molec-ular mechanism underlying increased HDC transcription is
fairly well understood. Following CCK2 activation, in-creased transcription of HDC is mediated via a PKC- andERK-dependent pathway (470, 472). The HDC gene pro-moter is then activated by at least three distinct nuclearfactors which bind to gastrin response elements, resulting ingene transcription (889, 890). Apart from augmenting genetranscription, gastrin regulates the degradation of HDC,which further increases intracellular enzyme levels (331,1214). Second, gastrin enhances the transcription of the vesic-ular monoamine transporter type 2 (VMAT2; SLC18A2),which is responsible for accumulating histamine in the se-cretory vesicles (376). Similarly to HDC, this effect dependson PKC and ERK activation and binding of a nuclear factorto a gastrin response element in the VMAT2 promoter re-gion (164, 1154). It should be mentioned that gastrin reg-ulates the transcription of a plethora of other genes whichserve a diverse array of roles, ranging from growth to me-tabolism (346). Amongst many others these include chro-mogranin A, which is essential for granule packaging and isa precursor of pancreastatin (see sect.VD3) (231). Third,gastrin induces the fusion of secretory granules and therelease of histamine into the gland environment. Secretionfollows a biphasic elevation of intracellular calcium concen-trations after activation of CCK2 (1201). The biphasic in-crease has been proposed to result from initial IP3-mediatedrelease from intracellular stores, which is followed by sub-sequent influx of calcium via L-type calcium channels fromthe extracellular space (1201). The importance of intracel-lular store mobilization has been contested by a differentgroup, which proposed that solely influx trough L-type, andto a lesser extent N-type, calcium channels triggers the se-cretory response (673). Lastly, gastrin has a trophic effecton the ECL cell (see sect. IIB2).
Apart from gastrin, ECL cells are stimulated by pituitaryadenylate cyclase activating polypeptide (PACAP), which isa neuropeptide expressed in the ENS of the gastric mucosa(737, 1054). PACAP has homology to vasoactive intestinalpolypeptide (VIP) and binds to a distinct receptor (PAC-1)on the ECL cell (1207, 1208). Binding of PACAP to PAC-1induces release of histamine (672, 798, 944, 1207). Similarresults have been obtained with VIP, which is attributableto partial agonism at PAC-1 (798, 941). Historically, inves-tigations yielded controversial results with regard to theeffects of exogenously administrated PACAP on acid secre-tion. Both an inhibition and stimulation of acid secretionfollowing PACAP injection are reported (760, 862, 944,1207). This discrepancy is most likely attributable to thefact that PACAP can also act as an agonist of the VIP re-ceptor (VPAC) on the somatostatin-secreting D-cell, lead-ing to a concomitant suppression of acid secretion by soma-tostatin release (1207). Indeed, if an anti-somatostatin an-tibody is injected into rats simultaneously with PACAP,acid secretion is elevated threefold from baseline (comparedwith 1.5-fold in the absence of an anti somatostatin anti-body) (1207). Evidence points to the fact that the PACAP-
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
197Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

stimulated release of somatostatin is of particular impor-tance in the mouse, as most studies showing a suppressionof acid secretion after PACAP administration were con-ducted in murine models.
PACAP has very similar effects on the ECL cell as gastrin.Similarly to gastrin, PACAP causes histamine release byincreasing intracellular calcium concentrations via calciuminflux through L-type, but also ligand-gated calcium chan-nels (673). In further analogy to gastrin, PACAP upregu-lates the expression of HDC and exerts trophic effects onthe ECL cell (590, 729, 810). Contradictory results withregard to the effects of acetylcholine on histamine releaseexist. It has been reported that acetylcholine can either stim-ulate or has no effect on the secretion of histamine in in vitroexperiments on isolated ECL cells (481, 672, 674, 941,946). In vivo application of muscarinic agonists, followedby measurement of histamine concentrations using micro-dialysis, also yielded no evidence for cholinergic stimulation(798). Conversely, it is well accepted that adrenergic stim-ulation leads to an increase in histamine release; however,the physiological relevance of adrenergic activation of ECLcells is not entirely clear (636, 672, 674, 798, 871, 941).
The ECL cell is inhibited by a variety of substances, themost prominent of which is somatostatin (204, 590, 798,941). Somatostatin is produced in D-cells of the oxynticmucosa and reaches the ECL cell in a paracrine fashionwhere it binds to the somatostatin receptor (SST2 and po-tentially SST5) (FIGURE 2) (570, 873). Receptor bindingleads to inhibition of histamine exocytosis via blockade ofmostly L-type calcium channels (105). This impedes theelevation of intracellular calcium concentrations caused byECL activators, such as gastrin (see above) (873). In addi-tion, somatostatin also inhibits the proliferation of ECLcells (570). Somatostatin can thus be seen as the globalhormonal antagonist to gastrin with regard to ECL cellfunction and proliferation. The neuronal inhibition of ECLcells is mainly carried out by the neuropeptide galanin (105,672, 798, 1209). Galanin is localized to neurons of the ENSand demonstrated an inhibitory effect on histamine secre-tion in in vitro and in vivo models (105, 302, 672, 731, 798,1209). Similarly to somatostatin, the molecular mechanismunderlying its inhibitory effect is an interference with cal-cium signaling via closure of L-type calcium channels (105).Lastly, prostaglandin E and nitric oxide also act as inhibi-tors of histamine release (105, 554, 798, 1002). Althoughneuropeptide YY (PYY) and calcitonin gene-related peptide(CGRP) have also been implicated in playing a role in ECLcell regulation, a detailed discussion is omitted in light ofcontradictory results which range from stimulation to inhi-bition of secretion (672, 674, 798, 1210).
B) CELLULAR EFFECTS. As mentioned earlier, stimulation of theECL cell is translated into an elevation in intracellular cal-cium concentrations, leading to exocytosis of preformed
histamine-containing secretory vesicles. The molecularmechanism of vesicle fusion with the apical membrane re-lies on the formation of the core SNARE complex, consist-ing of syntaxin, synaptobrevin, and SNAP-25. Synaptotag-min presumably acts as a calcium sensor relaying theintracellular calcium signal to the vesicle fusion proteinapparatus. The expression of all SNARE complex pro-teins has been confirmed in the ECL cell (471, 477,1215). In accordance with these findings, introduction ofthe neurotoxins tetanus toxin light chain and botulinumtoxin, which cleave constituents of the SNARE complexapparatus and thereby render it nonfunctional, result ininhibition of histamine secretion (477).
Very small amounts of histamine are sufficient to induceacid secretion. Histamine acts via the H2 receptor on theparietal cell, which has been discovered by Sir J. W. Black in1972 (106). For this seminal discovery, he was laterawarded the Nobel Prize in Physiology and Medicine. TheH2 receptor belongs to the family of seven-transmembranedomain GPCRs. Its activation predominantly leads to in-creases in the intracellular levels of cAMP, but also of cal-cium, which serve as stimulatory signals for H�-K�-ATPasetrafficking (67, 189, 738, 840, 1026, 1143). In analogy,pharmacological agents that elevate cAMP, such as IBMXor forskolin, induce acid secretion (1026, 1191). The in-crease in cAMP is due to activation of adenylate cyclase viaGs. The role of calcium in the process of histamine secretionremains a controversial matter. First, the mechanism lead-ing to histamine-induced increases in intracellular calciumhas been subject of discussion. Evidence exists that hista-mine can, apart from adenylate cyclase, also activate PLC,leading to calcium release from intracellular stores (607,1142, 1143). Conversely, it has been suggested that theobserved increases in intracellular calcium are a byproductof cAMP-mediated PKA activation, which in turn can reg-ulate the opening of calcium channels (144, 189, 840). Sec-ond, it is questionable to what degree the calcium signal isan integral and necessary part of the acid secretory responseto histamine (738, 840). Chelation of the transitory calciumincreases with BAPTA abolishes only the secretory responseof isolated gastric glands to histamine by �40%, while itcompletely eliminates the response to cholinergic stimula-tion (738). Also, live fluorescence imaging in isolated glandsshowed no spatiotemporal correlation between the hista-mine-induced increases in calcium and the onset of acidsecretion, thereby questioning an involvement of calcium inthe secretory response (840).
H2 receptor knockout animals effectively illustrate the sig-nificance of the histamine-gastrin axis in gastric physiology.Lack of the H2 receptor leads to a complete failure of gas-trin or histamine to induce acid secretion (584). The secre-tory response to carbachol, however, remains intact (584).Hypergastrinemia develops as a feedback mechanism withthe aim of reestablishing acid secretion, leading to mucosal
SASCHA KOPIC AND JOHN P. GEIBEL
198 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

hypertrophy (584). In light of the central role of the H2
receptor in parietal cell physiology, it has been successfullyused as a pharmacological target with the aim of suppress-ing gastric acid output (see sect. IIC2).
4. Somatostatin/D-cell
Somatostatin was isolated for the first time in 1973 fromovine hypothalamus and characterized as an inhibitor ofgrowth hormone release from the pituitary gland (124). Afew years later somatostatin was identified in endocrinecells of the stomach, which we now know as D-cells (638).
A) SYNTHESIS AND REGULATION OF RELEASE. Somatostatin is apeptide hormone that exists in two primary forms that dif-fer in their respective peptide length. The most abundantform in the gastric mucosa is somatostatin-14 (consisting of14 amino acids), whereas somatostatin-28 only constitutesa minute fraction of the total gastric somatostatin content(198, 1125). The two forms of somatostatin are cleavageproducts of a larger 116-amino acid pre-prohormone (pre-prosomatostatin), which in turn is processed to the 92-amino acid-long prosomatostatin (1000). It should be men-tioned that other cleavage products, such as antrin or so-matostatin-28(1–12) exist and are secreted together withsomatostatin (77, 885). Their physiological significance is,however, less well understood.
Somatostatin is the global antagonist of the acid secreta-gogues. It is produced by intestinal and gastric D-cells, thelatter of which exist in two populations in the stomach (61):an antral population locally inhibits the release of gastrinfrom G-cells, whereas a population localized to the acid-producing oxyntic mucosa directly regulates the parietalcell and inhibits histamine release from the ECL cell (FIG-URE 2) (19). The morphology of the D-cell is characteristicin that it possesses long cytoplasmic processes, which allowit to communicate with and regulate neighboring cells in aparacrine fashion (620, 632). It is worthwhile to distinguishthe two populations of gastric D-cells, as each populationpossesses unique physiological properties (1202).
The antral D-cell is mostly regulated by the local concen-trations of gastrin, cholecystokinin, and intraluminal pH.Gastrin induces somatostatin secretion from D-cells, whichcauses reciprocal inhibition of gastrin release from neigh-boring G-cells, thereby creating a local negative-feedbackloop (976, 1011, 1202). The molecular mechanism under-lying this loop is, however, less clear. CCK2 receptor is, if atall, only expressed at very low levels in the antral mucosa(749, 905, 967). It has been proposed that gastrin stimu-lates somatostatin release in the antrum in a receptor-inde-pendent mechanism (1202). This may be accomplished viadirect cell-cell contacts between the G- and the D-cell,which have been demonstrated with electron microscopy(620). Conversely, evidence for cholecystokinin and itsstimulatory role for somatostatin release via CCK1 is more
substantiated (749, 905, 967, 1202). Cholecystokinin isstructurally closely related to gastrin (both share an identi-cal 5-amino acid COOH terminus) and also exists in vari-ous peptide lengths (767). It is secreted by I-cells of the smallintestine following protein and fat-rich chyme entering theduodenum, and thus represents a classical mediator of theintestinal phase of acid secretion (594). As its name implies,cholecystokinin has originally been described as a stimula-tor of gallbladder contraction; however, its inhibitory influ-ence on gastric acid secretion is now well accepted andextensively described (593, 1203). Cholecystokinin canbind to both the CCK1 and CCK2 receptor with almostequal affinity, whereas the actions of gastrin are almostexclusively mediated by the CCK2 receptor. The dual affin-ity of cholecystokinin would imply a possible stimulatoryeffect on acid secretion via activation of CCK2 on ECL cells;however, in vivo the inhibitory effect mediated by activa-tion of CCK1 and CCK2 on D-cells prevails (593, 966,1202, 1203).
One of the most important stimulators of D-cell secretion isthe intragastric pH. A seminal observation demonstrating acorrelation between gastric acidity and the amount of se-creted somatostatin was made in dogs in the 1970s. It hasbeen shown that the amount of somatostatin directly in-creases in antral venous blood following gastric HCl infu-sion, while somatostatin levels were unaffected in venousblood from the oxyntic mucosa (982). Similar observationswere later made in isolated mouse stomach, however with-out topographic discrimination (975). Two main hypothe-ses as to how somatostatin is regulated by intragastric pHexist. The first states that the D-cell can directly act as a pHsensor, and the second postulates that the pH sensing ismediated by neurons, which in turn act on D-cells. To ac-complish putative direct pH sensing, several antral D-cellsare equipped with a distinct morphological feature. Theypossess apical projections that are in contact with the glan-dular lumen, potentially allowing them to constantly mon-itor the intraluminal milieu (620). These D-cells have beentermed open type. Conversely, the D-cells of the oxynticmucosa are mostly of the closed type, meaning that they areembedded in the mucosa without luminal contact. The mo-lecular identity of the putative apical pH sensor remainselusive. However, the presence of CaSR, which has pHsensing properties, was recently confirmed in preliminarystudies on the D-cell and may represent a possible candidatefor this mechanism (770). Apart from directly acting onD-cells, the effect of pH on somatostatin secretion may bemediated via afferent spinal neurons. Over 80% of the spi-nal afferent neurons contain the neuropeptide CGRP (397,758, 1047, 1116). Perfusion models of antral sleeves haveshown that the acid-induced rise in somatostatin is accom-panied by a concomitant increase in the concentrations ofthe neuropeptide CGRP (708). Furthermore, application ofa CGRP receptor blocker inhibited the release of somatosta-tin following acid exposure (708). As D-cells are known to
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
199Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

express the CGRP receptor, an involvement of CGRP inacid sensing is plausible (558). Again, this provokes thequestion of how CGRP-containing neurons may sense acid-ity on a molecular basis. The acid-sensitive channels tran-sient receptor potential vanilloid channel (TRPV1) and theacid-sensing ion channel 3 (ASIC3) had been proposed asmolecular acid sensors; however, latest experiments haveshown that the increase in CGRP still occurs in the geneticabsence of the channels (47, 96, 163).
Neuropeptides of the gastric ENS that stimulate the secre-tion of somatostatin include PACAP and VIP, which bothbind to the VPAC receptor expressed on D-cells (199, 657,1207). The presence of VIP and PACAP containing neu-rons, which integrate signals from the vagus nerve, has beendemonstrated in the gastric mucosa (302, 737). Further-more, cholinergic signals can act on the antral D-cell via theM3 receptor to promote secretion of somatostatin (140).This is in sharp contrast to D-cells from the oxyntic mucosathat are inhibited by cholinergic signals (197, 200, 1182).As mentioned earlier, the D-cells in the oxyntic mucosa alsodiffer in their morphology. D-cells in the oxyntic mucosaare of the closed type and have thus not been implicated toparticipate in acid sensing. They exert their acid-suppres-sive effects by the paracrine regulation of ECL and parietalcells. Further functional divergence between antrum and theoxyntic mucosa has been demonstrated in the regulation of thesomatostatin mRNA. For example, suppression of acid secre-tion with omeprazole in fasted animals markedly decreasedsomatostatin mRNA levels in the antrum, whereas the levels inthe oxyntic mucosa were affected to a much lesser extent,which further corroborates the hypothesis that the antral cellsare involved in luminal chemosensation (945).
B) CELLULAR EFFECTS. The effects of somatostatin on its targetcells are mediated by the SST2 receptor. Knockout of the re-ceptor causes a 10-fold increase in basal acid output, whichexemplifies the pivotal role somatostatin plays as a global sup-pressant of acid secretion (715). Somatostatin acts on all maincell types that are involved in the process of acid secretion, i.e.,parietal cells, ECL cells, and G-cells (FIGURE 2). The inhibitionof the G- and ECL cells has been discussed in the respectivesections. In the parietal cell, somatostatin has a clear directinhibitory effect on secretagogue-induced acid secretion (827,1177). This effect is partially attributable to activation of Gi,leading to inhibition of adenylate cyclase and a subsequentdecrease in intracellular cAMP levels (827).
In conclusion, somatostatin acts as the global brake on acidsecretion. By acting on G-cells, ECL cells, and parietal cells,it exerts its inhibitory action on every link in the regulatorychain leading to the secretion of gastric acid.
5. Other substances
A variety of other substances have been shown to haveeither direct or indirect effects on acid secretion. In the
interest of conciseness, their physiological effects will onlybe discussed briefly at this point.
A) SECRETIN. Secretin is a 27-amino acid peptide hormonethat is synthesized in duodenal S-cells and secreted into thecirculation in response to a low duodenal pH or passage ofdigestive products, such as fat (195, 955, 1153). A subpop-ulation of secretin-producing cells is also present in thegastric mucosa, where it may influence acid secretion in aparacrine manner (191–193). Given its secretory stimulus,it is regarded as a classic effector of the intestinal phase ofacid secretion. When it was first discovered in 1902 byBayliss and Starling (interestingly secretin was the first hor-mone ever to be discovered), it was noted that secretin in-duces pancreatic bicarbonate secretion, which leads to abuffering of the gastric acid entering the duodenum (68). Inthe stomach, secretin acts as an inhibitor of gastric motilityand acid secretion (141, 194, 269, 374, 532, 564, 656, 677,1107). The exact mechanism as to how secretin attenuatesthe secretion of acid is not exactly known, and several hy-potheses have been put forward. For example, it has beenshown that secretin induces the secretion of somatostatinfrom isolated D-cells (141). Increases in somatostatin levelswere also observed in isolated perfused stomach models (205,374). Others have proposed that secretin activates vagal pri-mary afferent neurons, which in turn leads to neuronal mod-ulation of acid secretion (656, 659). In opposition to this the-ory, it has also been demonstrated that the inhibitory effects ofsecretin are independent of vagotomy (677).
B) OXYNTOMODULIN. Oxyntomodulin is a peptide hormoneproduced in the mammalian intestine. It is closely related toglucagon and contains its entire amino acid sequence, ex-tended by a COOH-terminal octapeptide (66). In isolatedparietal cells, oxyntomodulin acts as an activator of acidsecretion (959). The integrated response to oxyntomodulinis, however, opposite. Systemic injection decreases gastricacid secretion in rat, cat, and human test subjects (53, 157,285, 524, 525, 965). The inhibitory effect is most likelymediated via somatostatin release (53).
C) SEROTONIN. It was recognized in the early 1950s that se-rotonin was present in the antral mucosa of dog stomachs(323). Serotonin is stored in granules of enterochromaffincells of the antrum (1099). It is released into the circulationand the gastric lumen in response to vagal stimulation (107,649). Intraluminal acidification serves as another stimulusfor serotonin release (1196). Serotonin has an inhibitoryeffect on the secretion of gastric acid (107, 153, 521, 650,720, 903). It is still poorly understood where serotonininterferes with acid secretion.
D) NEUROTENSIN. Neurotensin is a 13-amino acid neuropep-tide that was originally isolated from calf hypothalamus(161). In the periphery, it is also produced and secretedpostprandially by specialized endocrine cells (N-cells) of the
SASCHA KOPIC AND JOHN P. GEIBEL
200 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

small intestine (863). Various investigations have demon-strated that neurotensin suppresses the secretion of gastricacid and delays gastric emptying (25, 108, 486, 985). Thishas been shown by direct systemic injection, but also byimmunoneutralization of endogenous neurotensin in a re-verse approach (25, 108, 486, 985). In disagreement withthese findings, other investigators could only inhibit acidsecretion at unphysiologically high serum concentrations of�750 pmol (747). Of note, physiological postprandial neu-rotensin levels were measured to be �15 pmol by the sameinvestigators, questioning the role of neurotensin as a phys-iological endocrine inhibitor of acid secretion (747). Neu-rotensin is also located to nerve fibers of the enteric nervoussystem in the stomach, indicating that it may act as a localneuronal rather than an endocrine regulator. It has beenproposed that neurotensin may induce the secretion of so-matostatin and thereby exert its inhibitory action on acidsecretion (53, 414). Most recently, however, the low-affin-ity neurotenstin type 2 receptor (NTS2) has been identifiedon the parietal cell, suggesting a direct influence.
E) GHRELIN. Ghrelin is a recently discovered 28-amino acidpeptide hormone that is synthesized in P/D1 cells of thefundus (242). Since its discovery, multiple functions havebeen ascribed to it, ranging from being a regulator of appe-tite to being a modulator of bone remodeling. Its effects onbone are described in a separate section of this review (seesect. VD1). Apart from these functions, ghrelin also hasbeen implicated to affect gastric acid secretion, although itremains a matter of discussion in which direction, as periph-erally administered ghrelin has been reported to stimulate,inhibit, or not affect acid secretion (278, 355, 654, 719).The reason for these dichotomic results is largely unclear.The fact that ghrelin circulates in acylated and desacylatedforms adds further complexity to the subject (491). Indeed,acylated ghrelin has been shown to stimulate acid secretionfollowing peripheral injection, whereas desacylated ghrelinremained without effect (938). Further investigations areneeded to clarify the controversy surrounding ghrelin andits influence on gastric acid secretion.
F) NITRIC OXIDE. Nitric oxide (NO) is an important signalingmolecule that plays a role in multiple physiological pro-cesses, such as vasodilation or the immune response. In-deed, NO has been shown to mediate the hyperemic re-sponse of the gastric mucosa that occurs during acid secre-tion (553). However, NO also directly influences theproduction of acid. The effect of NO on acid secretion ismost likely inhibitory (81, 82, 555, 1002; opposed by Ref.426). NO is produced by various forms of NO synthases,one of which has been localized at high concentrations incells in the vicinity of parietal cells, allowing for a putativeparacrine regulation (80). NO has been proposed to exertits inhibitory action by either directly inhibiting the parietalcell or by suppressing the release of histamine from ECLcells (81, 82, 555, 1002). Intracellular increases in cGMP
concentrations have been observed in both cell types afterNO exposure, suggesting that guanylate cyclase is an intra-cellular target for NO (82, 1002).
G) INTERLEUKINS. Interleukins (IL) are cytokines that mainlycoordinate immune responses. In particular, IL-1� has beenshown to impact gastric acid secretion. IL-1� is a generalproinflammatory cytokine that plays an important role inthe stomach in the context of Helicobacter pylori infection.H. pylori infection triggers an elevation of IL-1� levels aspart of the host’s immune response (65). Peripheral injec-tion of IL-1� can profoundly suppress gastric acid secretion(912, 947, 1059, 1101, 1132). Multiple explanations forthis observation have been put forward. It has been sug-gested the IL-1� acts in the CNS, as intrathecal injectionalso has an acid-suppressive effect (948, 949). Others havesuggested that IL-1� promotes formation of prostaglandinsor NO, which in turn inhibit acid secretion (312, 947,1101). Yet, a direct effect on parietal cells and ECL cells isthe most likely explanation, as both cell types express theIL-1 receptor and have been shown to be inhibited in theirfunction in isolated cell models (69, 70, 872, 958).
C. The Pharmacological Suppressionof Acid Secretion
Decreasing gastric acidity is indicated in many pathologicalcontexts, including gastric reflux disease or peptic ulcer dis-ease. This target can be achieved by two main pharmaco-logical approaches: 1) the inhibition of gastric acid secre-tion or 2) the intraluminal neutralization of already secretedgastric acid (antacids). Gastric acid secretion can be atten-uated by either directly blocking its final molecular effector,namely, H�-K�-ATPase (PPIs and acid pump antagonists),or by interfering with the neurohormonal signaling path-way leading to its secretion (H2 antagonists). The followingsection attempts to discuss the four most common sub-stance classes employed to increase intragastric pH.
1. Direct pharmacological inhibition of H�-K�-ATPase
The inhibition of H�-K�-ATPase-mediated proton trans-port represents the main contemporary pharmacologicalstrategy for reducing gastric acidity. An increase of gastricpH is the main factor ameliorating acid-related disordersand has been show to directly correlate with healing rates of,for example, GERD (74). Two main substance groups exerttheir acid-reducing effect via inhibiting H�-K�-ATPase func-tion: PPIs and acid pump antagonists (APAs). Both substancesachieve this aim by distinct mechanisms.
Omeprazole was the first clinically available PPI (324). Thefirst patent on omeprazole was filed in 1979 by the Swedishcompany Astra AB (today AstraZeneca). The introductionas a prescription PPI followed in 1989. Today, the omepra-zole enantiomer esomeprazole (S-omeprazole) generates the
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
201Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

second highest revenue of all pharmaceuticals in the UnitedStates and is only surpassed by the statin atorvastatin (512).Furthermore, in the United States, PPIs are available asover-the-counter formulations, making them accessible forthe broad public. This is partially made possible by the highsafety profile of PPIs with a low incidence of unspecificadverse effects. Recently, however, concerns about thelong-term effects of chronic acid suppression have emergedwith regard to its impact on bone health (see sect. VA).
PPIs are delivered as pro-drugs through the bloodstream tothe parietal cell. They are weak bases (pKa �4), which caneasily pass the cell membrane and accumulate in acidic com-partments, such as the secretory canaliculus of the parietalcell. The pro-drug is then converted to the pharmacologi-cally active cyclic sulphenamide by the acidic pH in thesecretory canaliculus (670, 1007, 1135). Their specific ac-cumulation in acidic milieus and their pH-catalyzed conver-sion to active substances confers specificity and thus a highsafety profile to PPIs. Once activated, PPIs bind covalentlyvia disulfide bonds to H�-K�-ATPase, thereby inhibiting itscapacity to pump protons (89, 90, 1005, 1006, 1008). Thepattern of the cysteine residues, which are involved in PPIbinding, differ among the respective members of the PPIfamily: cysteine-813 reacts with all PPIs. In addition,omeprazole reacts with cysteine-892, lansoprazole withcysteine-321, and pantoprazole and tenatoprazole, respec-tively, with cysteine-822 (89, 90, 1005, 1006, 1008). Sincethe binding is covalent and irreversible, the inhibitory effectof PPIs lasts long beyond their plasma half-life, which usu-ally ranges between 0.5 and 2 h depending on the specificPPI (581, 1036). PPIs are generally metabolized by the he-patic cytochrome P-450 system, in particular CYP2C19and CYP3A4. This is of particular clinical importance, asCYP2C19 polymorphisms are known to exist. These poly-morphisms can impact the pharmacokinetics of PPIs byaffecting the metabolic rate of CYP2C19, which may haveconsequences for the optimal therapeutic regimen (582).Esomeprazole and rabeprazole seem to be less dependent onCYP2C19 metabolism (516, 983). Apart from the patternof cysteine reactivity, half-life and metabolism, PPIs alsovary in oral bioavailability (581).
Suppression of acid secretion can never be complete, asH�-K�-ATPase is subjected to a constant turnover (half-life�50 h) and needs to be stimulated for the conversion of thePPI to take place (936). Nevertheless, PPIs are highly effec-tive in reducing gastric acidity. Depending on the PPI andthe regimen, overall intragastric pH can be elevated by sev-eral pH units, up to a pH of 6 (compared with 1–2 atbaseline) (137, 425, 1036). For an excellent summary of PPIefficacy, please refer to Reference 1036.
APAs represent the second class of H�-K�-ATPase inhibi-tors. Unlike PPIs, they do not undergo irreversible binding,but rather act as potassium competitive antagonists. The
duration of inhibition is thus directly dependent on theplasma concentration of the inhibitor. As predicted by ho-mology modeling, mutational analysis, but also recentstructural data, APAs bind in the luminal cavity of H�-K�-ATPase in the vicinity of the potassium entry site where theyexert their inhibitory action (2, 42, 761, 1104, 1106). Al-though the inhibition of acid secretion has been shown to bevery effective, these substances are generally not in clinical use(577). For example, clinical trials of the APA AZD08650 haveshown no additional therapeutic effect compared with the PPIgold-standard, which resulted in abandonment of the drug in aclinical setting (262, 539).
2. H2 antagonists
The development of H2 blockers is inseparably intertwinedwith Sir Black’s discovery of the H2 receptor on the gastricparietal cell at the Smith Kline and French Laboratories(now GlaxoSmithKline) (106). In his original publication,Sir Black also describes burimamide as a competitive H2
antagonist that can effectively inhibit pentagastrin-stimu-lated gastric acid output in human volunteers (106). Furtherdevelopment of the antagonist led to the synthesis of cime-tidine, which was first commercially introduced in 1976 inthe United Kingdom, followed by the United States in 1977.Other commonly used members of H2-antagonist familynow include ranitidine, famotidine, and nizatidine.
H2 antagonists prevent histamine-mediated stimulation ofthe parietal cell by competitively interfering with its recep-tor. Although this effectively terminates the gastrin-hista-mine axis, the parietal cell is still susceptible to cholinergicstimulation via the M3 receptor. This partial inhibitionmainly accounts for the lower clinical efficacy of H2 antag-onists compared with PPIs, which directly target H�-K�-ATPase as the final target of all parietal cell stimuli (384).For example, a meta-analysis concluded that patientstreated for bleeding peptic ulcers are about twice as likely tosuffer from persistent or recurrent bleeding if treated withH2 antagonists compared with PPIs (384). Another meta-analysis also demonstrated a higher efficacy of PPIs in treat-ing esophagitis (83% healing rate with PPIs compared with52% with H2 antagonists)(567). Today, H2 antagonists arelargely superseded by PPIs due to their higher clinical effi-cacy. Furthermore, with the exception of famotidine, H2
antagonists are extensively metabolized in the liver by theCYP-450 system, leading to substantial drug-drug interac-tion profile (for review, see Ref. 506).
3. Antacids
Antacids directly neutralize gastric acid allowing immediateshort-term control of heartburn. They exist in various saltformulations, the most common of which are carbonatesalts, such as CaCO3, MgCO3, or NaHCO3. The use ofcalcium carbonate as a dietary calcium supplement is dis-
SASCHA KOPIC AND JOHN P. GEIBEL
202 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

cussed in a separate section (see sect. VC). Although eachformulation possesses its own spectrum of side effects, anotable condition in the context of this review is the milk-alkali syndrome, which is the result of a concomitant over-ingestion of calcium and alkali, such as CaCO3. Althoughthe syndrome became less prevalent with the introductionof modern ulcer therapies, it still poses a significant risk forpatients that may ingest CaCO3 as a calcium supplementfor the prevention of osteoporosis or as an antacid on aregular basis. Milk-alkali syndrome presents with the triadof metabolic alkalosis (carbonate), hpercalcemia (calcium),and renal insufficiency. The above average ingestion of cal-cium leads to increased plasma calcium levels due to excessabsorption and impaired renal secretion. PTH levels are lowdue to negative feedback (6). Hypercalcemia further causesrenal vasoconstriction, which decreases the glomerular fil-tration rate, and renal fluid loss because of activation of theCaSR, which in turn has loop-diuretic-like effects (see sect.IVD3). The activation of the CaSR is further potentiated bythe metabolic alkalosis, which increases its sensitivity tocalcium. All abnormalities are usually reversible after with-drawal of the offending agent and adequate treatment.
III. INTESTINAL CALCIUM ABSORPTION
The intestine is responsible for the absorption of dietarycalcium into our systemic circulation. Although the kidneyalso plays a pivotal role in calcium homeostasis by retainingand balancing systemic calcium via regulating its excretioninto the urine, renal calcium handling will not be the subjectof this review.
Current recommendations suggest that an average 40-yr-old adult should ingest �1,000 mg of calcium on a dailybasis (218). In the United States, this requirement is mostlymet (57). Up to 72% of the dietary calcium intake is attrib-utable to dairy products (218). Typically, the intestine ab-sorbs between 25 and 35% of the ingested calcium (1193).This occurs via two distinct pathways: 1) a paracellularpathway and 2) a transcellular pathway.
Calcium absorption via the paracellular route is tied to adownhill concentration gradient between the luminal andthe extracellular compartment and occurs throughout theentire intestine (although solvent drag induced paracellularflux may also play a role at low luminal calcium concentra-tions; Refs. 266, 1071, 1098). Conversely, transcellular ab-sorption can also take place against an uphill gradient, butrequires molecular machinery in the form of distinct cal-cium transport proteins which are expressed on the apicaland basolateral membranes of the enterocyte. This processdirectly requires energy in the form of hydrolyzable ATPand is alternatively termed “active” transport (versus “pas-sive” paracellular transport). The proximal small intestine,i.e., the duodenum and the jejunum, is the main site fortranscellular calcium absorption (825).
Since a concentration gradient is not a prerequisite for thisprocess, transcellular transport allows us to absorb calciumeven when the calcium concentration in the chyme is fairlylow. The relative importance of each respective absorptionpathway thus alternates with the amount of ingested cal-cium (46, 824, 1224). The rate of paracellular calcium up-take is canonically thought to remain constant, while tran-scellular transport can be upregulated under conditions ofdietary calcium restriction (46, 824, 1224). This regulationoccurs via the active metabolite of vitamin D [1,25(OH)2-vitamin D], which serves as a stimulator for transcellularcalcium uptake to prevent systemic calcium depletion.
A. Transcellular Calcium Absorption
1. Calcium entry
Evidence for active transport of calcium across the intestinalepithelium was established very early. With the use of a cal-cium radioisotope, various groups demonstrated 1,25(OH)2-vitamin D-dependent calcium transport against an imposedconcentration gradient in the small intestine of the rat (952,954, 1150). It has also been observed that active transportcan be induced by a low-calcium diet, which we now knowto stimulate the production of 1,25(OH)2-vitamin D (1133,1134). The degree of transport was highest in the duode-num and decreased in the more distal segments (952). Theduodenum is still considered the primary site where the bulkof transcellular transport occurs. To conduct active transcel-lular calcium absorption, the enterocyte has to be equippedwith an apical calcium entry pathway, a mechanism for cyto-solic calcium shuttling, and a basolateral calcium exit pathway(FIGURE 3). As the cytosolic concentration of free calciumis kept at a constant low level with typical concentrationsof �100 nM, apical calcium influx follows its electro-chemical gradient into the cell. In contrast, the extrusionof calcium on the basolateral membrane against an uphillgradient either directly requires ATP or energy stored inthe sodium gradient.
A) THE SEARCH FOR THE APICAL CALCIUM ENTRY PATHWAY. The mo-lecular identity of the apical calcium entry pathway was un-clear for a long time. Early experiments in isolated duodenalbrush-border vesicles revealed that calcium uptake was pas-sive, saturable, sensitive to ruthenium red, 1,25(OH)2-vitaminD dependent, and functionally optimal at a pH of 7.5 (740).This black box characterization suggested that a “specificcarrier” was responsible for calcium absorption and in ret-rospect already provided us with accurate key characteris-tics of the transient receptor potential vanilloid channeltype 6 (TRPV6), which was later established as the primaryapical calcium uptake channel (740). In subsequent at-tempts to further unravel the nature of the calcium uptakemechanism, various voltage-gated L-type calcium channelblockers were used (474, 717, 838). Although isolated du-odenal cells accumulated less calcium following application
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
203Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

of the inhibitors and 1,25(OH)2-vitamin D stimulation(717), in vivo calcium entry proved to be fairly insensitive totheir effects (with the exception of verapamil, which dem-onstrated some degree of inhibition if applied at very highconcentration in the millimolar range) (474, 838). The con-flicting reports may be attributable to the different experi-mental models that were used, as isolated single cells do notallow discrimination between apical and basolateral trans-port mechanisms. Furthermore, it has been argued that L-type calcium channels may play a role in the stimulatorypathway of vitamin D, rather than in calcium uptake per se(717). In conclusion, an involvement of L-type calciumchannels seemed rather inconclusive and the identity of thecalcium entry channel remained elusive.
B) TRPV6. The cloning of the calcium transport protein sub-type 1 (CaT1) in 1999 finally marked a turning point in thesearch for the elusive intestinal calcium entry channels(838). The work was pioneered by Hoenderop and col-leagues who had identified the main calcium entry proteinin the kidney (epithelial calcium channel type 1, ECaC) viaan expression cloning strategy a few months earlier (474).
CaT1 was identified by a similar approach. A rat duodenalcDNA library was functionally screened using a calciumuptake assay in a Xenopus oocyte expression system (838).This screening process yielded the 727-amino acid proteinCaT1, which showed a 75% sequence homology to rabbitECaC. Homology analysis also demonstrated a relationshipto the vanilloid reptor type 1 (VR1), a nonspecific cationchannel that is activated by capsaicin, the pungent ingredi-ent in chili peppers, and mostly mediates pain signalingthrough afferent sensory neurons (838). The nomenclaturechanged over time as new channel proteins were identified,and today we consider CaT1, ECaC, and VR1 to be mem-bers of the same transient potential receptor vanilloid(TRPV) ion channel family. Literature now refers to ECaCas TRPV5, to CaT1 as TRPV6, and to VR1 as TRPV1.
The structure of TRPV6 was predicted to have six trans-membrane domains and four ankyrin repeat domains,which serve as cytoskeletal linking sites (838). Channel con-ductance was not dependent on other ions and was inhib-itable by a low extracellular pH (838). Calcium uptake wasreduced by as much as �70% at a pH of 5.5, which con-
PMCA
NCXTRPV6
Ca2+
Transcription
Enterocyte
Transcription
Ca2+Ca2+
Ca2+
Na+
Ca2+
Calbindin-D 9k
RXR VDR
D
D
D
D
VDR
FIGURE 3. Transcellular and paracellular calcium absorption in the intestine. The transcellular intestinalabsorption of calcium relies on apical calcium entry through TRPV6, intracellular calcium transport by calbin-din-D9k, and basolateral calcium extrusion via either NCX or PMCA. 1,25(OH)2-vitamin D regulates most ofthese ion transport proteins on a transcriptional level. 1,25(OH)2-vitamin D passes the plasma membrane ofthe enterocyte and binds to its receptor (VDR), which then heterodimerizes with RXR to initiate transcription.Evidence also suggests that 1,25(OH)2-vitamin D regulates the permeability of tight junctions, which gate theparacellular absorption of calcium. D, 1,25(OH)2-vitamin D.
SASCHA KOPIC AND JOHN P. GEIBEL
204 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

firmed the early black box data observations made in intes-tinal brush-border vesicles (838). This behavior seemedcounterintuitive to the investigators, as TRPV6 expressionwas highest in the duodenum, which is exposed to an acidload from the stomach (838). Duodenal pH has been re-ported to be as low as �6.1–6.6 but is even lower acutelyafter gastric emptying (�5.4), which would entail signifi-cant inhibition of TRPV6-mediated calcium uptake (284,290, 838). Conductance was also modestly sensitive (10–15% inhibition) to L-type calcium channel blockers at highconcentrations, which partially clarified the preceding am-biguous observations made by other groups with these in-hibitors (318, 337, 717, 838).
Subsequently, the human analog of rat TRPV6 was cloned(it had 97% sequence homology and was rather confusinglynamed ECaC2), and its expression was confirmed in humanduodenum (64). The generation of a TRPV6 antibody al-lowed for first localization studies, which confirmed an api-cal localization of TRPV6 and thus reaffirmed its role as theprimary apical calcium entry pathway in the intestine(1220). Tissue expression of TRPV6 varies among species(461). In humans, TRPV6 was identified in the duodenum,jejunum, stomach, esophagus, kidney, placenta, mammarygland, pancreas, prostate, testis, and salivary gland, but wasalso found to be upregulated in a series of malignancies,including prostate, breast, colon, and ovarian cancer (461,792, 836, 839, 1168, 1220). The role of TRPV6 in thesetissues mostly remains to be elucidated.
TRPV6 displays some unique biophysical properties. Asmentioned earlier, TRPV6 consists of six transmembranesegments, like many voltage-gated cation channels. Unlikethese channels, TRPV6 lacks the voltage sensor domain inthe fourth �-helix and is in a constitutively open state atresting membrane potential. Analysis of the quarternystructure shows that it assembles in tetramers (476). Theankyrin domains were implicated to be responsible for te-tramer formation; however, more recent structural data ob-tained by crystallography question this hypothesis (311,848). It is thought that heterotetramers can also be formedwith subunits of closely related TRPV5 (476). In contrast tomost other members of the TRP channel family, TRPV6 is avery selective channel for calcium (475, 1058, 1197). Therelative permeability of TRPV6 for calcium over sodium(PCa/PNa) is �100, whereas TRPV1, for example, has aselectivity of PCa/PNa �10 (although this has recently beenshown to be variable) (206, 475, 1197). This high selectiv-ity is crucial for the maintenance of a constant membranepotential in the enterocyte during calcium absorption.TRPV6 is strongly inward rectifying, which has been attrib-uted to magnesium ions plugging the channel pore for out-ward ion movement during states of depolarization (1126).Magnesium also exerts a voltage-independent inhibitory ef-fect on TRPV6 current; however, the mechanism underly-ing this observation is unclear (475, 1126). Furthermore,
TRPV6 gating is sensitive to intracellular calcium. Increasesin calcium were shown to inhibit the channel, resembling anegative-feedback mechanism (475). Although global cal-cium concentrations in the cell largely remain constant, thechannel microenvironment is exposed to fluctuations in lo-cal calcium. This feedback loop may be important for finelytuning the amount of calcium influx and preventing calciumoverload of the enterocyte. The putative mechanism of thisregulation will be discussed later in this section.
In 2001 it was demonstrated that ATP modulates TRPV6activity by preventing channel rundown (475). Recent workby Al-Ansary et al. (15) suggests that ATP directly binds tothe channel, thereby inhibiting inactivation by locking thechannel in the open conformation. Binding of ATP may beantagonized by channel phosphorylation through PKC(15). In conclusion, TRPV6 is precisely regulated by its ownmicroenvironment. Calcium, magnesium, and protons havean inhibitory effect on the channel, whereas ATP preventschannel inactivation.
It is important to remember that apart from being a nutri-ent, calcium is a crucial intracellular messaging molecule.Therefore, the enterocyte has to tightly control its intracel-lular concentration and adapt uptake to energy status andbasolateral extrusion. To ensure this delicate intracellularhomeostasis, TRPV6 is associated with and regulated by avariety of auxiliary proteins. The first protein that has beenidentified to interact with TRPV6 was the S100A10-an-nexin2 complex (1112). The S100A10-annexin2 complexhas been implicated to play a role in protein trafficking andmembrane anchoring. Its association with TRPV6 is essen-tial for channel trafficking to occur, as a disruption of theinteraction leads to cytosolic scattering of the channel(1112). Formation of the S100A10-annexin2 complex andits association with TRPV6 involves activation of PKA andcalcineurinA (CnA) (117). Another protein that is requiredfor TRPV6 membrane insertion is rab11a (1111). In anal-ogy to S100A10-annexin2, perturbation of rab11a bindingresults in decreased surface expression of TRPV6 and chan-nel retention in the cytosol (1111). Furthermore, the proteinkinases SGK1 and WNK3 are known to promote mem-brane insertion of TRPV6; however, their exact site of ac-tion is still unclear (114, 1031). Once trafficked to the mem-brane, physical channel stability is maintained by a varietyof auxiliary proteins. The COOH-terminal tail of TRPV6contains a PDZ protein binding motif. PDZ proteins serveas membrane anchors and protein scaffolds and mediate theassembly of multiprotein complexes, thereby regulatingchannel activity. The PDZ protein sodium hydrogen ex-changer regulating factor (NHERF4) (aka PDZK2) has re-cently been identified to interact with TRPV6 (574, 1113).It has been speculated that NHERF4 serves as a scaffold forTRPV6 at the apical pole, which is underlined by the obser-vation that knockdown of NHERF4 by RNAi leads to de-creased TRPV6 current in HEK293 cells (574, 1113). Apart
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
205Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

from trafficking to the apical membrane, channel numbercan be regulated by internalization and degradation. Onepossibility of decreasing functional channels at the cell sur-face is protein ubiquitination. The process of ubiquitinationinvolves enzymatic tagging of target proteins, thus directingthem to the proteasome or lysosome for rapid degradation.The degradation tag is transferred to the target protein byE3 ubiquitin protein ligases, such as Nedd4–2. It is alreadywell understood how Nedd4–2-mediated ubiquitinationcan decrease the number, but also directly modulate theactivity, of the epithelial sodium channel (ENaC) in thekidney (825). A recent study demonstrated that a similarmechanism applies to TRPV6 (1212). Coexpression ofNedd4–2 and TRPV6 in oocytes resulted in decreased cal-cium flux and channel numbers (1212). Nedd4–2-mediatedTRPV6 ubiquitination could thus serve as a mechanism ofrapidly regulating channel retrieval from the plasma mem-brane (1212).
Several other proteins have been identified to associate withTRPV6 that do not affect channel numbers, but rather di-rectly regulate channel activity. The nisnap1 gene was iden-tified in the late 1990s; however, its function remained elu-sive (992). Recently, TRPV6 was shown to interact withnisnap1 (971). It is expressed in the intestine, but not thekidney, which is unusual as TRPV6 and TRPV5 are gener-ally regulated by similar auxiliary proteins. Electrophysio-logical measurements showed that nisnap1 inhibits TRPV6without affecting its surface expression (971). Very similarfunctional properties were attributed to RGS2, a proteinthat is mainly known to alter the GTPase activity of Gproteins. In analogy to nisnap1, RGS2 can inhibit TRPV6at the plasma membrane without affecting its traffickingdynamics (970).
As previously discussed, the activity of TRPV6 is finelyregulated by intracellular calcium concentrations. Eleva-tions in intracellular calcium levels exert an autoinhibi-tory effect on channel opening (475). Shortly after theidentification of TRPV6, calmodulin (CaM) was shownto bind to the channel in a calcium-dependent manner,and it was speculated that it mediates the calcium feed-back response (461, 791). Subsequent investigations dem-onstrated that CaM may indeed represent the molecularcalcium sensor (263, 619). Elegant FRET studies reportedthat CaM dynamically associates with TRPV6 in the pres-ence of calcium and that this association is terminated whenintracellular calcium is depleted (263). The association be-tween TRPV6 and CaM also correlates with decreased cur-rent flux through the channel (263). Although the ankyrinrepeat domains of the channel were thought to possiblyserve as binding sites for CaM, more recent structural in-sights provide rebutting evidence for this hypothesis (848).Instead, the COOH-terminal tail of TRPV6 has been sug-gested as the site where CaM binding occurs (263, 619,791). Hence, CaM can tune ion flux through TRPV6 and
most likely mediates the channel’s sensitivity to intracellu-lar calcium.
Phosphorylation by kinases and dephosphorylation byphosphatases represent a common cellular strategy for rap-idly modulating channel gating properties. The non-recep-tor tyrosine kinase Src has emerged as a candidate for thedirect phosphorylation of TRPV6, thereby increasing chan-nel conductance (1042). Src was previously shown to mod-ulate TRPV4 activity (1178). The effects of Src are antago-nized by the phosphatase PTP1B. Both enzymes act on thetyrosine residues Y161/162, which are located in the NH2-terminal tail of the channel (1041).
An interesting interaction without direct relevance for theintestine has been reported between renal TRPV5 andklotho (170). Klotho is a �-glucuronidase with a transmem-brane anchor that can be cleaved, resulting in shedding ofthe enzymatically active domain of the protein into theurine (170, 612). Klotho can then increase TRPV5-medi-ated calcium uptake by hydrolyzing N-linked oligosaccha-rides on extracellular channel domains, thereby preventingchannel retrieval from the plasma membrane (170). Al-though a recent report indicates that klotho can also affectTRPV6 activity in vitro, it is not expressed in the intestineand thus may only interact with renal TRPV6 (612, 683).Although this finding has no implications for intestinal cal-cium uptake, various bacteria and neutrophils produce�-glucuronidase, which may affect TRPV6 activity in theintestine (359, 1004).
Recently, Stumpf et al. (1046) described an association be-tween cyclophilin B (CyB) and TRPV6 in the placenta. Co-expression of both proteins in oocytes increased calciumuptake (1046). CyB was also detected by Western blot anal-ysis in the small intestine and colon; however, colocaliza-tion and functional studies in intestinal tissue remain to beperformed (1046).
C) THE TRPV6 KNOCKOUT CONUNDRUM. As will be discussed inmore detail later, 1,25(OH)2-vitamin D is one of the keyhormonal regulators of systemic calcium homeostasis (seesect. IVA). Increased levels of 1,25(OH)2-vitamin D lead toenhanced intestinal calcium absorption. Shortly after clon-ing of TRPV6, it was recognized that the channel is posi-tively regulated at the mRNA level by 1,25(OH)2-vitamin D(614, 1030, 1109, 1110). The TRPV6 promoter has mul-tiple binding sites for the 1,25(OH)2-vitamin D receptor(VDR) and is thus directly sensitive to increases in1,25(OH)2-vitamin D levels (736). Consequently, VDR-de-ficient animals display a marked decrease in TRPV6 mRNAlevels, whereas administration of 1,25(OH)2-vitamin D inwild-type animals results in an increase in mRNA transcrip-tion (1030, 1109, 1110). In conjunction with the rapidly ex-panding characterization of the channel itself, these observa-tions supported the dogma that TRPV6 is the essential player
SASCHA KOPIC AND JOHN P. GEIBEL
206 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

in transcellular calcium uptake and that this pathway isstrongly regulated by 1,25(OH)2-vitamin D.
With the introduction of novel genetic techniques, a TRPV6(�/�) mouse was created in 2007 by Bianco et al. (94). Theanimals presented with decreased intestinal calcium uptake,as measured by serum concentrations of a calcium radioiso-tope following gavage, decreased femoral bone density(9.3%) and increased 1,25(OH)2-vitamin D levels, as a re-sult of feedback regulation (94). These findings were inaccordance with the postulated role of TRPV6 as the pri-mary 1,25(OH)2-vitamin D-sensitive calcium uptake mech-anism in the intestine. However, the generation of anotherTRPV6 (�/�) animal line by Benn et al. (76) a year laterspawned a controversy in the field. In these animals, base-line calcium uptake was identical between wild-type and(�/�) groups. Surprisingly, calcium uptake could be in-creased in the (�/�) group by a low calcium diet and, moreimportantly, by 1,25(OH)2-vitamin D (an observation thatwas also confirmed by another group; Ref. 615) (76). Thesefindings profoundly questioned the role of TRPV6 in cal-cium absorption and suggested that a different moleculartarget of 1,25(OH)2-vitamin D mediates the increase in cal-cium uptake after exposure. All these observations were insharp contrast to the initial report by Bianco et al. (94).However, Benn et al. (76) also reported that compared withwild-type animals calcium uptake was reduced in TRPV6-deficient animals that were fed a low-calcium diet. Thissuggests that the animals may not be able to adequatelyincrease absorption, when confronted with a low dietaryavailability of calcium, which in turn suggests a role ofTRPV6 during states of dietary calcium insufficiency.
These controversial findings allow several conclusions andspeculations. 1) As with any model of targeted gene disrup-tion, a compensatory mechanism may be in place thatmasks and distorts the physiological importance of TRPV6.The animals may upregulate other, yet unidentified, cal-cium transport mechanisms to compensate for the loss ofTRPV6 function. 2) Rather than being a constitutivelyactive pathway, transcellular calcium absorption throughTRPV6 only occurs in states of low dietary calcium intake.This hypothesis has been put forward very early and has beenreaffirmed by a recent study that observed an increase in boneturnover in TRPV6 (�/�) animals on a low-calcium diet(46, 666, 824, 1224). Mobilization of bone calcium may benecessary in these animals to maintain systemic calciumconcentrations, which are double challenged by the lack ofTRPV6 and the insufficient calcium intake (666). Further-more, it has been extensively described that a low-calciumdiet induces gene expression of TRPV6 [presumablythrough an increase in 1,25(OH)2-vitamin D levels], sug-gesting a role of the channel during states of insufficientdietary calcium supply (76, 132, 639). 3) 1,25(OH)2-vita-min D may have many more targets in the intestinal mucosathan previously anticipated and may also regulate calcium
uptake through the paracellular pathway (76, 615). In con-clusion, the generation of TRPV6 (�/�) animals has sus-tainably challenged our model of transcellular calcium ab-sorption by questioning the relative importance of TRPV6and by introducing new potential targets of 1,25(OH)2-vitamin D regulation.
D) GENETIC POLYMORPHISMS OF TRPV6. Single nucleotide poly-morphisms (SNPs) are variations in the genomic sequencethat occur in one single base. If the frequency of a SNP or aspecific set of SNPs (haplotype) increases in a populationover time compared with other SNPs, it can be concludedthat this set of SNPs is associated with an evolutionaryadvantage, meaning that this gene locus was under selec-tion. Recent reports from various groups indicate thatTRPV6 was subjected to strong selection (12, 502, 1023,1050). Traces for selection can be found in any non-Africanpopulation (12, 502, 1023). The selective event in Euro-peans has presumably occurred �7,000 years ago andcoincides with the development of agriculture (502). Thiscorrelation also holds true for other populations (502). Ithas been speculated that a change in diet or resistance toemerging disease led to selection and fixation of the nowconserved haplotype (502). Interestingly, selection tookplace in parallel in many populations, pointing towards astrong selective stress that developed independently ineach region (502).
The electrophysiological properties of ancestral and derivedTRPV6 were investigated by two groups (502, 1050).Hughes et al. (502) observed no statistically significant di-vergence in channel behavior. The derived channel onlydisplayed a tendency towards decreased sensitivity to theautoinhibition by calcium, albeit not significant (P ��0.094) (502). The authors speculated that differences inprotein-protein interactions may have led to selection(502). Conversely, Sudo et al. (1050) reported increasedcalcium influx through the derived channel, which may con-stitute an evolutionary advantage by facilitating dietary cal-cium uptake. Regardless of the controversial functionaldata, these insights indirectly underline the importance ofTRPV6 and provide a counterweight to the conclusionsdrawn from the TRPV6 (�/�) animal model. It is unques-tionable that TRPV6 was under parallel independent selec-tion in many regions across the planet. This provokes thequestion of how strong selection can occur for a derivedchannel whose physiological difference to the ancestralform seems to be very subtle, yet complete disruption of thechannel in the mouse model only causes a very mild pheno-type. This inconsistency adequately exemplifies the caveatthat underlies the conclusions drawn from (�/�) animalsand reminds us of the fact that we are far from understand-ing the exact physiology of transcellular calcium uptake.
E) CAV1.3. TRPV6 may not be the only channel mediatingapical calcium absorption in the intestine. A recent investi-
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
207Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

gation provides another explanation for the initially ob-served partial sensitivity of transcellular calcium uptake toL-type calcium channel blockers. The voltage-gated cal-cium channel Cav1.3, a member of the L-type calcium chan-nel family, was recently identified in the apical membranesof the distal jejunum and proximal ileum (751). Previousobservations were emulated, as the investigators again dem-onstrated a decrease in calcium absorption following appli-cation of L-type calcium channel inhibitors in the corre-sponding segments (751). The authors argued that uptakethrough Cav1.3 may have previously been misinterpreted asparacellular calcium uptake (751). However, it should benoted that the calcium uptake assay used in this report didnot discriminate between transcellular and paracellular cal-cium movement. Subsequently, it has been observed thatL-type inhibitor-sensitive calcium flux is linked to stimula-tion of glucose uptake through the glucose transporter type2 (GLUT2) (692, 750). Cav1.3 may serve as an alternativecalcium entry pathway that is active in states of luminalcalcium abundance and that coregulates glucose absorption(692, 750). Further investigations will be needed to deter-mine the contribution of Cav1.3 to dietary calcium absorp-tion.
2. Calbindin-D 9k
The following section will address the question of whathappens to dietary calcium after it enters the enterocyte. Itshould be considered that transcellular calcium uptake andcytosolic calcium homeostasis are two contradicting re-quirements for the enterocyte. A prominent transcellularflux of free calcium will inevitably interfere with housekeep-ing functions of the cell, such as intracellular signaling.Furthermore, it has been calculated from in vivo data that ifcalcium were to diffuse freely (simple diffusion) through thecytosol, uptake rates would only be 1/70th of the actuallymeasured values (129). Simple diffusion would constitute abottleneck in the process of transcellular calcium absorp-tion if cytosolic calcium concentrations should be kept low.A partial solution to this problem was found as earlyas 1966, when Wasserman et al. (1151) identified a1,25(OH)2-vitamin D-inducible calcium binding protein inthe chick intestine. The authors observed that calcium ra-dioisotopes traveled faster across a cellophane membrane ifsuspended in intestinal homogenates from rachitic, i.e.,1,25(OH)2-vitamin D deficient, chicks than if suspended inthe homogenates from rachitic animals treated with1,25(OH)2-vitamin D (1151). This indicated that calciumwas bound to a protein in the enterocyte and that expres-sion of this protein was controlled by 1,25(OH)2-vitamin D(1151, 1152). Subsequently, the calcium binding proteinwas further characterized (1073, 1149, 1152). Expressionlevels were shown to be highest in the duodenum and togradually decrease in more distal segments, which corre-lated with the degree of calcium uptake that has been at-tributed to each intestinal segment respectively in priorfunctional investigations (1073). The mammalian isoform,
which had a lower molecular mass of �9 kDa (hence thename calbindin-D 9k), compared with the 28 kDa of theavian isoform, was later identified (138, 280, 283, 358).Concerning the functional role of calbindin-D 9k, it hadalready been speculated very early after its discovery that itmay serve as a calcium shuttling protein (951). Indeed, ini-tial calculations and later very basic experimental data con-firmed that calbindin-D 9k may mediate facilitated diffu-sion of calcium between the two poles of the enterocyte, inanalogy to the transport of oxygen by myoglobin in themuscle (321, 602). In a very fundamental investigation,calcium flux was measured between chambers that wereseparated by dialysis membranes. A 51% increase in trans-chamber calcium flux occurred in the presence of calbin-din-D 9k (321). However, it is hard to relate this number tophysiological values, given the simplification underlying theexperimental model. It has subsequently been calculatedthat calbindin-D 9k may facilitate diffusion of calcium by afactor of up to �60 (129). Rather than envisioning calbin-din-D 9k as a protein that individually shuttles calcium ionsacross the cell, one should imagine calbindin-D 9k as acalcium gradient amplifier (129, 602). As the intracellularconcentration of free calcium is in the nanomolar range, theintracellular gradient of free calcium between the apical andbasolateral pole can also only be in the nanomolar range.Diffusional flux, however, directly correlates with the con-centration gradient and can in consequence only be verysmall. Calbindin-D 9k is expressed in the enterocyte in themicromolar range and dynamically binds and releases cal-cium (714). Since the association between calbindin-D 9kand calcium is dynamic, the local concentration of calbin-din-D 9k-bound calcium will directly correlate with theconcentration of free calcium. It is thus the concentrationgradient of calbindin-D 9k-bound calcium throughout thecell that determines the flux rate of calcium. As this gradientcan be in the micromolar range, calbindin-D 9k serves as acalcium gradient amplifier (129, 602). It should be notedthat the real experimental data on calbindin-D 9k are fairlyscarce and that the bulk of scientific effort has gone intomathematical modeling of facilitated diffusion and calciumbinding kinetics (129, 321, 322, 602, 1021).
Functionally, several correlations between calbindin-D 9kand calcium uptake were identified. The calbindin-D 9kcontent of each intestinal segment correlates linearly withits ability for calcium uptake (129, 824, 1021). Althoughthis relation holds true on the experimental and the math-ematical modeling level, it does not prove causality (129,824, 1021). Furthermore, 1,25(OH)2-vitamin D and a low-calcium diet induce calbindin-D 9k on both the mRNA andprotein level, suggesting that it is involved in the process ofregulated calcium absorption (289, 604). In accordancewith these findings, VDR-deficient animals have a de-creased calbindin-D 9k mRNA content that cannot be res-cued by exogenous 1,25(OH)2-vitamin D administration(663, 1194). Although a 1,25(OH)2-vitamin D responsive
SASCHA KOPIC AND JOHN P. GEIBEL
208 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

element (VDRE) had been identified in the 5=-flanking re-gion of the calbindin-D 9k gene, later mutational analysisdemonstrated that this site was not essential for transcrip-tional regulation of calbindin-D 9k by 1,25(OH)2-vitaminD (217, 240). Hence, it is not clear how 1,25(OH)2-vitaminD exactly regulates calbindin-D 9k on a molecular level.Interestingly, intestinal calbindin-D 9k mRNA levels can berescued in VDR (�/�) animals by a high-calcium/phospho-rus/lactose diet, while extraintestinal calbindin-D 9kmRNA levels are unaffected (663). This suggests that, apartfrom endocrine regulation through 1,25(OH)2-vitamin D,intestinal calbindin-D 9k is also regulated by local factors(663). A direct short-term stimulatory effect of oral calciumintake on calbindin-D 9k levels had been observed before ina wild-type background (647). The mechanisms underlyingthe effect of diet on calbindin-D 9k levels are, however, stillobscure.
Despite the correlation between calbindin-D 9k levels and1,25(OH)2-vitamin D and the mathematical and experi-mental models, which support its role as a calcium shuttlingprotein, no clear evidence for the involvement of calbin-din-D 9k in transcellular calcium absorption existed. Thishad sparked controversy among investigators. In fact, avery early study concluded that although 1,25(OH)2-vita-min D induced both calbindin-D 9k and calcium absorp-tion, a discrepancy existed in the time course of both effects(424). Later, synthetic 1,25(OH)2-vitamin D derivatives,designed for a maximized effect on cell differentiation andsuppressed calciotropic activity, failed to increase serumcalcium levels while causing a sevenfold increase in calbin-din-D 9k mRNA [native 1,25(OH)2-vitamin D increasesboth serum calcium and calbindin-D 9k mRNA](604). In2006, a calbindin-D 9k (�/�) mouse was created by Kutu-zova et al. (613). The animals presented with no apparentphenotype abnormalities and had normal serum calciumconcentrations (613). Subsequent analysis of these animalsshowed that they responded equally well to 1,25(OH)2-vitamin D with regard to calcium absorption as wild-typeanimals (13). Of note, calcium absorption was assessed bymeasuring serum calcium following gavage of a calciumradioisotope and did not discriminate between transcellularand paracellular absorption (13). A different group repli-cated the findings made in the calbindin-D 9k (�/�) mouseand also did not find any appreciable variation in pheno-type or serum calcium concentrations (639). However, theinvestigators observed that during preweaning, when bothcalcium demand and absorption are at their peak, geneexpression of TRPV6 and the basolateral calcium extruder,plasma membrane calcium ATPase isoform 1b (PMCA1b),were highly induced in the calbindin-D 9k (�/�) animals(128, 639). This has been interpreted as a compensatoryupregulation of calcium transport proteins to ensure suffi-cient uptake in a state of high metabolic demand for cal-cium (639). Subsequently, a TRPV6 and calbindin-D 9kdouble (�/�) animal was created. The mature animals
show no disturbances in calcium homeostasis, although,similarly to TRPV 6 (�/�) animals, they cannot increasecalcium uptake in response to a dietary calcium challenge tothe same extent as wild-type animals (76).
In light of the insights gained through knockout animals,the role of calbindin-D 9k remains somewhat unclear.Again, it is difficult to dissect the physiological function ofcalbindin-D 9k in these animal models, given the assump-tion that the organism will pursue compensation for the lossof a gene product. In conclusion, it is undisputed that cal-bindin-D 9k is regulated by 1,25(OH)2-vitamin D, that itcan bind calcium and that theoretical modeling and veryfundamental experimental models verify that it can facili-tate diffusion of calcium across the enterocyte. The (�/�)models suggest that animals can compensate for the loss ofcalbindin-D 9k and maintain normal calcium homeostasis(13, 76, 613, 639). Furthermore, TRPV6, calbindin-D 9kand double (�/�) animals can still increase their calciumuptake in response to 1,25(OH)2-vitamin D or a low-cal-cium diet, respectively, albeit not to the same extent aswild-type animals (13, 76, 615). One may conclude thatneither of these proteins is necessary for transcellular up-take; however, it seems more likely that 1,25(OH)2-vitaminD has more targets than previously postulated and thatcompensatory mechanisms are in place.
3. Basolateral calcium extrusion
Once calcium reaches the basolateral membrane, it is ex-truded into the extracellular space, which completes theprocess of intestinal absorption. As extracellular calciumconcentrations are higher than cytosolic concentrations,this process requires energy. Two proteins are responsiblefor this task. 1) The PMCA extrudes calcium at the directexpense of ATP, whereas 2) the sodium-calcium exchanger(NCX) utilizes the energy stored in the sodium gradient totransport calcium out of the cell (FIGURE 3). It is this baso-lateral exit process that requires energy during transcellularcalcium uptake and that allows us to absorb calcium againstan uphill gradient when dietary concentrations are low.
A) THE PLASMA MEMBRANE CALCIUM ATPASE. The plasma mem-brane calcium ATPase (PMCA) is a virtually ubiquitousprotein that is responsible for intracellular calcium homeo-stasis by pumping calcium into the extracellular milieu,thereby keeping intracellular concentrations low. Thepump belongs to the family of P-type primary ion transportATPases, which among others also includes gastric H�-K�-ATPase (see sect. IIA1). Four isoforms of the protein exist;however, variety is increased by splicing (562, 1043). ThePMCA1b splice variant is most predominant in the smallintestine and the duodenum in particular, which suggest aninvolvement of this isoform in the process of transcellularcalcium absorption (341, 492). Given the ubiquitous ex-pression of PMCA, a detailed review of its structure and
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
209Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

function will be omitted. For a current and detailed review,please refer to Reference 1043.
PMCA was first characterized in the 1960s in the membraneof erythrocytes (956). Very early experiments in basolateralmembranes isolated from enterocytes identified a calcium-dependent enzyme with phosphatase activity, which servedas first evidence for PMCA in the intestine (100, 742). Sub-sequent investigations in basolateral vesicles from rat intes-tine concluded that two distinct calcium transport mecha-nisms existed in their membranes: an ATP-dependent(PMCA) and a sodium-dependent (NCX) mechanism (382,457, 573). Furthermore, it was shown that inhibition ofcalmodulin halved the amount of ATP-dependent calciumtransport (573). Today, we know that PMCA is highly reg-ulated by CaM, which can increase both the affinity of thepump to calcium and its turnover speed by a factor of up to10 (526, 627, 628, 756).
Interestingly, it has also been suggested that calbindin-D 9kcan directly stimulate calcium transport via PMCA (1136,1137). In addition to intracellular proteins, PMCA is alsoquantitatively regulated by endocrine factors. 1,25(OH)2-vitamin D can increase both the PMCA mRNA and proteincontent in enterocytes (35, 36, 62, 146, 382, 489, 614, 823,1109; contested by Ref. 1138). The data on the effects of alow-calcium diet on PMCA transcription are more controver-sial, as one study suggests induction whereas two other studiesobserved reduced mRNA levels (146, 583, 639). Of note,these observations were made in different species (chick vs.mouse). The sensitivity of the tissue to 1,25(OH)2-vitamin D isalso reported to decrease with age, which may representanother confounding factor underlying these observations(35, 36). In conclusion, the transcriptional regulation ofPMCA1b by 1,25(OH)2-vitamin D and its decreasing ex-pression along the length of the small intestine correlatewell with the canonical model of transcellular calcium ab-sorption. It is challenging to investigate the functionalcontribution of PMCA1b in the process of calcium ab-sorption, given its role as a housekeeping protein.PMCA1 is crucial during development, which results inembryonic death if knocked out (814, 1198). Conversely,heterozygote (�/�) animals present with no apparentphenotype, albeit parameters linked to calcium homeo-stasis were not assessed (814).
B) THE NCX. Long before the molecular identities of PMCAand NCX were known, it had been observed that calciumuptake in the intestine was dependent on extracellular so-dium (713). The authors concluded that “a sodium, calcium-exchange diffusion carrier may exist at the basal membraneof the cell,” which proved to be a remarkably accurateprediction (713). As mentioned before, later investigationsdelineated between an ATP and a sodium-dependent trans-port of calcium on the basolateral enterocyte membrane(382, 457, 573).
For a recent review on the structure and function of NCX,please refer to Reference 687. In brief, NCX exists in threeisoforms (NCX1–3), which are expressed in a broad varietyof cell types (687). The function of NCX has mainly beeninvestigated in excitatory tissues, given its role as a high-capacity calcium extrusion mechanism following excita-tion. To transport calcium against its strong electrochemi-cal gradient, NCX has to utilize three sodium ions to ac-complish extrusion of one calcium ion (85, 460). NCX1 isthe predominant isoform in the small intestine, where it hasbeen detected on the mRNA and the protein levels (275,688). However, NCX had been postulated to play a moreimportant role during calcium absorption in the kidneythan in the enterocyte, hence not much data on intestinalNCX are available to us (473). Furthermore, genetic dis-ruption of NCX1 is embryonically lethal, which imposessome limitations on our experimental methodology (600).A more recent study provides some functional evidence forNCX in the intestine. By measuring intracellular calciumconcentrations with a fluorescent indicator dye, Dong et al.(275) demonstrated that calcium uptake in a sodium-freeenvironment (to run NCX in its reversed configuration) wassignificantly decreased when NCX was pharmacologicallyinhibited. Despite our knowledge that NCX exists in en-terocytes and that it can extrude calcium under experimen-tal conditions, it is difficult to assess its relative contributionto transcellular calcium absorption.
In addition, NCX is not subjected to regulation by 1,25(OH)2-vitamin D, which further contributes to the ambiguity con-cerning its importance in the process of calcium absorption.This has been observed very early, when exogenous admin-istration of 1,25(OH)2-vitamin D to vitamin D-deficientanimals did not increase sodium-dependent calcium trans-port, while doubling transport through PMCA (382). Fur-thermore, it was recently shown that a calcium-depleteddiet decreases duodenal NCX1 mRNA levels (583).
Of note, two members of the potassium-dependent sodiumcalcium exchanger (NCKX) family, namely, NCKX 3 and4, were also identified in the small intestine (658, 687, 688).However, further functional investigations will be neededto clarify their role.
B. Paracellular Calcium Absorption
If we plot the amount of duodenal calcium absorption as afunction of the luminal calcium concentration, we can ob-serve that the absorption curve is comprised of two distinctkinetic components: a saturable/exponential componentand a nonsaturable/linear component (824, 825, 1134).The saturable component represents transcellular calciumuptake through the enterocyte, as both the number of cal-cium transport proteins and their turnover rate is limited.The nonsaturable component reflects calcium uptakethrough the paracellular pathway. The saturable compo-
SASCHA KOPIC AND JOHN P. GEIBEL
210 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

nent is less pronounced in the jejunum and disappears com-pletely in the ileum, indicating that transcellular calciumabsorption is restricted to the proximal segments of theintestine, as discussed previously (825) [this has been con-tested more recently, when transcellular flux was also notedin the ileum (46)]. Compared with the transcellular path-way, the paracellular route has not received much scientificattention. It has been put forward that the rate of paracel-lular calcium absorption is constant across the length of theintestine and is neither sensitive to 1,25(OH)2-vitamin Dnor a low-calcium diet (824, 825, 1224). However, pro-vided that enough dietary calcium is available to saturatethe transcellular pathway, observations indicate that netcalcium absorption is highest in the ileum, which has beenattributed to the sojourn time, rather than alterations inparacellular permeability (290, 710). In the rat, the chymespends some 74% of its transit time in the ileum, whichallows for a long exchange period between lumen andplasma (290). The diffusion rate itself is fairly low and onlyamounts to 2% of the rate if calcium were to diffuse freelybetween intestinal lumen and plasma (290). This effect is aconsequence of the diffusion barrier that tight junctions,which act as functional gating molecules of the paracellularpathway, impose on calcium flux.
Epithelial tight junctions are adhesion points between twoneighboring cells that seal their intercellular space against alumen, thereby restricting ion and water movement be-tween the two compartments. As water cannot be directlytransported, its movement is tied to ion fluxes, which inturn are determined by their respective concentration gra-dients across the epithelium. Each epithelial cell expressesan annulus of tight junction proteins at the apical end of thelateral membrane. Tight junctions are protein complexesthat consist of a variety of intra- and transcellular proteins.A detailed review of their structure would exceed the scopeof this article (for a recent review, please refer to Ref. 999).Briefly, the composition of the involved proteins determinesthe pore size, ion selectivity, and thereby the relative leaki-ness of each tight junction and the whole epithelium ingeneral. Furthermore, tight junctions create a lateral diffu-sion barrier for membrane proteins and help to maintain thefunctional polarity of the epithelial cell. It is important torecognize that tight junctions are not static complexes, butcan be rather dynamically regulated (999). This allows theepithelium to change its ion and water permeability in re-sponse to various stimuli (999).
As discussed previously, the rate of the nonsaturablecomponent of calcium absorption is documented to befairly constant and insensitive to 1,25(OH)2-vitamin D,which indicated that 1,25(OH)2-vitamin D may have noeffect on paracellular transport (824, 825, 1224). How-ever, in the late 1990s, Chirayath et al. (201) postulatedthat 1,25(OH)2-vitamin D can increase paracellular cal-cium flux in confluent Caco-2 cell cultures, which form
an epithelia-like monolayer with tight junctions. Thisconclusion is based on the observations that 1,25(OH)2-vitamin D decreased the transepithelial electric resis-tance, which is often used as a measure of tight junctionpermeability, and induced bidirectional, i.e., also “serosal”to “mucosal,” calcium flux in the cultured monolayers(201). A more recent investigation further substantiatedthis hypothesis. It has been shown that 1,25(OH)2-vitaminD regulates the mRNA levels of some tight junction proteinsin rat duodenum, which may alter their gating characteris-tics (354, 614). For example, the mRNA levels of claudin-3,a protein that directly determines tight junction permeabil-ity, were decreased 2.2-fold following 1,25(OH)2-vitaminD administration (614). Conversely, claudin-2 and -12mRNA and protein levels were increased (354). Functionalobservations in Caco-2 monolayers further demonstratethat overexpression of claudin-2 and -12 increases electricalconductivity and facilitates paracellular calcium flux (354).All of these events are tied to a 1,25(OH)2-vitamin D-me-diated promotion of transcriptional events. However, it isknown that 1,25(OH)2-vitamin D can also exert short-termnongenomic effects (1122) (see sect. IVA6B). A recent inves-tigation presents evidence for augmented solvent-dragparacellular calcium flux after acute administration of1,25(OH)2-vitamin D (1098). Solvent-drag mediated fluxmay occur at low calcium concentrations in the absence ofa calcium gradient. In this model, calcium is draggedthrough the paracellular space by water flux that is fueledby the hyperosmolar milieu in the paracellular space (266,626). 1,25(OH)2-vitamin D was shown to induce this cal-cium flux in the presence of initially equimolar calciumconcentrations between the mucosal and serosal compart-ments (1098).
Over the last years, evidence for the regulation of the para-cellular pathway by 1,25(OH)2-vitamin D has slowly accu-mulated. It is apparent that the canonical dogma whichpostulates that 1,25(OH)2-vitamin D only targets the tran-scellular pathway has to be revisited. Still, more experimen-tal investigations will be needed to ultimately clarify theeffects of 1,25(OH)2-vitamin D on paracellular calciumtransport. Should tight junctions indeed be subjected to regu-lation by 1,25(OH)2-vitamin D, this mechanism may partiallyexplain the sensitivity of calcium uptake in TRPV6 and cal-bindin-D 9k (�/�) animals to 1,25(OH)2-vitamin D.
C. Alternative Models of TranscellularCalcium Absorption
Two alternative models of transcellular calcium absorptionhave been put forward. One suggests that calcium is trans-ported through the enterocyte by vesicles (vesicular trans-port model) rather than facilitated diffusion, and the otherpostulates that 1,25(OH)2-vitamin D can induce intestinal cal-cium absorption in a rapid, nongenomic fashion via a putative1,25(OH)2-vitamin D surface receptor (transcaltachia).
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
211Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

The assumption that calcium is transported through the cellin vesicles is corroborated by a handful of observations. Ithas been demonstrated that 1,25(OH)2-vitamin D treat-ment increased the number of supranuclear lysosomes inrachitic chicks, compared with nontreated animals (247). Itwas later shown that the calcium content of lysosomes canmore than double following treatment with 1,25(OH)2-vi-tamin D, suggesting that they may play a role in the processof transcellular calcium movement (780). Compared withthe cumulative evidence that is in accordance with our ca-nonical model of calcium absorption, the role of vesiculartransport of calcium is still fairly obscure.
The model of transcaltachia mainly relies on the observa-tion that 1,25(OH)2-vitamin D can exert effects that are tooacute to be attributable to transcriptional events. For exam-ple, intestinal calcium absorption was increased in chickswithin 14 min of 1,25(OH)2-vitamin D exposure, an onsetwhich is too rapid as to be of a genomic nature (785). Itshould be noted that rapid effects of 1,25(OH)2-vitamin Dhave also been suggested to influence the paracellular path-way (see above). Undoubtedly a careful evaluation of theroute of calcium flux, i.e., transcellular versus paracellular,is necessary. At least, isolated intestinal cells respond withincreased uptake of radiolabeled calcium to acute 1,25(OH)2-vitamin D exposure (568). It has been postulated that apartfrom the VDR, a membrane-bound 1,25(OH)2-vitamin D ex-posure receptor, the 1,25(OH)2-vitamin D-MARRS (mem-brane-associated, rapid response, steroid binding) protein, me-diates the acute effects of 1,25(OH)2-vitamin D (568, 779,785).
IV. REGULATION OFCALCIUM HOMEOSTASIS
Eucalcemia is maintained by the concerted effort of vitaminD, PTH, and, to a lesser extent, calcitonin. All three hor-mones can influence serum calcium concentrations by act-ing on the intestine, the kidney, or bone. 1,25(OH)2-vita-min D, the active vitamin D metabolite, primarily modu-lates the intestinal absorption of calcium and will thereforebe discussed in most detail (FIGURE 4). Apart from hor-monal regulators that influence the absorption, excretion,and deposition of calcium, our body needs a mechanismthat allows it to sense the current levels of plasma calcium.This task is fulfilled by the CaSR. It oversees the preciseregulation of the calcitropic hormones.
A. Vitamin D
As discussed previously, vitamin D is one of the key regu-lators of calcium homeostasis. Our body has two sourcesfor vitamin D, namely, a dietary source (vitamin D2�3) andan endogenous source that relies on ultraviolet (UV) lightcatalyzed synthesis in the skin (vitamin D3) (FIGURE 5).
Nomenclature in this case is fairly misleading, as vitamins areper definition substances that cannot be generated by our bodyand have to be ingested from an external source. The fact thatwe can synthesize vitamin D3 in our skin classifies the sub-stance as a prohormone rather than a vitamin. As we will see,our current nomenclature is a byproduct of the historic eventsleading to the discovery of vitamin D.
1. Historical perspective
From a historical perspective, the identification of vitaminD is closely intertwined with attempts to understand thepathophysiology of rickets. Rickets is characterized bychildhood skeletal deformities resulting from inadequateosteoid mineralization and calcification of cartilage due todecreased serum calcium levels during development. Theadult form equivalent of rickets is termed osteomalacia.With the onset of industrialization, rickets became a prev-alent problem in the 18th, 19th, and the beginning of the20th century. In fact, the disease was so widespread at thebeginning of the 20th century that an investigation con-ducted by the German pathologist Schmorl on 386 children,who had died before the age of 4 years, concluded that 90%of them had had rickets (968). Even in present times nutri-tional rickets still remains a major public health concern indeveloping countries (303, 757, 809). The seminal observa-tions that led to the identification of vitamin D were pro-vided by Mellanby in 1919 (733). He observed that dogpups who were fed a severely restricted diet consisting ofporridge or bread were consistently developing rickets(733). Development of rickets could be averted if their dietwas supplemented with cod liver oil, which we now knowto contain a high concentration of vitamin D (733). Mel-lanby (733) concluded that “rickets is a deficiency diseasewhich develops in consequence of the absence of some ac-cessory food factor or factors.” Vitamin A had been discov-ered shortly before, and it was subsequently speculated thatit may represent the factor promoting bone formation(733). This hypothesis was later rebutted by American bio-chemist McCollum who concluded that “a substance whichis distinct from fat-soluble [vitamin] A” must be responsiblefor preventing rickets (727). Furthermore, he stated that hisexperiments “demonstrate the existence of a fourth Vita-min [vitamin D] whose specific property [. . .] is to regulatethe metabolism of bones” (727). In parallel to the unravel-ing of the dietary component of rickets, scientists were in-dependently discovering the importance of sunlight for dis-ease prevention. The Polish pediatrician Raczynski was mostlikely the first to demonstrate evidence for this hypothesis ex-perimentally (881). He kept one dog pup in the shade while alittermate was kept in the sunlight. Both dogs were breastfedby their mother. After 6 wk, the bones of the dog that was keptin the shade contained 36% less calcium (881). These obser-vations were followed up by the German pediatrician Huld-schinsky, who healed rachitic children after exposing themintermittently for 2 months to the UV rays generated by amercury vapor quartz lamp (504). Hess and Unger (447) rep-
SASCHA KOPIC AND JOHN P. GEIBEL
212 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

licated these findings by using sunlight treatment. Hess (446)later summed up the impact of these revolutionary observa-tions, which now seem intuitive to us: “We have known that agrowing plant cannot thrive in the dark, but have failed torealize that the same laws apply to growing animals.”
It was later recognized that it was sufficient to irradiate thefood administered to animals rather than the whole animalto prevent development of or heal rickets. Thus initially“inert” dietary substances with no antirachitic propertiescould be activated by UV light (385, 448–450, 505, 1037).It was concluded that irradiation caused the conversion of abiological precursor to an active form and that the samemechanism was physiologically taking place in the skin.Initially, it was speculated that cholesterol may serve as this
pro-vitamin. It was Windaus and Hess (in collaborationwith Rosenheim) who were the first to uncover its exactmolecular identity. They stated: “We conclude from ourexperiments with complete certainty that ergosterol [. . .]represents the anti-rachitic provitamin (1166). In 1928,Windaus received the Nobel Prize in Chemistry for “theservices rendered through his research into the constitutionof the sterols and their connection with the vitamins.” Theirradiation product of ergosterol was later purified andnamed vitamin D2 (ergocalciferol) (43, 896, 1164, 1167).Although these findings solved the question as to how UVirradiation generates Vitamin D2 from ergosterol, which hasantirachitic properties if ingested, the molecular mechanismsunderlying the antirachitic effects of cutaneous sunlight expo-sure still remained obscure. Since ergosterol is an exclusive
Parathyroid glands
Bone
Intestine
Kidney
Stimulates PTH secretion
Increases renal calcium absorption
Stimulates 1,25(OH)2-D synthesis
Increases renalcalcium absorption
Increases bone resorption
Kidney
Stimulates 1,2
eases renal
Hypocalcemia
PTH
Increases intestinalcalcium absorption
1,25(OH)2-D
FIGURE 4. Endocrine regulation of serum calcium levels. Calcium homeostasis is mainly regulated by PTH and1,25(OH)2-vitamin D. Both hormones act at their respective target organs to increase serum calcium levels.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
213Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

component of yeast and fungal membranes, a different precur-sor substance had to exist in animal skin. Again, it wasWindaus and colleagues who identified 7-dehydrocholesterolas the provitamin in porcine skin, which is converted to vita-min D3 (cholecalciferol) under irradiation (1165). After thesediscoveries, industrially produced vitamin D has rapidly beenused in medical applications and as a food fortification. To-
day, the main portion of dietary vitamin D ingestion in theUnited States stems from fortified dairy products (150).
2. Intestinal vitamin D absorption
To exert its antirachitic effects, dietary vitamin D has to beabsorbed into our circulation. Early everted gut sack exper-
7-dehydrocholesterol
Previtamin D
Isomerization
ER:CYP2R1
Mitochondria: CYP27A1
Mitochondria: CYP27B1
Calcium
PTH
Intestinal uptake
Glomerularfiltration
Vitamin D
Vitamin D
Vitamin D
25(OH)-vitamin D
25(OH)-vitamin D
1,25(OH)2-vitamin D
DBP
UV-B (290-315nm)
1,25(OH)2-vitamin D
Megalin
Keratinocyte
Hepatocyte
25(OH)-vitamin D DBP
25(OH)-vitamin D DBP
Vitamin D
Dietary vitamin D
DBP
Target organs
Proximal tubule
FIGURE 5. Vitamin D metabolism. Vitamin D can either be synthesized in the skin or absorbed from our diet.It is then transported to the liver where it undergoes 25-hydroxylation by one of two hepatic enzymes (CYP27A1or CYP2R1). During transport through the circulation, vitamin D is bound to a carrier protein (DBP). The25(OH)-vitamin-D-DBP complex passes the glomerular filter and is scavenged from the primary urine by theapical megalin receptor of the proximal tubule. Here, 25(OH)-vitamin D is converted to the active vitamin Dmetabolite 1,25(OH)2-vitamin D. DBP, vitamin D binding protein.
SASCHA KOPIC AND JOHN P. GEIBEL
214 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

iments demonstrated that this process has linear, nonsatu-rable, and passive kinetics, suggesting that no specific car-rier mechanism for vitamin D is in place (484). These ob-servations were later replicated in in vivo models (483).Absorption is highest in the proximal and mid small intes-tine (484). Since vitamin D is fat soluble, its absorptionmechanism is similar to that of dietary lipids. In an aqueousmedia, vitamin D aggregates in micelle-like structures(735). Its absorption is aided by the secretion of bile acids,which is underscored by the observation that patients suf-fering from cholestasis can present with vitamin D defi-ciency and develop bone disease, such as osteomalacia orosteoporosis (245, 445, 563, 721, 894, 953, 1018, 1080).Apart from bile salts, formation of mixed micelles contain-ing monoglycerides and free fatty acids represents anotherfactor that aids in vitamin D absorption (884, 1082; con-tested by Ref. 483). These substances increase micelle size,which promotes the solubilization of vitamin D, therebyincreasing uptake (884). Clinically, pancreatic insuffi-ciency, causing an impairment of triglyceride breakdownthrough insufficient lipase secretion, leads to decreased vi-tamin D absorption (1080, 1127). This is a particular prob-lem in cystic fibrosis patients, who often develop pancreaticand concomitant vitamin D insufficiencies (33, 230, 625,678, 924).
Following uptake into the enterocyte, vitamin D is packedinto chylomicrons and secreted into the lymph (288, 953). Ithas been demonstrated that after intestinal administrationof radioactive labeled vitamin D3, up to 90% of the recov-ered radioactive tracer was associated with the chylomicronfraction of the collected intestinal lymph (288). Further-more, patients suffering from the autosomal recessive chy-lomicron retention disease (Anderson disease; OMIM246700), which causes impairment of chylomicron process-ing and secretion in the enterocyte, can present with insuf-ficient levels of fat-soluble vitamins, such as vitamins D andE (535). The chylomicron remnants, which include vitaminD, are then scavenged by the liver after the lymph has en-tered the circulation through the thoracic duct (287, 407).However, it has been demonstrated in vitro and in vivo inhepatectomized and normal rats that vitamin D can directlytransfer from chylomicrons to a vitamin D binding protein(DBP; see sect. IVA5) in the blood plasma (286, 288). It hastherefore been suggested that at least a fraction of hepaticvitamin D uptake is mediated through DBP rather thanchylomicrons (286; contested by Ref. 407). In the liver,vitamin D is then hydroxylated at its 25 position to25(OH)-vitamin D. The metabolism of vitamin D will bethe subject of a later section.
The intestinal absorption of 25(OH)-vitamin D has beeninvestigated by many groups, with the aim of optimizingvitamin D administration in a therapeutic context by by-passing the first metabolic step in the liver (219, 245, 287,445, 645, 721, 1018, 1019, 1127). In general, enteric up-
take of 25(OH)-vitamin D is more effective than that ofvitamin D, which is partially attributable to a comparablylower dependency on bile acid secretion (219, 245, 287,645, 1018, 1019). The observation that patients withcholestasis still absorb 25(OH)-vitamin D effectively,whereas vitamin D absorption is impaired, corroboratesthis hypothesis (1018). There is some controversy with re-gard to the transport of 25(OH)-vitamin D following itsabsorption (287, 701, 1019). It has been argued that it maybe transported predominantly in the protein fraction of thelymph (287), i.e., not in chylomicrons, or that it is directlyabsorbed into the portal blood (701, 1019).
3. Cutaneous vitamin D synthesis
Cutaneous synthesis is our second source of vitamin D.Cutaneous production depends on exposure to UVB (290–315 nm) light (FIGURE 5). The UVB photons convert 7-de-hydrocholesterol, which is located in the plasma membraneof keratinocytes, to previtamin D3 (1117–1120). This de-pendency on sunlight causes a seasonal variation in vitaminD3 production, with synthesis being low during the wintermonths when the radiation angle of the sun flattens (187,478, 538, 1035, 1156). In consequence, changes in latituderesult in similar variability in production. Further factorsthat decrease production include pigmentation of the skinand application of sunscreen (209, 723), whereas an in-crease in altitude promotes production (478). Followingconversion from 7-dehydrocholesterol, previtamin D3
isomerizes to vitamin D3 (479). The isomerization processis temperature dependent and fairly slow (479, 1117). It hasbeen calculated that the half-life for the formation of vita-min D3 is �2.5 h (1085). Interestingly, in vitro experimentsconducted in isotropic medium demonstrated that theisomerization rate was 10 times slower than in in vivo ex-periments (1085). This was later attributed to the fact thatamphiphatic interactions with phospholipids of the cellmembrane stabilize the previtamin D3 conformer whichthen isomerizes to vitamin D3 (1086). The cellular microen-vironment of the reaction thus greatly optimizes the isomer-ization to vitamin D3. After its synthesis, vitamin D3 isbound to DBP and carried though the bloodstream to itstarget organs. Observations made in patients indicate thatthe vitamin D3 plasma levels peak �2 days after sunlightexposure, which is due to the slow isomerization rate in theskin (7).
4. Vitamin D metabolism and its regulation
Irrespective of the source (endogenous or exogenous), vita-min D is metabolized in the liver to 25(OH)-vitamin D(FIGURE 5). Evidence for the existence of biologically activevitamin D metabolites emerged in the 1960s (686, 799).25(OH)-vitamin D was identified by means of injecting ratswith radiolabeled vitamin D and subsequent silicic acid col-umn chromatography of lipid extracts from serum and var-
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
215Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

ious tissues (686). Chromatography revealed the presenceof a vitamin D metabolite in serum, liver, bone, and feces inrats and in human serum (256, 686). Furthermore, it wasshown that the vitamin D metabolite was biologically activeby reverting rickets in diseased animals and by increasingintestinal calcium transport and bone metabolism (686,752). The metabolite was characterized as 25(OH)-vitaminD and subsequently successfully synthesized (111, 112). Itwas soon recognized that hepatectomized rats were not ef-fectively converting vitamin D to 25(OH)-vitamin D, sug-gesting that the liver was the main organ responsible for25-hydroxylation (864, 865). The ability of the liver tometabolize vitamin D was also confirmed in perfused liversand tissue homogenates (490). Historically, a long contro-versy existed with regard to the subcellular localization ofthe enzyme that hydroxylates vitamin D (25-hydroxylase)in the liver, as enzyme activity was observed in both mito-chondrial and microsomal fractions of liver homogenates(93, 102, 103, 258, 696, 1053). Extensive investigationsindicated that both the microsomal and mitochondrial 25-hydroxylase are members of the cytochrome P-450 family(102–104, 696, 835). Both fractions demonstrated distinctenzymatic kinetics. The mitochondrial enzyme was charac-terized as a low-affinity high-capacity enzyme, whereas themicrosomal fraction displayed high-affinity low-capacitycharacteristics (103, 104, 356, 696).
The mitochondrial 25-hydroxylase (CYP27A1) was firstpurified to homogeneity from rabbit liver mitochondria(235). It was demonstrated that this cytochrome P-450 wasnot specific to vitamin D and could also hydroxylate othersubstrates, most notably cholesterol (27-hydroxylation),which represents an important step in the formation of bileacids (235). In retrospect, CYP27A1 had been purified 4years earlier; however, only the 27-hydroxylation of cho-lesterol had been investigated and its effects on vitamin Dhad remained obscure (1162). Subsequently, the enzyme’scDNA was cloned from rabbit, rat, and human, and its dualrole in vitamin D and steroid conversion was confirmed (26,149, 1048, 1103). The full gene structure was identified afew years later (646). Although no crystal structure of theenzyme is available to us, a homology model based on otherCYP family members has been proposed (874). In the liver,CYP27A1 is expressed on the mRNA level in hepatocytes,endothelial, stellate, and Kupffer cells (1078). Furthermore,CYP27A1 expression was confirmed in a variety of othertissues, including duodenum, adrenal glands, kidney, lung,vascular endothelium, brain, retina, skin, muscle, and os-teoblasts; however, their potential contribution to vitaminD metabolism remains unclear (26, 51, 135, 184, 370, 383,508, 640, 898, 979). Interestingly, an extrahepatic conver-sion of vitamin D had been suggested previously to occur inthe kidney and the intestine (1097). Marked differences inCYP27A1 activity can be observed between males and fe-males. For example, CYP27A1 enzyme activity and mRNAexpression were demonstrated to be increased in female rats
(933, 1078). Higher expression in females was also con-firmed in biopsy samples from human subjects (370). Aregulation via sex hormones may underlie this phenome-non, as injection of estradiol was shown to induceCYP27A1 activity (933). Interestingly, seasonal variationsin expression were also observed, which may represent aconfounding factor for decreased 25(OH)-vitamin D levelsduring the winter months (370).
It should be noted that CYP27A1 can also hydroxylatevitamin D3 at other positions (402, 950). These includepositions 27 and 26; however, the ratio for 25-:27-:26-hydroxylation has been estimated to be only 100:15:3,which demonstrates that 25-hydroxylation of vitamin D3 isthe most essential reaction catalyzed by the enzyme (950).More importantly, CYP27A1 can also use its own product25(OH)-vitamin D as a substrate to further act as a 1�-hydroxylase and produce the hormonally active form ofvitamin D, namely, 1,25(OH)2-vitamin D (50, 51, 950). Aswill be discussed later, this reaction is normally catalyzed inthe kidney by another CYP family member (CYP27B1). Atthe moment, it is not clear what the physiological signifi-cance of 1�-hydroxylation by CYP27A1 is.
Mutations in CYP27A1 cause the autosomal recessive dis-order cerebrotendinous xanthomatosis (CTX; OMIM213700). The disease was first described in 1937 and ischaracterized by cholestanol deposits that are most promi-nent in tendons, especially the Achilles tendon, the brain,and the lung. Patients present with progressive neurologicdefects, atherosclerosis, and cataracts and commonly sufferfrom diarrhea. The inadequate bile acid synthesis was firstnoted in 1974 by Setoguchi et al. (993). Shortly after thecDNA of CYP27A1 was cloned, it was demonstrated thatmutations of this enzyme were responsible for CTX (148).In agreement with the dual role of CYP27A1, CTX patientsalso suffer from osteoporosis, low 25(OH)-vitamin D lev-els, and impaired intestinal calcium absorption (83, 320).Three CYP27A1 mutations that are known to cause CTXand still lead to protein expression were recreated in vitro,and enzymatic activity was assayed. Depending on the ex-pression system, these mutants showed lower or higher 25-hydroxylation activity than the wt enzyme, which led theauthors to questions the enzyme’s role in vitamin D metab-olism (403). It should be considered that 1) many more(�38) mutations underlying CTX exist, 2) by far not allpatients exhibit disturbances in bone or vitamin D homeo-stasis, and 3) the investigated mutant enzymes may onlycause disturbances in cholesterol, rather than vitamin Dmetabolism (83, 320, 403). In the light of these limitations,it should be questioned whether CTX represents an aptmodel system to evaluate CYP27A1 in the context of vita-min D metabolism.
With the introduction of novel genetic tools, a cyp27a1(�/�) mouse was created in 1998 (918). However, the phe-
SASCHA KOPIC AND JOHN P. GEIBEL
216 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

notype of CTX could not be reproduced, albeit fecal bileacid content was markedly decreased (918). Rather surpris-ingly, serum 25(OH)-vitamin D levels were increased in(�/�) animals, which either pointed to compensatory up-regulation of other, maybe microsomal, enzymes or a non-involvement of cyp27a1 in vitamin D metabolism in themouse (918). The (�/�) mouse model was later character-ized in more detail, but no new conclusions with regard tovitamin D were drawn (902).
Another caveat that needs to be considered when assessingthe physiological importance of CYP27A1 for vitamin Dmetabolism is that the enzyme cannot 25-hydroxylate di-etary vitamin D2 (402). This observation underlines thenecessity for another 25-hydroxylase which physiologicallymetabolizes vitamin D2. The microsomal 25-hydroxylasewas a clear candidate for this process; however, it has onlyrecently received more extensive scientific attention.
The molecular identity of the microsomal 25-hydroxylasewas unclear, until it was unmasked by Cheng et al. (184) in2003 as CYP2R1. CYP2R1 is expressed on the mRNA levelin a plethora of tissues, but most prominently in the liverand testes (184). As illustrated by a recent investigation, thetestes may play a role in calcium homeostasis. Patients withtesticulopathy (and concomitant lower CYP2R1 expres-sion) were shown to have decreased 25(OH)-vitamin D lev-els and osteoporosis (333). The protein’s crystal structurehas recently been resolved in complex with vitamin D3
(1045). Unlike CYP27A1, CYP2R1 has been shown to 25-hydroxylate both vitamin D2 and vitamin D3, which may bea solution to the enigma of vitamin D2 metabolism (184).The physiological relevance of CYP2R1 was underscoredby the characterization of a patient who presented with low25(OH)-vitamin D levels and was shown to have a transi-tion mutation in the CYP2R1 gene (183). Furthermore, aremarkable large-scale study has recently tried to establish acorrelation between 25(OH)-vitamin D status and the ge-notype of 33,996 individuals. It was found that lower25(OH)-vitamin D levels correlated with variants in theCYP2R1 gene (1146) (a smaller study came to similar con-clusions, Ref. 139). This represents an outstanding finding,as the influence of CYP27A1 mutations on 25(OH)-vitaminD production is far less conclusive. Given the dispropor-tionate quantity of scientific data, it is at this moment dif-ficult to evaluate the relative contribution of each 25-hy-droxylase to vitamin D metabolism, but more and moreevidence for the importance of CYP2R1 is accumulating.
The regulation of 25-hydroxylation has been the subject ofcontroversy in the past, which is partially due to the factthat multiple enzymes may metabolize vitamin D, and thatit was challenging to experimentally discriminate betweenthese enzyme entities. Thus evidence which supports (91,92, 741, 1078) and questions (258, 1097) the existence of25-hydroxylase regulation can be found. A detailed analysis
of these observations is beyond the scope of this review, butthe most recent investigation should be considered in moredetail, given the advances in our experimental repertoire: ithas been demonstrated in the rat that 1,25(OH)2-vitamin Dcan downregulate hepatic CYP27A1 transcription with aconcomitant reduction in enzyme activity (1078). Theseobservations strongly corroborate the hypothesis that the25-hydroxylation step is subjected to negative-feedbackregulation. The exact mechanism of this regulatory mecha-nism remains elusive, especially since the CYP27A1 gene isnot under control of a VDRE (369, 988, 1078).
Following its synthesis, 25(OH)-vitamin D binds to DBPand is transported to the kidney, where it undergoes furtherconversion to 1,25(OH)2-vitamin D, the hormonally activeform of vitamin D (FIGURE 5). Historically, 1,25(OH)2-vitamin D was first identified in the nuclei of intestinal cellsas an uncharacterized vitamin D metabolite (429, 634). Thebiological activity of the metabolite was determined to bemuch higher than that of vitamin D, and it was eventuallyisolated and identified as 1,25(OH)2-vitamin D (480, 586,633, 800). 1,25(OH)2-vitamin D is up to 10 times morepotent than vitamin D. The importance of the kidney for thesynthesis of 1,25(OH)2-vitamin D was soon discovered, asnephrectomized rats were neither able to convert 25(OH)-vitamin D, nor absorb calcium effectively (339, 458).Briefly thereafter, patients with chronic renal insufficiencywere shown to lack the capability to metabolize 25(OH)-vitamin D, which further established the role of the kidneyas the major conversion site (724). The impairment of1,25(OH)2-vitamin D synthesis in the course of chronicrenal deficiency is a cofactor in the development of renalosteodystrophy, a bone mineralization deficiency due toderanged mineral balance. Of note, the kidney is not theexclusive site of CYP27B1 expression. 1�-Hydroxylase hasbeen detected in a variety of other tissues, including theplacenta, decidua, skin, brain, vascular endothelium, pan-creas, colon, but also in monocytes and dendritic cells (451–453, 603, 1204–1206). The role of extrarenal 1,25(OH)2-vitamin D synthesis is not entirely clear. Beyond modulatingcalcium homeostasis, vitamin D has been shown to have immu-nomodulatory and antiproliferative effects (see sect. IVA6).Given these observations, it has been speculated that extrare-nal local 1,25(OH)2-vitamin D production and paracrine se-cretion may represent important factors for the maintenanceof the “barrier function” in these tissues (451, 453).
In the kidney, 1�-hydroxylation of 25(OH)-vitamin Dtakes place in the inner mitochondrial membrane of theepithelial cells of the proximal tubule (393).
The cellular uptake mechanism of 25(OH)-vitamin D by thetubule cells will be subject of a later section. The 1�-hy-droxylase responsible for the conversion is also a member ofthe cytochrome P-450 family (CYP27B1) and was firstcloned in 1997 by St-Arnaud et al. from rat cDNA (1034).
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
217Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

The human homolog was cloned shortly thereafter (349,748). Interestingly, mapping of the CYP27B1 gene revealedthat the locus was identical to the gene locus of the auto-somal recessive disorder pseudo vitamin D deficiency rick-ets, type 1A (PDDR1A, OMIM 264700) (1034). PDDR ischaracterized by low serum calcium, secondary hyperpara-thyroidism, and low 1,25(OH)2-vitamin D levels (869) (ofnote, the original article wrongly suggests an autosomaldominant inheritance pattern). Patients can exhibit ricketsor osteomalacia due to increased mobilization of calcium.The gene locus of PDDR1A had been mapped by linkageanalysis; however, before the cloning of CYP27B1, it wasnot clear whether a defect in the enzyme itself or distur-bances in its regulation were responsible for the disease(617, 618, 1223). The clear-cut phenotype of PPDR1A ef-fectively illustrates the pivotal role of CYP27B1 and thelack of redundancy at this essential step of vitamin D me-tabolism. The characteristic features of PDDR1A can essen-tially be emulated if cyp27b1 is knocked out in a mousemodel (238, 822). The serum calcium levels and the second-ary hyperparathyroidism can be normalized if these animalsare fed a high-calcium, phosphorus, lactose diet, albeit bonegrowth remains impaired (239).
The activity of CYP27B1 is subjected to tight hormonalregulation. The key regulator of 1,25(OH)2-vitamin D syn-thesis is PTH, which is secreted by the parathyroid glands inresponse to low serum calcium concentrations in an effortto increase calcium uptake and release bone calcium intothe circulation. The regulation of calcium homeostasis bythe parathyroid glands and the CaSR will be covered insubsequent sections (see sect. IV, B and D). Apart from thisstimulatory input, CYP27B1 is under negative control by itsown product. 1,25(OH)2-vitamin D represses CYP27B1 ona transcriptional level (116, 125, 443, 591, 764). Althoughstudies in (�/�) animals suggest that the VDR is essentialfor autoinhibition to take place, the promoter region ofCYP27B1 does not include a canonical VDRE (125, 591,764). It is thus most likely that the transcriptional regu-lation through 1,25(OH)2-vitamin D is indirect (125,591). Alternatively, so-called E-box-type elements wererecently proposed to act as negative VDREs (575). More-over, CYP27B1 can be directly regulated by the localcalcium concentrations. High extracellular calcium inhib-its 1,25(OH)2-vitamin D synthesis, whereas low calciumconcentrations induce its production (109). It has been pro-posed that changes in calcium modulate VDR expressionand thereby the sensitivity of cell to the local negative feed-back by 1,25(OH)2-vitamin D (702). Some evidence sug-gests that the CaSR mediates the regulatory effects of cal-cium on CYP27B1 activity (FIGURE 8) (702). Other factorsthat regulate CYP27B1 activity include fibroblast growthfactor 23 (FGF23), calcitonin, prolactin, sex steroids (atleast in avian species), and phosphate (716, 913, 1067,1068, 1217).
Apart from regulating the synthesis of the vitamin Dmetabolites, our body also tightly controls their degrada-tion. The first step of vitamin D catabolism is 24-hy-droxylation, which is carried out by the mitochondrialenzyme CYP24A1. The primary site for vitamin D catab-olism is the kidney, but CYP24A1 is also strongly expressedin other extrarenal tissues, such as the intestine, osteoblasts,keratinocytes, prostate, placenta, brain, and heart (11, 181,796). CYP24A1 can hydroxylate both 25(OH)-vitamin Dand 1,25(OH)2-vitamin D, thereby creating 24,25(OH)2-vitamin D and 1,24,25(OH)3-vitamin D, respectively (14).24-Hydroxylation is followed by a series of oxidation/re-duction reactions which finally yield the excretable productcalcitroic acid (703, 893). At least in the proximal tubule ofthe kidney, the regulation of CYP24A1 is reciprocal to thatof CYP27B1. 1,25(OH)2-vitamin D upregulates CYP24A1,thereby stimulating its own breakdown, whereas PTH inhibitsCYP24A1 (37, 180, 812, 1069, 1222). While 1,25(OH)2-vi-tamin D increases the transcription of CYP24A1 (the gene hastwo upstream VDREs), PTH exerts its inhibitory effects bydecreasing CYP24A1 mRNA stability (1222). In osteoblasticand distal convoluted tubule cell lines, PTH has synergisticeffects with 1,25(OH)2-vitamin D in inducing CYP24A1 (37,1189). In analogy to CYP27B1, CYP24A1 is further regulatedby FGF23, calcitonin, and phosphate (361, 513, 1175).
5. Vitamin D transport and cellular uptake
The hypothesis that vitamin D may be bound to a carriersubstance in serum was first expressed in the late 1950s,when it was demonstrated that the alpha fraction of humanserum had high anti-rachitic properties (1079). It was latershown that DBP is identical to the group specific component(Gc) protein, which had been characterized independentlyby Hirschfeld and colleagues around the same time (236,464, 465). DBP (�58 kDa; 458 amino acids) is synthesizedin the liver and is closely related to albumin and �-fetopro-tein, which are all derived from the same ancestral gene(221, 875, 1158, 1187, 1188). The crystal structure of DBPhas been resolved at a resolution of 2.3 Å in complex with25(OH)-vitamin D (1121). DBP can bind vitamin D and allof its metabolites (408). There is, however, a difference inthe relative affinity for the vitamin D steroids, with theaffinity for 25(OH)-vitamin D being highest (Kd �10�8 M),followed by 1,25(OH)2-vitamin D and vitamin D (Kd
�10�7 M) (408). In humans, vitamin D2 and D3 metabo-lites are bound with equal affinity to DBP (406). Given itslong plasma half-life, 25(OH)-vitamin D is also measuredas the primary clinical parameter to assess the vitamin Dstatus of patients. Although the plasma concentration ofDBP is �4–8 �M, only �5% of the binding sites are occu-pied by vitamin D sterols (408, 409). DBP has a very fastturnover rate. It has been estimated that up to 28% of DBPare replaced every day (557). This turnover entails a highdemand for synthesis output by the liver. In consequence,patients with liver disease demonstrate lower DBP and totalvitamin D levels than healthy subjects (97, 409). This rela-
SASCHA KOPIC AND JOHN P. GEIBEL
218 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

tionship is reversed during pregnancy, when the levels ofDBP and vitamin D sterols are increased (97, 409, 609, 685,892). Of note, DBP is not the exclusive carrier substance forvitamin D sterols. Albumin and lipoproteins were shown totransport a fraction (�15%) of vitamin D (1015).
Given its multitude of functions, DBP has been regarded as anessential protein. Indeed, an analysis of over 80,000 humanserum samples showed that DBP was present in all of them,which led to the hypothesis that deleterious mutations ofDBP were lethal (213). Rather surprisingly, DBP (�/�)mice thrive well with growth curves identical to theirlittermates, although their 25(OH)-vitamin D and1,25(OH)2-vitamin D levels (total) are severely decreased(937). If challenged with a low vitamin D diet, the DBP(�/�) animals develop secondary hyperparathyroidism,leading to defects in bone mineralization (937). It is un-clear, however, to what extent albumin and lipoproteinscompensate for the loss of the primary vitamin D carriersubstance.
Not much is known about the cellular uptake of vitamin D.As all other steroids, free vitamin D can passively diffusethrough the plasma membrane because of its lipohilic na-ture. However, due to the high concentration of DBP and itsaffinity towards vitamin D ligands, only a fraction of vita-min D circulates in the free form. For example, 0.003% of25(OH)-vitamin D is transported as an unbound sterol inserum, which raises the question whether passive diffusionrepresents a sufficient uptake pathway (98). At least25(OH)-vitamin D has been proposed to be delivered tothe proximal kidney tubule for further conversion to1,25(OH)2-vitamin D by a different and remarkable mech-anism. Rather than diffusing passively, it has been proposedthat the 25(OH)-vitamin D-DBP complex passes the glo-merular filter and is endocytosed by the epithelial cell of theproximal tubule (FIGURE 5) (805). The endocytotic processis mediated by megalin (aka gp330), which is a multifunc-tional clearance receptor on the luminal membrane. Micelacking functional megalin were shown to lose DBP andvitamin D in the urine and develop vitamin D deficiency(805). A kidney specific megalin (�/�) animal was recentlycreated, and the observations made in the global (�/�)animal, which had a very low perinatal survival rate of 2%,could essentially be replicated (643). Furthermore, defectsin cubulin, a membrane protein that colocalizes with mega-lin, cause a similar phenotype (806). The experimental dataare further supported by clinical observations made in pa-tients suffering from Fanconi syndrome. Fanconi syn-drome is a global reabsorption deficiency of the proximaltubule, which can develop as a result of heavy metalpoisoning and/or drugs or may have inherited causes.These patients were shown to lose DBP in their urine,which may reflect the inability of the tubule cell to endo-cytose DBP (805, 1076, 1100). A similar endocytoticuptake mechanism has been proposed for mammary
cells, which can also convert 25(OH)-vitamin D to1.25(OH)2-vitamin D(926).
6. Cellular effects of vitamin D
The cellular effects of 1,25(OH)2-vitamin D can be catego-rized into two major pathways, which are defined by theirrespective speed of onset: 1) slow genomic responses and2) rapid nongenomic responses. Both pathways requirebinding of 1,25(OH)2-vitamin D to its intracellular recep-tor, the VDR (503, 787). The VDR (NR1I1, nuclear recep-tor subfamily 1, group I, member 1) belongs to the super-family of nuclear receptors, which amongst others alsoincludes the estrogen, testosterone, or glucocorticoid recep-tors. VDR was first identified in the late 1960s in the chro-matin fraction of chick intestinal mucosa, where1,25(OH)2-vitamin D increases the rate of intestinal cal-cium uptake (430). The 427-amino acid protein (molecularmass 48.3 kDa) was cloned in 1988 by Baker et al. (59). Thecrystal structure of the VDR is available to us with1,25(OH)2-vitamin D bound to the receptor’s ligand bind-ing domain (914).
A) GENOMIC EFFECTS. Following ligand binding, nuclear recep-tors typically act as transcription factors and induce or re-press the transcription of certain target genes. In the case ofVDR, 1,25(OH)2-vitamin D binds to the receptor, whichsubsequently heterodimerizes with the retinoid X receptor(RXR) (FIGURE 3) (1027, 1083). The VDR-RXR complexthen interacts with a VDRE in the 5= promoter region of theregulated gene resulting in transactivation. Alternatively, ithas been proposed that VDR can bind to the VDRE beforeligand binding occurs (920).
I) Intestine. The intestine is one of the primary target sites of1,25(OH)2-vitamin D. 1,25(OH)2-vitamin D upregulatesthe expression of intestinal TRPV6, calbindin-D 9k, andPMCA, which are canonically regarded to mediate the pro-cess of transcellular calcium absorption (FIGURE 3) (see sect.IIIA). Furthermore, 1,25(OH)2-vitamin D may modulatecalcium uptake through the paracellular route (see sect.IIIB). By increasing the amount of absorbed calcium,1,25(OH)2-vitamin D directly elevates serum calcium lev-els. This represents one of the final links in the regulatorychain of calcium homeostasis which starts with sensing oflow calcium levels by the parathyroid gland and ends withincreased synthesis of 1,25(OH)2-vitamin D by the kidney.The significance of 1,25(OH)2-vitamin D for intestinal cal-cium absorption is illustrated by 1,25(OH)2-vitamin D-de-ficient patients, which absorb up to 80% less calcium fromtheir meal compared with healthy individuals (996). Al-though similar results were obtained in animal models,probably one of the more illustrative observations has beenmade in VDR-deficient animals (825, 1110). Deletion ofVDR correlates with a massively impaired capacity to ab-sorb intestinal calcium resulting in low plasma calcium lev-els and hyperparathyroidism (1110). This phenotype is re-
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
219Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

versible by intestine-specific expression of VDR on a VDR(�/�) background (712, 1181). Thus animals that lack theVDR, except in the intestine, present with normal serumcalcium and PTH levels (1181). In conclusion, it is unques-tionable that 1,25(OH)2-vitamin D and its receptor are thekey regulators of intestinal calcium absorption.
II) Bone. Some evidence exists that 1,25(OH)2-vitamin Dmay have direct influences on the formation of bone (FIG-URE 4). The VDR is expressed in osteoblasts, osteoclasts,and chondrocytes (115, 533, 623, 730). Most of the directeffects of 1,25(OH)2-vitamin D are thought to be mediatedby osteoblasts. 1,25(OH)2-vitamin D has been shown topromote osteoblast differentiation from mesenchymal stemcells and to regulate the synthesis of various osteoblast pro-teins, such as osteocalcin, alkaline phosphatase, collagen I,osteopontin, and RANKL (45, 78, 79, 665, 709, 804, 870,925). In general, however, the effects of 1,25(OH)2-vitaminD on osteoblast maturation and protein synthesis are verypleiotropic and depended on the duration of the exposureand the differentiation stage at which the osteoblast is ex-posed (817). Effects of 1,25(OH)2-vitamin D on the miner-alization of bone have also been reported. For example, anincrease in the mineralization of extracellular matrix wasobserved following concomitant 1,25(OH)2-vitamin D andvitamin K exposure (599, 745). Yet, the overall direct influ-ence of 1,25(OH)2-vitamin D on bone metabolism is some-what obscure. This is illustrated by VDR-deficient animals.Naturally, these animals develop rickets and osteomalaciadue to impaired intestinal calcium absorption. If the ani-mals are, however, maintained normocalcemic, the skeletalphenotype is completely rescued (21, 661). Although, theseobservations question the importance of 1,25(OH)2-vita-min D as a direct regulator of bone metabolism, a subse-quent investigation by Panda et al. (821) came to a differentconclusion. The authors reported that osteoblast numbers,mineral apposition rates, and overall bone volume werereduced in normocalcemic (rescue diet) cyp27b1/VDR(double �/�) animals, suggesting that the 1,25(OH)2-vita-min D system is necessary for intact bone formation (821).The reason for these discrepant findings is generally un-clear; however, differences in the length of exposure to therescue diet have been put forward as a possible cause (821).For a more detailed review of the effects of vitamin D onbone, please refer to References 1033, 1114.
III) Kidney. The kidney is not only the major site of1,25(OH)2-vitamin D synthesis (see above), but also repre-sents a vitamin D target organ. The kidney acts as keyregulator of calcium homeostasis by changing the amountof calcium that is reabsorbed from the primary urine. Themajority of the calcium that is filtered through the glomer-ulus is reabsorbed in the proximal tubule through the para-cellular space, with the amount of absorbed calcium grad-ually decreasing along the nephron. Fine regulation of cal-cium absorption occurs in the distal tubule and collecting
duct. The mechanism by which the distal tubule conductstranscellular calcium absorption is highly analogous to theproximal intestine. The epithelial cells of the distal tubuleexpress TRPV5 (the “sister” channel of TRPV6) as the api-cal calcium entry channel, calbindin-D 28k and NCX1 andPMCA1b as basolateral calcium extruders (203, 474, 610,837, 922). In analogy to the intestine, 1,25(OH)2-vitamin Dupregulates the majority of these proteins in an effort toincrease renal calcium reabsorption (203, 474, 610, 837,922).
B) NONGENOMIC EFFECTS. In contrast to the genomic effects of1,25(OH)2-vitamin D, which have been known for decades,the rapid cellular responses have only recently receivedmore scientific attention. While the transcriptional events of1,25(OH)2-vitamin D take place on a time scale of a fewhours to days, the rapid nongenomic responses occur withinminutes of exposure. One of the first evidences, which inretrospect can be attributed to a nongenomic response, wasthe observation made in 1941 by Selye that intraperitonealinjection of steroids had an anesthetic effect (990). Interest-ingly, the rapid responses to 1,25(OH)2-vitamin D also re-quire the presence of the VDR, as these responses cannot beelicited in VDR deficient animals (503, 787). It should benoted that other proteins such as 1,25(OH)2-vitamin-D-MARRS have also been suggested as candidates for a mem-brane associated 1,25(OH)2-vitamin D receptor (782). At-tempts at identifying the subcellular localization of theVDR in the rapid response context have yielded that VDR isalso present in plasma membrane invaginations, the so-called caveolae (503, 802). These VDR-containing mem-brane microdomains have been identified in multiple tis-sues, including the intestine, kidney, and lung, and are iden-tified by coexpression of caveolin-1, which is used as amarker protein for caveolae (503, 802). Functionally, notmany rapid response effects of 1,25(OH)2-vitamin D havebeen characterized. For example, it has been demonstratedthat 1,25(OH)2-vitamin D can influence ion channel gatingin osteoblasts, modulate the contraction of cardiomyocytes,lead to insulin secretion in pancreatic �-cells via elevatingintracellular calcium, and cause photoprotection in keratin-ocytes (273, 540, 1088, 1200, 1216). In the intestine, thephenomenon of transcaltachia (see sect. IIIC) has been at-tributed to rapid actions of 1,25(OH)2-vitamin D (801).
In addition to 1,25(OH)2-vitamin D, the VDR also bindsthe secondary bile acid lithocholic acid (704). Secondarybile acids are bile acids that have been metabolized by theintestinal gut flora. Lithocholic acid is toxic and has beenimplicated to play a role in intestinal carcinogenesis (601).It has been suggested that the VDR may serve as a second-ary bile acid sensor and induce lithocholic acid breakdownthrough CYP3A activation (537). The noncanonical VDRstimulation by lithocholic acid may thus serve as an auto-protective mechanism (704). Apart from inducing CYP3A,lithocholic acid has been demonstrated to increase expres-
SASCHA KOPIC AND JOHN P. GEIBEL
220 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

sion of TRPV6 in intestinal cell lines, which corroborates itsrole as a physiological VDR agonist (517).
We are far from understanding the full spectrum of theeffects of 1,25(OH)2-vitamin D, and unfortunately, thescope of this review does not allow a detailed analysis ofthese processes. In general, our knowledge concerning thephysiological role of 1,25(OH)2-vitamin D is massively ex-panding beyond the horizon of calcium homeostasis. Evi-dence is accumulating that 1,25(OH)2-vitamin D can influ-ence the renin-angiotensin-aldosterone system and maythereby act as a regulator of blood pressure (660, 662,1219). Furthermore, low vitamin D status is associated withan increased incidence of colorectal, ovarian, and breastcancer(363, 364, 642, 984). Vitamin D also acts as a potentmodulator of the immune response and cell proliferation.
B. PTH
Experiments dating back to the beginning of the 1900s havedemonstrated that surgical removal of the parathyroidgland results in tetany. It was recognized very early thatadministration of calcium could ameliorate or prevent themanifestation of tetany, and it was subsequently concludedthat the parathyroid glands play an important role in cal-cium metabolism (690, 826, 939). In 1925, extracts fromthe parathyroids were for the first time shown to controltetany in dogs (216). This finding marked the discovery ofPTH, which is one of the three prime hormones regulatingcalcium homeostasis.
1. Production and secretion
PTH is a 84-amino acid peptide hormone produced in theparathyroid glands. Its amino acid sequence was first estab-lished in 1970 in bovine (126, 788). Cloning of the humancDNA followed a decade later (440). The PTH gene en-codes a 115-amino acid precursor hormone (preproPTH),which is enzymatically cleaved in a two step process to itsmature 84-amino acid secreted form (565). The NH2-ter-minal prepro-signaling sequence is necessary for correcthormone processing and trafficking (340, 546). Thisknowledge is mainly founded on truncation studies andobservations made in patients with mutations in the PTHgene, which can result in familial isolated hypothyroidism,a disorder characterized by hypocalcemia and low PTHlevels (38, 340, 828, 1055). For example, a well-character-ized T-to-C point mutation in the prepro signaling sequencethat causes FIH leads to accumulation of the precursor hor-mone in the ER (243, 546). The impaired processing trig-gers ER stress, ultimately apoptosis and PTH insufficiency(243).
Following its cleavage to mature PTH, the hormone isstored in secretory vesicles and released into the circulationin response to low plasma calcium. The regulation of PTH
secretion is extremely tight, given the body’s need to main-tain the calcium concentration within a narrow window(1.1–1.3 mM). Small alterations in calcium homeostasis canhave deleterious effects, for example, on the excitability ofneurons and muscles. The low plasma half-life of PTH of �5min allows for a precise regulation of this balance (95). Toachieve controlled and rapid on-demand secretion of PTH, theparathyroid is equipped with an ultrasensitive extracellularCaSR, which constantly monitors the plasma calcium levelsand triggers intracellular signaling events and PTH releaseupon imminent drops in calcium levels (FIGURE 6) (see sect.IVD). PTH is further regulated on a transcriptional level by1,25(OH)2-vitamin D, creating a negative-feedback loop(154, 930, 931).
2. PTH1R
PTH exerts its physiological effects via activation of a mem-brane-bound GPCR, the parathyroid hormone receptortype 1 (PTH1R) (PTH2R is mostly expressed in the CNSand tissues that are not involved in calcium handling andwill thus not be reviewed). Of note, PTH1R is not exclu-sively located at the plasma membrane but can also localizeto the cell nucleus. The physiological significance of nuclearPTH1R is currently unclear but may represent a novel sig-naling paradigm for the actions of PTH (830, 856, 857,1155).
Full-length PTH is not required to activate PTH1R. TheNH2-terminal domain of PTH mediates most of the physi-ological effects of the hormone and is responsible for bind-ing in the �-�-�� binding fold of PTH1R (861). This is whyclinically PTH(1–34) is used as a PTH analog with identicalbiological activity (753, 867, 919, 1094). Conversely, NH2-terminal truncation of PTH(1–34) to PTH(2–34) changesthe characteristics to a partial receptor agonist, whereasfurther truncation to PTH(3–34) results in loss of biologicalactivity (1094).
PTH1R was first cloned from opossum in 1991, which wasfollowed by identification of the highly homologous humancDNA shortly thereafter (536, 964). In the nonactivatedstate the receptor is expressed as a homodimer at the cellsurface, which dissociates upon PTH binding (860).PTH1R is a member of the class B (class 2, secretin family)GPCRs. As many other GPCRs, it undergoes N-linked gly-cosylation at four asparagine residues (1218). Mutationalanalysis revealed that site-specific mutation of all four sitesdecreases cell surface expression, whereas impairment offewer glycosylation sites does not seem to have significanteffects on trafficking or ligand binding (1218). Further-more, the extracellular domain of the receptor includes acharacteristic disulfide bond pattern involving six cysteineresidues (392). These residues are thought to be essential forstabilizing the hydrophobic �-�-�� binding pocket forPTH, which is conserved among all members of class B
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
221Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

GPCRs and has recently been crystallized in the presence ofPTH (861).
Binding of PTH causes activation of at least two distinct Gproteins. G�q/11 mediates intracellular calcium release viaphospholipase C (PLC) activation and increases in inositoltrisphosphate (IP3), whereas G�s activates adenylyl cyclaseleading to rises in cAMP (5, 188, 808, 859).
PTH1R can be regulated on a variety of levels, ranging fromtrafficking and internalization to direct protein interactionsat the cell surface. Desensitization of PTH1R is mediated byGRK2 binding/phosphorylation and �-arrestin binding,which uncouples the receptor from its associated G proteinsand triggers its internalization (267, 326, 330, 1123). For
example, knockout of �-arrestin causes increased and sus-tained levels of the second messenger cAMP in primaryosteoblast cultures upon PTH stimulation (327). PTH1Ralso associates with the scaffolding protein NHERF1,which stabilizes the receptor at the cell membrane and pre-vents its endocytosis and desensitization (1022, 1139). Thiseffect of NHERF1 is partially attributable to a prevention ofan interaction between �-arrestin and PTH1R (1140). Co-localization of NHERF1, �-arrestin, and PTH1R has beendemonstrated and suggests that NHERF1 is constitutivelybound, whereas �-arrestin association is more dependenton receptor activation (580). Interestingly, it has recentlybecome apparent that �-arrestin not only plays a role inreceptor desensitization, but also mediates activation ofdownstream signaling cascades, such as MAPKs, in a G
PLA2
Kinase phosphorylation
Increases VDR expression
PTH
Parathyroid gland
Inhibits PTHsecretion
Reduces PTHsynthesis
Nucleus
Inhibition ofcell growth
RXR VDRD
D
D
VDR
1,25(OH)2-D
Calcium
Calcium
Ca
CaCa
Ca
PLC
IP3
AA
DAG PIP2Gq
ER
FIGURE 6. CaSR signaling in the parathyroid gland. Increased serum calcium levels lead to an inhibition ofPTH secretion. Serum calcium levels are measured by the CaSR receptor. Activation of CaSR causesgeneration of arachidonic acid (AA) metabolites, which inhibit the release of PTH and increase the expressionof VDR, thereby increasing the cell’s sensitivity to the negative feedback exerted by 1,25(OH)2-vitamin D.1,25(OH)2-vitamin D suppresses the synthesis of PTH. Furthermore, CaSR activation inhibits parathyroid glandgrowth.
SASCHA KOPIC AND JOHN P. GEIBEL
222 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

protein-independent manner (380). Current scientific effortthus focuses on the development of so-called “biased”PTH1R agonists, which can selectively trigger G protein- or�-arrestin-dependent signaling events, allowing for a moreselective therapeutic repertoire (381, 1160). Furthermore,NHERF may also modulate the cell’s response to PTH bind-ing. In the presence of NHERF2, the cell’s calcium responsevia PLC is augmented, whereas the cAMP response is damp-ened, presumably via recruitment of G�i (698). BothNHERF and �-arrestin provide effective examples of howreceptor-associated proteins can modulate canonical signal-ing events or even, as is the case with �-arrestin, initiatesignaling events in their own right.
PTH1R can also be regulated by its external environment.The extracellular receptor domain can be cleaved by metal-loproteases, resulting in receptor degradation (579). PTHbinding prevents this proteolytic cleavage, thus stabilizingPTH1R at the cell surface. The physiological importance ofthis mechanism is not yet fully understood. However,MMPs are involved in bone remodeling and may in conse-quence locally regulate the sensitivity of osteoblasts to PTH(579).
3. Cellular effects
PTH exerts its effects in two primary target tissues: boneand the kidney.
In the kidney, PTH causes phostphaturia, increases calciumabsorption, and induces the synthesis of 1,25(OH)2-vita-min D. In-detail analysis of renal phosphate handling isbeyond the scope of this review and has been summarizedpreviously (334, 765). In brief, phosphaturia mainly resultsfrom downregulation of the Na-Pi transporter type IIa(NaPi-IIa) at the apical membrane of the proximal tubule,thereby reducing the amount of reabsorbed phosphate fromthe primary urine. Rather than directly modulating thetransporter’s activity, PTH exposure mainly affects thenumber of active cotransporters on the plasma membrane.Activation of basolateral PTH1R causes retrieval of NaPi-IIa and targets it for lysosomal degradation, resulting indiminished Pi reuptake (566, 682, 847). Apart from NaPi-IIa, at least two other apical phosphate transporters arepresent in the proximal tubule: NaPi-IIc and PiT-2 (986,1124). Currently, there is some evidence that PTH can alsoregulate NaPi-IIc and PiT-2, but additional studies remainto be conducted (855, 987). Although a contribution ofthese transporters to renal phosphate reabsorption is highlylikely, knockout studies suggest that NaPi-IIa is responsiblefor �80% of total phosphate transport, thus representingthe major uptake mechanism (72, 468).
It has been recognized for over 30 years that PTH canstimulate the synthesis of the active vitamin D metabolite1,25(OH)2-vitamin D in the kidney (116, 338) (see sect.IVA4). 1,25(OH)2-vitamin D in consequence enhances the
intestinal and renal uptake of calcium in an effort to coun-teract hypocalcemia, which initially led to secretion of PTH.The PTH-stimulated increase in 1,25(OH)2-vitamin D lev-els is achieved on a transcriptional level. PTH upregulatesthe transcription of CYP27B1, the mitochondrial enzymewhich is responsible for the conversion from 25(OH)-vita-min D to 1,25(OH)2-vitamin D. Transcriptional upregula-tion occurs via PTH binding to PTH1R, leading to increasesin the second messenger cAMP and activation of PKA (125,442, 763, 764, 921).
Apart from inducing the synthesis of 1,25(OH)2-vitamin D,PTH can directly upregulate the renal reabsorption of cal-cium. The regulation of calcium absorption by PTH occursin distal segments of the nephron, mostly in the distal con-voluted tubule and the connecting tubule (99, 379, 1003,1172). In close analogy to the duodenum, these segmentsexpress calcium transport proteins, which are responsiblefor mediating the process of active transcellular calciumabsorption in the kidney, namely, TRPV5, calbindin-D28k, and NCX1. PTH can regulate all of these protein levelson a transcriptional level (1108). Interestingly, this seems tobe accomplished independently of 1,25(OH)2-vitamin D,which also positively regulates most of these transporters(see sect. IVA6) (1108). It is therefore difficult to dissect therelative contribution of each of the two hormones in thephysiological regulation of the calcium transport proteins.In addition to transcriptional activation, PTH was shown tocause direct phosphorylation of TRPV5, thereby increasingits opening probability (249). The channel is phosphory-lated at threonine-709 in a PKA-dependent fashion (249).Elevation of intracellular cAMP levels and concomitantPKA activation are classical downstream effects of PTH1Ractivation in the kidney (248, 1172).
In bone, PTH exerts a dichotomous effect depending on thepattern of exposure. It is well documented that pulsatilePTH exposure has anabolic effects on bone mass, whereascontinuous release increases plasma calcium by bone catab-olism (FIGURE 7) (27, 348, 401, 469, 1065). The observa-tion that intermittent PTH administration increases bonemass has led to the use of PTH as a treatment strategy forosteoporosis (621, 671, 897). The enhanced bone forma-tion mainly results from an increase in osteoblast numbers.This phenomenon has been partially attributed to a PTH-mediated induction of osteoblast differentiation and an in-hibition of their apoptosis (75, 274, 518, 530, 531, 684,969, 1032). Multiple mechanisms underlying the anti-apo-ptotic effects of intermittent PTH on osteoblasts have beensuggested. Among others, these include runt-related tran-scription factor 2 (Runx2)-mediated transcription of sur-vival genes and increased DNA repair (75, 969). It hasfurther been shown that fibroblast growth factor 2 (FGF2)is partially needed as an endogenous cofactor for the ana-bolic effects of PTH to take place (934).
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
223Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

Continuous PTH exposure, on the other hand, mainly af-fects osteoclast numbers and activation, thereby increasingbone turnover. Since osteoclasts are canonically thought tonot express PTH1R (although this view has recently beenchallenged, Ref. 260), the catabolic effects of PTH are re-layed through osteoblast signaling. The PTH-inducedcrosstalk between osteoblasts and osteoclast is mainly me-diated by receptor activator of nuclear factor �B (RANK),osteoprotegrin (OPG), and RANK ligand (RANKL). BothRANKL and OPG are expressed by osteoblasts and exertopposing actions on osteoclasts. RANKL promotes oste-oclastogenesis by binding to RANK on osteoclasts. Con-versely, OPG serves as a soluble decoy receptor for RANKLand thus inhibits its interaction with RANK, thereby sup-pressing osteoclastogenesis. In accordance with this model,RANKL-deficient animals develop osteopetrosis because ofinsufficient osteoclasts activation (592). Sustained PTH ex-posure affects RANK-RANKL signaling by downregulat-ing antiresorptive OPG, while simultaneously stimulat-ing production of RANKL by osteoblasts (FIGURE 7)(350, 497, 679, 689). The enhanced RANK-RANKL sig-naling induces formation of osteoclasts, which in turnleads to enhanced bone resorption and elevates serumcalcium levels.
In the intestine, several observations suggest that PTH mayhave a direct, i.e., non-1,25(OH)2-vitamin-D mediated, ef-fect on intestinal calcium absorption. Both isolated entero-cytes and intestinal loops demonstrated an increase in cal-cium uptake following acute PTH exposure (781, 783,784). However, more investigations are needed to clearlyestablish a direct regulatory role of PTH in the context ofintestinal calcium uptake.
4. PTH fragments
It should be noted that full-length PTH(1–84) is not theonly circulating form of the hormone in the body. VariousPTH fragments can be found in the circulation, which par-tially originate directly from the parathyroid gland and par-tially represent products of peripheral cleavage. The para-thyroid itself releases COOH- and NH2-terminal hormonefragments, which are generated by cysteine proteases (ca-thepsin B and H) in distinct secretory vesicles of the gland(418, 427, 693). Interestingly, the fraction of secreted hor-mone fragments changes with extracellular calcium condi-tions. It has been reported that more fragments are releasedunder conditions of hypercalcemia, when secretion of full-length PTH is suppressed (417, 418, 605, 726). Peripheralproteolysis represents the second source of PTH fragments.This process occurs predominantly in liver and the kidney(127, 234, 989). The group of fragments that have receivedthe most amount of scientific attention is the large NH2-terminally truncated non-PTH(1–84) fragments. PTH(7–84) is the quantitatively major member of this group, whichis secreted by the parathyroids (233). The group of non-PTH(1–84) fragments can represent up to 20% of circulat-ing PTH, but can increase in patients with renal failuredramatically to up to 50% because of impaired renal clear-ance (130, 131, 444, 648). This is of particular interest, as ithas become recently apparent that the non-PTH(1–84)fragments exert biological activity. In general, non-PTH(1–84) fragments antagonize the effects of PTH in its primarytarget tissues, bone and the kidney but also the parathyroidgland directly. It has been shown that PTH(7–84) can in-hibit PTH release from the parathyroid, presumably in anautocrine fashion, despite low serum calcium concentra-
PTH
Intermittent Chronic
PTH1R
Osteoblastproliferation
Osteoblast Osteoclast
Osteoclastdifferentiation
H+
RANKL RANK
OPG
V-ATPase
FIGURE 7. The effects of PTH on bone. PTH has a dual effect on bone. Intermittent PTH exposure causesosteoblast proliferation, leading to an increase in bone mass. Continuous PTH exposure results in RANKLupregulation and concomitant OPG suppression (OPG serves as a decoy receptor for RANKL and prevents itsinteraction with osteoclast RANK). The stimulated RANKL-RANK interaction leads to osteoclast proliferationand increased bone turnover.
SASCHA KOPIC AND JOHN P. GEIBEL
224 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

tions (493). In bone, PTH(7–84) blocks the effects of PTHon calcium mobilization in thyroparathyroidectomized rats(786). More detailed investigations revealed that PTH(7–84) reduces calcium release from bone in vivo and inhibitsthe formation of osteoclast-like cells in murine primarymarrow cultures (272). In the kidney, PTH(7–84) can in-hibit the formation of 1,25(OH)2-vitamin D, presumablyvia a posttranscriptional mechanism (768, 1102).
Since activation of PTH1R requires an intact NH2-terminaldomain of PTH, it has been speculated that non-PTH(1–84) fragments exert their function through a pathway dis-tinct of PTH1R. The existence of a COOH-terminal PTHreceptor has thus been postulated (270–272, 786). The mo-lecular identity of this receptor is, however, not yet re-solved. Another mechanism through which non-PTH(1–84) fragments may exert their biological activity is down-regulation of PTH1R. It has been demonstrated thatPTH(7–84) causes internalization of PTH1R, thus offset-ting the effects of PTH by decreasing the number of avail-able receptors at the cell surface (1022).
In conclusion, non-PTH(1–84) fragments act as PTH an-tagonists and are secreted by the parathyroid in response tohypercalcemia.
C. Calcitonin
Calcitonin is a peptide hormone that has been discovered byCopp et al. in 1962 as a factor that reduces serum calciumconcentrations (160, 227). Calcitonin production was ini-tially falsely ascribed to the parathyroid glands, and it wasonly later that the thyroid gland had been established as thesource of calcitonin (463). The primary sites of calcitoninproduction are the parafollicular cells (C-cells) of the thy-roid gland. Calcitonin exerts its hypocalcemic effects pri-marily by inhibition of osteoclast activity. It should benoted that the importance of calcitonin in day-to-day cal-cium homeostasis in humans is rather negligible (see sect.IVC4). For this reason, it will only be reviewed concisely.
1. Production and secretion
Calcitonin is encoded by the CALCA gene and is initiallysynthesized as a 141-amino acid precursor (preprocalci-tonin), which is later processed to the mature 32-amino acidhormone (637). The same gene also encodes the neuropep-tide CGRP. Production of either peptide is dependent ontissue-specific RNA splicing. Although encoded by a differ-ent gene, amylin also belongs to the calcitonin peptide fam-ily. All three peptides, i.e., calcitonin, CGRP, and amylin,share some overlapping functions with regard to osteoclastsuppression (16, 229, 1199). Calcitonin is released from theC-cells in response to rising concentrations of plasma cal-cium. The CaSR is responsible for the molecular process ofcalcium sensing on the parafollicular cells (351, 367, 728).
2. The calcitonin receptor
Calcitonin exerts its physiological functions via activationof the calcitonin receptor. The calcitonin receptor is a seven-transmembrane domain GPCR. In particular, it is a memberof the family B subfamily of GPCRs (669). It shares signif-icant homology with other receptors of the family, whichinclude the PTH, GHRH, PACAP, VIP, secretin, glucagon,and glucagon-like peptide receptors.
The calcitonin receptor is expressed in the two most exten-sively described calcitonin target tissues, i.e., osteoclastsand the kidney, but also in other adult tissues, such as theprostate, CNS, skeletal muscle, and placenta (17, 329, 428,790, 878, 1174). Multiple isoforms of the calcitonin recep-tor occur in the body, which results from different RNAsplicing directed by tissue-specific promoters (17, 30, 389,606). Activation of the calcitonin receptor mostly translatesinto a rise of intracellular cAMP levels via Gs-dependentactivation of adenylate cyclase (167, 332, 435, 669). Al-though the cAMP/PKA pathway appears to be dominant,activation of both PLC and PLD have also been reported(167, 332, 776).
3. Cellular effects
A) OSTEOCLASTS. Shortly after the discovery of calcitonin andits hypocalcemic effects, investigators set out to identify itsphysiological site of action. First evidence for an effect ofcalcitonin on bone metabolism came from experiments onrat embryonic bone in tissue culture. It was observed thatcalcitonin caused a decreased basal release of calcium fromthese preparations (343). These observations served as thefirst evidence of how calcitonin lowers serum calcium levels.Furthermore, calcitonin blocked the resorptive actions ofPTH on bone, albeit only temporarily (342, 343). After 4–6days of combined treatment (calcitonin � PTH), calciumrelease rose again (342). This desensitization to the effectsof calcitonin has been coined as the calcitonin “escape”phenomenon (342). Today we know that the transient ef-fect of calcitonin on osteoclasts is attributable to a down-regulation of surface calcitonin receptors and their synthe-sis (882, 1061, 1129, 1130).
As alluded to before, calcitonin directly inhibits the actionof osteoclasts, causing the balance between bone absorp-tion and formation to shift towards anabolism. Calcitoninexerts its inhibitory effects on osteoclasts via activation ofits receptor, which is expressed in abundance on their sur-face (428, 790, 878). Exposure to calcitonin triggers dis-tinct morphological changes in the osteoclast. Osteoclastsare highly motile cells that resorb bone via formation ofso-called resorptive pits, which are membrane invagina-tions that are luminally acidified by active proton secretion.Calcitonin has been shown to inhibit the formation of theseresorptive bays in vitro (487, 1057). Furthermore, oste-oclast motility is markedly decreased, causing the cell to
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
225Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

enter a state of functional quiescence (169). Apart fromdirectly altering osteoclast function, calcitonin also affectsosteoclast differentiation. Calcitonin inhibits the formationof multinucleated mature osteoclasts by arresting their dif-ferentiation in more immature stages (1060).
B) KIDNEY. Renal calcium handling is the second organfunction that is influenced by calcitonin. However, it isnot entirely clear whether calcitonin causes calciuria orenhances calcium reabsorption from the urine. The con-flicting results may be to some extent attributable to spe-cies differences. In humans, calcitonin likely increases theexcretion calcium through the urine and thereby acts inconcert with its inhibitory action on osteoclasts to lowerserum calcium levels (31, 32, 143, 215, 819, 1016). Con-versely, most studies demonstrating an increase in therenal reabsorption of calcium and magnesium were con-ducted in rats, rabbits, or mice (84, 158, 159, 265, 304,877, 883, 1225). A single investigation established a cal-cium-conserving effect of calcitonin in human (160). Theprimary site of action for calcitonin in the rat is the thickascending limb (TAL) of the loop of Henle, where calci-tonin has been demonstrated to bind its receptor, in-crease local adenylate cyclase activity, and promote cal-cium reabsorption (166, 168). Apart from enhancing thereabsorption of calcium, calcitonin also promotes thevectorial transport of NaCl in the rat TAL, thereby am-plifying the corticomedullary concentration gradient,which is a prerequisite for the subsequent concentrationof urine in the collecting duct (265, 304). In the rabbit,the calcium-conserving effects of calcitonin seem to bemediated by the distal tubule (1225).
It has also been speculated that calcitonin may act di-rectly on the collecting duct in a similar fashion to anti-diuretic hormone (ADH or vasopressin), i.e., to concen-trate the urine by increasing the reabsorption of waterfrom the primary urine (251). Indeed, calcitonin wasshown to increase the apical expression of aquaporin 2(AQP2) in principal cells of the collecting duct (119).Apical insertion of AQP2 and subsequent transepithelialwater movement is the primary mechanism by whichADH causes concentration of the urine to lower plasmaosmolarity.
In conclusion, the direct impact of calcitonin on renalcalcium handling is quite vague and may be of minorimportance. However, calcitonin also has another, indi-rect effect on calcium homeostasis. Calcitonin wasshown to be an important regulator of the expression ofCYP27B1, the renal enzyme responsible for the conver-sion of 25(OH)-vitamin D to 1,25(OH)2-vitamin D(1009, 1217). In normocalcemic rats, CYP27B1 mRNAlevels were inducible by calcitonin administration, lead-ing to an increase in the production of 1,25(OH)2-vita-min D (1009, 1217). Furthermore, CYP24A1 was in-
duced in HEK-293 cells following calcitonin exposure,suggesting a regulatory role of calcitonin in vitamin Dcatabolism (361). In addition to its putative direct effecton calcium reabsorption, calcitonin may thus affect nor-mal calcium metabolism indirectly by modulating thelevels of circulating 1,25(OH)2-vitamin D.
4. The relevance of calcitonin forcalcium homeostasis
The relevance of calcitonin for day-to-day calcium balanceis highly debatable. This is corroborated by fundamentalobservations during conditions of decreased or increasedcalcitonin levels, neither of which result in an appreciablephenotype in terms of calcium balance. For example, pa-tients with medullary carcinomas of the thyroid (MTC), atumor of the thyroid C-cells resulting in the hypersecretionof calcitonin, were shown to have normal bone mineraldensities (1176). Animal studies further substantiate thisconundrum. A reduction in serum calcitonin levels by thy-roidectomy in rats did not impact serum calcium levels(223, 1064). In light of this evidence, the question arises asto what the physiological role of calcitonin is.
It has been suggested that calcitonin is an evolutionary rem-nant (462). This is substantiated by the fact that calcitoninfrom other species is more potent than human calcitonin.Teleost calcitonin has the highest biological activity in hu-mans, which may be a result of their higher dependence onthe hormone. For example, salmon calcitonin has an ap-proximately sixfold higher affinity to calcitonin receptorthan human calcitonin (28, 328). Furthermore, it is lesseffectively eliminated by the kidney, resulting in a longerplasma half-life (405). The differences in the biological ac-tivity between calcitonin forms led to the introduction ofsalmon calcitonin as a treatment for skeletal disorders, suchas osteoporosis or Paget’s disease (1077).
Given its ambiguous role in regular calcium homeostasis, ithas been postulated that calcitonin may be of importanceduring states of high calcium demand, such as during lac-tation (1170). It has been demonstrated that calcitonin andCGRP (�/�) mice show greater loss of skeletal mass duringlactation than wt animals (1170). Since calcitonin andCGRP are encoded by the same gene, animals were con-trolled by CGRP substitution, which was without effect(1170). Another mechanism by which calcitonin may beosteoprotective during lactation or pregnancy is by induc-ing the renal synthesis of 1,25(OH)2-vitamin D (1217).
D. The CaSR
The CaSR is a G protein-coupled membrane-bound recep-tor that is the primary sensor for calcium and is the first linkin the regulatory chain of calcium homeostasis. By regulat-ing the release of PTH from the parathyroid to modulate
SASCHA KOPIC AND JOHN P. GEIBEL
226 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

current serum calcium levels, it presides over the subsequenthierarchical cascade of vitamin D synthesis and calciumhandling in the vitamin D target organs, such as the intes-tine, kidney, and bone. More recent investigations havedemonstrated that the CaSR is not exclusively expressed inthe parathyroid gland, but is also present locally in thevitamin D target organs. This diverse expression suggeststhat CaSR can modulate organ function locally and outsideof the strict PTH-vitamin D-organ axis. Thus a short andlocal feedback loop is created, which allows the organs torespond rapidly to the local calcium environment. A de-tailed description of the receptor’s role in each tissue isbeyond the scope of this article, but an attempt will be madeto identify the key features of CaSR in these local sites in asubsequent section (FIGURE 8). For excellent in-depth re-views, please refer to Refs. 372, 711, 906.
The importance of CaSR as a regulator of calcium balanceis underlined by clinical pathologies that are caused by itsmutation. Loss-of-function mutations cause familial hy-pocalciuric hypercalcaemia (FHH; OMIM 145980) andneonatal severe hyperparathyroidism (NSHPT; OMIM239200), whereas activating mutations cause autosomaldominant hypocalcemia (OMIM 601198). These muta-tions mostly change the threshold of receptor activation ineither direction. Currently, �300 different mutations arereported, two-thirds of which represent inactivating muta-tions (241). Given its broad expression pattern, the de-ranged sensing of blood calcium levels in these disorders notonly affects the secretion of PTH from the parathyroidglands, but also causes local dysfunction in other organs,such as the kidney where calcium absorption is perturbed.
1. Structure and signaling
The CaSR was first cloned by Brown et al. (134) in 1993from bovine parathyroid using a Xenopus oocyte expres-sion cloning system. Cloning of the human CaSR followed2 years later (366). The CaSR is a 1,028-amino acid proteinthat belongs to the superfamily of classic 7-transmembranedomain G protein-coupled receptors (134, 366). It is mainlyexpressed as a homodimer on the cell surface (55). Thedimerization process has been shown to take place in the ERand is mediated by the formation of disulfide bonds be-tween cysteine residues (C129, C131) and noncovalent in-teractions of leucine residues (L112, L156) in the extracel-lular domain of the receptor (54, 529, 858, 888, 1213).Following assembly in the ER, the CaSR undergoesN-linked glycosylation in the Golgi apparatus, some ofwhich is pivotal for cell surface expression (887). The traf-ficking between ER and Golgi apparatus is regulated by thesmall GTP-binding protein Rab1 (1221). Knockdown andmutations of Rab1 in HEK cells results in decreased num-bers of CaSR at the cell surface (1221). Conversely, theinternalization of CaSR is thought to be mediated by ubiq-uitination by the E3 ligase dorfin (498).
On the cell surface, the CaSR resides in caveolin-1-richplasma membrane domains, which also contain associatedsignaling proteins (571). These signaling complexes areformed with the help of scaffolding proteins. The COOH-terminal tail of CaSR binds to filamin A, an actin bindingprotein (48, 467). Silencing of filamin A with siRNAs re-sults in the attenuation of MAPK signaling by the receptor(496) (see below).
In lack of a crystal structure of CaSR, the exact binding sitesof calcium on the extracellular domain remain subject ofspeculation. So far, applicable structural data has only beenobtained from the metabotropic glutamate receptor type I(mGluR1), which belongs to the same family of type CGPCRs. In this model, glutamate binds to key residueswhich are located in a cavity, embedded in between twolobular domains (LB1 and LB2) of the extracellular tail(611). This structural hallmark has been aptly coined thereceptor’s Venus fly trap module. This motif is conservedamong other GPCRs of the same family. Multiple attemptsto identify the calcium binding sites have been undertakenusing computational homology modeling (499, 500, 1014).These models have postulated between one and five calciumbinding sites (499, 500, 1014). With the employment ofmutational analysis, it has been possible to validate func-tionality of some of these putative binding sites (500). Mon-itoring of the intracellular calcium response to increasingextracellular calcium levels in CaSR transfected HEK cellshad indicated previously that the Hill coefficient for thisresponse was �3.1, suggesting that multiple calcium bind-ing sites may exist (834).
It should be noted that the CaSR can also be stimulated byother polyvalent cations (Mg2�, Pb2�, Cd2�, Fe2�, Ba2�,Ni2�, Co2�, or Gd3
�) and larger polycationic molecules,such as spermine, spermidine, putricine, protamine, andneomycin (134, 416, 880). Furthermore, several substancescan allosterically modify the receptor and potentiate its sen-sitivity to its direct agonists. These include pharmacologicalsmall molecule substances (calcimimetics) that are in clini-cal use for the treatment of conditions, such as secondaryhyperparathyroidism, and L-type amino acids, which en-able the CaSR to act as a nutrient sensor (220). Truncationstudies have demonstrated that the Venus fly trap motif isnecessary for allosteric modification by L-type amino acids(759). The affinity of calcium to the CaSR can also be mod-ulated by changes in extracellular pH (279, 879). An acidicextracellular milieu has been shown to decrease the sensi-tivity of CaSR to its agonists, whereas an increased extra-cellular pH has converse effects (879).
The intracellular domain of CaSR contains five PKC phos-phorylation sites (366). Mutational analysis demonstratedthat PKC-mediated phosphorylation of the CaSR at Thr-888 blunts its response to extracellular calcium, as evi-denced by inhibited calcium release from intracellular
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
227Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

Differentiationand function
Osteoblast Osteoclast
?
? ?
H+
RANKL RANK
V-ATPase
PPIsAPAs
Parietal cell
K+
H+H,K-ATPase
Circulation
ECL-cell +parietal cellactivation
G-cell
Gastrin
CaSR
CaSR
Mitochondria: CYP27B1
25(OH)-vitamin D
CaSR
CaSR
CaSR
1,25(OH)2-vitamin D
Proximal tubule
HPO42–
H2O
H2O
Na+NaPi-IIa
V-ATPase
CaSR
Collecting duct
Thick ascending limb ofthe loop of Henle
Na+
NKCC2
K+
K+
2Cl–
ROMK
AQP2
CaSR
Ca2+
CaSR
H+
CaSR
CaSR CaSR
CaSR
Distal convoluted tubule
CaSR
TRPV5
Ca2+
Cl–
CFTR
CaSR
CaSR
Enterocyte
Calcium-sensing receptor
Intestine
BoneStomach
Kidney
1
1
2
2
3
FIGURE 8. CaSR in the gastrointestinal tract, kidney, and bone. Kidney: the effects of CaSR activation on iontransport in various nephron segments are shown. In the proximal tubule, CaSR stimulates phosphateabsorption and 1,25(OH)2-vitamin D synthesis. In the thick ascending limb of the loop of Henle, CaSR inhibitsapical potassium channels (ROMK), thereby inhibiting NKCC2 (potassium recycling). The resulting changes inthe lumen-positive potential inhibit paracellular calcium uptake. In the distal convoluted tubule, CaSR presum-ably stimulates apical calcium entry through TRPV5. In the collecting duct, CaSR stimulates proton extrusionthrough the V-type ATPase and inhibits urine concentration through AQP2. Stomach: in the parietal cell, CaSRinduces acid secretion by activating H�-K�-ATPase. In the G-cell, CaSR activation results in gastrin secretion.Of note, CaSR serves as a luminal nutrient and calcium sensor on the G-cell. Bone: CaSR on osteoblastspresumably regulates their differentiation and RANKL expression. Intestine: in the intestine, CaSR activationreduces water secretion by inhibiting chloride secretion through CFTR.
SASCHA KOPIC AND JOHN P. GEIBEL
228 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

stores (56, 246). The phosphorylation occurs in response toreceptor activation and thus represents an autoinhibitoryfeedback mechanism (246). �-Arrestins are most likely in-volved in the process of PKC-associated desensitization(681, 853). Conversely, dephosphorylation of the Thr-888residue is carried out by a calyculin-sensitive phosphatase,thereby restoring the receptor’s initial sensitivity (246). An-other mechanism of desensitization is mediated by a G pro-tein receptor kinase (GRK), most likely by interfering withG�q regulated pathways (see below) (681, 853).
Once stimulated, the CaSR activates a variety of intracellu-lar signaling cascades. Being a GPCR, most of these pro-cesses are mediated by G proteins. Specifically, G�q/11, G�i,and G�12/13 have been shown to be coupled to the CaSR(40, 175, 495, 849). The expression of all subunits wasconfirmed in bovine parathyroid (1115). G�i mediates thesuppression of cAMP levels by inhibiting adenylyl cyclaseand activates the ERK/MAPK pathway (175, 250, 375,572). Activation of G�q/11 results in increased intracellularcalcium concentrations via activation of PLC and IP3 trig-gered calcium release (133, 1010). As demonstrated in HEKcells, this cascade can also activate further downstreamphospholipase A2 leading to production of arachidonic acidmetabolites (415). G�12/13 is thought to regulate phospho-lipase D and phosphatidylinositol 4-kinase (PI 4-K); how-ever, this interaction has only been demonstrated in heter-ologous cell culture system (494, 495).
2. CaSR in the parathyroid
CaSR regulates parathyroid function at three levels: 1) therelease of PTH from secretory granules, 2) de novo synthe-sis of PTH, and 3) parathyroid cell growth.
Activation of CaSR by increasing plasma calcium results inan inhibition of PTH release, thereby lowering calcium lev-els. It is thought that this response is mediated by the gen-eration of arachidonic acid metabolites via G�q and PLA2
activation (FIGURE 6) (121, 152). Cultured porcine parathy-roid cells demonstrated an increase in arachidonic acid pro-duction after CaSR stimulation while PTH release was in-hibited (121). Furthermore, exogenous administration ofarachidonic acid suppressed PTH release from the parathy-roid cells (121). Similar effects were demonstrated for thearachidonic acid metabolites 12- and 15-hydroxyeicosatet-ranoic acid, suggesting that they represent the downstreameffectors of arachidonic acid production (120).
Apart from directly controlling PTH release, CaSR alsomodulates PTH synthesis. PTH gene transcription is mainlyregulated by 1,25(OH)2-vitamin D. Binding of 1,25(OH)2-vitamin D to the VDR causes a decrease in pre-pro-PTHmRNA levels creating a negative-feedback loop (154, 930,931). However, it was recognized before the identificationof the CaSR that serum calcium can modulate the actions of1,25(OH)2-vitamin D on PTH gene transcription (930). It
was shown that increases in calcium can potentiate the in-hibitory effects of 1,25(OH)2-vitamin D (930). This effect ismost likely mediated by CaSR, whose activation can decreasePTH transcription by augmenting the inhibitory effects of1,25(OH)2-vitamin D. Molecularly this is achieved by upregu-lating the expression of the VDR (151, 162, 362, 653, 916).The current working model states that activation of CaSRcauses an increase of arachidonic acid metabolites and activa-tion of the MAPK pathway, which in turn results in increasedVDR mRNA levels (FIGURE 6) (151). This allows the parathy-roid to adjust its 1,25(OH)2-vitamin D sensitivity to the cur-rent plasma calcium levels.
The molecular mechanisms underlying the trophic effects ofCaSR activation are less clear. Earlier observations had al-ready suggested that hypocalcemia is associated with para-thyroid cell proliferation (778). Currently, the CaSR spe-cific calcimimetics provide the most useful insight into theregulation of parathyroid growth by CaSR. Calcimimeticsadministered in the context of both animal models andclinical studies of hyperparathyroidism demonstrate thatactivation of CaSR leads to a reduction in gland size(510, 589, 746, 1128). Conversely, inactivating muta-tions of CaSR result in parathyroid enlargement. Para-thyroid-selective genetic disruption of G�q was further-more shown to cause moderate hyperparathyroidismwith increased plasma PTH levels and gland hyperplasia,suggesting a role of G�q in the regulation of parathyroidcell growth (849). Similar findings were reported inG�q/11 double KO animals (1159).
3. CaSR in the kidney
The CaSR acts as an important regulator of ion and waterhomeostasis in the kidney. It should be noted that it canexert its effects on calcium transport independently of otherhormonal regulators, such as PTH and 1,25(OH)2-vitaminD. The CaSR is expressed along most of the nephron, albeitin varying subcellular localizations (FIGURE 8) (907, 908).In the proximal tubule, CaSR is localized apically at thebase of the brush border, where it has been implicated toplay a role in phosphate transport (52, 907, 909). The pri-mary regulator of phosphate transport in the proximal tu-bule of the kidney is PTH. In brief, increased PTH levelsinhibit phosphate reabsorption from the lumen. Activationof the apical CaSR can partially reverse the effects of PTHand restore phosphate absorption (52). Conversely, PTHand high phosphate levels reduce CaSR expression (909).Furthermore, it is likely that the CaSR mediates the inhibi-tory effects of calcium on 1,25(OH)2-vitamin D synthesis inthe proximal tubule (109, 702).
In the thick ascending limb of the loop of Henle, CaSR islocated on the basolateral membrane (907). In this nephronsegment, the receptor acts as a major modulator of mon-ovalent and polyvalent ion absorption. Activation of CaSRleads to an inhibition of the apical renal outer medullary
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
229Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

potassium (ROMK; Kir1.1) channel, mainly through ara-chidonic acid metabolites created by PLA2 (1147, 1148).Apical ROMK releases potassium ions into the lumen,which in turn are needed to fuel apical ion uptake throughthe Na�-K�-2Cl� (NKCC2) cotransporter. By decreasingapical potassium efflux, CaSR inhibits sodium and chlorideuptake through NKCC2 (906). This correlation is reflectedin much earlier observations, which report that calciuminfusions can decrease tubular sodium clearance (300, 718,1052). In addition, impairment of NKCC2 has also impli-cations for calcium absorption. Reduced NKCC2 activitydecreases the lumen-positive potential and negatively af-fects countercurrent multiplication, and in consequence thenephron’s ability to concentrate urine (434). Both mecha-nisms will lead to impaired calcium absorption (434). Cal-cium absorption in the medullary portion of the thick as-cending limb is thought to occur predominantly as passiveuptake through the paracellular route (995). Similar obser-vations have been made when blocking NKCC2 pharmaco-logically with the loop diuretic furosemide (299). It has thusbeen proposed that activation of basolateral CaSR has“loop diuretic-like” effects, reducing NaCl but also calciumabsorption in the kidney (434).
In contrast to the medullary section, the cortical portion ofthe thick ascending limb has been proposed to have pre-dominantly active calcium uptake properties, which are un-der the hormonal regulation of PTH and calcitonin (344,509). PTH increases calcium absorption in this segment,and it has been shown that, similarly to phosphate absorp-tion in the proximal tubule, activation of CaSR can sup-press the effects of PTH (264, 754). The absorption of NaCldoes not seem to be affected by CaSR (264, 754).
The distal convoluted tubule and the connecting tubule areresponsible for the fine-tuning of calcium reabsorption inthe kidney. To achieve this goal, they are equipped withmolecular machinery, similar to that in the duodenum(TRPV5, calbindin-D 28k, NCX1, and PMCA1b) to ab-sorb calcium against its electrochemical gradient throughthe transcellular pathway (680). In analogy to the proximalsmall intestine, these transporters are predominantly regu-lated through 1,25(OH)2-vitamin D, but also PTH. CaSRcolocalizes with TRPV5 in this segment (1090). Its activa-tion causes increase calcium influx through TRPV5 andmay thereby locally and rapidly adapt active absorption tothe urine calcium concentration (FIGURE 8) (1090).
Apart from regulating calcium and phosphate absorption inthe kidney, CaSR modulates proton and water movement inthe collecting duct. In the intercalated cells of the collectingduct, apical V-ATPase acidifies the urine in an effort tomaintain systemic acid-base homeostasis. It has been shownthat luminal calcium and neomycin can induce V-ATPaseactivity via activation of CaSR, thereby causing proton se-cretion into the urine (FIGURE 8) (901). Since the formation
of calcium kidney stones is dependent on luminal pH, it hasbeen speculated that this may represent an autoprotectivemechanism that prevents nephrolithiasis (901). Further-more, stimulation of apical CaSR in the principal cells of thecollecting duct leads to decreased ADH (vasopressin)-stim-ulated water reabsorption through AQP2 (FIGURE 8) (942,943). Taken together, activation of CaSR has diuretic ef-fects via inhibiting NKCC2 in the thick ascending limb ofthe loop of Henle and by inhibiting AQP2-mediated waterreabsorption the collecting duct.
4. CaSR in the gastrointestinal tract
The CaSR is distributed along most of the gastrointestinaltract, ranging from the stomach to the large intestine (186,360, 744, 932, 998). We are now only slowly beginning tounravel its function in this diverse array of tissues. In thestomach, CaSR localizes to the basolateral membrane ofthe acid-secreting parietal cells and to all membranes of thegastrin-secreting G-cells (FIGURE 8) (142, 182, 886). Pri-mary cultures of G-cells were shown to release gastrin afterstimulation of the CaSR with calcium (142, 886). The re-lease is mediated via calcium influx into the cytosol throughnonselective cation channels opening after CaSR stimula-tion (142). These findings provide the molecular basis forthe observation that rises in serum calcium can increaseserum gastrin levels (see sect. IIB2). The apical expression ofCaSR in G-cells theoretically enables it to act as a luminalnutrient sensor modulating gastric acid secretion and otherparameters. In recent studies there is direct evidence show-ing that gastrin levels increase in mice after calcium andL-type amino acid ingestion (325). This effect was abol-ished in CaSR (�/�) animals (325). In healthy human testsubjects, pharmacological stimulation of CaSR leads to aconcomitant increase in gastrin levels and gastric acid out-put (165). CaSR on G-cells was thus postulated to play animportant role in the gastric phase of acid secretion bymaintaining acid output by maintaining gastrin secretion(325).
Apart from being expressed on G-cells, CaSR is also local-ized on the basolateral membrane of the acid-secreting pa-rietal cell, where it exerts effects that are independent ofgastrin and other secretagogues. Activation of parietal cellCaSR has been reported to increase H�-K�-ATPase-medi-ated proton secretion, thereby acidifying the gastric lumen(FIGURE 8) (145, 291, 373). This stimulatory effect wasdemonstrated for direct activators, such as calcium orGd3�, but also allosteric modifiers, such as L-type aminoacids (145, 291, 373). In parallel to other tissues, the intra-cellular activation signal for H�-K�-ATPase is mediated byrises in intracellular calcium, PLC, MAPK, and PKC (899).In conclusion, both rises in luminal and plasma calciumconcentrations can induce gastric acid secretion either indi-rectly through gastrin release or directly through parietalcell activation. The physiological significance of this obser-vation remains the subject of speculation, but may be linked
SASCHA KOPIC AND JOHN P. GEIBEL
230 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

to facilitating calcium uptake by increasing acid output. Asdescribed in a subsequent section, it has been speculatedthat gastric acid increases the bioavailability of ingestedcalcium (see sect. V). Alternatively, CaSR may primarilyfunction as a nutrient sensor in the stomach (amino acidsensing), which maintains constant acid output in the gas-tric (apical G-cell sensing) and postprandial (basolateralparietal cell) phase of digestion, when circulating levels ofamino acids are high (325).
In the intestine, functional investigations on CaSR havemainly been conducted in colonic epithelia, where CaSRlocalizes to both the basolateral and apical membranes ofthe colonic crypt (173, 186, 360). Expression patterns varyslightly in the small intestine, with general basolateral ex-pression and additional weak apical expression in the villus(173, 360). Furthermore, CaSR is expressed in both theMeissner’s and Auberach’s plexuses. Early experiments onsingle perfused colonic crypts demonstrated that intracellu-lar calcium concentrations could be increased when expos-ing the crypts to classic CaSR agonists and that forskolin-stimulated fluid secretion could be inhibited (186). This andsubsequent investigations indicate that CaSR plays an im-portant role as a modulator of colonic fluid secretion (185,186). Subsequently, attempts have been made to take ad-vantage of the “constipatory” effects of CaSR activation inpathophysiological settings. Activations of CaSR in thecourse of diarrheagenic enterotoxin exposure was shown todecrease fluid secretion via increased breakdown of cyclicnucleotides (371). Although the potential clinical applica-tions of ameliorating the symptoms of secretory diarrheaare promising, more efforts will have to be made to fullyunravel the physiological role of CaSR in intestinal ion andfluid transport. So far it is not clear whether intestinal CaSRcan modulate calcium absorption, as is the case in the kid-ney.
5. CaSR in bone
It is well established that CaSR is expressed in osteoblasts,osteoclasts, and their respective precursors (172, 174, 542,1183–1185, 1192). The functional role of CaSR in thesecells is, however, less clear. Undoubtedly, both cell lines areexposed to local fluctuations in calcium concentrationsmaking an adaptive response to the calcium environmentplausible. Indeed, changes in extracellular calcium concen-tration have been shown to regulate various cell functions,mostly in in vitro models. Extracellular calcium can stimu-late the proliferation, migration, and differentiation of os-teoblasts (174, 297, 1183, 1184, 1186). Similarly, calciumwas proposed as a differentiation signal for osteoclasts(542, 544, 734). Significant doubt about the in vivo impor-tance of CaSR in bone has emerged with the generation ofthe CaSR (�/�) mice. Although CaSR knockout results inrickets, these animals suffer from severe hyperparathyroid-ism, which did not allow a discrimination between the ef-fects of high PTH and CaSR on bone turnover (365). Con-
comitant genetic ablation of the parathyroid gland or PTHsecretion, however, revealed that the skeletal phenotype ofCaSR single mutation (�/�) could mostly be rescued, sug-gesting that the skeletal abnormalities were due to highcirculating PTH levels rather than CaSR inactivation (598,1096). Furthermore, CaSR does not seem to be the exclu-sive calcium-sensing mechanism in osteoblasts, as changesin extracellular calcium can still elicit functional responsesin CaSR (�/�) osteoblasts (852). This observation has beenattributed to another GPCR with calcium-sensing capabil-ities, namely, GPRC6A (850, 851). Although GPRC6A hasa higher activation threshold for calcium, it also responds tothe CaSR allosteric activator R568 (851). GPRC6A activa-tion may thus represent a confounding factor in most invitro studies on osteoblasts and their modulation by CaSR.Also, GPRC6A knockout leads to osteopenia, further un-derlining the possibility of an alternate calcium-sensingpathway in bone (850). Osteoblasts extracted from theseGPRC6A-deficient animals show decreased sensitivity toextracellular calcium and in vitro mineralization defects(854).
Although these observations have profoundly questionedthe physiological significance of CaSR in bone, closer ex-amination still favors a role of CaSR in bone turnover. Withthe recent advances in genetic methods, an osteoblast-spe-cific CaSR (�/�) model has been created (171). These ani-mals have severely stunted growth and skeletal develop-ment, clearly suggesting an involvement of CaSR in normalosteoblast function (171). The previous conflicting evidencegained from global CaSR (�/�) models with survival rescueby elimination of PTH synthesis have been attributed to thepossible expression of alternate CaSR splice variants, whichmay compensate for the deletion of full-length CaSR inthese animals (171, 915). In an attempt to further elucidatethe function of CaSR in osteoblasts, the reverse approachhas been executed by specifically upregulating CaSR in os-teoblasts with use of a constitutively active receptor mutant(296). Upregulation of CaSR results in bone loss, as evidencedby a decrease in bone volume and density, specifically of tra-becular bone (296). These findings are accompanied by anincreased number of osteoclasts, whereas osteoblast parame-ters were essentially unchanged (296). Activation of CaSR hasbeen speculated to promote RANKL production by osteo-blasts, which serves as an osteoclastogenic signal (296). Osteo-blasts may thus recruit osteoclasts and induce their maturationvia CaSR signaling and increased RANKL expression, whichwould explain the observed increase in bone turnover andosteoclast numbers in the setting of constitutive CaSR activa-tion (241).
V. THE STOMACH AND CALCIUM
Preceding parts of this review have independently summa-rized the physiology of acid secretion, intestinal calciumabsorption, and their respective regulation. The following
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
231Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

section will attempt to illustrate the functional intersectionsbetween these seemingly unrelated fields. In particular, thequestion of whether acid is needed to absorb calcium effec-tively from the gut or whether the stomach contributes tothe regulation of calcium homeostasis by secretion of anendocrine substance will be investigated.
A. Proton Pump Inhibitors and the Riskof Fracture
In May 2010, the Food and Drug Administration (FDA)released the following safety announcement: “Healthcareprofessionals and users of proton pump inhibitors shouldbe aware of the possible increased risk of fractures of thehip, wrist, and spine with the use of proton pump inhibi-tors, and weigh the known benefits against the potentialrisks when deciding to use them” (319).
Proton pump inhibitors (PPIs, see sect. IIC1) are in wide-spread use for the treatment of acid-related disorders, suchas gastroesophageal reflux disease (GERD) or gastric ulcerdisease. They exert their curative effects by inhibiting theacid output of the stomach. Over the recent years, mostlyepidemiological evidence has accumulated which links theintake of PPIs to an increased risk of sustaining fractures,especially in the elderly population. Yang et al. (1190) pub-lished one of the earliest and largest studies investigatingthis potential correlation in 2006. Examining a populationof over 13,000 hip fracture cases and over 135,000 controlsover the age of 50, the authors concluded that long-term(over 1 year) PPI use was associated with an increase in hipfractures (AOR � 1.44) (1190). Although the likelihood ofsustaining a fracture following PPI intake may seem fairlylow, the implications for public health are substantial. Thishas multiple reasons: PPIs represent the third most com-monly prescribed medication in the United States and arealso available as over-the-counter formulations. Further-more, there is an ongoing debate whether PPIs are overpre-scribed, putting certain populations at unnecessary risk ofside effects. In combination with the high incidence of os-teoporotic fractures, the mean incidence of hip fracturesalone between 1986 and 2005 was 957 per 100,000 womenover the age of 65 per year, a small increase in risk suddenlyhas implications for a very large population (123).
The roots of this controversy may potentially be traced backto the 1940s and 1950s. Before the advent of PPIs, total andpartial gastrectomies or vagotomies were performed to con-trol acid-related disorders. It was soon apparent that pa-tients who underwent these radical surgical procedures de-veloped osteoporosis/-malacia (58, 305, 732, 876). A studythat assessed the prevalence of osteomalacia in gastrecto-mized patients concluded that up to 12% of patients (19%of females) had histologically overt osteomalacia, althoughgeneral disturbances in calcium metabolism were estimatedto occur in up to 28% of patients (208, 368). Other inves-
tigations came to lower prevalence results of �5–10%(1091). The osteomalacia was also shown to translate intoan increased incidence of fractures in these patients (795).Naturally, gastrectomy represents a radical intervention,and the reasons for this correlation may be multifactorial,but reduced acid output may be of significance.
Back in the field of PPIs, the seminal epidemiologic investi-gation by Yang et al. was subsequently followed up by anumber of studies, which also focused on other types offractures, other populations, and other drugs reducing gas-tric acid output, such as H2 receptor antagonists (202, 228,252, 394, 400, 559, 868, 923). Although their conclusionswere somewhat controversial, a recent meta-analysis sup-ports the initial hypothesis that a correlation between PPIintake and fracture risk (hip, spine, and any-site fractures)exists (1195). The meta-analysis considered 11 studies andidentified an overall odds ratio of 1.30 for all fracture typescombined (1195). There was no association between H2
blocker intake and an increase in fracture risk, althoughsome single studies supported a link (228, 1195). Anothermeta-analysis came to a comparable conclusion with regardto an increased fracture risk under PPI exposure (616).
B. Gastric Acid and IntestinalCalcium Uptake
A variety of reasons could theoretically account for theobservation that PPIs increase the likelihood of fractures.The most prominent hypothesis assumes that the reducedacidity in the stomach impairs the intestinal absorption ofdietary calcium. This assumption is based on both patientobservations and experimental animal data. Alas, the num-ber of animal studies, which in contrast to investigations inhumans per default allow more radical experimental de-signs and genetic manipulation, is very small.
1. Effects of gastrectomy, vagotomy, and PPIs onmineral metabolism in humans
Before discussing the reports that try to correlate PPI usewith calcium uptake, it is worthwhile to examine olderliterature on patients that had undergone partial or totalgastrectomy. As discussed previously, these procedures areknown to be linked to bone disease. In contrast to PPIs,which eliminate the singular factor of acid secretion, gas-trectomies also influence gastric emptying, the emulsifica-tion of food stuffs, and food habits. It is thus more difficultto draw conclusions on the influence of acid secretion oncalcium absorption from gastrectomized patients than fromindividuals on PPI therapy. A further caveat lies in the typeof gastrectomy, as different surgical procedures are andwere in use. Some surgeries bypass the duodenum (BillrothII, Roux-en-Y, total gastrectomy), whereas some leave theduodenal passage intact (Billroth I).
SASCHA KOPIC AND JOHN P. GEIBEL
232 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

A common finding among gastrectomized patients is theirlow 25(OH)-vitamin D levels, while levels of 1,25(OH)2-vitamin D seem to be increased (101, 244, 378, 511, 794,972, 1081). The pathophysiological reason for this is notentirely clear. It has been argued that bone disease and low25(OH)-vitamin D are a result of impaired vitamin D ab-sorption following surgery; however, the consensus seemsto be that uptake rates of vitamin D is not impaired in thesepatients (245, 378; contested by Ref. 1081). The vitamin Dinsufficiency may also be a byproduct of improper nutrition(378). As fat and milk intolerance can develop, especially insurgeries which exclude the duodenum (Billroth II), achange of dietary habits with insufficient intake of the fat-soluble vitamin D may be an underlying cause. Indeed,long-term longitudinal studies suggest that maintainingbody weight reduces the risk of developing bone diseaseafter gastrectomy, which emphasizes the role of adequatenutrition (667, 668). On the other hand, Billroth I and IIpatients show the same loss in bone density, although Bill-roth II surgery (bypassing of the duodenum) is associatedwith a much higher degree of fat malabsorption (110, 651).A different investigation even concluded that Billroth I pa-tients have a higher loss in bone density than Billroth IIpatients (794). A more recent report suggests that the prob-lem underlying bone disease after gastrectomy may be im-paired calcium absorption, rather than dietary vitamin Ddeficiency (244). It has been shown that high 1,25(OH)2-vitamin D levels accelerate the breakdown of 25(OH)-vita-min D (210–212, 244). The observed low 25(OH)-vitaminD levels in gastrectomized patients may thus be a byproductof increased catabolism, and not insufficient intake,whereas the high 1,25(OH)2-vitamin D levels may representcompensatory upregulation due to insufficient calcium ab-sorption or intake (244). Calcium absorption in gastrecto-mized patients (Billroth I � II) has been reported to be in thelow-normal range, while 1,25(OH)2-vitamin D levels areincreased (794). In line with these findings, secondary hy-perparathyroidism, an indicator of compensatory upregu-lation due to low serum calcium levels, is a known findingafter gastrectomy (101, 244, 1171). Other investigations onintestinal calcium absorption in gastrectomized patientscame to very contradictory results, ranging from increasedto impaired absorption (8, 34, 255, 398, 585, 794). Manyof these reports failed to assess 1,25(OH)2-vitamin D andPTH levels, which means that adaptive mechanisms maymask the insufficient baseline uptake of calcium in the in-testine (8, 34, 255, 398, 585, 794). In conclusion, the exactpathogenesis of postgastrectomy osteopenia remains some-what unclear. The disorder may be attributable to vitaminD insufficiency, impaired calcium absorption, inappropri-ate diet, or a combination of all factors.
The intrusiveness of gastric surgery makes it difficult todissect the influence of gastric acid on these parameters.This is why vagotomized patients are a somewhat more aptpatient population to study the effects of gastric acid on
calcium uptake, albeit the number of studies on this cohortis very limited. Vagotomy abolishes the parasympatheticinput to the stomach and thereby decreases the amount ofsecreted acid. Although the gross anatomy of the stomachremains intact, other parameters, such as gastrin levels, arealso deranged given the important role of the vagus nerve inthe regulation of gastric acid secretion (see sect. IIB). Whilebone disease is generally not reported in these patients, low25(OH)-vitamin D levels are common (514, 793). Similarlyto gastrectomy, the 1,25(OH)2-vitamin D levels are con-comitantly elevated, suggesting adaptive upregulation po-tentially to compensate for decreased calcium absorption(793). As discussed previously, the decreased 25(OH)-vita-min D could be indicative of augmented catabolism of thevitamin (244). Serum calcium is commonly decreased or inthe lower normal range, while intestinal calcium absorptionis increased, presumably in response to elevated 1,25(OH)2-vitamin D (110, 974). Secondary hyperparathyroidism doesnot manifest (793, 974).
In general, the disturbance in mineral metabolism is morepronounced in gastrectomized patients than in vagoto-mized patients, as evidenced by the higher incidence of bonedisease and secondary hyperparathyroidism. It is challeng-ing to draw clear conclusions on the influence of gastric acidon calcium absorption in either patient group. Yet, it isapparent that compensatory mechanisms are in place inthese patients, as evidenced by the increased 1,25(OH)2-vitamin D and PTH levels. Less efficient calcium uptake dueto decreased acid output may be one explanation for this,but without further analysis this conclusion remains specu-lative.
With the advent of PPIs and H2 blockers, the number ofsurgical interventions to control acid-related disorders de-creased massively. Given their high specificity, PPIs selec-tively eliminate gastric acid output. Several investigationsthat try to tie PPI intake to a disturbance in mineral metab-olism exist. Graziani et al. (396) observed in eight healthyvolunteers that postprandial calcium concentrations didnot increase in subjects on a PPI regime (omeprazole 20 mg3� daily), whereas control subjects demonstrated a clearspike in serum calcium levels. Urine calcium excretion wasalso reduced compared with the control group (396). Asimilar effect of PPIs was later observed by two independentgroups in patients undergoing hemodialysis (395, 423). Itshould be noted that neither of these studies directly as-sessed intestinal calcium absorption, but rather measuredserum calcium as an indirectly related parameter. Morerecently, intestinal calcium absorption was measured byO’Connell et al. (807) using a radiolabeled calcium isotope.The investigators reported that 7 days of PPI (omeprazole20 mg 1� daily) intake significantly reduced calcium ab-sorption in elderly women under fasting conditions com-pared with the placebo group. Although these studies sup-port a role of PPIs in reducing calcium uptake, conflicting
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
233Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

evidence exists. Several investigations that assessed calciumabsorption using radioactive tracers and a whole gut lavagetechnique found no evidence for a decrease in absorptionunder short-term PPI treatment (421, 991, 1173). It is notclear why these discrepancies in the outcomes of the trialsexist. There is, however, variability in the experimentaltechnique to measure calcium uptake, the cohorts investi-gated (young vs. postemenopausal women vs. dialysis pa-tients) and the form of calcium administration (calciumsalts vs. whole meals), which may partially account for thedivergent results. Indeed, different calcium salts are ab-sorbed with different effectiveness in acid suppressed indi-viduals, which will be subject of later discussion (see sect.VC). Furthermore, different populations may have differentcapacities for endocrine compensation.
In summary, it is experimentally difficult to unmask thepotential correlation between a reduction in gastric acidityand calcium absorption, given our body’s high capacity forcompensation. In addition, slight alterations in mineral ho-meostasis may take years to manifest themselves clinically,for example, in osteopenia or fractures. Without followingup on test subjects on a long-term basis, snapshot measure-ments which may still lie within clinically normal range canbe misleading.
2. Effects of gastrectomy, vagotomy, and PPIs onmineral metabolism in the animal model
To further elucidate the problem of osteopenia followinggastrectomy or PPI use, several animal studies tried to rep-licate and expand the observations made in human testsubjects.
For example, Axelson et al. (49) measured serum calciumconcentrations in rats who had undergone parathyroidec-tomy and various surgical procedures to reduce gastric acidoutput (vagotomy, antrectomy, gastrectomy). While para-thyroidectomy alone predictably reduced serum calciumlevels, the gastric operations (with intact parathyroidglands) had little to no effect on calcium concentrations(49). Interestingly, intestinal calcium absorption was evenincreased in the latter group. The authors attributed thisobservation to a compensatory upregulation of PTH secre-tion and concomitant 1,25(OH)2-vitamin D production. Toeliminate this factor, gastrectomy or fundectomy was con-ducted after parathyroidectomy, thereby depriving the ani-mals of their compensatory machinery. This interventionresulted in massive hypocalcemia and death after a fewdays, which led the authors to conclude that acid secretionis important for the maintenance of calcium homeostasis(49). Another investigation in rats that had undergoneantrectomy (Billroth I) observed a significantly decreasedabsorption of calcium (345). Fundectomy did not affectcalcium absorption (927). However, both studies employedthe balance method to calculate calcium absorption, whichis considered less accurate than using radiotracers. In pigs,
total gastrectomy causes massively reduced calcium uptakeand secondary hyperparathyroidism (700). In this study,the duodenum was surgically bypassed by esophagojeju-nostomy, thereby eliminating the site of maximal activecalcium absorption and limiting the conclusion that can bedrawn (700).
In addition, several reports of vagotomy in a rat modelare available to us (49, 307, 308, 928). It has been dem-onstrated that vagotomy alone has no effect on the rate ofintestinal absorption (307, 928). Secondary hyperpara-thyroidism was observed by one group, while PTH levelswere reported to be unaffected by the other group (307,928). 1,25(OH)2-vitamin D was not measured, whichwould have provided further evidence of compensationdue to decreased calcium bioavailability. However, if va-gotomy and parathyroidectomy are performed together,intestinal calcium absorption is significantly impairedcompared with vagotomy or parathyroidectomy alone(307). This is in accordance with the low serum calciumconcentrations found in gastrectomized and parathyroid-ectomized rats (49).
PPIs were also used to relate acid secretion to bone dis-ease in rats. Bone weight did not change in rats that weretreated for 4 wk with omeprazole (841). Alas, calciumabsorption was not measured in these animals, and adecrease in bone weight represents a very terminal andlong-term outcome. A more recent investigation bySchinke et al. (963) demonstrates that mice which havebeen genetically manipulated to be achlorhydric (CCK2
�/�) have decreased serum calcium levels as well as de-velop osteoporosis and secondary hyperparathyroidismin an effort to maintain calcium balance (963). This studyis especially noteworthy, as acid secretion is knocked outselectively in this mouse model while the stomach re-mains intact (stomach morphology). Furthermore, a ge-netic mutation that has been associated with osteopetro-sis (a disease characterized by increased bone density)due to osteoclast malfunction was also shown to causedecreased gastric acid secretion. These patients presentwith lower serum calcium values. Rather than being aproduct of impaired bone resorption (osteoclast defect),the hypocalcemia may thus be related to impaired intes-tinal calcium absorption (gastric acid secretory defect)(963).
C. Calcium Salts
Many investigators have employed calcium salts to de-termine the efficacy of intestinal calcium absorption. Fur-thermore, calcium salts are in wide clinical use as a di-etary supplement. As will be discussed in this section,calcium salts differ in their bioavailability, which notonly represents a potential source of error in experimen-tal designs, but more importantly, has extensive clinicalimplications.
SASCHA KOPIC AND JOHN P. GEIBEL
234 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

Calcium salts represent the most common supplementationform of calcium for individuals who do not meet their ad-equate daily intake. The indications for supplementationcan be diverse, but mostly include conditions such as osteo-porosis/-penia or preventative intake after menopause, dur-ing glucocorticoid intake or if lactose intolerant. In the year2000, the National Health Interview Survey concluded that11% of Americans ingest calcium supplements on a dailybasis (739). Females account for 80% of this population,mostly to ensure supply after menopause (739). Calciumsalts exist in multiple formulations. The most commonlyused salts are calcium carbonate, calcium citrate, calciumlactate, and calcium gluconate. Calcium carbonate is themost widely used formulation, because it contains the high-est percentage of elemental calcium per weight (40%),which equates to small tablet size and easier ingestion (997).In comparison, calcium citrate contains 21% elemental cal-cium, calcium lactate 14%, and calcium gluconate 9%(997). However, the calcium salts do not only differ in theircalcium fraction, but are massively divergent with regard totheir solubility in water. Calcium carbonate is the least wa-ter-soluble salt at a neutral pH. For example, calcium citratedissolves 17 times more readily in water than calcium car-bonate (997). Very fundamental in vitro solubility experi-ments have shown that after 1 h in 500 ml of water only 1%of the initial 500 mg of calcium carbonate are dissolved at37°C (997). The solubility of calcium carbonate can begreatly improved by an acidic environment (390, 997). Ad-justing the pH to 5.5 in the same experiment dissolves 86%of the calcium carbonate; further lowering it to 2.5, a valuethat can be expected in the stomach, increases the dissolvedfraction to 100%. Given these differences in solubility, aplethora of studies have investigated the bioavailability ofthe various calcium salts, mostly focusing on the differencebetween calcium carbonate and calcium citrate. Again, theconclusions are heterogenic. Several studies suggest thatcalcium carbonate is absorbed less effectively than the moresoluble calcium citrate (422, 438, 439, 789), while othersconclude that there is no difference in bioavailability (432,433, 520, 547, 831, 832, 891, 997, 1038). A detailed anal-ysis of the individual trials is beyond the scope of this re-view. It suffices to say that there is strong variability in theexperimental methods (direct absorption measurements vs.measurement of postprandial serum calcium vs. urine ex-cretion) and design of the studies (populations; administra-tion in the fasting state vs. with a meal). A confoundingfactor to the results of these studies may be the gastric pH atthe time of the measurement. As discussed earlier, calciumcarbonate is not very soluble at more alkali pH values,which may have implications for patients using these sup-plements while on PPI therapy (997). Furthermore, mealsdramatically affect gastric pH and may change the bioavail-ability of the supplements. Indeed, there seems to be a cor-relation between gastric pH and the absorbability of cal-cium carbonate. The first observation indicative of this as-sociation was made by Ivanovich et al. in the late 1960s
(520). The group reported that absorption of calcium car-bonate was severely impaired in four male patients sufferingfrom achlorhydria (520). Compared with five control sub-jects, who absorbed between 9 and 18% of the ingestedcalcium carbonate, these patients only absorbed 0–2%. In-terestingly, when gastric acid secretion of one of these pa-tients was stimulated by administration of betazol hydro-chloride (a histamine analog), calcium carbonate absorp-tion rose from 2 to 10% (520). This investigation somewhatspawned the entire controversy of whether gastric acid isnecessary to absorb calcium effectively from the intestine. Asimilar investigation was conducted later by Recker(891) in a larger sample of achlorhydric patients. Theinvestigator concluded that 1) control subjects absorbcalcium carbonate and calcium citrate equally well,2) but that achlorhydric patients lose their capability toabsorb calcium carbonate, while calcium citrate absorp-tion is increased (presumably through compensatory up-regulation of the absorption via vitamin D) (891). It isimportant to mention that these absorption assays wereconducted in the fasting state. When the achlorhydricpatients ingested the calcium carbonate salt together witha meal, their calcium uptake normalized. It cannot beconclusively answered which factor of the meal was re-sponsible for the increase, as several food components,such as fiber and protein, are known to affect calciumuptake. However, the authors speculated that the pH(5.8) of the meal was sufficiently low to dissolve theingested calcium carbonate (891). Furthermore, a previ-ously cited study that demonstrated decreased calciumabsorption under PPI therapy employed calcium carbon-ate as source of calcium for the conducted measurements(807). Patients with gastric bypass surgery also absorbcalcium carbonate less effectively than calcium citrate(1089). The importance of acid for the absorption ofcalcium carbonate was also demonstrated in the previ-ously discussed achlorhydric CCK2 (�/�) mouse model(963). The osteoporotic phenotype and secondary hyper-parathyroidism in these achlorhydric mice could only befully rescued by a high-calcium gluconate (2%) diet, butnot by a high-calcium carbonate (2%) diet (963). In thelight of these reports, it is evident that although the bio-availability of calcium salts in the healthy individual maybe equal, an impairment of acid secretion has a negativeeffect on the bioavailability of calcium carbonate, pre-sumably because of decreased solubility. Given the factthat calcium carbonate is the most commonly used for-mulation for calcium substitution therapy, these findingsmay partially account for the statistical correlation be-tween PPI use and the increased risk of sustaining frac-tures.
Another factor that needs to be taken into considerationwhen assessing solubility of calcium salts is the PCO2
(390). In the local milieu of the duodenum, the PCO2 canreach values of up to 300 mmHg, resulting from the
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
235Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

pancreatic secretion of bicarbonate (929). Solubility ex-periments of calcium carbonate have shown that a highPCO2 negatively affects its solubility, as the carbonateenters equilibrium with CO2 (390). Compared with othercalcium salts, the particularly low bioavailability of cal-cium carbonate in acid suppressed patients may thus be acompounded effect of reduced acid secretion and a highduodenal PCO2.
D. The Endocrine Stomach andCalcium Homeostasis
Apart from being a mere acid secretory organ, the stomachalso plays an important role as an endocrine organ. Itshould be noted that all of the aforementioned surgical orpharmacological interventions, i.e., gastrectomies, vagoto-mies, or pharmacological acid suppression therapy, will in-evitably impact the endocrine functions of the stomach. It istherefore plausible that not only the changes in intragastricpH affect the absorption of calcium, but that the dysregu-lation of the endocrine stomach is responsible for changes incalcium homeostasis. The following section will addresshow hormones that are secreted by the stomach may impactcalcium and bone homeostasis.
1. Ghrelin
Ghrelin has been discovered fairly recently (1999) by Ko-jima and colleagues and is mainly implicated in regulatingfood intake in the hypothalamus (588, 777). Ghrelin levelsare inversely correlated with body mass and elevated inconditions of fasting, such as anorexia nervosa (377). Ghre-lin is mainly synthesized and secreted in a pulsatile mannerby special neuroendocrine cells (P/D1 cells) in the fundicregion of the stomach (242, 777). The influence of ghrelinon gastric acid secretion is discussed in a separate section(see section IIB5E). A few years after its discovery, it wasshown that ghrelin can also directly affect osteoblasts (254,357, 576, 691). Ghrelin induces osteoblast proliferationand differentiation and inhibits their apoptosis (357, 576,691, 1141). It is not entirely clear whether this effect ismediated via the ghrelin surface receptor, the growth hor-mone secretagogue receptor 1a (GHS-R1a), or not. Whilethe receptor is expressed in rat and murine osteoblasts andits pharmacological inhibition abolishes the effects of ghre-lin on differentiation and proliferation, no GHS-R1amRNA could be detected in a human osteoblast cell line(254, 357, 691). It should be noted that this effect is inde-pendent of growth hormone (GH). Ghrelin serves as a po-tent stimulator of GH secretion from the pituitary gland,which in turn acts as an activator of osteoblasts through theGH/IGF-I axis. However, the observations that 1) pharma-cological inhibition of GHS-R1a attenuates the effects ofghrelin and that 2) GH-deficient rats are still sensitive toghrelin, suggest a direct effect on osteoblasts (357). In vivo,the activation of osteoblasts translates to an increase in
bone mineral density (BMD) in rat and murine models (261,357). Ghrelin also promotes the formation of new bonefollowing injury (261). For example, mice that received astandardized bone injury demonstrated 1.6 times more newbone surface if treated with ghrelin compared with controlanimals (261).
Several studies aimed to identify a link between serum ghre-lin levels and BMD in human populations. The most recent,and one of the largest (n � 707 subjects), investigationassessed BMD with peripheral quantitative computed to-mography (pQCT). This technique allows for separateanalysis of trabecular and cortical bone. The results showeda positive correlation between ghrelin and trabecular BMDin elderly men and women (775). A different large-scalestudy, investigating a similar cohort (n � 977) found noassociation using dual-energy X-ray and single-photon ab-sorptiometry (1157). These techniques, however, do notpermit a discrimination between cortical and trabecularbone. Other small-scale studies also came to contradictoryconclusions (388, 811). The reason for these discrepanciesis elusive. Since the formation of trabecular bone representsa more dynamic process, its direct measurement may bemore sensitive to subtle changes than overall bone densitymeasurement (775). Baseline plasma ghrelin levels werealso shown to be inversely correlated to type 1 collagen �C-telopeptide (�CTX), a marker for bone resorption (501).
The source of ghrelin represents another potential caveat. Invitro studies suggest that osteoblasts can also synthesizeghrelin (254, 357). Ghrelin was identified on the mRNAand protein level by two investigations (254, 357). A differ-ent group did not find evidence for ghrelin in osteoblasts(214). This has important implications, as ghrelin may besecreted in an auto-/paracrine fashion, which would makeplasma ghrelin levels less significant for osteoblast activa-tion. On the other hand, (partial) gastrectomy significantlydecreases plasma ghrelin concentrations, which could con-tribute to postgastrectomy osteopenia, although these mayjust be two independent factors. Total gastrectomy causes adrop in plasma ghrelin levels by as much as 70% (528).Partial gastrectomy also severely decreases plasma ghrelin;however, levels normalize depending on the type of resec-tion to 48–88% of the preoperative levels due to compen-satory production in the remaining gastric mucosa (528).This recovery already occurs after 7days. It thus remains tobe elucidated if the slightly decreased ghrelin levels aftersmall gastric resections can account for the long-term phe-nomenon of postgastrectomy osteopenia. Furthermore, inmice, the reduction of bone mass after gastrectomy cannotbe rescued by exogenous administration of ghrelin (277).Ghrelin administration did also not affect markers of boneresorption in gastrectomized patients, although these pa-rameters were only measured very acutely 4 h after ghrelininfusion (501). So far, no data on the effect of chronicghrelin treatment on BMD are available.
SASCHA KOPIC AND JOHN P. GEIBEL
236 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

Although decreased ghrelin levels could in theory be a con-tributing factor to the reduction of bone mass followinggastrectomy, it is unknown if PPIs can directly affect ghrelinlevels. A potential link between PPI-related fractures andghrelin levels remains to be investigated. An indirect asso-ciation may be present in patients with Helicobacter pyloriinfections. These infections represent a common indicationfor PPI intake and were suggested to coincide with reducedghrelin in plasma and the gastric mucosa (527). Given therecent discovery of ghrelin’s impact on osteoblast function,many questions still remain to be answered. It is, however,clear that our view of the stomach as a mere acid secretorypouch needs to be expanded to a new level.
2. Gastrin
Gastrin represents one of the main acid secretagogues (seesect. IIB2). It is secreted by specialized G-cells in the antrumof the stomach and the duodenum. The released gastrinenters the circulation and induces acid secretion in gastricparietal cells via the CCK2 receptor. It has been hypothe-sized fairly early that plasma gastrin may have an impact onbone metabolism. Injection of gastrin and its synthetic an-alog pentagastrin was shown to decrease plasma calciumlevels in pigs and rats in the 1970s (222, 980). This effectwas attributed to gastrin-stimulated release of calcitoninfrom the thyroid gland. Indeed, pentagastrin was shown tobe a potent stimulator of calcitonin secretion in variousspecies and is still in clinical use to evaluate thyroid C-cellhyperplasia and medullary carcinomas (155, 156, 226, 441,829). Although a clinical correlation between plasma gas-trin levels and plasma calcitonin has been demonstrated byone study in patients with Zollinger-Ellison syndrome (hy-pergastrinemic patients) and in pigs, it is unclear if nativegastrin, i.e., not pentagastrin, acts as an important secreta-gogue for calcitonin in humans (224, 1020). In fact, otherinvestigations found no association between gastrin andcalcitonin levels in other cohorts (122, 454).
At least in the rat, the hypothesis of the gastrin-calcitoninaxis has been severely challenged. Although gastrin de-creases plasma calcium levels in rats, the same effect occursin (para)thyroidectomized animals, suggesting that calci-tonin is not involved in this process (980). Furthermore,cultured rat thyroid cells could not be stimulated to releasecalcitonin if incubated with gastrin (225). Fundectomy- andomeprazole-induced hypergastrinemia also did not affectcalcitonin levels in rats (843, 927). Interestingly, hypocal-cemia after gastrin injection could not be induced in ratsthat had been (para)thyroidectomized and gastrectomized(844, 981). This observation led to the conclusion that gas-trin may stimulate the release of an unknown substancefrom the rat stomach, which in turn exerts calcitropic ac-tivity. In accordance with this hypothesis, mucosal extractsfrom rat stomachs were shown to have the same hypocal-cemic effects as gastrin and to stimulate uptake of radiola-beled calcium into the bone (844). These findings were also
replicated in chicken (842). The unknown hormone wastentatively named ”gastrocalcin“ (844). When ghrelin wasdiscovered, it was speculated that it might represent a can-didate hormone for gastrocalcin. However, unlike gastro-calcin, ghrelin is not under gastrin control, making thisproposition unlikely (276). Subsequent investigations sug-gested that the origin of gastrocalcin were the gastric ECLcells. ECL extracts can indeed trigger a calcium second mes-senger response in osteoblast (629, 630). Yet, functionalevidence for gastrocalcin-mediated osteoblast activation isstill lacking. A recent report postulates that parathyroidhormone-like hormone (PTHLH) may in fact be gastrocal-cin (676). PTHLH exerts similar physiological effects asPTH by sharing a common receptor and is commonly ele-vated in paraneoplastic syndromes (1056). PTHLH hasbeen identified in ECL cells, and its transcription has beenshown to be inducible by gastrin in parietal cells (523, 676).Of note, PTH causes effects opposite to those assigned togastrin and gastrocalcin, namely, hypercalcemia. Furtherstudies will thus be needed to corroborate this hypothesis.
Whatever the exact effector hormone of gastrin may be,changes in gastrin levels cannot entirely explain the clinicalphenomenon of postgastrectomy osteopenia and PPI-re-lated fractures. Although vagotomy and PPIs undoubtedlyincrease serum gastrin levels through a negative-feedbackmechanism, most partial and all total gastrectomies resultin hypogastrinemia. Yet both hyper- and hypogastrinemicconditions have similar outcomes, i.e., osteopenia and in-creased risks of fractures. It is, of course, plausible thatdifferent factors contribute to this outcome in each individ-ual group. Gastrin may be involved in certain pathologies,but given that its true impact on bone metabolism is some-what elusive, this assumption remains speculative.
Acid suppression
?
Gastrin
Pancreastatin Calcitonin
Calcium solubility
Intestinal absorption
PTH
FIGURE 9. Model summarizing the potential impact of acid sup-pression on calcium homeostasis.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
237Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

3. Pancreastatin
Pancreastatin is a cleavage product of chromogranin A thatwas initially isolated from porcine pancreas (1072). GastricECL cells are also known to harbor significant amounts ofchromogranin A and pancreastatin. Pancreastatin is se-creted together with histamine from ECL cells in responseto their neuroendocrine stimulation (see sect. IIB3) (176). Inrat, it has been shown that the serum pancreastatin levelscorrelate with the secretory status of ECL cells. States thatenhance ECL cell secretion, such as gastrin infusion, re-sulted in elevated serum pancreastatin levels (411). In ac-cordance with this hypothesis, and of special relevance forthe topic of this review, PPI therapy also resulted in in-creased serum pancreastatin levels (the ECL is stimulated bygastrin, which in turn is released in response to high gastricpH) (411). These observations led the investigators to con-clude that ECL cells are a major contributor to the serumlevels of pancreastatin in the rat and that these levels changein parallel with ECL cell secretion (411). This is also cor-roborated by the observation that gastrectomy reduces pan-creastatin levels in rats (644).
Pancreastatin exerts a variety of metabolic effects. Apartfrom influencing energy metabolism, pancreasstatin wasshown to affect the secretion of PTH from the parathyroidgland. In isolated bovine and porcine parathyroid cells,pancreastatin has a clear inhibitory effect on PTH secretion(282, 317, 911). The suppression of PTH functions on atranscriptional level (1211). Reduced PTH secretion in turnwould have a potential impact on calcium and bone metab-olism. Whether the same observations are valid for humansis less clear, as pancreastatin failed to inhibit PTH secretionfrom isolated human parathyroid cells (911). Regardless,the volume of data on pancreastatin and its influence on theparathyroid gland is very small, and further investigationswould be necessary to establish this intriguing link. Apartfrom potential modulation of parathyroid secretion, pan-creastatin has also been shown to have an inhibitory effecton gastric acid secretion (655).
In summary, it should be noted that the stomach secretesnot only acid, but also hormones that have been shown todirectly alter calcium and/or bone homeostasis. The secre-tion of these hormones depends on the neuroendocrine ma-chinery that also regulates acid secretion. It is thereforeplausible that the correlation between states of impairedacid secretion and impaired bone mineralization is multi-factorial by depending on intragastric pH and serum levelsof gastric hormones (FIGURE 9).
VI. CONCLUSIONS
We set out in this review to demonstrate that gastric andintestinal physiology are intertwined to regulate calciumabsorption and secretion to maintain bone health. In this
review we have focused on the important role calcium playsas a first and second messenger in the maintenance of bonehealth. By relying on a complex series of receptors, chan-nels, and transport proteins, calcium is tightly controlled atthe cellular and tissue level to ensure its bioavailability tobone. Modulations to any of these pathways by disease,mutation, or pharmaceutical perturbation can lead to clin-ical changes in bone health.
ACKNOWLEDGMENTS
S. Kopic is a Howard Hughes Medical Institute Interna-tional Student Research Fellow. Special thanks to SashkaDimitrievska for her untiring support and critical editing ofthe manuscript.
Address for reprint requests and other correspondence: J. P.Geibel, Yale School of Medicine, 310 Cedar St., BML 238,New Haven, CT 06510 (e-mail: [email protected]).
DISCLOSURES
No conflicts of interest, financial or otherwise, are declaredby the authors.
REFERENCES
1. Abe K, Kaya S, Taniguchi K, Hayashi Y, Imagawa T, Kikumoto M, Oiwa K, SakaguchiK. Evidence for a relationship between activity and the tetraprotomeric assembly ofsolubilized pig gastric H/K-ATPase. J Biochem 138: 293–301, 2005.
2. Abe K, Tani K, Fujiyoshi Y. Conformational rearrangement of gastric H�,K�-ATPaseinduced by an acid suppressant. Nat Commun 2: 155, 2011.
3. Abe K, Tani K, Fujiyoshi Y. Structural and functional characterization of H�,K�-ATPase with bound fluorinated phosphate analogs. J Struct Biol 170: 60–68, 2010.
4. Abe K, Tani K, Nishizawa T, Fujiyoshi Y. Inter-subunit interaction of gastric H�,K�-ATPase prevents reverse reaction of the transport cycle. EMBO J 28: 1637–1643,2009.
5. Abou-Samra AB, Juppner H, Force T, Freeman MW, Kong XF, Schipani E, Urena P,Richards J, Bonventre JV, Potts JT Jr. Expression cloning of a common receptor forparathyroid hormone and parathyroid hormone-related peptide from rat osteo-blast-like cells: a single receptor stimulates intracellular accumulation of both cAMPand inositol trisphosphates and increases intracellular free calcium. Proc Natl Acad SciUSA 89: 2732–2736, 1992.
6. Abreo K, Adlakha A, Kilpatrick S, Flanagan R, Webb R, Shakamuri S. The milk-alkalisyndrome. A reversible form of acute renal failure. Arch Intern Med 153: 1005–1010,1993.
7. Adams JS, Clemens TL, Parrish JA, Holick MF. Vitamin-D synthesis and metabolismafter ultraviolet irradiation of normal and vitamin-D-deficient subjects. N Engl J Med306: 722–725, 1982.
8. Agnew JE, Holdsworth CD. The effect of fat on calcium absorption from a mixedmeal in normal subjects, patients with malabsorptive disease, and patients with apartial gastrectomy. Gut 12: 973–977, 1971.
9. Aihara T, Fujishita T, Kanatani K, Furutani K, Nakamura E, Taketo MM, Matsui M,Chen D, Okabe S. Impaired gastric secretion and lack of trophic responses tohypergastrinemia in M3 muscarinic receptor knockout mice. Gastroenterology 125:1774–1784, 2003.
SASCHA KOPIC AND JOHN P. GEIBEL
238 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

10. Aihara T, Nakamura Y, Taketo MM, Matsui M, Okabe S. Cholinergically stimulatedgastric acid secretion is mediated by M3 and M5 but not M1 muscarinic acetylcholinereceptors in mice. Am J Physiol Gastrointest Liver Physiol 288: G1199–G1207, 2005.
11. Akeno N, Saikatsu S, Kawane T, Horiuchi N. Mouse vitamin D-24-hydroxylase:molecular cloning, tissue distribution, transcriptional regulation by 1alpha,25-dihy-droxyvitamin D3. Endocrinology 138: 2233–2240, 1997.
12. Akey JM, Swanson WJ, Madeoy J, Eberle M, Shriver MD. TRPV6 exhibits unusualpatterns of polymorphism and divergence in worldwide populations. Hum Mol Genet15: 2106–2113, 2006.
13. Akhter S, Kutuzova GD, Christakos S, DeLuca HF. Calbindin D9k is not required for1,25-dihydroxyvitamin D3-mediated Ca2� absorption in small intestine. Arc BiochemBiophys 460: 227–232, 2007.
14. Akiyoshi-Shibata M, Sakaki T, Ohyama Y, Noshiro M, Okuda K, Yabusaki Y. Furtheroxidation of hydroxycalcidiol by calcidiol 24-hydroxylase. A study with the matureenzyme expressed in Escherichia coli. Eur J Biochem 224: 335–343, 1994.
15. Al-Ansary D, Bogeski I, Disteldorf BMJ, Becherer U, Niemeyer BA. ATP modulatesCa2� uptake by TRPV6 and is counteracted by isoform-specific phosphorylation.FASEB J 24: 425–435, 2010.
16. Alam AS, Moonga BS, Bevis PJ, Huang CL, Zaidi M. Amylin inhibits bone resorptionby a direct effect on the motility of rat osteoclasts. Exp Physiol 78: 183–196, 1993.
17. Albrandt K, Brady EM, Moore CX, Mull E, Sierzega ME, Beaumont K. Molecularcloning and functional expression of a third isoform of the human calcitonin receptorand partial characterization of the calcitonin receptor gene. Endocrinology 136:5377–5384, 1995.
18. Allen LH. Calcium bioavailability and absorption: a review. Am J Clin Nutr 35: 783–808, 1982.
19. Alumets J, Ekelund M, El Munshid HA, Hakanson R, Loren I, Sundler F. Topographyof somatostatin cells in the stomach of the rat: possible functional significance. CellTissue Res 202: 177–188, 1979.
20. Aly A, Shulkes A, Baldwin GS. Short term infusion of glycine-extended gastrin(17)stimulates both proliferation and formation of aberrant crypt foci in rat colonicmucosa. Int J Cancer 94: 307–313, 2001.
21. Amling M, Priemel M, Holzmann T, Chapin K, Rueger JM, Baron R, Demay MB.Rescue of the skeletal phenotype of vitamin D receptor-ablated mice in the setting ofnormal mineral ion homeostasis: formal histomorphometric and biomechanical anal-yses. Endocrinology 140: 4982–4987, 1999.
22. Andersen BN. Species variation in the tyrosine sulfation of mammalian gastrins. GenComp Endocrinol 58: 44–50, 1985.
23. Anderson NG, Hanson PJ. Involvement of calcium-sensitive phospholipid-depen-dent protein kinase in control of acid secretion by isolated rat parietal cells. BiochemJ 232: 609–611, 1985.
24. Andersson K, Cabero JL, Mattsson H, Hakanson R. Gastric acid secretion afterdepletion of enterochromaffin-like cell histamine. A study with alpha-fluoromethyl-histidine in rats. Scand J Gastroenterol 31: 24–30, 1996.
25. Andersson S, Chang D, Folkers K, Rosell S. Inhibition of gastric acid secretion in dogsby neurotensin. Life Sci 19: 367–370, 1976.
26. Andersson S, Davis DL, Dahlback H, Jornvall H, Russell DW. Cloning, structure, andexpression of the mitochondrial cytochrome P-450 sterol 26-hydroxylase, a bile acidbiosynthetic enzyme. J Biol Chem 264: 8222–8229, 1989.
27. Andreassen TT, Ejersted C, Oxlund H. Intermittent parathyroid hormone (1–34)treatment increases callus formation and mechanical strength of healing rat frac-tures. J Bone Miner Res 14: 960–968, 1999.
28. Andreotti G, Mendez BL, Amodeo P, Morelli MA, Nakamuta H, Motta A. Structuraldeterminants of salmon calcitonin bioactivity: the role of the Leu-based amphipathicalpha-helix. J Biol Chem 281: 24193–24203, 2006.
29. Anisuzzaman AS, Morishima S, Suzuki F, Tanaka T, Muramatsu I. Identification ofM(1) muscarinic receptor subtype in rat stomach using a tissue segment bindingmethod, the effects of immobilization stress on the muscarinic receptors. Eur JPharmacol 599: 146–151, 2008.
30. Anusaksathien O, Laplace C, Li X, Ren Y, Peng L, Goldring SR, Galson DL. Tissue-specific and ubiquitous promoters direct the expression of alternatively spliced tran-scripts from the calcitonin receptor gene. J Biol Chem 276: 22663–22674, 2001.
31. Ardaillou R. Kidney and calcitonin. Nephron 15: 250–260, 1975.
32. Ardaillou R, Vuagnat P, Milhaud G, Richet G. Effects of thyrocalcitonin on the renalexcretion of phosphates, calcium and hydrogen ions in man. Nephron 4: 298–314,1967.
33. Aris RM, Lester GE, Dingman S, Ontjes DA. Altered calcium homeostasis in adultswith cystic fibrosis. Osteoporos Int 10: 102–108, 1999.
34. Arman E, Nilsson LH, Reizenstein P. Studies in the dumping syndrome. VI. Calciumdeficiency after partial gastrectomy. Am J Dig Dis 15: 455–462, 1970.
35. Armbrecht HJ, Boltz MA, Kumar VB. Intestinal plasma membrane calcium pumpprotein and its induction by 1,25(OH)2D3 decrease with age. Am J Physiol Gastroin-test Liver Physiol 277: G41–G47, 1999.
36. Armbrecht HJ, Boltz MA, Wongsurawat N. Expression of plasma membrane calciumpump mRNA in rat intestine: effect of age and 1,25-dihydroxyvitamin D. BiochimBiophys Acta 1195: 110–114, 1994.
37. Armbrecht HJ, Hodam TL, Boltz MA, Partridge NC, Brown AJ, Kumar VB. Inductionof the vitamin D 24-hydroxylase (CYP24) by 1,25-dihydroxyvitamin D3 is regulatedby parathyroid hormone in UMR106 osteoblastic cells. Endocrinology 139: 3375–3381, 1998.
38. Arnold A, Horst SA, Gardella TJ, Baba H, Levine MA, Kronenberg HM. Mutation ofthe signal peptide-encoding region of the preproparathyroid hormone gene in famil-ial isolated hypoparathyroidism. J Clin Invest 86: 1084–1087, 1990.
39. Arnold R, Koop H, Schwarting H, Tuch K, Willemer B. Effect of acid inhibition ongastric endocrine cells. Scand J Gastroenterol Suppl 125: 14–19, 1986.
40. Arthur JM, Collinsworth GP, Gettys TW, Quarles LD, Raymond JR. Specific couplingof a cation-sensing receptor to G protein �-subunits in MDCK cells. Am J PhysiolRenal Physiol 273: F129–F135, 1997.
41. Asano S, Kawada K, Kimura T, Grishin AV, Caplan MJ, Takeguchi N. The roles ofcarbohydrate chains of the beta-subunit on the functional expression of gastricH�,K�-ATPase. J Biol Chem 275: 8324–8330, 2000.
42. Asano S, Yoshida A, Yashiro H, Kobayashi Y, Morisato A, Ogawa H, Takeguchi N,Morii M. The cavity structure for docking the K�-competitive inhibitors in the gastricproton pump. J Biol Chem 279: 13968–13975, 2004.
43. Askew FA, Bruce HM, Callow RK, Philpot JS, Webster TA. Crystalline vitamin D.Nature 128: 758, 1931.
44. Athmann C, Zeng N, Scott DR, Sachs G. Regulation of parietal cell calcium signalingin gastric glands. Am J Physiol Gastrointest Liver Physiol 279: G1048–G1058, 2000.
45. Atkins GJ, Anderson PH, Findlay DM, Welldon KJ, Vincent C, Zannettino AC,O’Loughlin PD, Morris HA. Metabolism of vitamin D3 in human osteoblasts: evi-dence for autocrine and paracrine activities of 1 alpha,25-dihydroxyvitamin D3. Bone40: 1517–1528, 2007.
46. Auchere D, Tardivel S, Gounelle JC, Drueke T, Lacour B. Role of transcellularpathway in ileal Ca2� absorption: stimulation by low-Ca2� diet. Am J Physiol Gastro-intest Liver Physiol 275: G951–G956, 1998.
47. Auer J, Reeh PW, Fischer MJ. Acid-induced CGRP release from the stomach does notdepend on TRPV1 or ASIC3. Neurogastroenterol Motil 22: 680–687, 2010.
48. Awata H, Huang C, Handlogten ME, Miller RT. Interaction of the calcium-sensingreceptor and filamin, a potential scaffolding protein. J Biol Chem 276: 34871–34879,2001.
49. Axelson J, Persson P, Gagnemo-Persson R, Hakanson R. Importance of the stomachin maintaining calcium homoeostasis in the rat. Gut 32: 1298–1302, 1991.
50. Axen E, Postlind H, Sjoberg H, Wikvall K. Liver mitochondrial cytochrome P450CYP27 and recombinant-expressed human CYP27 catalyze 1�-hydroxylation of25-hydroxyvitamin D3. Proc Natl Acad Sci USA 91: 10014–10018, 1994.
51. Axen E, Postlind H, Wikvall K. Effects on CYP27 mRNA expression in rat kidney andliver by 1�,25-dihydroxyvitamin D3, a suppressor of renal 25-hydroxyvitamin D3
1�-hydroxylase activity. Biochem Biophys Res Commun 215: 136–141, 1995.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
239Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

52. Ba J, Brown D, Friedman PA. Calcium-sensing receptor regulation of PTH-inhibit-able proximal tubule phosphate transport. Am J Physiol Renal Physiol 285: F1233–F1243, 2003.
53. Bado A, Cloarec D, Moizo L, Laigneau JP, Bataille D, Lewin MJ. Neurotensin andoxyntomodulin-(30–37) potentiate PYY regulation of gastric acid and somatostatinsecretions. Am J Physiol Gastrointest Liver Physiol 265: G113–G117, 1993.
54. Bai M, Trivedi S, Brown EM. Dimerization of the extracellular calcium-sensing re-ceptor (CaR) on the cell surface of CaR-transfected HEK293 cells. J Biol Chem 273:23605–23610, 1998.
55. Bai M, Trivedi S, Kifor O, Quinn SJ, Brown EM. Intermolecular interactions betweendimeric calcium-sensing receptor monomers are important for its normal function.Proc Natl Acad Sci USA 96: 2834–2839, 1999.
56. Bai M, Trivedi S, Lane CR, Yang Y, Quinn SJ, Brown EM. Protein kinase C phosphor-ylation of threonine at position 888 in Ca2�
o-sensing receptor (CaR) inhibits cou-pling to Ca2� store release. J Biol Chem 273: 21267–21275, 1998.
57. Bailey RL, Dodd KW, Goldman JA, Gahche JJ, Dwyer JT, Moshfegh AJ, Sempos CT,Picciano MF. Estimation of total usual calcium and vitamin D intakes in the UnitedStates. J Nutr 140: 817–822, 2010.
58. Baird IM, Oleesky S. Osteomalacia following gastric surgery. Gastroenterology 33:284–292, 1957.
59. Baker AR, McDonnell DP, Hughes M, Crisp TM, Mangelsdorf DJ, Haussler MR, PikeJW, Shine J, O’Malley BW. Cloning and expression of full-length cDNA encodinghuman vitamin D receptor. Proc Natl Acad Sci USA 85: 3294–3298, 1988.
60. Bakke I, Qvigstad G, Brenna E, Sandvik AK, Waldum HL. Gastrin has a specificproliferative effect on the rat enterochromaffin-like cell, but not on the parietal cell:a study by elutriation centrifugation. Acta Physiol Scand 169: 29–37, 2000.
61. Baldissera FG, Nielsen OV, Holst JJ. The intestinal mucosa preferentially releasessomatostatin-28 in pigs. Regul Pept 11: 251–262, 1985.
62. Balesaria S, Sangha S, Walters JR. Human duodenum responses to vitamin D metab-olites of TRPV6 and other genes involved in calcium absorption. Am J Physiol Gastro-intest Liver Physiol 297: G1193–G1197, 2009.
63. Barger G, Dale HH. The presence in ergot and physiological activity of beta-imida-zolylethylamine. J Physiol 40: xxxviii-xl, 1910.
64. Barley NF, Howard A, O’Callaghan D, Legon S, Walters JR. Epithelial calcium trans-porter expression in human duodenum. Am J Physiol Gastrointest Liver Physiol 280:G285–G290, 2001.
65. Basso D, Scrigner M, Toma A, Navaglia F, Di Mario F, Rugge M, Plebani M. Helico-bacter pylori infection enhances mucosal interleukin-1 beta, interleukin-6, the solublereceptor of interleukin-2. Int J Clin Lab Res 26: 207–210, 1996.
66. Bataille D, Blache P, Mercier F, Jarrousse C, Kervran A, Dufour M, Mangeat P,Dubrasquet M, Mallat A, Lotersztajn S. Glucagon and related peptides Molecularstructure and biological specificity. Ann NY Acad Sci 527: 168–185, 1988.
67. Batzri S, Gardner JD. Cellular cyclic AMP in dispersed mucosal cells from guinea pigstomach. Biochim Biophys Acta 541: 181–189, 1978.
68. Bayliss WM, Starling EH. The mechanism of pancreatic secretion. J Physiol 28: 325–353, 1902.
69. Beales IL, Calam J. Inhibition of carbachol stimulated acid secretion by interleukin1beta in rabbit parietal cells requires protein kinase C. Gut 48: 782–789, 2001.
70. Beales IL, Calam J. Interleukin 1 beta and tumour necrosis factor alpha inhibit acidsecretion in cultured rabbit parietal cells by multiple pathways. Gut 42: 227–234,1998.
71. Beales IL, Ogunwobi OO. Glycine-extended gastrin inhibits apoptosis in Barrett’soesophageal and oesophageal adenocarcinoma cells through JAK2/STAT3 activa-tion. J Mol Endocrinol 42: 305–318, 2009.
72. Beck L, Karaplis AC, Amizuka N, Hewson AS, Ozawa H, Tenenhouse HS. Targetedinactivation of Npt2 in mice leads to severe renal phosphate wasting, hypercalciuria,and skeletal abnormalities. Proc Natl Acad Sci USA 95: 5372–5377, 1998.
73. Beil W, Mannschedel W, Sewing KF. Protein kinase C and parietal cell function.Biochem Biophys Res Commun 149: 720–728, 1987.
74. Bell NJ, Burget D, Howden CW, Wilkinson J, Hunt RH. Appropriate acid suppressionfor the management of gastro-oesophageal reflux disease. Digestion 51 Suppl 1:59–67, 1992.
75. Bellido T, Ali AA, Plotkin LI, Fu Q, Gubrij I, Roberson PK, Weinstein RS, O’Brien CA,Manolagas SC, Jilka RL. Proteasomal degradation of Runx2 shortens parathyroidhormone-induced anti-apoptotic signaling in osteoblasts. A putative explanation forwhy intermittent administration is needed for bone anabolism. J Biol Chem 278:50259–50272, 2003.
76. Benn BS, Ajibade D, Porta A, Dhawan P, Hediger M, Peng JB, Jiang Y, Oh GT, JeungEB, Lieben L, Bouillon R, Carmeliet G, Christakos S. Active intestinal calcium trans-port in the absence of transient receptor potential vanilloid type 6 and calbindin-D9k. Endocrinology 149: 3196–3205, 2008.
77. Benoit R, Ling N, Esch F. A new prosomatostatin-derived peptide reveals a patternfor prohormone cleavage at monobasic sites. Science 238: 1126–1129, 1987.
78. Beresford JN, Bennett JH, Devlin C, Leboy PS, Owen ME. Evidence for an inverserelationship between the differentiation of adipocytic and osteogenic cells in ratmarrow stromal cell cultures. J Cell Sci 102: 341–351, 1992.
79. Beresford JN, Joyner CJ, Devlin C, Triffitt JT. The effects of dexamethasone and1,25-dihydroxyvitamin D3 on osteogenic differentiation of human marrow stromalcells in vitro. Arch Oral Biol 39: 941–947, 1994.
80. Berg A, Kechagias S, Sjostrand SE, Ericson AC. Morphological support for paracrineinhibition of gastric acid secretion by nitric oxide in humans. Scand J Gastroenterol 36:1016–1021, 2001.
81. Berg A, Redeen S, Ericson AC, Sjostrand SE. Nitric oxide-an endogenous inhib-itor of gastric acid secretion in isolated human gastric glands. BMC Gastroenterol4: 16, 2004.
82. Berg A, Redeen S, Grenegard M, Ericson AC, Sjostrand SE. Nitric oxide inhibitsgastric acid secretion by increasing intraparietal cell levels of cGMP in isolated humangastric glands. Am J Physiol Gastrointest Liver Physiol 289: G1061–G1066, 2005.
83. Berginer VM, Shany S, Alkalay D, Berginer J, Dekel S, Salen G, Tint GS, Gazit D.Osteoporosis and increased bone fractures in cerebrotendinous xanthomatosis.Metabolism 42: 69–74, 1993.
84. Berndt TJ, Knox FG. Effects of parathyroid hormone and calcitonin on electrolyteexcretion in the rabbit. Kidney Int 17: 473–478, 1980.
85. Bers DM, Ginsburg KS. Na:Ca stoichiometry and cytosolic Ca-dependent activationof NCX in intact cardiomyocytes. Ann NY Acad Sci 1099: 326–338, 2007.
86. Berthoud HR. Morphological analysis of vagal input to gastrin releasing peptide andvasoactive intestinal peptide containing neurons in the rat glandular stomach. J CompNeurol 370: 61–70, 1996.
87. Bertrand C, Kowalski-Chauvel A, Do C, Resa C, Najib S, Daulhac L, Wang TC,Ferrand A, Seva C. A gastrin precursor, gastrin-gly, upregulates VEGF expression incolonic epithelial cells through an HIF-1-independent mechanism. Int J Cancer 126:2847–2857, 2010.
88. Bertrand CA, Zhang R, Pilewski JM, Frizzell RA. SLC26A9 is a constitutively active,CFTR-regulated anion conductance in human bronchial epithelia. J Gen Physiol 133:421–438, 2009.
89. Besancon M, Shin JM, Mercier F, Munson K, Miller M, Hersey S, Sachs G. Membranetopology and omeprazole labeling of the gastric H�,K�-adenosinetriphosphatase.Biochemistry 32: 2345–2355, 1993.
90. Besancon M, Simon A, Sachs G, Shin JM. Sites of reaction of the gastric H�-K�-ATPase with extracytoplasmic thiol reagents. J Biol Chem 272: 22438–22446, 1997.
91. Bhattacharyya MH, DeLuca HF. The regulation of calciferol-25-hydroxylase in thechick. Biochem Biophys Res Commun 59: 734–741, 1974.
92. Bhattacharyya MH, DeLuca HF. The regulation of rat liver calciferol-25-hydroxylase.J Biol Chem 248: 2969–2973, 1973.
93. Bhattacharyya MH, DeLuca HF. Subcellular location of rat liver calciferol-25-hydrox-ylase. Arch Biochem Biophys 160: 58–62, 1974.
94. Bianco SD, Peng JB, Takanaga H, Suzuki Y, Crescenzi A, Kos CH, Zhuang L, FreemanMR, Gouveia CH, Wu J, Luo H, Mauro T, Brown EM, Hediger MA. Marked distur-
SASCHA KOPIC AND JOHN P. GEIBEL
240 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

bance of calcium homeostasis in mice with targeted disruption of the Trpv6 calciumchannel gene. J Bone Miner Res 22: 274–285, 2007.
95. Bieglmayer C, Prager G, Niederle B. Kinetic analyses of parathyroid hormone clear-ance as measured by three rapid immunoassays during parathyroidectomy. ClinChem 48: 1731–1738, 2002.
96. Bielefeldt K, Davis BM. Differential effects of ASIC3 and TRPV1 deletion on gastro-esophageal sensation in mice. Am J Physiol Gastrointest Liver Physiol 294: G130–G138,2008.
97. Bikle DD, Gee E, Halloran B, Haddad JG. Free 1,25-dihydroxyvitamin D levels inserum from normal subjects, pregnant subjects, and subjects with liver disease. J ClinInvest 74: 1966–1971, 1984.
98. Bikle DD, Gee E, Halloran B, Kowalski MA, Ryzen E, Haddad JG. Assessment of thefree fraction of 25-hydroxyvitamin D in serum and its regulation by albumin and thevitamin D-binding protein. J Clin Endocrinol Metab 63: 954–959, 1986.
99. Bindels RJ, Hartog A, Timmermans J, Van Os CH. Active Ca2� transport in primarycultures of rabbit kidney CCD: stimulation by 1,25-dihydroxyvitamin D3 and PTH.Am J Physiol Renal Fluid Electrolyte Physiol 261: F799–F807, 1991.
100. Birge SJ, Gilbert HR. Indentification of an intestinal sodium and calcium-dependentphosphatase stimulated by parathyroid hormone. J Clin Invest 54: 710–717, 1974.
101. Bisballe S, Eriksen EF, Melsen F, Mosekilde L, Sorensen OH, Hessov I. Osteopeniaand osteomalacia after gastrectomy: interrelations between biochemical markers ofbone remodelling, vitamin D metabolites, and bone histomorphometry. Gut 32:1303–1307, 1991.
102. Bjorkhem I, Hansson R, Holmberg I, Wikvall K. 25-Hydroxylation of vitamin D3 by areconstituted system from rat liver microsomes. Biochem Biophys Res Commun 90:615–622, 1979.
103. Bjorkhem I, Holmberg I. Assay and properties of a mitochondrial 25-hydroxylaseactive on vitamine D3. J Biol Chem 253: 842–849, 1978.
104. Bjorkhem I, Holmberg I, Oftebro H, Pedersen JI. Properties of a reconstitutedvitamin D3 25-hydroxylase from rat liver mitochondria. J Biol Chem 255: 5244–5249,1980.
105. Bjorkqvist M, Bernsand M, Eliasson L, Hakanson R, Lindstrom E. Somatostatin,misoprostol and galanin inhibit gastrin- and PACAP-stimulated secretion of hista-mine and pancreastatin from ECL cells by blocking specific Ca2� channels. Regul Pept130: 81–90, 2005.
106. Black JW, Duncan WA, Durant CJ, Ganellin CR, Parsons EM. Definition and antag-onism of histamine H2-receptors. Nature 236: 385–390, 1972.
107. Black JW, Fisher EW, Smith AN. The effects of 5-hydroxytryptamine on gastricsecretion in anaesthetized dogs. J Physiol 141: 27–34, 1958.
108. Blackburn AM, Fletcher DR, Bloom SR, Christofides ND, Long RG, Fitzpatrick ML,Baron JH. Effect of neurotensin on gastric function in man. Lancet 1: 987–989, 1980.
109. Bland R, Walker EA, Hughes SV, Stewart PM, Hewison M. Constitutive expression of25-hydroxyvitamin D3-1alpha-hydroxylase in a transformed human proximal tubulecell line: evidence for direct regulation of vitamin D metabolism by calcium. Endo-crinology 140: 2027–2034, 1999.
110. Blichert-Toft M, Beck A, Christiansen C, Transbol I. Effects of gastric resection andvagotomy on blood and bone mineral content. World J Surg 3: 99–102, 133–105,1979.
111. Blunt JW, DeLuca HF. The synthesis of 25-hydroxycholecalciferol. A biologicallyactive metabolite of vitamin D3. Biochemistry 8: 671–675, 1969.
112. Blunt JW, DeLuca HF, Schnoes HK. 25-Hydroxycholecalciferol. A biologically activemetabolite of vitamin D3. Biochemistry 7: 3317–3322, 1968.
113. Boel E, Vuust J, Norris F, Norris K, Wind A, Rehfeld JF, Marcker KA. Molecularcloning of human gastrin cDNA: evidence for evolution of gastrin by gene duplica-tion. Proc Natl Acad Sci USA 80: 2866–2869, 1983.
114. Bohmer C, Palmada M, Kenngott C, Lindner R, Klaus F, Laufer J, Lang F. Regulationof the epithelial calcium channel TRPV6 by the serum and glucocorticoid-induciblekinase isoforms SGK1 and SGK3. FEBS Lett 581: 5586–5590, 2007.
115. Boivin G, Mesguich P, Pike JW, Bouillon R, Meunier PJ, Haussler MR, Dubois PM,Morel G. Ultrastructural immunocytochemical localization of endogenous 1,25-di-hydroxyvitamin D3 and its receptors in osteoblasts and osteocytes from neonatalmouse and rat calvaria. Bone Miner 3: 125–136, 1987.
116. Booth BE, Tsai HC, Morris RC Jr. Vitamin D status regulates 25-hydroxyvitaminD3-1 alpha-hydroxylase and its responsiveness to parathyroid hormone in the chick.J Clin Invest 75: 155–161, 1985.
117. Borthwick LA, Neal A, Hobson L, Gerke V, Robson L, Muimo R. The annexin2–S100A10 complex and its association with TRPV6 is regulated by cAMP/PKA/CnAin airway and gut epithelia. Cell Calcium 44: 147–157, 2008.
118. Bosl MR, Stein V, Hubner C, Zdebik AA, Jordt SE, Mukhopadhyay AK, Davidoff MS,Holstein AF, Jentsch TJ. Male germ cells and photoreceptors, both dependent onclose cell-cell interactions, degenerate upon ClC-2 Cl� channel disruption. EMBO J20: 1289–1299, 2001.
119. Bouley R, Lu HA, Nunes P, Da Silva N, McLaughlin M, Chen Y, Brown D. Calcitoninhas a vasopressin-like effect on aquaporin-2 trafficking and urinary concentration. JAm Soc Nephrol 22: 59–72, 2011.
120. Bourdeau A, Moutahir M, Souberbielle JC, Bonnet P, Herviaux P, Sachs C, Lieber-herr M. Effects of lipoxygenase products of arachidonate metabolism on parathyroidhormone secretion. Endocrinology 135: 1109–1112, 1994.
121. Bourdeau A, Souberbielle JC, Bonnet P, Herviaux P, Sachs C, Lieberherr M. Phos-pholipase-A2 action and arachidonic acid metabolism in calcium-mediated parathy-roid hormone secretion. Endocrinology 130: 1339–1344, 1992.
122. Brandsborg M, Nielsen HE, Brandsborg O, Olsen KJ, Lovgreen NA. The role ofserum gastrin in the secretion of calcitonin: studies in patients with pernicious anae-mia and in healthy subjects. Scand J Gastroenterol 15: 23–28, 1980.
123. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hipfractures in the United States. JAMA 302: 1573–1579, 2009.
124. Brazeau P, Vale W, Burgus R, Ling N, Butcher M, Rivier J, Guillemin R. Hypothalamicpolypeptide that inhibits the secretion of immunoreactive pituitary growth hor-mone. Science 179: 77–79, 1973.
125. Brenza HL, DeLuca HF. Regulation of 25-hydroxyvitamin D3 1alpha-hydroxylasegene expression by parathyroid hormone and 1,25-dihydroxyvitamin D3. ArchBiochem Biophys 381: 143–152, 2000.
126. Brewer HB Jr, Ronan R. Bovine parathyroid hormone: amino acid sequence. ProcNatl Acad Sci USA 67: 1862–1869, 1970.
127. Bringhurst FR, Stern AM, Yotts M, Mizrahi N, Segre GV, Potts JT Jr. Peripheralmetabolism of PTH: fate of biologically active amino terminus in vivo. Am J PhysiolEndocrinol Metab 255: E886–E893, 1988.
128. Brommage R. Measurement of calcium and phosphorus fluxes during lactation in therat. J Nutr 119: 428–438, 1989.
129. Bronner F, Pansu D, Stein WD. An analysis of intestinal calcium transport across therat intestine. Am J Physiol Gastrointest Liver Physiol 250: G561–G569, 1986.
130. Brossard JH, Cloutier M, Roy L, Lepage R, Gascon-Barre M, D’Amour P. Accumu-lation of a non-(1–84) molecular form of parathyroid hormone (PTH) detected byintact PTH assay in renal failure: importance in the interpretation of PTH values. JClin Endocrinol Metab 81: 3923–3929, 1996.
131. Brossard JH, Whittom S, Lepage R, D’Amour P. Carboxyl-terminal fragments ofparathyroid hormone are not secreted preferentially in primary hyperparathyroid-ism as they are in other hypercalcemic conditions. J Clin Endocrinol Metab 77: 413–419, 1993.
132. Brown AJ, Krits I, Armbrecht HJ. Effect of age, vitamin D, and calcium on theregulation of rat intestinal epithelial calcium channels. Arch Biochem Biophys 437:51–58, 2005.
133. Brown E, Enyedi P, LeBoff M, Rotberg J, Preston J, Chen C. High extracellular Ca2�
and Mg2� stimulate accumulation of inositol phosphates in bovine parathyroid cells.FEBS Lett 218: 113–118, 1987.
134. Brown EM, Gamba G, Riccardi D, Lombardi M, Butters R, Kifor O, Sun A, HedigerMA, Lytton J, Hebert SC. Cloning and characterization of an extracellular Ca2�-sensing receptor from bovine parathyroid. Nature 366: 575–580, 1993.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
241Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

135. Brown J 3rd, Theisler C, Silberman S, Magnuson D, Gottardi-Littell N, Lee JM, YagerD, Crowley J, Sambamurti K, Rahman MM, Reiss AB, Eckman CB, Wolozin B.Differential expression of cholesterol hydroxylases in Alzheimer’s disease. J BiolChem 279: 34674–34681, 2004.
136. Brown MR, Chew CS. Multiple effects of phorbol ester on secretory activity in rabbitgastric glands and parietal cells. Can J Physiol Pharmacol 65: 1840–1847, 1987.
137. Bruley des Varannes S, Levy P, Lartigue S, Dellatolas F, Lemaire M, Galmiche JP.Comparison of lansoprazole with omeprazole on 24-hour intragastric pH, acid se-cretion and serum gastrin in healthy volunteers. Aliment Pharmacol Ther 8: 309–314,1994.
138. Bruns ME, Fleisher EB, Avioli LV. Control of vitamin D-dependent calcium-bindingprotein in rat intestine by growth and fasting. J Biol Chem 252: 4145–4150, 1977.
139. Bu FX, Armas L, Lappe J, Zhou Y, Gao G, Wang HW, Recker R, Zhao LJ. Compre-hensive association analysis of nine candidate genes with serum 25-hydroxy vitaminD levels among healthy Caucasian subjects. Hum Genet 128: 549–556, 2010.
140. Buchan AM, MacLeod MD, Meloche RM, Kwok YN. Muscarinic regulation of soma-tostatin release from primary cultures of human antral epithelial cells. Pharmacology44: 33–40, 1992.
141. Buchan AM, Meloche RM, Kwok YN, Kofod H. Effect of cholecystokinin and secretinon somatostatin release from cultured antral cells. Gastroenterology 104: 1414–1419, 1993.
142. Buchan AM, Squires PE, Ring M, Meloche RM. Mechanism of action of the calcium-sensing receptor in human antral gastrin cells. Gastroenterology 120: 1128–1139,2001.
143. Buclin T, Cosma Rochat M, Burckhardt P, Azria M, Attinger M. Bioavailability andbiological efficacy of a new oral formulation of salmon calcitonin in healthy volun-teers. J Bone Miner Res 17: 1478–1485, 2002.
144. Bugrim AE. Regulation of Ca2� release by cAMP-dependent protein kinase. A mech-anism for agonist-specific calcium signaling? Cell Calcium 25: 219–226, 1999.
145. Busque SM, Kerstetter JE, Geibel JP, Insogna K. L-type amino acids stimulate gastricacid secretion by activation of the calcium-sensing receptor in parietal cells. Am JPhysiol Gastrointest Liver Physiol 289: G664–G669, 2005.
146. Cai Q, Chandler JS, Wasserman RH, Kumar R, Penniston JT. Vitamin D and adapta-tion to dietary calcium and phosphate deficiencies increase intestinal plasma mem-brane calcium pump gene expression. Proc Natl Acad Sci USA 90: 1345–1349, 1993.
147. Calhoun BC, Lapierre LA, Chew CS, Goldenring JR. Rab11a redistributes to apicalsecretory canaliculus during stimulation of gastric parietal cells. Am J Physiol CellPhysiol 275: C163–C170, 1998.
148. Cali JJ, Hsieh CL, Francke U, Russell DW. Mutations in the bile acid biosyntheticenzyme sterol 27-hydroxylase underlie cerebrotendinous xanthomatosis. J BiolChem 266: 7779–7783, 1991.
149. Cali JJ, Russell DW. Characterization of human sterol 27-hydroxylase. A mitochon-drial cytochrome P-450 that catalyzes multiple oxidation reaction in bile acid biosyn-thesis. J Biol Chem 266: 7774–7778, 1991.
150. Calvo MS, Whiting SJ, Barton CN. Vitamin D intake: a global perspective of currentstatus. J Nutr 135: 310–316, 2005.
151. Canadillas S, Canalejo R, Rodriguez-Ortiz ME, Martinez-Moreno JM, Estepa JC,Zafra R, Perez J, Munoz-Castaneda JR, Canalejo A, Rodriguez M, Almaden Y. Theup-regulation of the parathyroid VDR expression by extracellular calcium is medi-ated by the ERK1/2-MAPK signaling pathway. Am J Physiol Renal Physiol 2010.
152. Canalejo A, Canadillas S, Ballesteros E, Rodriguez M, Almaden Y. Importance ofarachidonic acid as a mediator of parathyroid gland response. Kidney Int Suppl S10–S13, 2003.
153. Canfield SP, Spencer JE. The inhibitory effects of 5-hydroxytryptamine on gastricacid secretion by the rat isolated stomach. Br J Pharmacol 78: 123–129, 1983.
154. Cantley LK, Russell J, Lettieri D, Sherwood LM. 1,25-Dihydroxyvitamin D3 sup-presses parathyroid hormone secretion from bovine parathyroid cells in tissue cul-ture. Endocrinology 117: 2114–2119, 1985.
155. Care AD, Bates RF, Swaminathan R, Ganguli PC. The role of gastrin as a calcitoninsecretagogue. J Endocrinol 51: 735–744, 1971.
156. Care AD, Bruce JB, Boelkins J, Kenny AD, Conaway H, Anast CS. Role of pancre-ozymin-cholecystokinin and structurally related compounds as calcitonin secreto-gogues. Endocrinology 89: 262–271, 1971.
157. Carles-Bonnet C, Jarrousse C, Niel H, Martinez J, Bataille D. Oxyntomodulin and its(19–37) and (30–37) fragments inhibit histamine-stimulated gastric acid secretion inthe conscious rat. Eur J Pharmacol 203: 245–252, 1991.
158. Carney S, Thompson L. Acute effect of calcitonin on rat renal electrolyte transport.Am J Physiol Renal Fluid Electrolyte Physiol 240: F12–F16, 1981.
159. Carney SL. Acute effect of endogenous calcitonin on rat renal function. Miner Elec-trolyte Metab 21: 411–416, 1995.
160. Carney SL. Calcitonin and human renal calcium and electrolyte transport. MinerElectrolyte Metab 23: 43–47, 1997.
161. Carraway R, Leeman SE. The isolation of a new hypotensive peptide, neurotensin,from bovine hypothalami. J Biol Chem 248: 6854–6861, 1973.
162. Carrillo-Lopez N, Alvarez-Hernandez D, Gonzalez-Suarez I, Roman-Garcia P, Val-divielso JM, Fernandez-Martin JL, Cannata-Andia JB. Simultaneous changes in thecalcium-sensing receptor and the vitamin D receptor under the influence of calciumand calcitriol. Nephrol Dial Transplant 23: 3479–3484, 2008.
163. Caterina MJ, Rosen TA, Tominaga M, Brake AJ, Julius D. A capsaicin-receptor ho-mologue with a high threshold for noxious heat. Nature 398: 436–441, 1999.
164. Catlow K, Ashurst HL, Varro A, Dimaline R. Identification of a gastrin responseelement in the vesicular monoamine transporter type 2 promoter and requirementof 20 S proteasome subunits for transcriptional activity. J Biol Chem 282: 17069–17077, 2007.
165. Ceglia L, Harris SS, Rasmussen HM, Dawson-Hughes B. Activation of the calciumsensing receptor stimulates gastrin and gastric acid secretion in healthy participants.Osteoporos Int 20: 71–78, 2009.
166. Chabardes D, Gagnan-Brunette M, Imbert-Teboul M, Gontcharevskaia O, Mon-tegut M, Clique A, Morel F. Adenylate cyclase responsiveness to hormones in vari-ous portions of the human nephron. J Clin Invest 65: 439–448, 1980.
167. Chabre O, Conklin BR, Lin HY, Lodish HF, Wilson E, Ives HE, Catanzariti L, Hem-mings BA, Bourne HR. A recombinant calcitonin receptor independently stimulates3=,5=-cyclic adenosine monophosphate and Ca2�/inositol phosphate signaling path-ways. Mol Endocrinol 6: 551–556, 1992.
168. Chai SY, Christopoulos G, Cooper ME, Sexton PM. Characterization of binding sitesfor amylin, calcitonin, and CGRP in primate kidney. Am J Physiol Renal Physiol 274:F51–F62, 1998.
169. Chambers TJ, Magnus CJ. Calcitonin alters behaviour of isolated osteoclasts. J Pathol136: 27–39, 1982.
170. Chang Q, Hoefs S, van der Kemp AW, Topala CN, Bindels RJ, Hoenderop JG. Thebeta-glucuronidase klotho hydrolyzes and activates the TRPV5 channel. Science 310:490–493, 2005.
171. Chang W, Tu C, Chen TH, Bikle D, Shoback D. The extracellular calcium-sensingreceptor (CaSR) is a critical modulator of skeletal development. Sci Signal 1: ra1,2008.
172. Chang W, Tu C, Chen TH, Komuves L, Oda Y, Pratt SA, Miller S, Shoback D.Expression and signal transduction of calcium-sensing receptors in cartilage andbone. Endocrinology 140: 5883–5893, 1999.
173. Chattopadhyay N, Cheng I, Rogers K, Riccardi D, Hall A, Diaz R, Hebert SC, SoybelDI, Brown EM. Identification and localization of extracellular Ca2�-sensing receptorin rat intestine. Am J Physiol Gastrointest Liver Physiol 274: G122–G130, 1998.
174. Chattopadhyay N, Yano S, Tfelt-Hansen J, Rooney P, Kanuparthi D, BandyopadhyayS, Ren X, Terwilliger E, Brown EM. Mitogenic action of calcium-sensing receptor onrat calvarial osteoblasts. Endocrinology 145: 3451–3462, 2004.
175. Chen CJ, Barnett JV, Congo DA, Brown EM. Divalent cations suppress 3=,5=-aden-osine monophosphate accumulation by stimulating a pertussis toxin-sensitive gua-nine nucleotide-binding protein in cultured bovine parathyroid cells. Endocrinology124: 233–239, 1989.
176. Chen D, Marvik R, Ronning K, Andersson K, Waldum HL, Hakanson R. Gastrin-evoked secretion of pancreastatin and histamine from ECL cells and of acid from
SASCHA KOPIC AND JOHN P. GEIBEL
242 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

parietal cells in isolated, vascularly perfused rat stomach. Effects of isobutyl methyl-xanthin and alpha-fluoromethylhistidine. Regul Pept 65: 133–138, 1996.
177. Chen D, Zhao CM, Al-Haider W, Hakanson R, Rehfeld JF, Kopin AS. Differentiationof gastric ECL cells is altered in CCK(2) receptor-deficient mice. Gastroenterology123: 577–585, 2002.
178. Chen D, Zhao CM, Dockray GJ, Varro A, Van Hoek A, Sinclair NF, Wang TC, Koh TJ.Glycine-extended gastrin synergizes with gastrin 17 to stimulate acid secretion ingastrin-deficient mice. Gastroenterology 119: 756–765, 2000.
179. Chen D, Zhao CM, Hakanson R, Samuelson LC, Rehfeld JF, Friis-Hansen L. Alteredcontrol of gastric acid secretion in gastrin-cholecystokinin double mutant mice. Gas-troenterology 126: 476–487, 2004.
180. Chen KS, DeLuca HF. Cloning of the human 1 alpha,25-dihydroxyvitamin D-3 24-hydroxylase gene promoter and identification of two vitamin D-responsive ele-ments. Biochim Biophys Acta 1263: 1–9, 1995.
181. Chen S, Glenn DJ, Ni W, Grigsby CL, Olsen K, Nishimoto M, Law CS, Gardner DG.Expression of the vitamin d receptor is increased in the hypertrophic heart. Hyper-tension 52: 1106–1112, 2008.
182. Cheng I, Qureshi I, Chattopadhyay N, Qureshi A, Butters RR, Hall AE, Cima RR,Rogers KV, Hebert SC, Geibel JP, Brown EM, Soybel DI. Expression of an extracel-lular calcium-sensing receptor in rat stomach. Gastroenterology 116: 118–126, 1999.
183. Cheng JB, Levine MA, Bell NH, Mangelsdorf DJ, Russell DW. Genetic evidence thatthe human CYP2R1 enzyme is a key vitamin D 25-hydroxylase. Proc Natl Acad SciUSA 101: 7711–7715, 2004.
184. Cheng JB, Motola DL, Mangelsdorf DJ, Russell DW. De-orphanization of cyto-chrome P450 2R1: a microsomal vitamin D 25-hydroxilase. J Biol Chem 278: 38084–38093, 2003.
185. Cheng SX, Geibel JP, Hebert SC. Extracellular polyamines regulate fluid secretion inrat colonic crypts via the extracellular calcium-sensing receptor. Gastroenterology126: 148–158, 2004.
186. Cheng SX, Okuda M, Hall AE, Geibel JP, Hebert SC. Expression of calcium-sensingreceptor in rat colonic epithelium: evidence for modulation of fluid secretion. Am JPhysiol Gastrointest Liver Physiol 283: G240–G250, 2002.
187. Chesney RW, Rosen JF, Hamstra AJ, Smith C, Mahaffey K, DeLuca HF. Absence ofseasonal variation in serum concentrations of 1,25-dihydroxyvitamin D despite a risein 25-hydroxyvitamin D in summer. J Clin Endocrinol Metab 53: 139–142, 1981.
188. Cheung R, Erclik MS, Mitchell J. Increased expression of G11alpha in osteoblasticcells enhances parathyroid hormone activation of phospholipase C and AP-1 regu-lation of matrix metalloproteinase-13 mRNA. J Cell Physiol 204: 336–343, 2005.
189. Chew CS. Cholecystokinin, carbachol, gastrin, histamine, and forskolin increase[Ca2�]i in gastric glands. Am J Physiol Gastrointest Liver Physiol 250: G814–G823,1986.
190. Chew CS, Brown MR. Release of intracellular Ca2� and elevation of inositol trispho-sphate by secretagogues in parietal and chief cells isolated from rabbit gastric mu-cosa. Biochim Biophys Acta 888: 116–125, 1986.
191. Chey WY, Chang CH, Pan HJ, Chang C, Kim BM, Park IS, Chang TM. Evidence onthe presence of secretin cells in the gastric antral and oxyntic mucosa. Regul Pept 111:183–190, 2003.
192. Chey WY, Chang TM, Park HJ, Lee KY, Escoffery R. Secretin-like immunoreactivityand biological activity in the antral mucosa. Endocrinology 113: 651–656, 1983.
193. Chey WY, Escoffery R. Secretion cells in the gastrointestinal tract. Endocrinology 98:1390–1395, 1976.
194. Chey WY, Hitanant S, Hendricks J, Lorber SH. Effect of secretin and cholecystokininon gastric emptying and gastric secretion in man. Gastroenterology 58: 820–827,1970.
195. Chey WY, Lee YH, Hendricks JG, Rhodes RA, Tai HH. Plasma secretin concentra-tions in fasting and postprandial state in man. Am J Dig Dis 23: 981–988, 1978.
196. Chiba T, Fisher SK, Agranoff BW, Yamada T. Autoregulation of muscarinic andgastrin receptors on gastric parietal cells. Am J Physiol Gastrointest Liver Physiol 256:G356–G363, 1989.
197. Chiba T, Fujita T, Yamada T. Carbachol inhibits stimulant-induced increases in fundicD-cell cytosolic Ca2� concentration. Am J Physiol Gastrointest Liver Physiol 257:G308–G312, 1989.
198. Chiba T, Park J, Yamada T. Biosynthesis of somatostatin in canine fundic D cells. J ClinInvest 81: 282–287, 1988.
199. Chiba T, Taminato T, Kadowaki S, Abe H, Chihara K, Seino Y, Matsukura S, Fujita T.Effects of glucagon, secretin, and vasoactive intestinal polypeptide on gastric soma-tostatin and gastrin release from isolated perfused rat stomach. Gastroenterology 79:67–71, 1980.
200. Chiba T, Yamada T. Mechanisms for muscarinic inhibition of somatostatin releasefrom canine fundic D cells. Metabolism 39: 122–124, 1990.
201. Chirayath MV, Gajdzik L, Hulla W, Graf J, Cross HS, Peterlik M. Vitamin D increasestight-junction conductance and paracellular Ca2� transport in Caco-2 cell cultures.Am J Physiol Gastrointest Liver Physiol 274: G389–G396, 1998.
202. Chiu HF, Huang YW, Chang CC, Yang CY. Use of proton pump inhibitors increasedthe risk of hip fracture: a population-based case-control study. PharmacoepidemiolDrug Safety 19: 1131–1136, 2010.
203. Christakos S, Brunette MG, Norman AW. Localization of immunoreactive vitaminD-dependent calcium binding protein in chick nephron. Endocrinology 109: 322–324,1981.
204. Chuang CN, Tanner M, Lloyd KC, Wong H, Soll AH. Endogenous somatostatininhibits histamine release from canine gastric mucosal cells in primary culture. Am JPhysiol Gastrointest Liver Physiol 265: G521–G525, 1993.
205. Chung I, Li P, Lee K, Chang T, Chey WY. Dual inhibitory mechanism of secretinaction on acid secretion in totally isolated, vascularly perfused rat stomach. Gastro-enterology 107: 1751–1758, 1994.
206. Chung MK, Guler AD, Caterina MJ. TRPV1 shows dynamic ionic selectivity duringagonist stimulation. Nat Neurosci 11: 555–564, 2008.
207. Cid LP, Montrose-Rafizadeh C, Smith DI, Guggino WB, Cutting GR. Cloning of aputative human voltage-gated chloride channel (CIC-2) cDNA widely expressed inhuman tissues. Hum Mol Genet 4: 407–413, 1995.
208. Clark CG, Crooks J, Dawson AA, Mitchell PE. Disordered calcium metabolism afterpolya partial gastrectomy. Lancet 1: 734–738, 1964.
209. Clemens TL, Adams JS, Henderson SL, Holick MF. Increased skin pigment reducesthe capacity of skin to synthesise vitamin D3. Lancet 1: 74–76, 1982.
210. Clements MR, Davies M, Fraser DR, Lumb GA, Mawer EB, Adams PH. Metabolicinactivation of vitamin D is enhanced in primary hyperparathyroidism. Clin Sci 73:659–664, 1987.
211. Clements MR, Davies M, Hayes ME, Hickey CD, Lumb GA, Mawer EB, Adams PH.The role of 1,25-dihydroxyvitamin D in the mechanism of acquired vitamin D defi-ciency. Clin Endocrinol 37: 17–27, 1992.
212. Clements MR, Johnson L, Fraser DR. A new mechanism for induced vitamin Ddeficiency in calcium deprivation. Nature 325: 62–65, 1987.
213. Cleve H. The variants of the group-specific component. A review of their distribu-tion in human populations. Isr J Med Sci 9: 1133–1146, 1973.
214. Cocchi D, Maccarinelli G, Sibilia V, Tulipano G, Torsello A, Pazzaglia UE, Giustina A,Netti C. GH-releasing peptides and bone. J Endocrinol Invest 28: 11–14, 2005.
215. Cochran M, Peacock M, Sachs G, Nordin BE. Renal effects of calcitonin. Br Med J 1:135–137, 1970.
216. Collip JB. The extraction of a parathyroid hormone which will prevent or controlparathyroid tetany and which regulates the level of blood calcium. J Biol Chem 63:395–438, 1925.
217. Colnot S, Ovejero C, Romagnolo B, Porteu A, Lacourte P, Thomasset M, Perret C.Transgenic analysis of the response of the rat calbindin-D 9k gene to vitamin D.Endocrinology 141: 2301–2308, 2000.
218. Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. DietaryReference Intakes for Calcium and Vitamin D. Washington, DC: National AcademyPress, 2010.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
243Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

219. Compston JE, Thompson RP. Intestinal absorption of 25-hydroxyvitamin D andosteomalacia in primary biliary cirrhosis. Lancet 1: 721–724, 1977.
220. Conigrave AD, Quinn SJ, Brown EM. L-Amino acid sensing by the extracellularCa2�-sensing receptor. Proc Natl Acad Sci USA 97: 4814–4819, 2000.
221. Cooke NE, David EV. Serum vitamin D-binding protein is a third member of thealbumin and alpha fetoprotein gene family. J Clin Invest 76: 2420–2424, 1985.
222. Cooper CW, Biggerstaff CR, Wiseman CW, Carlone MF. Hypocalcemic effect ofpentagastrin and related gastrointestinal hormnal peptides in the rat. Endocrinology91: 1455–1461, 1972.
223. Cooper CW, Hirsch PF, Munson PL. Importance of endogenous thyrocalcitonin forprotection against hypercalcemia in the rat. Endocrinology 86: 406–415, 1970.
224. Cooper CW, McGuigan JE, Schwesinger WH, Brubaker RL, Munson PL. Correlationbetween levels of gastrin and thyrocalcitonin in pig thyroid venous blood. Endocri-nology 95: 302–307, 1974.
225. Cooper CW, Ramp WK, Becker DI, Ontjes DA. In vitro secretion of immunoreactiverat thyrocalcitonin. Endocrinology 101: 304–311, 1977.
226. Cooper CW, Schwesinger WH, Mahgoub AM, Ontjes DA. Thyrocalcitonin: stimu-lation of secretion by pentagastrin. Science 172: 1238–1240, 1971.
227. Copp DH, Cameron EC, Cheney BA, Davidson AG, Henze KG. Evidence for calci-tonin: a new hormone from the parathyroid that lowers blood calcium. Endocrinology70: 638–649, 1962.
228. Corley DA, Kubo A, Zhao W, Quesenberry C. Proton pump inhibitors and hista-mine-2 receptor antagonists are associated with hip fractures among at-risk patients.Gastroenterology 139: 93–101, 2010.
229. Cornish J, Callon KE, Bava U, Kamona SA, Cooper GJ, Reid IR. Effects of calcitonin,amylin, calcitonin gene-related peptide on osteoclast development. Bone 29: 162–168, 2001.
230. Couper RT, Corey M, Moore DJ, Fisher LJ, Forstner GG, Durie PR. Decline ofexocrine pancreatic function in cystic fibrosis patients with pancreatic sufficiency.Pediatr Res 32: 179–182, 1992.
231. Cramer T, Juttner S, Plath T, Mergler S, Seufferlein T, Wang TC, Merchant J, HockerM. Gastrin transactivates the chromogranin A gene through MEK-1/ERK- and PKC-dependent phosphorylation of Sp1 and CREB. Cell Signal 20: 60–72, 2008.
232. Cuppoletti J, Sachs G. Regulation of gastric acid secretion via modulation of a chlo-ride conductance. J Biol Chem 259: 14952–14959, 1984.
233. D’Amour P, Brossard JH, Rousseau L, Nguyen-Yamamoto L, Nassif E, Lazure C,Gauthier D, Lavigne JR, Zahradnik RJ. Structure of non-(1–84) PTH fragments se-creted by parathyroid glands in primary and secondary hyperparathyroidism. KidneyInt 68: 998–1007, 2005.
234. D’Amour P, Segre GV, Roth SI, Potts JT Jr. Analysis of parathyroid hormone and itsfragments in rat tissues: chemical identification and microscopical localization. J ClinInvest 63: 89–98, 1979.
235. Dahlback H, Wikvall K. 25-Hydroxylation of vitamin D3 by a cytochrome P-450 fromrabbit liver mitochondria. Biochem J 252: 207–213, 1988.
236. Daiger SP, Schanfield MS, Cavalli-Sforza LL. Group-specific component (Gc) pro-teins bind vitamin D and 25-hydroxyvitamin D. Proc Natl Acad Sci USA 72: 2076–2080, 1975.
237. Dale HH, Laidlow PP. The physiological action of beta-iminazolylethylamine. J Physiol41: 318–344, 1910.
238. Dardenne O, Prud’homme J, Arabian A, Glorieux FH, St-Arnaud R. Targeted inac-tivation of the 25-hydroxyvitamin D(3)-1(alpha)-hydroxylase gene (CYP27B1) cre-ates an animal model of pseudovitamin D-deficiency rickets. Endocrinology 142:3135–3141, 2001.
239. Dardenne O, Prud’homme J, Hacking SA, Glorieux FH, St-Arnaud R. Correction ofthe abnormal mineral ion homeostasis with a high-calcium, high-phosphorus, high-lactose diet rescues the PDDR phenotype of mice deficient for the 25-hydroxyvita-min D-1alpha-hydroxylase (CYP27B1). Bone 32: 332–340, 2003.
240. Darwish HM, DeLuca HF. Identification of a 1,25-dihydroxyvitamin D3-responseelement in the 5=-flanking region of the rat calbindin D-9k gene. Proc Natl Acad SciUSA 89: 603–607, 1992.
241. Database Csr. http://www.casrdb.mcgill.ca/ [retrieved September 2011].
242. Date Y, Kojima M, Hosoda H, Sawaguchi A, Mondal MS, Suganuma T, Matsukura S,Kangawa K, Nakazato M. Ghrelin, a novel growth hormone-releasing acylated pep-tide, is synthesized in a distinct endocrine cell type in the gastrointestinal tracts of ratsand humans. Endocrinology 141: 4255–4261, 2000.
243. Datta R, Waheed A, Shah GN, Sly WS. Signal sequence mutation in autosomaldominant form of hypoparathyroidism induces apoptosis that is corrected by achemical chaperone. Proc Natl Acad Sci USA 104: 19989–19994, 2007.
244. Davies M, Heys SE, Selby PL, Berry JL, Mawer EB. Increased catabolism of 25-hydroxyvitamin D in patients with partial gastrectomy and elevated 1,25-dihy-droxyvitamin D levels. Implications for metabolic bone disease. J Clin EndocrinolMetab 82: 209–212, 1997.
245. Davies M, Mawer EB, Krawitt EL. Comparative absorption of vitamin D3 and 25-hydroxyvitamin D3 in intestinal disease. Gut 21: 287–292, 1980.
246. Davies SL, Ozawa A, McCormick WD, Dvorak MM, Ward DT. Protein kinaseC-mediated phosphorylation of the calcium-sensing receptor is stimulated by recep-tor activation and attenuated by calyculin-sensitive phosphatase activity. J Biol Chem282: 15048–15056, 2007.
247. Davis WL, Jones RG. Lysosomal proliferation in rachitic avian intestinal absorptivecells following 1,25-dihydroxycholecalciferol. Tissue Cell 14: 585–595, 1982.
248. De Groot T, Kovalevskaya NV, Verkaart S, Schilderink N, Felici M, van der HagenEA, Bindels RJ, Vuister GW, Hoenderop JG. Molecular mechanisms of calmodulinaction on TRPV5 and modulation by parathyroid hormone. Mol Cell Biol 31: 2845–2853, 2011.
249. De Groot T, Lee K, Langeslag M, Xi Q, Jalink K, Bindels RJ, Hoenderop JG. Parathy-roid hormone activates TRPV5 via PKA-dependent phosphorylation. J Am Soc Neph-rol 20: 1693–1704, 2009.
250. De Jesus Ferreira MC, Helies-Toussaint C, Imbert-Teboul M, Bailly C, Verbavatz JM,Bellanger AC, Chabardes D. Co-expression of a Ca2�-inhibitable adenylyl cyclaseand of a Ca2�-sensing receptor in the cortical thick ascending limb cell of the ratkidney. Inhibition of hormone-dependent cAMP accumulation by extracellularCa2�. J Biol Chem 273: 15192–15202, 1998.
251. De Rouffignac C, Elalouf JM. Effects of calcitonin on the renal concentrating mech-anism. Am J Physiol Renal Fluid Electrolyte Physiol 245: F506–F511, 1983.
252. De Vries F, Cooper AL, Cockle SM, Van Staa TP, Cooper C. Fracture risk in patientsreceiving acid-suppressant medication alone and in combination with bisphospho-nates. Osteoporosis Int 20: 1989–1998, 2009.
253. Dedek K, Waldegger S. Colocalization of KCNQ1/KCNE channel subunits in themouse gastrointestinal tract. Pflügers Arch 442: 896–902, 2001.
254. Delhanty PJ, van der Eerden BC, van der Velde M, Gauna C, Pols HA, Jahr H, ChibaH, van der Lely AJ, van Leeuwen JP. Ghrelin and unacylated ghrelin stimulate humanosteoblast growth via mitogen-activated protein kinase (MAPK)/phosphoinositide3-kinase (PI3K) pathways in the absence of GHS-R1a. J Endocrinol 188: 37–47, 2006.
255. Deller DJ. Radiocalcium absorption after partial gastrectomy. Am J Dig Dis 11: 10–19,1966.
256. DeLuca HF, Lund J, Rosenbloom A, Lobeck CC. Metabolism of tritiated vitamin D3
in familial vitamin D-resistant rickets with hypophosphatemia. J Pediatr 70: 828–832,1967.
257. DelValle J, Yamada T. Amino acids and amines stimulate gastrin release from canineantral G-cells via different pathways. J Clin Invest 85: 139–143, 1990.
258. Delvin EE, Arabian A, Glorieux FH. Kinetics of liver microsomal cholecalciferol25-hydroxylase in vitamin D-depleted and -repleated rats. Biochem J 172: 417–422,1978.
259. Demarest JR, Loo DD, Sachs G. Activation of apical chloride channels in the gastricoxyntic cell. Science 245: 402–404, 1989.
260. Dempster DW, Hughes-Begos CE, Plavetic-Chee K, Brandao-Burch A, Cosman F,Nieves J, Neubort S, Lu SS, Iida-Klein A, Arnett T, Lindsay R. Normal human oste-
SASCHA KOPIC AND JOHN P. GEIBEL
244 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

oclasts formed from peripheral blood monocytes express PTH type 1 receptors andare stimulated by PTH in the absence of osteoblasts. J Cell Biochem 95: 139–148,2005.
261. Deng F, Ling J, Ma J, Liu C, Zhang W. Stimulation of intramembranous bone repair inrats by ghrelin. Exp Physiol 93: 872–879, 2008.
262. Dent J, Kahrilas PJ, Hatlebakk J, Vakil N, Denison H, Franzen S, Lundborg P. Arandomized, comparative trial of a potassium-competitive acid blocker (AZD0865)and esomeprazole for the treatment of patients with nonerosive reflux disease. AmJ Gastroenterol 103: 20–26, 2008.
263. Derler I, Hofbauer M, Kahr H, Fritsch R, Muik M, Kepplinger K, Hack ME, Moritz S,Schindl R, Groschner K, Romanin C. Dynamic but not constitutive association ofcalmodulin with rat TRPV6 channels enables fine tuning of Ca2�-dependent inacti-vation. J Physiol 577: 31–44, 2006.
264. Desfleurs E, Wittner M, Simeone S, Pajaud S, Moine G, Rajerison R, Di Stefano A.Calcium-sensing receptor: regulation of electrolyte transport in the thick ascendinglimb of Henle’s loop. Kidney Blood Press Res 21: 401–412, 1998.
265. Di Stefano A, Wittner M, Nitschke R, Braitsch R, Greger R, Bailly C, Amiel C, RoinelN, de Rouffignac C. Effects of parathyroid hormone and calcitonin on Na�, Cl�, K�,Mg2� and Ca2� transport in cortical and medullary thick ascending limbs of mousekidney. Pflügers Arch 417: 161–167, 1990.
266. Diamond JM, Bossert WH. Standing-gradient osmotic flow. A mechanism for cou-pling of water and solute transport in epithelia. J Gen Physiol 50: 2061–2083, 1967.
267. Dicker F, Quitterer U, Winstel R, Honold K, Lohse MJ. Phosphorylation-indepen-dent inhibition of parathyroid hormone receptor signaling by G protein-coupledreceptor kinases. Proc Natl Acad Sci USA 96: 5476–5481, 1999.
268. Dimaline R, Sandvik AK. Histidine decarboxylase gene expression in rat fundus isregulated by gastrin. FEBS Lett 281: 20–22, 1991.
269. Dinoso V, Chey WY, Hendricks J, Lorber SH. Intestinal mucosal hormones andmotor function of the stomach in man. J Appl Physiol 26: 326–329, 1969.
270. Divieti P, Geller AI, Suliman G, Juppner H, Bringhurst FR. Receptors specific for thecarboxyl-terminal region of parathyroid hormone on bone-derived cells: determi-nants of ligand binding and bioactivity. Endocrinology 146: 1863–1870, 2005.
271. Divieti P, Inomata N, Chapin K, Singh R, Juppner H, Bringhurst FR. Receptors for thecarboxyl-terminal region of pth(1–84) are highly expressed in osteocytic cells. En-docrinology 142: 916–925, 2001.
272. Divieti P, John MR, Juppner H, Bringhurst FR. Human PTH-(7–84) inhibits boneresorption in vitro via actions independent of the type 1 PTH/PTHrP receptor.Endocrinology 143: 171–176, 2002.
273. Dixon KM, Deo SS, Norman AW, Bishop JE, Halliday GM, Reeve VE, Mason RS. Invivo relevance for photoprotection by the vitamin D rapid response pathway. JSteroid Biochem Mol Biol 103: 451–456, 2007.
274. Dobnig H, Turner RT. The effects of programmed administration of human para-thyroid hormone fragment (1–34) on bone histomorphometry and serum chemistryin rats. Endocrinology 138: 4607–4612, 1997.
275. Dong H, Sellers ZM, Smith A, Chow JY, Barrett KE. Na�/Ca2� exchange regulatesCa2�-dependent duodenal mucosal ion transport and HCO3
� secretion in mice. AmJ Physiol Gastrointest Liver Physiol 288: G457–G465, 2005.
276. Dornonville de la Cour C, Bjorkqvist M, Sandvik AK, Bakke I, Zhao CM, Chen D,Hakanson R. A-like cells in the rat stomach contain ghrelin and do not operate undergastrin control. Regul Pept 99: 141–150, 2001.
277. Dornonville de la Cour C, Lindqvist A, Egecioglu E, Tung YC, Surve V, Ohlsson C,Jansson JO, Erlanson-Albertsson C, Dickson SL, Hakanson R. Ghrelin treatmentreverses the reduction in weight gain and body fat in gastrectomised mice. Gut 54:907–913, 2005.
278. Dornonville de la Cour C, Lindstrom E, Norlen P, Hakanson R. Ghrelin stimulatesgastric emptying but is without effect on acid secretion and gastric endocrine cells.Regul Pept 120: 23–32, 2004.
279. Doroszewicz J, Waldegger P, Jeck N, Seyberth H, Waldegger S. pH dependence ofextracellular calcium sensing receptor activity determined by a novel technique.Kidney Int 67: 187–192, 2005.
280. Dorrington KJ, Hui A, Hofmann T, Hitchman AJ, Harrison JE. Porcine intestinalcalcium-binding protein. Molecular properties and the effect of binding calcium ions.J Biol Chem 249: 199–204, 1974.
281. Dorwart MR, Shcheynikov N, Wang Y, Stippec S, Muallem S. SLC26A9 is a Cl�
channel regulated by the WNK kinases. J Physiol 584: 333–345, 2007.
282. Drees BM, Hamilton JW. Pancreastatin and bovine parathyroid cell secretion. BoneMiner 17: 335–346, 1992.
283. Drescher D, DeLuca HF. Vitamin D stimulated calcium binding protein from ratintestinal mucosa. Purification and some properties. Biochemistry 10: 2302–2307,1971.
284. Dressman JB, Berardi RR, Dermentzoglou LC, Russell TL, Schmaltz SP, Barnett JL,Jarvenpaa KM. Upper gastrointestinal (GI) pH in young, healthy men and women.Pharm Res 7: 756–761, 1990.
285. Dubrasquet M, Bataille D, Gespach C. Oxyntomodulin (glucagon-37 or bioactiveenteroglucagon): a potent inhibitor of pentagastrin-stimulated acid secretion in rats.Biosci Rep 2: 391–395, 1982.
286. Dueland S, Helgerud P, Pedersen JI, Berg T, Drevon CA. Plasma clearance, transfer,and distribution of vitamin D3 from intestinal lymph. Am J Physiol Endocrinol Metab245: E326–E331, 1983.
287. Dueland S, Pedersen JI, Helgerud P, Drevon CA. Absorption, distribution, transportof vitamin D3 and 25-hydroxyvitamin D3 in the rat. Am J Physiol Endocrinol Metab 245:E463–E467, 1983.
288. Dueland S, Pedersen JI, Helgerud P, Drevon CA. Transport of vitamin D3 from ratintestine. Evidence for transfer of vitamin D3 from chylomicrons to alpha-globulins.J Biol Chem 257: 146–150, 1982.
289. Duflos C, Bellaton C, Baghdassarian N, Gadoux M, Pansu D, Bronner F. 1,25-Dihydroxycholecalciferol regulates rat intestinal calbindin D9k posttranscriptionally.J Nutr 126: 834–841, 1996.
290. Duflos C, Bellaton C, Pansu D, Bronner F. Calcium solubility, intestinal sojourn timeand paracellular permeability codetermine passive calcium absorption in rats. J Nutr125: 2348–2355, 1995.
291. Dufner MM, Kirchhoff P, Remy C, Hafner P, Muller MK, Cheng SX, Tang LQ, HebertSC, Geibel JP, Wagner CA. The calcium-sensing receptor acts as a modulator ofgastric acid secretion in freshly isolated human gastric glands. Am J Physiol Gastroin-test Liver Physiol 289: G1084–G1090, 2005.
292. Duman JG, Pathak NJ, Ladinsky MS, McDonald KL, Forte JG. Three-dimensionalreconstruction of cytoplasmic membrane networks in parietal cells. J Cell Sci 115:1251–1258, 2002.
293. Duman JG, Tyagarajan K, Kolsi MS, Moore HP, Forte JG. Expression of rab11a N124Iin gastric parietal cells inhibits stimulatory recruitment of the H�-K�-ATPase. Am JPhysiol Cell Physiol 277: C361–C372, 1999.
294. Durr KL, Abe K, Tavraz NN, Friedrich T. E2P state stabilization by the N-terminaltail of the H�-K�-ATPase beta-subunit is critical for efficient proton pumping underin vivo conditions. J Biol Chem 284: 20147–20154, 2009.
295. DuVal JW, Saffouri B, Weir GC, Walsh JH, Arimura A, Makhlouf GM. Stimulation ofgastrin and somatostatin secretion from the isolated rat stomach by bombesin. Am JPhysiol Gastrointest Liver Physiol 241: G242–G247, 1981.
296. Dvorak MM, Chen TH, Orwoll B, Garvey C, Chang W, Bikle DD, Shoback DM.Constitutive activity of the osteoblast Ca2�-sensing receptor promotes loss of can-cellous bone. Endocrinology 148: 3156–3163, 2007.
297. Dvorak MM, Siddiqua A, Ward DT, Carter DH, Dallas SL, Nemeth EF, Riccardi D.Physiological changes in extracellular calcium concentration directly control osteo-blast function in the absence of calciotropic hormones. Proc Natl Acad Sci USA 101:5140–5145, 2004.
298. Edkins JS. The chemical mechanism of gastric secretion. J Physiol 34: 133–144, 1906.
299. Edwards BR, Baer PG, Sutton RA, Dirks JH. Micropuncture study of diuretic effectson sodium and calcium reabsorption in the dog nephron. J Clin Invest 52: 2418–2427,1973.
300. Edwards BR, Sutton RA, Dirks JH. Effect of calcium infusion on renal tubular reab-sorption in the dog. Am J Physiol 227: 13–18, 1974.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
245Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

301. Edwards LW, Herrington JL Jr. Vagotomy and gastro-enterostomy; vagotomy andconservative gastrectomy; a comparative study. Ann Surg 137: 873–883, 1953.
302. Ekblad E, Ekelund M, Graffner H, Hakanson R, Sundler F. Peptide-containing nervefibers in the stomach wall of rat and mouse. Gastroenterology 89: 73–85, 1985.
303. El Hag AI, Karrar ZA. Nutritional vitamin D deficiency rickets in Sudanese children.Ann Trop Paediatr 15: 69–76, 1995.
304. Elalouf JM, Roinel N, de Rouffignac C. ADH-like effects of calcitonin on electrolytetransport by Henle’s loop of rat kidney. Am J Physiol Renal Fluid Electrolyte Physiol 246:F213–F220, 1984.
305. Ellman P, Irwin DB. Osteomalacia following gastrectomy. Postgrad Med J 35: 358–361, 1959.
306. Emmelin N, Kahlson GS. Histamine as a physiological excitant of acid gastric secre-tion. Acta Physiol Scand 8: 289–304, 1944.
307. Engelhardt W, Grohmann C, Schwille PO, Geus A. Calcium absorption in the rat asinfluenced by highly selective vagotomy with special regard to endogenous gastrin.Res Exp Med 180: 1–9, 1982.
308. Engelhardt W, Rumenapf G, Schwille PO. Effects of highly selective vagotomy onsmall intestinal calcium transport in the rat. Miner Electrolyte Metab 10: 239–243,1984.
309. Engqvist-Goldstein AE, Warren RA, Kessels MM, Keen JH, Heuser J, Drubin DG.The actin-binding protein Hip1R associates with clathrin during early stages ofendocytosis and promotes clathrin assembly in vitro. J Cell Biol 154: 1209 –1223,2001.
310. Ericsson P, Hakanson R, Rehfeld JF, Norlen P. Gastrin release: antrum microdialysisreveals a complex neural control. Regul Pept 161: 22–32, 2010.
311. Erler I, Hirnet D, Wissenbach U, Flockerzi V, Niemeyer BA. Ca2�-selective tran-sient receptor potential V channel architecture and function require a specificankyrin repeat. J Biol Chem 279: 34456–34463, 2004.
312. Esplugues JV, Barrachina MD, Calatayud S, Pique JM, Whittle BJ. Nitric oxide medi-ates the inhibition by interleukin-1 beta of pentagastrin-stimulated rat gastric acidsecretion. Br J Pharmacol 108: 9–10, 1993.
313. Fahrmann M, Kaufhold M, Pfeiffer AF, Seidler U. Protein kinase C-alpha attenuatescholinergically stimulated gastric acid secretion of rabbit parietal cells. Br J Pharmacol139: 545–554, 2003.
314. Fahrmann M, Kaufhold M, Rieg T, Seidler U. Different actions of protein kinase Cisoforms alpha and epsilon on gastric acid secretion. Br J Pharmacol 136: 938–946,2002.
315. Fahrmann M, Mohlig M, Schatz H, Pfeiffer A. Purification and characterization of aCa2�/calmodulin-dependent protein kinase II from hog gastric mucosa using a pro-tein-protein affinity chromatographic technique. Eur J Biochem 255: 516–525, 1998.
316. Fahrmann M, Pfeiffer A. Copurification of two holoenzyme-forming calcium/cal-modulin-dependent protein kinase II isoforms as holoenzyme from porcine stom-ach. Arch Biochem Biophys 380: 151–158, 2000.
317. Fasciotto BH, Gorr SU, DeFranco DJ, Levine MA, Cohn DV. Pancreastatin, a pre-sumed product of chromogranin-A (secretory protein-I) processing, inhibits secre-tion from porcine parathyroid cells in culture. Endocrinology 125: 1617–1622, 1989.
318. Favus MJ, Angeid-Backman E. Effects of 1,25(OH)2D3 and calcium channel blockerson cecal calcium transport in the rat. Am J Physiol Gastrointest Liver Physiol 248:G676–G681, 1985.
319. FDA. FDA Drug Safety Communication: possible increased risk of fractures of thehip, wrist, and spine with the use of proton pump inhibitors Food and Drug Admin-istration. http://www.fda.gov/drugs/drugsafety/postmarketdrugsafetyinformationforpatientsandproviders/ucm213206.htm [retrieved July 2011].
320. Federico A, Dotti MT, Lore F, Nuti R. Cerebrotendinous xanthomatosis: pathophys-iological study on bone metabolism. J Neurol Sci 115: 67–70, 1993.
321. Feher JJ. Facilitated calcium diffusion by intestinal calcium-binding protein. Am JPhysiol Cell Physiol 244: C303–C307, 1983.
322. Feher JJ, Fullmer CS, Wasserman RH. Role of facilitated diffusion of calcium bycalbindin in intestinal calcium absorption. Am J Physiol Cell Physiol 262: C517–C526,1992.
323. Feldberg W, Toh CC. Distribution of 5-hydroxytryptamine (serotonin, enteramine)in the wall of the digestive tract. J Physiol 119: 352–362, 1953.
324. Fellenius E, Berglindh T, Sachs G, Olbe L, Elander B, Sjostrand SE, Wallmark B.Substituted benzimidazoles inhibit gastric acid secretion by blocking (H� �
K�)ATPase. Nature 290: 159–161, 1981.
325. Feng J, Petersen CD, Coy DH, Jiang JK, Thomas CJ, Pollak MR, Wank SA. Calcium-sensing receptor is a physiologic multimodal chemosensor regulating gastric G-cellgrowth and gastrin secretion. Proc Natl Acad Sci USA 107: 17791–17796, 2010.
326. Ferrari SL, Behar V, Chorev M, Rosenblatt M, Bisello A. Endocytosis of ligand-humanparathyroid hormone receptor 1 complexes is protein kinase C-dependent andinvolves beta-arrestin2. Real-time monitoring by fluorescence microscopy. J BiolChem 274: 29968–29975, 1999.
327. Ferrari SL, Pierroz DD, Glatt V, Goddard DS, Bianchi EN, Lin FT, Manen D, Boux-sein ML. Bone response to intermittent parathyroid hormone is altered in mice nullfor �-Arrestin2. Endocrinology 146: 1854–1862, 2005.
328. Findlay DM, Michelangeli VP, Orlowski RC, Martin TJ. Biological activities and re-ceptor interactions of des-Leu16 salmon and des-Phe16 human calcitonin. Endocri-nology 112: 1288–1291, 1983.
329. Firsov D, Bellanger AC, Marsy S, Elalouf JM. Quantitative RT-PCR analysis of calci-tonin receptor mRNAs in the rat nephron. Am J Physiol Renal Fluid Electrolyte Physiol269: F702–F709, 1995.
330. Flannery PJ, Spurney RF. Domains of the parathyroid hormone (PTH) receptorrequired for regulation by G protein-coupled receptor kinases (GRKs). BiochemPharmacol 62: 1047–1058, 2001.
331. Fleming JV, Wang TC. Amino- and carboxy-terminal PEST domains mediate gastrinstabilization of rat L-histidine decarboxylase isoforms. Mol Cell Biol 20: 4932–4947, 2000.
332. Force T, Bonventre JV, Flannery MR, Gorn AH, Yamin M, Goldring SR. A clonedporcine renal calcitonin receptor couples to adenylyl cyclase and phospholipase C.Am J Physiol Renal Fluid Electrolyte Physiol 262: F1110–F1115, 1992.
333. Foresta C, Strapazzon G, De Toni L, Perilli L, Di Mambro A, Muciaccia B, Sartori L,Selice R. Bone mineral density and testicular failure: evidence for a role of vitamin D25-hydroxylase in human testis. J Clin Endocrinol Metab 96: E646–E652, 2011.
334. Forster IC, Hernando N, Biber J, Murer H. Proximal tubular handling of phosphate:a molecular perspective. Kidney Int 70: 1548–1559, 2006.
335. Forte JG, Forte GM, Saltman P. K�-stimulated phosphatase of microsomes fromgastric mucosa. J Cell Physiol 69: 293–304, 1967.
336. Forte JG, Zhu L. Apical recycling of the gastric parietal cell H�-K�-ATPase. Annu RevPhysiol 72: 273–296, 2010.
337. Fox J, Green DT. Direct effects of calcium channel blockers on duodenal calciumtransport in vivo. Eur J Pharmacol 129: 159–164, 1986.
338. Fraser DR, Kodicek E. Regulation of 25-hydroxycholecalciferol-1-hydroxylase activ-ity in kidney by parathyroid hormone. Nat New Biol 241: 163–166, 1973.
339. Fraser DR, Kodicek E. Unique biosynthesis by kidney of a biological active vitamin Dmetabolite. Nature 228: 764–766, 1970.
340. Freeman MW, Wiren KM, Rapoport A, Lazar M, Potts JT Jr, Kronenberg HM.Consequences of amino-terminal deletions of preproparathyroid hormone signalsequence. Mol Endocrinol 1: 628–638, 1987.
341. Freeman TC, Howard A, Bentsen BS, Legon S, Walters JR. Cellular and regionalexpression of transcripts of the plasma membrane calcium pump PMCA1 in rabbitintestine. Am J Physiol Gastrointest Liver Physiol 269: G126–G131, 1995.
342. Friedman J, Au WY, Raisz LG. Responses of fetal rat bone to thyrocalcitonin in tissueculture. Endocrinology 82: 149–156, 1968.
343. Friedman J, Raisz LG. Thyrocalcitonin: inhibitor of bone resorption in tissue culture.Science 150: 1465–1467, 1965.
SASCHA KOPIC AND JOHN P. GEIBEL
246 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

344. Friedman PA. Basal and hormone-activated calcium absorption in mouse renal thickascending limbs. Am J Physiol Renal Fluid Electrolyte Physiol 254: F62–F70, 1988.
345. Fries W, Rumenapf G, Schwille PO. Disturbances of mineral and bone metabolismfollowing gastric antrectomy in the rat. Bone Miner 19: 245–256, 1992.
346. Friis-Hansen L, Schjerling CK, de la Cour CD, Hakanson R, Rehfeld JF. Characteristics ofgastrin controlled ECL cell specific gene expression. Regul Pept 140: 153–161, 2007.
347. Friis-Hansen L, Sundler F, Li Y, Gillespie PJ, Saunders TL, Greenson JK, Owyang C,Rehfeld JF, Samuelson LC. Impaired gastric acid secretion in gastrin-deficient mice.Am J Physiol Gastrointest Liver Physiol 274: G561–G568, 1998.
348. Frolik CA, Black EC, Cain RL, Satterwhite JH, Brown-Augsburger PL, Sato M, HockJM. Anabolic and catabolic bone effects of human parathyroid hormone (1–34) arepredicted by duration of hormone exposure. Bone 33: 372–379, 2003.
349. Fu GK, Lin D, Zhang MY, Bikle DD, Shackleton CH, Miller WL, Portale AA. Cloningof human 25-hydroxyvitamin D-1 alpha-hydroxylase and mutations causing vitaminD-dependent rickets type 1. Mol Endocrinol 11: 1961–1970, 1997.
350. Fu Q, Jilka RL, Manolagas SC, O’Brien CA. Parathyroid hormone stimulates receptoractivator of NFkappa B ligand and inhibits osteoprotegerin expression via proteinkinase A activation of cAMP-response element-binding protein. J Biol Chem 277:48868–48875, 2002.
351. Fudge NJ, Kovacs CS. Physiological studies in heterozygous calcium sensing receptor(CaSR) gene-ablated mice confirm that the CaSR regulates calcitonin release in vivo.BMC Physiol 4: 5, 2004.
352. Fujii T, Takahashi Y, Ikari A, Morii M, Tabuchi Y, Tsukada K, Takeguchi N, Sakai H.Functional association between K�-Cl� cotransporter-4 and H�,K�-ATPase in theapical canalicular membrane of gastric parietal cells. J Biol Chem 284: 619–629, 2009.
353. Fujita A, Horio Y, Higashi K, Mouri T, Hata F, Takeguchi N, Kurachi Y. Specificlocalization of an inwardly rectifying K(�) channel, Kir4.1, at the apical membrane ofrat gastric parietal cells; its possible involvement in K(�) recycling for the H(�)-K(�)-pump. J Physiol 540: 85–92, 2002.
354. Fujita H, Sugimoto K, Inatomi S, Maeda T, Osanai M, Uchiyama Y, Yamamoto Y,Wada T, Kojima T, Yokozaki H, Yamashita T, Kato S, Sawada N, Chiba H. Tightjunction proteins claudin-2 and -12 are critical for vitamin D-dependent Ca2� ab-sorption between enterocytes. Mol Biol Cell 19: 1912–1921, 2008.
355. Fukumoto K, Nakahara K, Katayama T, Miyazatao M, Kangawa K, Murakami N.Synergistic action of gastrin and ghrelin on gastric acid secretion in rats. BiochemBiophys Res Commun 374: 60–63, 2008.
356. Fukushima M, Suzuki Y, Tohira Y, Nishii Y, Suzuki M. 25-Hydroxylation of 1alpha-hydroxyvitamin D3 in vivo and in perfused rat liver. FEBS Lett 65: 211–214, 1976.
357. Fukushima N, Hanada R, Teranishi H, Fukue Y, Tachibana T, Ishikawa H, Takeda S,Takeuchi Y, Fukumoto S, Kangawa K, Nagata K, Kojima M. Ghrelin directly regulatesbone formation. J Bone Miner Res 20: 790–798, 2005.
358. Fullmer CS, Wasserman RH. Isolation and partial characterization of intestinal calci-um-binding proteins from the cow, pig, horse, guinea pig, and chick. Biochim BiophysActa 393: 134–142, 1975.
359. Gadelle D, Raibaud P, Sacquet E. beta-Glucuronidase activities of intestinal bacteriadetermined both in vitro and in vivo in gnotobiotic rats. Appl Environ Microbiol 49:682–685, 1985.
360. Gama L, Baxendale-Cox LM, Breitwieser GE. Ca2�-sensing receptors in intestinalepithelium. Am J Physiol Cell Physiol 273: C1168–C1175, 1997.
361. Gao XH, Dwivedi PP, Omdahl JL, Morris HA, May BK. Calcitonin stimulates expres-sion of the rat 25-hydroxyvitamin D3-24-hydroxylase (CYP24) promoter in HEK-293 cells expressing calcitonin receptor: identification of signaling pathways. J MolEndocrinol 32: 87–98, 2004.
362. Garfia B, Canadillas S, Canalejo A, Luque F, Siendones E, Quesada M, Almaden Y,Aguilera-Tejero E, Rodriguez M. Regulation of parathyroid vitamin D receptor ex-pression by extracellular calcium. J Am Soc Nephrol 13: 2945–2952, 2002.
363. Garland C, Shekelle RB, Barrett-Connor E, Criqui MH, Rossof AH, Paul O. Dietaryvitamin D and calcium and risk of colorectal cancer: a 19-year prospective study inmen. Lancet 1: 307–309, 1985.
364. Garland FC, Garland CF, Gorham ED, Young JF. Geographic variation in breastcancer mortality in the United States: a hypothesis involving exposure to solar radi-ation. Prev Med 19: 614–622, 1990.
365. Garner SC, Pi M, Tu Q, Quarles LD. Rickets in cation-sensing receptor-deficientmice: an unexpected skeletal phenotype. Endocrinology 142: 3996–4005, 2001.
366. Garrett JE, Capuano IV, Hammerland LG, Hung BC, Brown EM, Hebert SC, Nem-eth EF, Fuller F. Molecular cloning and functional expression of human parathyroidcalcium receptor cDNAs. J Biol Chem 270: 12919–12925, 1995.
367. Garrett JE, Tamir H, Kifor O, Simin RT, Rogers KV, Mithal A, Gagel RF, Brown EM.Calcitonin-secreting cells of the thyroid express an extracellular calcium receptorgene. Endocrinology 136: 5202–5211, 1995.
368. Garrick R, Ireland AW, Posen S. Bone abnormalities after gastric surgery. A prospec-tive histological study. Ann Intern Med 75: 221–225, 1971.
369. Garuti R, Croce MA, Piccinini L, Tiozzo R, Bertolini S, Calandra S. Functional analysisof the promoter of human sterol 27-hydroxylase gene in HepG2 cells. Gene 283:133–143, 2002.
370. Gascon-Barre M, Demers C, Ghrab O, Theodoropoulos C, Lapointe R, Jones G,Valiquette L, Menard D. Expression of CYP27A, a gene encoding a vitamin D-25hydroxylase in human liver and kidney. Clin Endocrinol 54: 107–115, 2001.
371. Geibel J, Sritharan K, Geibel R, Geibel P, Persing JS, Seeger A, Roepke TK, Deich-stetter M, Prinz C, Cheng SX, Martin D, Hebert SC. Calcium-sensing receptorabrogates secretagogue-induced increases in intestinal net fluid secretion by enhanc-ing cyclic nucleotide destruction. Proc Natl Acad Sci USA 103: 9390–9397, 2006.
372. Geibel JP, Hebert SC. The functions and roles of the extracellular Ca2�-sensingreceptor along the gastrointestinal tract. Annu Rev Physiol 71: 205–217, 2009.
373. Geibel JP, Wagner CA, Caroppo R, Qureshi I, Gloeckner J, Manuelidis L, Kirchhoff P,Radebold K. The stomach divalent ion-sensing receptor scar is a modulator of gastricacid secretion. J Biol Chem 276: 39549–39552, 2001.
374. Gerber JG, Payne NA. Secretin inhibits canine gastric acid secretion in response topentagastrin by modulating gastric histamine release. J Pharmacol Exp Ther 279:718–723, 1996.
375. Gerbino A, Ruder WC, Curci S, Pozzan T, Zaccolo M, Hofer AM. Termination ofcAMP signals by Ca2� and G�i via extracellular Ca2� sensors: a link to intracellularCa2� oscillations. J Cell Biol 171: 303–312, 2005.
376. Gerhard M, Neumayer N, Presecan-Siedel E, Zanner R, Lengyel E, Cramer T,Hocker M, Prinz C. Gastrin induces expression and promoter activity of the vesicularmonoamine transporter subtype 2. Endocrinology 142: 3663–3672, 2001.
377. Germain N, Galusca B, Le Roux CW, Bossu C, Ghatei MA, Lang F, Bloom SR, EstourB. Constitutional thinness and lean anorexia nervosa display opposite concentrationsof peptide YY, glucagon-like peptide 1, ghrelin, and leptin. Am J Clin Nutr 85: 967–971, 2007.
378. Gertner JM, Lilburn M, Domenech M. 25-Hydroxycholecalciferol absorption in ste-atorrhoea and postgastrectomy osteomalacia. Br Med J 1: 1310–1312, 1977.
379. Gesek FA, Friedman PA. On the mechanism of parathyroid hormone stimulation ofcalcium uptake by mouse distal convoluted tubule cells. J Clin Invest 90: 749–758,1992.
380. Gesty-Palmer D, Chen M, Reiter E, Ahn S, Nelson CD, Wang S, Eckhardt AE, CowanCL, Spurney RF, Luttrell LM, Lefkowitz RJ. Distinct beta-arrestin- and G protein-dependent pathways for parathyroid hormone receptor-stimulated ERK1/2 activa-tion. J Biol Chem 281: 10856–10864, 2006.
381. Gesty-Palmer D, Flannery P, Yuan L, Corsino L, Spurney R, Lefkowitz RJ, LuttrellLM. A beta-arrestin-biased agonist of the parathyroid hormone receptor (PTH1R)promotes bone formation independent of G protein activation. Sci Transl Med 1:1ra1, 2009.
382. Ghijsen WE, De Jong MD, Van Os CH. Kinetic properties of Na�/Ca2� exchange inbasolateral plasma membranes of rat small intestine. Biochim Biophys Acta 730: 85–94, 1983.
383. Gilardi F, Viviani B, Galmozzi A, Boraso M, Bartesaghi S, Torri A, Caruso D, CrestaniM, Marinovich M, de Fabiani E. Expression of sterol 27-hydroxylase in glial cells andits regulation by liver X receptor signaling. Neuroscience 164: 530–540, 2009.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
247Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

384. Gisbert JP, Gonzalez L, Calvet X, Roque M, Gabriel R, Pajares JM. Proton pumpinhibitors versus H2-antagonists: a meta-analysis of their efficacy in treating bleedingpeptic ulcer. Aliment Pharmacol Ther 15: 917–926, 2001.
385. Goldblatt H, Soames KM. Studies on the fat-soluble growth-promoting factor.Biochem J 17: 446, 1923.
386. Goldenring JR, Shen KR, Vaughan HD, Modlin IM. Identification of a small GTP-binding protein, Rab25, expressed in the gastrointestinal mucosa, kidney, and lung. JBiol Chem 268: 18419–18422, 1993.
387. Goldenring JR, Soroka CJ, Shen KR, Tang LH, Rodriguez W, Vaughan HD, Stoch SA,Modlin IM. Enrichment of rab11, a small GTP-binding protein, in gastric parietal cells.Am J Physiol Gastrointest Liver Physiol 267: G187–G194, 1994.
388. Gonnelli S, Caffarelli C, Del Santo K, Cadirni A, Guerriero C, Lucani B, Franci B, NutiR. The relationship of ghrelin and adiponectin with bone mineral density and boneturnover markers in elderly men. Calcif Tissue Int 83: 55–60, 2008.
389. Gorn AH, Rudolph SM, Flannery MR, Morton CC, Weremowicz S, Wang TZ, KraneSM, Goldring SR. Expression of two human skeletal calcitonin receptor isoformscloned from a giant cell tumor of bone. The first intracellular domain modulatesligand binding and signal transduction. J Clin Invest 95: 2680–2691, 1995.
390. Goss SL, Lemons KA, Kerstetter JE, Bogner RH. Determination of calcium saltsolubility with changes in pH and PCO2, simulating varying gastrointestinal environ-ments. J Pharm Pharmacol 59: 1485–1492, 2007.
391. Grahammer F, Herling AW, Lang HJ, Schmitt-Graff A, Wittekindt OH, Nitschke R,Bleich M, Barhanin J, Warth R. The cardiac K� channel KCNQ1 is essential for gastricacid secretion. Gastroenterology 120: 1363–1371, 2001.
392. Grauschopf U, Lilie H, Honold K, Wozny M, Reusch D, Esswein A, Schafer W,Rucknagel KP, Rudolph R. The N-terminal fragment of human parathyroid hormonereceptor 1 constitutes a hormone binding domain and reveals a distinct disulfidepattern. Biochemistry 39: 8878–8887, 2000.
393. Gray RW, Omdahl JL, Ghazarian JG, DeLuca HF Hydroxycholecalciferol-1-hydrox-ylase. Subcellular location and properties. J Biol Chem 247: 7528–7532, 1972.
394. Gray SL, Lacroix AZ, Larson J, Robbins J, Cauley JA, Manson JE, Chen Z. Protonpump inhibitor use, hip fracture, and change in bone mineral density in postmeno-pausal women: results from the women’s health initiative. Arch Internal Med 170:765–771, 2010.
395. Graziani G, Badalamenti S, Como G, Gallieni M, Finazzi S, Angelini C, Brancaccio D,Ponticelli C. Calcium and phosphate plasma levels in dialysis patients after dietaryCa-P overload: Role of gastric acid secretion. Nephron 91: 474–479, 2002.
396. Graziani G, Como G, Badalamenti S, Finazzi S, Malesci A, Gallieni M, Brancaccio D,Ponticelli C. Effect of gastric acid secretion on intestinal phosphate and calciumabsorption in normal subjects. Nephrology Dialysis Transplantation 10: 1376–1380,1995.
397. Green T, Dockray GJ. Characterization of the peptidergic afferent innervation of thestomach in the rat, mouse and guinea-pig. Neuroscience 25: 181–193, 1988.
398. Gregory DH, Van Uelft R. Calcium absorption following gastric resection. Am JGastroenterol 57: 34–40, 1972.
399. Gregory RA, Tracy HJ. The constitution and properties of two gastrins extractedfrom hog antral mucosa. Gut 5: 103–114, 1964.
400. Grisso JA, Kelsey JL, O’Brien LA, Miles CG, Sidney S, Maislin G, LaPann K, Moritz D,Peters B. Risk factors for hip fracture in men. Am J Epidemiol 145: 786–793, 1997.
401. Gunness-Hey M, Hock JM. Increased trabecular bone mass in rats treated withhuman synthetic parathyroid hormone. Metab Bone Dis Relat Res 5: 177–181, 1984.
402. Guo YD, Strugnell S, Back DW, Jones G. Transfected human liver cytochrome P-450hydroxylates vitamin D analogs at different side-chain positions. Proc Natl Acad SciUSA 90: 8668–8672, 1993.
403. Gupta RP, Patrick K, Bell NH. Mutational analysis of CYP27A1: assessment of 27-hydroxylation of cholesterol and 25-hydroxylation of vitamin D. Metabolism 56:1248–1255, 2007.
404. Gyomorey K, Yeger H, Ackerley C, Garami E, Bear CE. Expression of the chloridechannel ClC-2 in the murine small intestine epithelium. Am J Physiol Cell Physiol (couldnot determine journal name) 279: 1787–1794, 2000.
405. Habener JF, Singer FR, Deftos LJ, Neer RM, Potts JT Jr. Explanation for unusualpotency of salmon calcitonin. Nat New Biol 232: 91–92, 1971.
406. Haddad JG, Hillman L, Rojanasathit S. Human serum binding capacity and affinity for25-hydroxyergocalciferol and 25-hydroxycholecalciferol. J Clin Endocrinol Metab 43:86–91, 1976.
407. Haddad JG, Jennings AS, Aw TC. Vitamin D uptake and metabolism by perfused ratliver: influences of carrier proteins. Endocrinology 123: 498–504, 1988.
408. Haddad JG Jr, Walgate J. 25-Hydroxyvitamin D transport in human plasma. Isolationand partial characterization of calcifidiol-binding protein. J Biol Chem 251: 4803–4809, 1976.
409. Haddad JG Jr, Walgate J. Radioimmunoassay of the binding protein for vitamin D andits metabolites in human serum: concentrations in normal subjects and patients withdisorders of mineral homeostasis. J Clin Invest 58: 1217–1222, 1976.
410. Hakanson R, Blom H, Carlsson E, Larsson H, Ryberg B, Sundler F. Hypergastrinae-mia produces trophic effects in stomach but not in pancreas and intestines. RegulPept 13: 225–233, 1986.
411. Hakanson R, Ding XQ, Norlen P, Chen D. Circulating pancreastatin is a marker forthe enterochromaffin-like cells of the rat stomach. Gastroenterology 108: 1445–1452, 1995.
412. Hakanson R, Liedberg G. The role of endogenous gastrin in the activation of gastrichistidine decarboxylase in the rat. Effect of antrectomy and vagal denervation. Eur JPharmacol 12: 94–103, 1970.
413. Hakanson R, Owman C. Concomitant histochemical demonstration of histamineand catecholamines in enterochromaffin-like cells of gastric mucosa. Life Sci 6: 759–766, 1967.
414. Hammer RA, Fernandez C, Ertan A, Arimura A. Anesthetic dependence of theinhibitory effect of neurotensin on pentagastrin-stimulated acid secretion in rats. Apossible role for somatostatin. Life Sci 48: 333–339, 1991.
415. Handlogten ME, Huang C, Shiraishi N, Awata H, Miller RT. The Ca2�-sensing re-ceptor activates cytosolic phospholipase A2 via a Gqalpha-dependent ERK-indepen-dent pathway. J Biol Chem 276: 13941–13948, 2001.
416. Handlogten ME, Shiraishi N, Awata H, Huang C, Miller RT. Extracellular Ca2�-sensing receptor is a promiscuous divalent cation sensor that responds to lead. Am JPhysiol Renal Physiol 279: F1083–F1091, 2000.
417. Hanley DA, Ayer LM. Calcium-dependent release of carboxyl-terminal fragments ofparathyroid hormone by hyperplastic human parathyroid tissue in vitro. J Clin Endo-crinol Metab 63: 1075–1079, 1986.
418. Hanley DA, Takatsuki K, Sultan JM, Schneider AB, Sherwood LM. Direct release ofparathyroid hormone fragments from functioning bovine parathyroid glands in vitro.J Clin Invest 62: 1247–1254, 1978.
419. Hansen CP. The pharmacokinetics and pharmacodynamics of progastrin-derivedpeptides. Dan Med Bull 50: 310–319, 2003.
420. Hansen CP, Goetze JP, Stadil F, Rehfeld JF. Excretion of progastrin products inhuman urine. Am J Physiol Gastrointest Liver Physiol 276: G985–G992, 1999.
421. Hansen KE, Jones AN, Lindstrom MJ, Davis LA, Ziegler TE, Penniston KL, Alvig AL,Shafer MM. Do proton pump inhibitors decrease calcium absorption? J Bone MinerRes 25: 2510–2519, 2010.
422. Hanzlik RP, Fowler SC, Fisher DH. Relative bioavailability of calcium from calciumformate, calcium citrate, and calcium carbonate. J Pharmacol Exp Ther 313: 1217–1222, 2005.
423. Hardy P, Sechet A, Hottelart C, Oprisiu R, Abighanem O, Said S, Rasombololona M,Brazier M, Moriniere P, Achard JM, Pruna A, Fournier A. Inhibition of gastric secre-tion by omeprazole and efficiency of calcium carbonate on the control of hyperphos-phatemia in patients on chronic hemodialysis. Artificial Organs 22: 569–573, 1998.
424. Harmeyer J, Deluca HF. Calcium-binding protein and calcium absorption after vita-min D administration. Arch Biochem Biophys 133: 247–254, 1969.
425. Hartmann M, Theiss U, Huber R, Luhmann R, Bliesath H, Wurst W, Lucker PW.Twenty-four-hour intragastric pH profiles and pharmacokinetics following single andrepeated oral administration of the proton pump inhibitor pantoprazole in compar-ison to omeprazole. Aliment Pharmacol Ther 10: 359–366, 1996.
SASCHA KOPIC AND JOHN P. GEIBEL
248 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

426. Hasebe K, Horie S, Komasaka M, Yano S, Watanabe K. Stimulatory effects of nitricoxide donors on gastric acid secretion in isolated mouse stomach. Eur J Pharmacol420: 159–164, 2001.
427. Hashizume Y, Waguri S, Watanabe T, Kominami E, Uchiyama Y. Cysteine protein-ases in rat parathyroid cells with special reference to their correlation with parathy-roid hormone (PTH) in storage granules. J Histochem Cytochem 41: 273–282, 1993.
428. Hattersley G and Chambers TJ. Calcitonin receptors as markers for osteoclasticdifferentiation: correlation between generation of bone-resorptive cells and cellsthat express calcitonin receptors in mouse bone marrow cultures. Endocrinology125: 1606–1612, 1989.
429. Haussler MR, Myrtle JF, Norman AW. The association of a metabolite of vitamin D3
with intestinal mucosa chromatin in vivo. J Biol Chem 243: 4055–4064, 1968.
430. Haussler MR, Norman AW. Chromosomal receptor for a vitamin D metabolite. ProcNatl Acad Sci USA 62: 155–162, 1969.
431. He W, Liu W, Chew CS, Baker SS, Baker RD, Forte JG, Zhu L. Acid secretion-associated translocation of KCNJ15 in gastric parietal cells. Am J Physiol GastrointestLiver Physiol 301: G591–G600, 2011.
432. Heaney RP, Dowell MS, Bierman J, Hale CA, Bendich A. Absorbability and costeffectiveness in calcium supplementation. J Am Coll Nutr 20: 239–246, 2001.
433. Heaney RP, Recker RR, Weaver CM. Absorbability of calcium sources: the limitedrole of solubility. Calcified Tissue Int 46: 300–304, 1990.
434. Hebert SC, Brown EM, Harris HW. Role of the Ca2�-sensing receptor in divalentmineral ion homeostasis. J Exp Biol 200: 295–302, 1997.
435. Heersche JN, Marcus R, Aurbach GD. Calcitonin and the formation of 3=,5=-AMP inbone and kidney. Endocrinology 94: 241–247, 1974.
436. Heitzmann D, Koren V, Wagner M, Sterner C, Reichold M, Tegtmeier I, Volk T,Warth R. KCNE beta subunits determine pH sensitivity of KCNQ1 potassium chan-nels. Cell Physiol Biochem 19: 21–32, 2007.
437. Helander KG, Bamberg K, Sachs G, Melle D, Helander HF. Localization of mRNA forthe muscarinic M1 receptor in rat stomach. Biochim Biophys Acta 1312: 158–162,1996.
438. Heller HJ, Greer LG, Haynes SD, Poindexter JR, Pak CY. Pharmacokinetic andpharmacodynamic comparison of two calcium supplements in postmenopausalwomen. J Clin Pharmacol 40: 1237–1244, 2000.
439. Heller HJ, Stewart A, Haynes S, Pak CY. Pharmacokinetics of calcium absorptionfrom two commercial calcium supplements. J Clin Pharmacol 39: 1151–1154, 1999.
440. Hendy GN, Kronenberg HM, Potts JT Jr, Rich A. Nucleotide sequence of clonedcDNAs encoding human preproparathyroid hormone. Proc Natl Acad Sci USA 78:7365–7369, 1981.
441. Hennessy JF, Wells SA Jr, Ontjes DA, Cooper CW. A comparison of pentagastrininjection and calcium infusion as provocative agents for the detection of medullarycarcinoma of the thyroid. J Clin Endocrinol Metab 39: 487–495, 1974.
442. Henry HL. Parathyroid hormone modulation of 25-hydroxyvitamin D3 metabolismby cultured chick kidney cells is mimicked and enhanced by forskolin. Endocrinology116: 503–510, 1985.
443. Henry HL. Regulation of the hydroxylation of 25-hydroxyvitamin D3 in vivo and inprimary cultures of chick kidney cells. J Biol Chem 254: 2722–2729, 1979.
444. Herberth J, Fahrleitner-Pammer A, Obermayer-Pietsch B, Krisper P, Holzer H,Malluche HH, Dobnig H. Changes in total parathyroid hormone (PTH), PTH-(1–84)and large C-PTH fragments in different stages of chronic kidney disease. Clin Nephrol65: 328–334, 2006.
445. Herlong HF, Recker RR, Maddrey WC. Bone disease in primary biliary cirrhosis:histologic features and response to 25-hydroxyvitamin D. Gastroenterology 83: 103–108, 1982.
446. Hess AF. The prevention and cure of rickets by sunlight. Am J Public Health 12:104–107, 1922.
447. Hess AF, Unger LJ. The cure of infantile rickets by sunlight. J Am Med Assoc 77: 39,1921.
448. Hess AF, Weinstock M. Antirachitic properties imparted to inert fluids by ultravioletirradiation. Proc Soc Exp Biol Med 22: 6–7, 1924.
449. Hess AF, Weinstock M. Antirachitic properties imparted to lettuce and to growingwheat by ultraviolet irradiation. Proc Soc Exp Biol Med 22: 5, 1924.
450. Hess AF, Weinstock M. A further report on imparting antirachitic properties to inertsubstances by ultra-violet irradiation. J Biol Chem 63: 297–307, 1925.
451. Hewison M, Burke F, Evans KN, Lammas DA, Sansom DM, Liu P, Modlin RL, AdamsJS. Extra-renal 25-hydroxyvitamin D3-1alpha-hydroxylase in human health and dis-ease. J Steroid Biochem Mol Biol 103: 316–321, 2007.
452. Hewison M, Freeman L, Hughes SV, Evans KN, Bland R, Eliopoulos AG, Kilby MD,Moss PA, Chakraverty R. Differential regulation of vitamin D receptor and its ligandin human monocyte-derived dendritic cells. J Immunol 170: 5382–5390, 2003.
453. Hewison M, Zehnder D, Chakraverty R, Adams JS. Vitamin D and barrier function: anovel role for extra-renal 1 alpha-hydroxylase. Mol Cell Endocrinol 215: 31–38, 2004.
454. Heynen G, Brassine A, Daubresse JC, Ligny G, Kanis JA, Gaspar S, Franchimont P.Lack of clinical and physiological relationship between gastrin and calcitonin in man.Eur J Clin Invest 11: 331–335, 1981.
455. Higham A, Noble P, Thompson DG, Dockray GJ. Increased sensitivity of gastrin cellsto gastric distension following antral denervation in the rat. J Physiol 503: 169–175,1997.
456. Hildebrand P, Lehmann FS, Ketterer S, Christ AD, Stingelin T, Beltinger J, GibbonsAH, Coy DH, Calam J, Larsen F, Beglinger C. Regulation of gastric function byendogenous gastrin releasing peptide in humans: studies with a specific gastrin re-leasing peptide receptor antagonist. Gut 49: 23–28, 2001.
457. Hildmann B, Schmidt A, Murer H. Ca2�-transport across basal-lateral plasma mem-branes from rat small intestinal epithelial cells. J Membr Biol 65: 55–62, 1982.
458. Hill LF, Van den Berg CJ, Mawer EB. Vitamin D metabolism in experimental uraemia:effects on intestinal transport 45Ca and on formation of 1,25-dihydroxycholecalcif-erol in rat. Nat New Biol 232: 189–191, 1971.
459. Hills DM, Gerskowitch VP, Roberts SP, Welsh NJ, Shankley NP, Black JW. Pharma-cological analysis of the CCKB/gastrin receptors mediating pentagastrin-stimulatedgastric acid secretion in the isolated stomach of the immature rat. Br J Pharmacol 119:1401–1410, 1996.
460. Hinata M, Yamamura H, Li L, Watanabe Y, Watano T, Imaizumi Y, Kimura J. Stoi-chiometry of Na�-Ca2� exchange is 3:1 in guinea-pig ventricular myocytes. J Physiol545: 453–461, 2002.
461. Hirnet D, Olausson J, Fecher-Trost C, Bodding M, Nastainczyk W, Wissenbach U,Flockerzi V, Freichel M. The TRPV6 gene, cDNA and protein. Cell Calcium 33:509–518, 2003.
462. Hirsch PF, Baruch H. Is calcitonin an important physiological substance? Endocrine21: 201–208, 2003.
463. Hirsch PF, Gauthier GF, Munson PL. Thyroid hypocalcemic principle and recurrentlaryngeal nerve injury as factors affecting the response to parathyroidectomy in rats.Endocrinology 73: 244–252, 1963.
464. Hirschfeld J. Immune-electrophoretic demonstration of qualitative differences inhuman sera and their relation to the haptoglobins. Acta Pathol Microbiol Scand 47:160–168, 1959.
465. Hirschfeld J. Individual precipitation patterns of normal rabbit sera. A preliminaryreport. Acta Pathol Microbiol Scand 46: 229–238, 1959.
466. Hirschowitz BI, Fong J, Molina E. Effects of pirenzepine and atropine on vagal andcholinergic gastric secretion and gastrin release and on heart rate in the dog. JPharmacol Exp Ther 225: 263–268, 1983.
467. Hjalm G, MacLeod RJ, Kifor O, Chattopadhyay N, Brown EM. Filamin-A binds to thecarboxyl-terminal tail of the calcium-sensing receptor, an interaction that partici-pates in CaR-mediated activation of mitogen-activated protein kinase. J Biol Chem276: 34880–34887, 2001.
468. Hoag HM, Martel J, Gauthier C, Tenenhouse HS. Effects of Npt2 gene ablation andlow-phosphate diet on renal Na�/phosphate cotransport and cotransporter geneexpression. J Clin Invest 104: 679–686, 1999.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
249Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

469. Hock JM, Gera I. Effects of continuous and intermittent administration and inhibitionof resorption on the anabolic response of bone to parathyroid hormone. J Bone MinerRes 7: 65–72, 1992.
470. Hocker M, Henihan RJ, Rosewicz S, Riecken EO, Zhang Z, Koh TJ, Wang TC. Gastrinand phorbol 12-myristate 13-acetate regulate the human histidine decarboxylasepromoter through Raf-dependent activation of extracellular signal-regulated kinase-related signaling pathways in gastric cancer cells. J Biol Chem 272: 27015–27024,1997.
471. Hocker M, John M, Anagnostopoulos J, Buhr HJ, Solimena M, Gasnier B, Henry JP,Wang TC, Wiedenmann B. Molecular dissection of regulated secretory pathways inhuman gastric enterochromaffin-like cells: an immunohistochemical analysis. His-tochem Cell Biol 112: 205–214, 1999.
472. Hocker M, Zhang Z, Fenstermacher DA, Tagerud S, Chulak M, Joseph D, Wang TC.Rat histidine decarboxylase promoter is regulated by gastrin through a protein kinaseC pathway. Am J Physiol Gastrointest Liver Physiol 270: G619–G633, 1996.
473. Hoenderop JG, Nilius B, Bindels RJ. Calcium absorption across epithelia. Physiol Rev85: 373–422, 2005.
474. Hoenderop JG, van der Kemp AW, Hartog A, van de Graaf SF, van Os CH, WillemsPH, Bindels RJ. Molecular identification of the apical Ca2� channel in 1,25-dihy-droxyvitamin D3-responsive epithelia. J Biol Chem 274: 8375–8378, 1999.
475. Hoenderop JG, Vennekens R, Muller D, Prenen J, Droogmans G, Bindels RJ, Nilius B.Function and expression of the epithelial Ca2� channel family: comparison of mam-malian ECaC1 and 2. J Physiol 537: 747–761, 2001.
476. Hoenderop JG, Voets T, Hoefs S, Weidema F, Prenen J, Nilius B, Bindels RJ. Homo-and heterotetrameric architecture of the epithelial Ca2� channels TRPV5 andTRPV6. EMBO J 22: 776–785, 2003.
477. Hohne-Zell B, Galler A, Schepp W, Gratzl M, Prinz C. Functional importance ofsynaptobrevin and SNAP-25 during exocytosis of histamine by rat gastric entero-chromaffin-like cells. Endocrinology 138: 5518–5526, 1997.
478. Holick MF, Chen TC, Lu Z, Sauter E. Vitamin D and skin physiology: a D-lightfulstory. J Bone Miner Res 22 Suppl 2: V28–33, 2007.
479. Holick MF, MacLaughlin JA, Clark MB, Holick SA, Potts JT Jr, Anderson RR, Blank IH,Parrish JA, Elias P. Photosynthesis of previtamin D3 in human skin and the physiologicconsequences. Science 210: 203–205, 1980.
480. Holick MF, Schnoes HK, DeLuca HF, Suda T, Cousins RJ. Isolation and identificationof 1,25-dihydroxycholecalciferol. A metabolite of vitamin D active in intestine. Bio-chemistry 10: 2799–2804, 1971.
481. Hollande F, Gusdinar T, Bali JP, Magous R. Neurohormonal regulation of histaminerelease from isolated rabbit fundic mucosal cells. Agents Actions 38: 149–157, 1993.
482. Hollande F, Imdahl A, Mantamadiotis T, Ciccotosto GD, Shulkes A, Baldwin GS.Glycine-extended gastrin acts as an autocrine growth factor in a nontransformedcolon cell line. Gastroenterology 113: 1576–1588, 1997.
483. Hollander D, Muralidhara KS, Zimmerman A. Vitamin D-3 intestinal absorption invivo: influence of fatty acids, bile salts, and perfusate pH on absorption. Gut 19:267–272, 1978.
484. Hollander D, Truscott TC. Mechanism and site of small intestinal uptake of vitaminD3 in pharmacological concentrations. Am J Clin Nutr 29: 970–975, 1976.
485. Holst MC, Kelly JB, Powley TL. Vagal preganglionic projections to the enteric ner-vous system characterized with Phaseolus vulgaris-leucoagglutinin. J Comp Neurol381: 81–100, 1997.
486. Holst Pedersen J, Skov Olsen P, Kirkegaard P. Effect of neurotensin and neurotensinfragments on gastric acid secretion in man. Regul Pept 15: 77–86, 1986.
487. Holtrop ME, Raisz LG, Simmons HA. The effects of parathyroid hormone, colchi-cine, and calcitonin on the ultrastructure and the activity of osteoclasts in organculture. J Cell Biol 60: 346–355, 1974.
488. Hori K, Takahashi Y, Horikawa N, Furukawa T, Tsukada K, Takeguchi N, Sakai H. Isthe ClC-2 chloride channel involved in the Cl� secretory mechanism of gastricparietal cells? FEBS Lett 575: 105–108, 2004.
489. Horst R, Prapong S, Reinhardt T, Koszewski N, Knutson J, Bishop C. Comparison ofthe relative effects of 1,24-dihydroxyvitamin D(2) [1, 24-(OH)(2)D(2)], 1,24-dihy-
droxyvitamin D(3) [1,24-(OH)(2)D(3)], 1,25-dihydroxyvitamin D(3) [1,25-(OH)(2)D(3)] on selected vitamin D-regulated events in the rat. Biochem Pharmacol60: 701–708, 2000.
490. Horsting M, DeLuca HF. In vitro production of 25-hydroxycholecalciferol. BiochemBiophys Res Commun 36: 251–256, 1969.
491. Hosoda H, Kojima M, Matsuo H, Kangawa K. Ghrelin and des-acyl ghrelin: two majorforms of rat ghrelin peptide in gastrointestinal tissue. Biochem Biophys Res Commun279: 909–913, 2000.
492. Howard A, Legon S, Walters JR. Human and rat intestinal plasma membrane calciumpump isoforms. Am J Physiol Gastrointest Liver Physiol 265: G917–G925, 1993.
493. Huan J, Olgaard K, Nielsen LB, Lewin E. Parathyroid hormone 7–84 induces hy-pocalcemia and inhibits the parathyroid hormone 1–84 secretory response to hy-pocalcemia in rats with intact parathyroid glands. J Am Soc Nephrol 17: 1923–1930,2006.
494. Huang C, Handlogten ME, Miller RT. Parallel activation of phosphatidylinositol 4-ki-nase and phospholipase C by the extracellular calcium-sensing receptor. J Biol Chem277: 20293–20300, 2002.
495. Huang C, Hujer KM, Wu Z, Miller RT. The Ca2�-sensing receptor couples toG�12/13 to activate phospholipase D in Madin-Darby canine kidney cells. Am J PhysiolCell Physiol 286: C22–C30, 2004.
496. Huang C, Wu Z, Hujer KM, Miller RT. Silencing of filamin A gene expression inhibitsCa2�-sensing receptor signaling. FEBS Lett 580: 1795–1800, 2006.
497. Huang JC, Sakata T, Pfleger LL, Bencsik M, Halloran BP, Bikle DD, Nissenson RA.PTH differentially regulates expression of RANKL and OPG. J Bone Miner Res 19:235–244, 2004.
498. Huang Y, Niwa J, Sobue G, Breitwieser GE. Calcium-sensing receptor ubiquitinationand degradation mediated by the E3 ubiquitin ligase dorfin. J Biol Chem 281: 11610–11617, 2006.
499. Huang Y, Zhou Y, Castiblanco A, Yang W, Brown EM, Yang JJ. Multiple Ca2�-bindingsites in the extracellular domain of the Ca2�-sensing receptor corresponding tocooperative Ca2� response. Biochemistry 48: 388–398, 2009.
500. Huang Y, Zhou Y, Yang W, Butters R, Lee HW, Li S, Castiblanco A, Brown EM, YangJJ. Identification and dissection of Ca2�-binding sites in the extracellular domain ofCa2�-sensing receptor. J Biol Chem 282: 19000–19010, 2007.
501. Huda MS, Durham BH, Wong SP, Dovey TM, McCulloch P, Kerrigan D, Pinkney JH,Fraser WD, Wilding JP. Lack of an acute effect of ghrelin on markers of boneturnover in healthy controls and post-gastrectomy subjects. Bone 41: 406–413,2007.
502. Hughes DA, Tang K, Strotmann R, Schoneberg T, Prenen J, Nilius B, Stoneking M.Parallel selection on TRPV6 in human populations. PLoS ONE 3: e1686, 2008.
503. Huhtakangas JA, Olivera CJ, Bishop JE, Zanello LP, Norman AW. The vitamin Dreceptor is present in caveolae-enriched plasma membranes and binds 1alpha,25(OH)2-vitamin D3 in vivo and in vitro. Mol Endocrinol 18: 2660–2671, 2004.
504. Huldschinsky K. Heilung von Rachitis durch künstliche Höhensonne. Deutsche MedWochenschrift 45: 712, 1919.
505. Hume EM, Smith HH. The effect of irradiation of the environment with ultra-violetlight upon the growth and calcification of rats, fed on a diet deficient in fat-solublevitamins: the part played by irradiated sawdust. Biochem J 18: 1334–1345, 1924.
506. Humphries TJ, Merritt GJ. Review article: drug interactions with agents used to treatacid-related diseases. Aliment Pharmacol Ther 13 Suppl 3: 18–26, 1999.
507. Hunyady B, Mezey E, Pacak K, Harta G, Palkovits M. Distribution of muscarinicreceptor mRNAs in the stomachs of normal or immobilized rats. Inflammopharma-cology 4: 399–413, 1996.
508. Ichikawa F, Sato K, Nanjo M, Nishii Y, Shinki T, Takahashi N, Suda T. Mouse primaryosteoblasts express vitamin D3 25-hydroxylase mRNA and convert 1 alpha-hy-droxyvitamin D3 into 1 alpha,25-dihydroxyvitamin D3. Bone 16: 129–135, 1995.
509. Imai M. Calcium transport across the rabbit thick ascending limb of Henle’s loopperfused in vitro. Pflügers Arch 374: 255–263, 1978.
SASCHA KOPIC AND JOHN P. GEIBEL
250 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

510. Imanishi Y, Kawata T, Kenko T, Wada M, Nagano N, Miki T, Arnold A, Inaba M.Cinacalcet HCl suppresses Cyclin D1 oncogene-derived parathyroid cell prolifera-tion in a murine model for primary hyperparathyroidism. Calcif Tissue Int 89: 29–35,2011.
511. Imawari M, Kozawa K, Akanuma Y, Koizumi S, Itakura H, Kosaka K. Serum 25-hydroxyvitamin D and vitamin D-binding protein levels and mineral metabolism afterpartial and total gastrectomy. Gastroenterology 79: 255–258, 1980.
512. IMSHealth. Top Products by U.S. Spending 2010 http://www.imshealth.com/deployedfiles/ims/Global/Content/Corporate/Press%20Room/Top-line%20Market%20Data/2010%20Top-line%20Market%20Data/2010_Top_Products_by_Sales.pdf [retrieved November 2011].
513. Inoue Y, Segawa H, Kaneko I, Yamanaka S, Kusano K, Kawakami E, Furutani J, Ito M,Kuwahata M, Saito H, Fukushima N, Kato S, Kanayama HO, Miyamoto K. Role of thevitamin D receptor in FGF23 action on phosphate metabolism. Biochem J 390: 325–331, 2005.
514. Irving AD, Smith G, Catto GR. Does metabolic bone disease follow truncal vagotomyand gastrojejunostomy? Br Med J 287: 1516, 1983.
515. Isenberg JI, Walsh JH, Grossman MI. Zollinger-Ellison syndrome. Gastroenterology65: 140–165, 1973.
516. Ishizaki T, Horai Y. Review article: cytochrome P450 and the metabolism of protonpump inhibitors–emphasis on rabeprazole. Aliment Pharmacol Ther 13 Suppl 3: 27–36, 1999.
517. Ishizawa M, Matsunawa M, Adachi R, Uno S, Ikeda K, Masuno H, Shimizu M, IwasakiK, Yamada S, Makishima M. Lithocholic acid derivatives act as selective vitamin Dreceptor modulators without inducing hypercalcemia. J Lipid Res 49: 763–772, 2008.
518. Ishizuya T, Yokose S, Hori M, Noda T, Suda T, Yoshiki S, Yamaguchi A. Parathyroidhormone exerts disparate effects on osteoblast differentiation depending on expo-sure time in rat osteoblastic cells. J Clin Invest 99: 2961–2970, 1997.
519. Ito R, Sato K, Helmer T, Jay G, Agarwal K. Structural analysis of the gene encodinghuman gastrin: the large intron contains an Alu sequence. Proc Natl Acad Sci USA 81:4662–4666, 1984.
520. Ivanovich P, Fellows H, Rich C. The absorption of calcium carbonate. Ann Intern Med66: 917–923, 1967.
521. Jaffe BM, Kopen DF, Lazan DW. Endogenous serotonin in the control of gastric acidsecretion. Surgery 82: 156–163, 1977.
522. Jain RN, Al-Menhali AA, Keeley TM, Ren J, El-Zaatari M, Chen X, Merchant JL, RossTS, Chew CS, Samuelson LC. Hip1r is expressed in gastric parietal cells and isrequired for tubulovesicle formation and cell survival in mice. J Clin Invest 118:2459–2470, 2008.
523. Jain RN, Samuelson LC. Transcriptional profiling of gastrin-regulated genes in mousestomach. Physiol Genomics 29: 1–12, 2007.
524. Jarrousse C, Audousset-Puech MP, Dubrasquet M, Niel H, Martinez J, Bataille D.Oxyntomodulin (glucagon-37) and its C-terminal octapeptide inhibit gastric acidsecretion. FEBS Lett 188: 81–84, 1985.
525. Jarrousse C, Niel H, Audousset-Puech MP, Martinez J, Bataille D. Oxyntomodulinand its C-terminal octapeptide inhibit liquid meal-stimulated acid secretion. Peptides7 Suppl 1: 253–256, 1986.
526. Jeffery DA, Roufogalis BD, Katz S. The effect of calmodulin on the phosphoproteinintermediate of Mg2�-dependent Ca2�-stimulated adenosine triphosphatase in hu-man erythrocyte membranes. Biochem J 194: 481–486, 1981.
527. Jeffery PL, McGuckin MA, Linden SK. Endocrine impact of Helicobacter pylori: focuson ghrelin and ghrelin o-acyltransferase. World J Gastroenterol 17: 1249–1260, 2011.
528. Jeon TY, Lee S, Kim HH, Kim YJ, Son HC, Kim DH, Sim MS. Changes in plasmaghrelin concentration immediately after gastrectomy in patients with early gastriccancer. J Clin Endocrinol Metab 89: 5392–5396, 2004.
529. Jiang Y, Minet E, Zhang Z, Silver PA, Bai M. Modulation of interprotomer relation-ships is important for activation of dimeric calcium-sensing receptor. J Biol Chem 279:14147–14156, 2004.
530. Jilka RL, O’Brien CA, Ali AA, Roberson PK, Weinstein RS, Manolagas SC. Intermit-tent PTH stimulates periosteal bone formation by actions on post-mitotic preosteo-blasts. Bone 44: 275–286, 2009.
531. Jilka RL, Weinstein RS, Bellido T, Roberson P, Parfitt AM, Manolagas SC. Increasedbone formation by prevention of osteoblast apoptosis with parathyroid hormone. JClin Invest 104: 439–446, 1999.
532. Jin HO, Lee KY, Chang TM, Chey WY, Dubois A. Secretin: a physiological regulatorof gastric emptying and acid output in dogs. Am J Physiol Gastrointest Liver Physiol 267:G702–G708, 1994.
533. Johnson JA, Grande JP, Roche PC, Kumar R. Ontogeny of the 1,25-dihydroxyvitaminD3 receptor in fetal rat bone. J Bone Miner Res 11: 56–61, 1996.
534. Johnson LR, Lichtenberger LM, Copeland EM, Dudrick SJ, Castro GA. Action ofgastrin on gastrointestinal structure and function. Gastroenterology 68: 1184–1192,1975.
535. Jones B, Jones EL, Bonney SA, Patel HN, Mensenkamp AR, Eichenbaum-Voline S,Rudling M, Myrdal U, Annesi G, Naik S, Meadows N, Quattrone A, Islam SA, Naou-mova RP, Angelin B, Infante R, Levy E, Roy CC, Freemont PS, Scott J, Shoulders CC.Mutations in a Sar1 GTPase of COPII vesicles are associated with lipid absorptiondisorders. Nat Genet 34: 29–31, 2003.
536. Juppner H, Abou-Samra AB, Freeman M, Kong XF, Schipani E, Richards J, Kola-kowski LF Jr, Hock J, Potts JT Jr, Kronenberg HM. A G protein-linked receptor forparathyroid hormone and parathyroid hormone-related peptide. Science 254:1024–1026, 1991.
537. Jurutka PW, Thompson PD, Whitfield GK, Eichhorst KR, Hall N, Dominguez CE,Hsieh JC, Haussler CA, Haussler MR. Molecular and functional comparison of 1,25-dihydroxyvitamin D3 and the novel vitamin D receptor ligand, lithocholic acid, inactivating transcription of cytochrome P450 3A4. J Cell Biochem 94: 917–943, 2005.
538. Juttmann JR, Visser TJ, Buurman C, de Kam E, Birkenhager JC. Seasonal fluctuationsin serum concentrations of vitamin D metabolites in normal subjects. Br Med J 282:1349–1352, 1981.
539. Kahrilas PJ, Dent J, Lauritsen K, Malfertheiner P, Denison H, Franzen S, HasselgrenG. A randomized, comparative study of three doses of AZD0865 and esomeprazolefor healing of reflux esophagitis. Clin Gastroenterol Hepatol 5: 1385–1391, 2007.
540. Kajikawa M, Ishida H, Fujimoto S, Mukai E, Nishimura M, Fujita J, Tsuura Y, OkamotoY, Norman AW, Seino Y. An insulinotropic effect of vitamin D analog with increasingintracellular Ca2� concentration in pancreatic beta-cells through nongenomic signaltransduction. Endocrinology 140: 4706–4712, 1999.
541. Kajimura M, Reuben MA, Sachs G. The muscarinic receptor gene expressed in rabbitparietal cells is the m3 subtype. Gastroenterology 103: 870–875, 1992.
542. Kameda T, Mano H, Yamada Y, Takai H, Amizuka N, Kobori M, Izumi N, KawashimaH, Ozawa H, Ikeda K, Kameda A, Hakeda Y, Kumegawa M. Calcium-sensing recep-tor in mature osteoclasts, which are bone resorbing cells. Biochem Biophys ResCommun 245: 419–422, 1998.
543. Kanai S, Hosoya H, Akimoto S, Ohta M, Matsui T, Takiguchi S, Funakoshi A, MiyasakaK. Gastric acid secretion in cholecystokinin-1 receptor, -2 receptor, and -1, -2receptor gene knockout mice. J Physiol Sci 59: 23–29, 2009.
544. Kanatani M, Sugimoto T, Kanzawa M, Yano S, Chihara K. High extracellular calciuminhibits osteoclast-like cell formation by directly acting on the calcium-sensing re-ceptor existing in osteoclast precursor cells. Biochem Biophys Res Commun 261:144–148, 1999.
545. Karam SM, Straiton T, Hassan WM, Leblond CP. Defining epithelial cell progenitorsin the human oxyntic mucosa. Stem Cells 21: 322–336, 2003.
546. Karaplis AC, Lim SK, Baba H, Arnold A, Kronenberg HM. Inefficient membranetargeting, translocation, and proteolytic processing by signal peptidase of a mutantpreproparathyroid hormone protein. J Biol Chem 270: 1629–1635, 1995.
547. Karp HJ, Ketola ME, Lamberg-Allardt CJ. Acute effects of calcium carbonate, calciumcitrate and potassium citrate on markers of calcium and bone metabolism in youngwomen. Br J Nutr 102: 1341–1347, 2009.
548. Karvar S, Yao X, Crothers JM Jr, Liu Y, Forte JG. Localization and function of solubleN-ethylmaleimide-sensitive factor attachment protein-25 and vesicle-associated
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
251Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

membrane protein-2 in functioning gastric parietal cells. J Biol Chem 277: 50030–50035, 2002.
549. Karvar S, Yao X, Duman JG, Hybiske K, Liu Y, Forte JG. Intracellular distribution andfunctional importance of vesicle-associated membrane protein 2 in gastric parietalcells. Gastroenterology 123: 281–290, 2002.
550. Karvar S, Zhu L, Crothers J Jr, Wong W, Turkoz M, Forte JG. Cellular localization andstimulation-associated distribution dynamics of syntaxin-1 and syntaxin-3 in gastricparietal cells. Traffic 6: 654–666, 2005.
551. Kato K, Hayashizaki Y, Takahashi Y, Himeno S, Matsubara K. Molecular cloning ofthe human gastrin gene. Nucleic Acids Res 11: 8197–8203, 1983.
552. Kato K, Himeno S, Takahashi Y, Wakabayashi T, Tarui S, Matsubara K. Molecularcloning of human gastrin precursor cDNA. Gene 26: 53–57, 1983.
553. Kato S, Abe Y, Konishi M, Kuroda N, Takeuchi K. Mechanism of gastric hyperemicresponse during acid secretion in rats: relation to nitric oxide, prostaglandins, sen-sory neurons. J Clin Gastroenterol 25 Suppl 1: S48–55, 1997.
554. Kato S, Aihara E, Yoshii K, Takeuchi K. Dual action of prostaglandin E2 on gastric acidsecretion through different EP-receptor subtypes in the rat. Am J Physiol GastrointestLiver Physiol 289: G64–G69, 2005.
555. Kato S, Kitamura M, Korolkiewicz RP, Takeuchi K. Role of nitric oxide in regulationof gastric acid secretion in rats: effects of NO donors and NO synthase inhibitor. BrJ Pharmacol 123: 839–846, 1998.
556. Kaufhold MA, Krabbenhoft A, Song P, Engelhardt R, Riederer B, Fahrmann M,Klocker N, Beil W, Manns M, Hagen SJ, Seidler U. Localization, trafficking, andsignificance for acid secretion of parietal cell Kir4.1 and KCNQ1 K� channels. Gas-troenterology 134: 1058–1069, 2008.
557. Kawakami M, Blum CB, Ramakrishnan R, Dell RB, Goodman DS. Turnover of theplasma binding protein for vitamin D and its metabolites in normal human subjects.J Clin Endocrinol Metab 53: 1110–1116, 1981.
558. Kawashima K, Ishihara S, Karim Rumi MA, Moriyama N, Kazumori H, Suetsugu H,Sato H, Fukuda R, Adachi K, Shibata M, Onodera S, Chiba T, Kinoshita Y. Localizationof calcitonin gene-related peptide receptors in rat gastric mucosa. Peptides 23: 955–966, 2002.
559. Kaye JA, Jick H. Proton pump inhibitor use and risk of hip fractures in patientswithout major risk factors. Pharmacotherapy 28: 951–959, 2008.
560. Kazumori H, Ishihara S, Kawashima K, Fukuda R, Chiba T, Kinoshita Y. Analysis ofgastrin receptor gene expression in proliferating cells in the neck zone of gastricfundic glands using laser capture microdissection. FEBS Lett 489: 208–214, 2001.
561. Keeley TM, Samuelson LC. Cytodifferentiation of the postnatal mouse stomach innormal and Huntingtin-interacting protein 1-related-deficient mice. Am J Physiol Gas-trointest Liver Physiol 299: G1241–G1251, 2010.
562. Keeton TP, Burk SE, Shull GE. Alternative splicing of exons encoding the calmodulin-binding domains and C termini of plasma membrane Ca2�-ATPase isoforms 1, 2, 3,and 4. J Biol Chem 268: 2740–2748, 1993.
563. Kehayoglou AK, Holdsworth CD, Agnew JE, Whelton MJ, Sherlock S. Bone diseaseand calcium absorption in primary biliary cirrhosis with special reference to vita-min-D therapy. Lancet 1: 715–718, 1968.
564. Keinke O, Ehrlein HJ, Wulschke S. Mechanical factors regulating gastric emptyingexamined by the effects of exogenous cholecystokinin and secretin on canine gas-troduodenal motility. Can J Physiol Pharmacol 65: 287–292, 1987.
565. Kemper B, Habener JF, Mulligan RC, Potts JT Jr, Rich A. Pre-proparathyroid hor-mone: a direct translation product of parathyroid messenger RNA. Proc Natl Acad SciUSA 71: 3731–3735, 1974.
566. Keusch I, Traebert M, Lotscher M, Kaissling B, Murer H, Biber J. Parathyroid hor-mone and dietary phosphate provoke a lysosomal routing of the proximal tubularNa/Pi-cotransporter type II. Kidney Int 54: 1224–1232, 1998.
567. Khan M, Santana J, Donnellan C, Preston C, Moayyedi P. Medical treatments in theshort term management of reflux oesophagitis. Cochrane Database Syst RevCD003244, 2007.
568. Khanal RC, Peters TM, Smith NM, Nemere I. Membrane receptor-initiated signalingin 1,25(OH)2D3-stimulated calcium uptake in intestinal epithelial cells. J Cell Biochem105: 1109–1116, 2008.
569. Kidd M, Hauso O, Drozdov I, Gustafsson BI, Modlin IM. Delineation of the chemo-mechanosensory regulation of gastrin secretion using pure rodent G cells. Gastroen-terology 137: 231–241, 2009.
570. Kidd M, Modlin IM, Black JW, Boyce M, Culler M. A comparison of the effects ofgastrin, somatostatin and dopamine receptor ligands on rat gastric enterochromaf-fin-like cell secretion and proliferation. Regul Pept 143: 109–117, 2007.
571. Kifor O, Diaz R, Butters R, Kifor I, Brown EM. The calcium-sensing receptor islocalized in caveolin-rich plasma membrane domains of bovine parathyroid cells. JBiol Chem 273: 21708–21713, 1998.
572. Kifor O, MacLeod RJ, Diaz R, Bai M, Yamaguchi T, Yao T, Kifor I, Brown EM.Regulation of MAP kinase by calcium-sensing receptor in bovine parathyroid andCaR-transfected HEK293 cells. Am J Physiol Renal Physiol 280: F291–F302, 2001.
573. Kikuchi K, Kikuchi T, Ghishan FK. Characterization of calcium transport by basolat-eral membrane vesicles of human small intestine. Am J Physiol Gastrointest LiverPhysiol 255: G482–G489, 1988.
574. Kim HJ, Yang DK, So I. PDZ domain-containing protein as a physiological modulatorof TRPV6. Biochem Biophys Res Commun 361: 433–438, 2007.
575. Kim MS, Fujiki R, Murayama A, Kitagawa H, Yamaoka K, Yamamoto Y, Mihara M,Takeyama K, Kato S. 1Alpha,25(OH)2D3-induced transrepression by vitamin D re-ceptor through E-box-type elements in the human parathyroid hormone gene pro-moter. Mol Endocrinol 21: 334–342, 2007.
576. Kim SW, Her SJ, Park SJ, Kim D, Park KS, Lee HK, Han BH, Kim MS, Shin CS, Kim SY.Ghrelin stimulates proliferation and differentiation and inhibits apoptosis in osteo-blastic MC3T3-E1 cells. Bone 37: 359–369, 2005.
577. Kirchhoff P, Andersson K, Socrates T, Sidani S, Kosiek O, Geibel JP. Characteristicsof the K�-competitive H�,K�-ATPase inhibitor AZD0865 in isolated rat gastricglands. Am J Physiol Gastrointest Liver Physiol 291: G838–G843, 2006.
578. Kirton CM, Wang T, Dockray GJ. Regulation of parietal cell migration by gastrin inthe mouse. Am J Physiol Gastrointest Liver Physiol 283: G787–G793, 2002.
579. Klenk C, Schulz S, Calebiro D, Lohse MJ. Agonist-regulated cleavage of the extra-cellular domain of parathyroid hormone receptor type 1. J Biol Chem 285: 8665–8674, 2010.
580. Klenk C, Vetter T, Zurn A, Vilardaga JP, Friedman PA, Wang B, Lohse MJ. Formationof a ternary complex among NHERF1, beta-arrestin, parathyroid hormone recep-tor. J Biol Chem 285: 30355–30362, 2010.
581. Klotz U. Pharmacokinetic considerations in the eradication of Helicobacter pylori.Clin Pharmacokinet 38: 243–270, 2000.
582. Klotz U, Schwab M, Treiber G. CYP2C19 polymorphism and proton pump inhibi-tors. Basic Clin Pharmacol Toxicol 95: 2–8, 2004.
583. Ko SH, Choi KC, Oh GT, Jeung EB. Effect of dietary calcium and 1,25-(OH)2D3 onthe expression of calcium transport genes in calbindin-D9k and -D28k double knock-out mice. Biochem Biophys Res Commun 379: 227–232, 2009.
584. Kobayashi T, Tonai S, Ishihara Y, Koga R, Okabe S, Watanabe T. Abnormal functionaland morphological regulation of the gastric mucosa in histamine H2 receptor-defi-cient mice. J Clin Invest 105: 1741–1749, 2000.
585. Kocian J, Brodan V. New observations on the absorption of 47Ca in patients withpartial gastrectomy. Digestion 12: 193–200, 1975.
586. Kodicek E, Lawson DE, Wilson PW. Biological activity of a polar metabolite ofvitamin D. Nature 228: 763–764, 1970.
587. Koh TJ, Field JK, Varro A, Liloglou T, Fielding P, Cui G, Houghton J, Dockray GJ,Wang TC. Glycine-extended gastrin promotes the growth of lung cancer. Cancer Res64: 196–201, 2004.
588. Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K. Ghrelin is agrowth-hormone-releasing acylated peptide from stomach. Nature 402: 656–660,1999.
SASCHA KOPIC AND JOHN P. GEIBEL
252 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

589. Komaba H, Nakanishi S, Fujimori A, Tanaka M, Shin J, Shibuya K, Nishioka M,Hasegawa H, Kurosawa T, Fukagawa M. Cinacalcet effectively reduces parathyroidhormone secretion and gland volume regardless of pretreatment gland size in pa-tients with secondary hyperparathyroidism. Clin J Am Soc Nephrol 5: 2305–2314,2010.
590. Komasaka M, Horie S, Watanabe K, Murayama T. Antisecretory effect of somatosta-tin on gastric acid via inhibition of histamine release in isolated mouse stomach. EurJ Pharmacol 452: 235–243, 2002.
591. Kong XF, Zhu XH, Pei YL, Jackson DM, Holick MF. Molecular cloning, character-ization, and promoter analysis of the human 25-hydroxyvitamin D3-1alpha-hydrox-ylase gene. Proc Natl Acad Sci USA 96: 6988–6993, 1999.
592. Kong YY, Yoshida H, Sarosi I, Tan HL, Timms E, Capparelli C, Morony S, Oliveira-dos-Santos AJ, Van G, Itie A, Khoo W, Wakeham A, Dunstan CR, Lacey DL, Mak TW,Boyle WJ, Penninger JM. OPGL is a key regulator of osteoclastogenesis, lymphocytedevelopment and lymph-node organogenesis. Nature 397: 315–323, 1999.
593. Konturek JW, Stoll R, Konturek SJ, Domschke W. Cholecystokinin in the control ofgastric acid secretion in man. Gut 34: 321–328, 1993.
594. Konturek SJ, Bilski J, Cieszkowski M. Role of cholecystokinin in the intestinal fat- andacid-induced inhibition of gastric secretion. Regul Pept 42: 97–109, 1992.
595. Konturek SJ, Kwiecien N, Obtulowicz W, Mikos E, Sito E, Oleksy J, Popiela T.Cephalic phase of gastric secretion in healthy subjects and duodenal ulcer patients:role of vagal innervation. Gut 20: 875–881, 1979.
596. Kopin AS, Lee YM, McBride EW, Miller LJ, Lu M, Lin HY, Kolakowski LF Jr, BeinbornM. Expression cloning and characterization of the canine parietal cell gastrin recep-tor. Proc Natl Acad Sci USA 89: 3605–3609, 1992.
597. Kopp R, Pfeiffer A. Effects of phorbol ester treatment on dibutyryl cyclic adeno-sine-5= monophosphate- and carbachol-stimulated aminopyrine accumulation in iso-lated rat parietal cells. Scand J Gastroenterol 35: 686–693, 2000.
598. Kos CH, Karaplis AC, Peng JB, Hediger MA, Goltzman D, Mohammad KS, Guise TA,Pollak MR. The calcium-sensing receptor is required for normal calcium homeostasisindependent of parathyroid hormone. J Clin Invest 111: 1021–1028, 2003.
599. Koshihara Y, Hoshi K, Ishibashi H, Shiraki M. Vitamin K2 promotes 1alpha,25(OH)2
vitamin D3-induced mineralization in human periosteal osteoblasts. Calcif Tissue Int59: 466–473, 1996.
600. Koushik SV, Wang J, Rogers R, Moskophidis D, Lambert NA, Creazzo TL, ConwaySJ. Targeted inactivation of the sodium-calcium exchanger (Ncx1) results in the lackof a heartbeat and abnormal myofibrillar organization. FASEB J 15: 1209–1211, 2001.
601. Kozoni V, Tsioulias G, Shiff S, Rigas B. The effect of lithocholic acid on proliferationand apoptosis during the early stages of colon carcinogenesis: differential effect onapoptosis in the presence of a colon carcinogen. Carcinogenesis 21: 999–1005, 2000.
602. Kretsinger RH, Mann JE, Simmonds JG. Model of facilitated diffusion of calcium bythe intestinal calcium-binding protein. In: Proceedings of the Fifth Workshop on VitaminD, edited by Norman AW, Schaefer K, Herrath DV, Grigoleit HG. Berlin: Debruyter,1982, p. 232–248.
603. Kreutz M, Andreesen R, Krause SW, Szabo A, Ritz E, Reichel H. 1,25-Dihydroxyvi-tamin D3 production and vitamin D3 receptor expression are developmentally reg-ulated during differentiation of human monocytes into macrophages. Blood 82:1300–1307, 1993.
604. Krisinger J, Strom M, Darwish HD, Perlman K, Smith C, DeLuca HF. Induction ofcalbindin-D 9k mRNA but not calcium transport in rat intestine by 1,25-dihydroxyvi-tamin D3 24-homologs. J Biol Chem 266: 1910–1913, 1991.
605. Kubler N, Krause U, Wagner PK, Beyer J, Rothmund M. The secretion of parathyroidhormone and its fragments from dispersed cells of adenomatous parathyroid tissueat different calcium concentrations. Exp Clin Endocrinol 88: 101–108, 1986.
606. Kuestner RE, Elrod RD, Grant FJ, Hagen FS, Kuijper JL, Matthewes SL, O’Hara PJ,Sheppard PO, Stroop SD, Thompson DL. Cloning and characterization of an abun-dant subtype of the human calcitonin receptor. Mol Pharmacol 46: 246–255, 1994.
607. Kuhn B, Schmid A, Harteneck C, Gudermann T, Schultz G. G proteins of the Gqfamily couple the H2 histamine receptor to phospholipase C. Mol Endocrinol 10:1697–1707, 1996.
608. Kulaksiz H, Arnold R, Goke B, Maronde E, Meyer M, Fahrenholz F, Forssmann WG,Eissele R. Expression and cell-specific localization of the cholecystokinin B/gastrinreceptor in the human stomach. Cell Tissue Res 299: 289–298, 2000.
609. Kumar R, Cohen WR, Silva P, Epstein FH. Elevated 1,25-dihydroxyvitamin D plasmalevels in normal human pregnancy and lactation. J Clin Invest 63: 342–344, 1979.
610. Kumar R, Schaefer J, Grande JP, Roche PC. Immunolocalization of calcitriol receptor,24-hydroxylase cytochrome P-450, and calbindin D28k in human kidney. Am J PhysiolRenal Fluid Electrolyte Physiol 266: F477–F485, 1994.
611. Kunishima N, Shimada Y, Tsuji Y, Sato T, Yamamoto M, Kumasaka T, Nakanishi S,Jingami H, Morikawa K. Structural basis of glutamate recognition by a dimericmetabotropic glutamate receptor. Nature 407: 971–977, 2000.
612. Kuro-o M, Matsumura Y, Aizawa H, Kawaguchi H, Suga T, Utsugi T, Ohyama Y,Kurabayashi M, Kaname T, Kume E, Iwasaki H, Iida A, Shiraki-Iida T, Nishikawa S,Nagai R, Nabeshima YI. Mutation of the mouse klotho gene leads to a syndromeresembling ageing. Nature 390: 45–51, 1997.
613. Kutuzova GD, Akhter S, Christakos S, Vanhooke J, Kimmel-Jehan C, DeLuca HF.Calbindin D9k knockout mice are indistinguishable from wild-type mice in pheno-type and serum calcium level. Proc Natl Acad Sci USA 103: 12377–12381, 2006.
614. Kutuzova GD, Deluca HF. Gene expression profiles in rat intestine identify pathwaysfor 1,25-dihydroxyvitamin D3 stimulated calcium absorption and clarify its immuno-modulatory properties. Arch Biochem Biophys 432: 152–166, 2004.
615. Kutuzova GD, Sundersingh F, Vaughan J, Tadi BP, Ansay SE, Christakos S, DelucaHF. TRPV6 is not required for 1alpha,25-dihydroxyvitamin D3-induced intestinalcalcium absorption in vivo. Proc Natl Acad Sci USA 105: 19655–19659, 2008.
616. Kwok CS, Yeong JK, Loke YK. Meta-analysis: risk of fractures with acid-suppressingmedication. Bone 48: 768–776, 2011.
617. Labuda M, Labuda D, Korab-Laskowska M, Cole DE, Zietkiewicz E, Weissenbach J,Popowska E, Pronicka E, Root AW, Glorieux FH. Linkage disequilibrium analysis inyoung populations: pseudo-vitamin D-deficiency rickets and the founder effect inFrench Canadians. Am J Hum Genet 59: 633–643, 1996.
618. Labuda M, Morgan K, Glorieux FH. Mapping autosomal recessive vitamin D depen-dency type I to chromosome 12q14 by linkage analysis. Am J Hum Genet 47: 28–36,1990.
619. Lambers TT, Weidema AF, Nilius B, Hoenderop JG, Bindels RJ. Regulation of themouse epithelial Ca2� channel TRPV6 by the Ca2�-sensor calmodulin. J Biol Chem279: 28855–28861, 2004.
620. Lamberts R, Stumps D, Plumpe L, Creutzfeldt W. Somatostatin cells in rat antralmucosa: qualitative and quantitative ultrastructural analyses in different states ofgastric acid secretion. Histochemistry 95: 373–382, 1991.
621. Lane NE, Sanchez S, Modin GW, Genant HK, Pierini E, Arnaud CD. Parathyroidhormone treatment can reverse corticosteroid-induced osteoporosis. Results of arandomized controlled clinical trial. J Clin Invest 102: 1627–1633, 1998.
622. Langhans N, Rindi G, Chiu M, Rehfeld JF, Ardman B, Beinborn M, Kopin AS. Abnor-mal gastric histology and decreased acid production in cholecystokinin-B/gastrinreceptor-deficient mice. Gastroenterology 112: 280–286, 1997.
623. Langub MC, Reinhardt TA, Horst RL, Malluche HH, Koszewski NJ. Characterizationof vitamin D receptor immunoreactivity in human bone cells. Bone 27: 383–387,2000.
624. Lapierre LA, Avant KM, Caldwell CM, Ham AJ, Hill S, Williams JA, Smolka AJ,Goldenring JR. Characterization of immunoisolated human gastric parietal cells tu-bulovesicles: identification of regulators of apical recycling. Am J Physiol GastrointestLiver Physiol 292: G1249–G1262, 2007.
625. Lark RK, Lester GE, Ontjes DA, Blackwood AD, Hollis BW, Hensler MM, Aris RM.Diminished and erratic absorption of ergocalciferol in adult cystic fibrosis patients.Am J Clin Nutr 73: 602–606, 2001.
626. Larsen EH, Nedergaard S, Ussing HH. Role of lateral intercellular space and sodiumrecirculation for isotonic transport in leaky epithelia. Rev Physiol Biochem Pharmacol141: 153–212, 2000.
627. Larsen FL, Katz S, Roufogalis BD. Calmodulin regulation of Ca2� transport in humanerythrocytes. Biochem J 200: 185–191, 1981.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
253Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

628. Larsen FL, Vincenzi FF. Calcium transport across the plasma membrane: stimulationby calmodulin. Science 204: 306–309, 1979.
629. Larsson B, Gritli-Linde A, Norlen P, Lindstrom E, Hakanson R, Linde A. Extracts ofECL-cell granules/vesicles and of isolated ECL cells from rat oxyntic mucosa evoke aCa2� second messenger response in osteoblastic cells. Regul Pept 97: 153–161,2001.
630. Larsson B, Norlen P, Lindstrom E, Zhao D, Hakanson R, Linde A. Effects of ECL cellextracts and granule/vesicle-enriched fractions from rat oxyntic mucosa on cAMPand IP3 in rat osteoblast-like cells. Regul Pept 106: 13–18, 2002.
631. Larsson H, Carlsson E, Ryberg B, Fryklund J, Wallmark B. Rat parietal cell functionafter prolonged inhibition of gastric acid secretion. Am J Physiol Gastrointest LiverPhysiol 254: G33–G39, 1988.
632. Larsson LI, Goltermann N, de Magistris L, Rehfeld JF, Schwartz TW. Somatostatincell processes as pathways for paracrine secretion. Science 205: 1393–1395, 1979.
633. Lawson DE, Fraser DR, Kodicek E, Morris HR, Williams DH. Identification of 1,25-dihydroxycholecalciferol, a new kidney hormone controlling calcium metabolism.Nature 230: 228–230, 1971.
634. Lawson DE, Wilson PW, Kodicek E. New vitamin D metabolite localized in intestinalcell nuclei. Nature 222: 171–172, 1969.
635. Lawton DE, Simcock DC, Candy EJ, Simpson HV. Gastrin secretion by ovine antralmucosa in vitro. Comp Biochem Physiol A Mol Integr Physiol 126: 233–243, 2000.
636. Lawton GP, Tang LH, Miu K, Gilligan CJ, Absood A, Modlin IM. Adrenergic andcromolyn sodium modulation of ECL cell histamine secretion. J Surg Res 58: 96–104,1995.
637. Le Moullec JM, Jullienne A, Chenais J, Lasmoles F, Guliana JM, Milhaud G, MoukhtarMS. The complete sequence of human preprocalcitonin. FEBS Lett 167: 93–97, 1984.
638. Leclerc R, Pelletier G, Puviani R, Arimura A, Schally AV. Immunohistochemical lo-calization of somatostatin in endocrine cells of the rat stomach. Mol Cell Endocrinol 4:257–261, 1976.
639. Lee GS, Lee KY, Choi KC, Ryu YH, Paik SG, Oh GT, Jeung EB. Phenotype of acalbindin-D9k gene knockout is compensated for by the induction of other calciumtransporter genes in a mouse model. J Bone Miner Res 22: 1968–1978, 2007.
640. Lee JW, Fuda H, Javitt NB, Strott CA, Rodriguez IR. Expression and localization ofsterol 27-hydroxylase (CYP27A1) in monkey retina. Exp Eye Res 83: 465–469, 2006.
641. Lee MP, Ravenel JD, Hu RJ, Lustig LR, Tomaselli G, Berger RD, Brandenburg SA, LitziTJ, Bunton TE, Limb C, Francis H, Gorelikow M, Gu H, Washington K, Argani P,Goldenring JR, Coffey RJ, Feinberg AP. Targeted disruption of the Kvlqt1 genecauses deafness and gastric hyperplasia in mice. J Clin Invest 106: 1447–1455, 2000.
642. Lefkowitz ES, Garland CF. Sunlight, vitamin D, and ovarian cancer mortality rates inUS women. Int J Epidemiol 23: 1133–1136, 1994.
643. Leheste JR, Melsen F, Wellner M, Jansen P, Schlichting U, Renner-Muller I, Andre-assen TT, Wolf E, Bachmann S, Nykjaer A, Willnow TE. Hypocalcemia and osteop-athy in mice with kidney-specific megalin gene defect. FASEB J 17: 247–249, 2003.
644. Lehto-Axtelius D, Chen D, Surve VV, Hakanson R. Post-gastrectomy osteopenia inthe rat: bone structure is preserved by retaining 10%-30% of the oxyntic gland area.Scand J Gastroenterol 37: 437–443, 2002.
645. Leichtmann GA, Bengoa JM, Bolt MJ, Sitrin MD. Intestinal absorption of cholecalcif-erol and 25-hydroxycholecalciferol in patients with both Crohn’s disease and intes-tinal resection. Am J Clin Nutr 54: 548–552, 1991.
646. Leitersdorf E, Reshef A, Meiner V, Levitzki R, Schwartz SP, Dann EJ, Berkman N, CaliJJ, Klapholz L, Berginer VM. Frameshift and splice-junction mutations in the sterol27-hydroxylase gene cause cerebrotendinous xanthomatosis in Jews or Moroccanorigin. J Clin Invest 91: 2488–2496, 1993.
647. Lemay J, Demers C, Hendy GN, Gascon-Barré M. Oral calcium transiently increasescalbindin(9k) gene expression in adult rat duodena. Calcified Tissue Int 60: 43–47,1997.
648. Lepage R, Roy L, Brossard JH, Rousseau L, Dorais C, Lazure C, D’Amour P. Anon-(1–84) circulating parathyroid hormone (PTH) fragment interferes significantlywith intact PTH commercial assay measurements in uremic samples. Clin Chem 44:805–809, 1998.
649. Lepard KJ, Chi J, Mohammed JR, Gidener S, Stephens RL Jr. Gastric antisecretoryeffect of serotonin: quantitation of release and site of action. Am J Physiol EndocrinolMetab 271: E669–E677, 1996.
650. LePard KJ, Stephens RL Jr. Serotonin inhibits gastric acid secretion through a 5-hy-droxytryptamine1-like receptor in the rat. J Pharmacol Exp Ther 270: 1139–1144,1994.
651. Leth RD, Abrahamsson H, Kilander A, Lundell LR. Malabsorption of fat after partialgastric resection. A study of pathophysiologic mechanisms. Eur J Surg 157: 205–208,1991.
652. Levant JA, Walsh JH, Isenberg JI. Stimulation of gastric secretion and gastrin releaseby single oral doses of calcium carbonate in man. N Engl J Med 289: 555–558, 1973.
653. Levi R, Ben-Dov IZ, Lavi-Moshayoff V, Dinur M, Martin D, Naveh-Many T, Silver J.Increased parathyroid hormone gene expression in secondary hyperparathyroidismof experimental uremia is reversed by calcimimetics: correlation with posttransla-tional modification of the trans acting factor AUF1. J Am Soc Nephrol 17: 107–112,2006.
654. Levin F, Edholm T, Ehrstrom M, Wallin B, Schmidt PT, Kirchgessner AM, Hilsted LM,Hellstrom PM, Naslund E. Effect of peripherally administered ghrelin on gastricemptying and acid secretion in the rat. Regul Pept 131: 59–65, 2005.
655. Lewis JJ, Zdon MJ, Adrian TE, Modlin IM. Pancreastatin: a novel peptide inhibitor ofparietal cell secretion. Surgery 104: 1031–1036, 1988.
656. Li P, Chang TM, Chey WY. Secretin inhibits gastric acid secretion via a vagal afferentpathway in rats. Am J Physiol Gastrointest Liver Physiol 275: G22–G28, 1998.
657. Li P, Chang TM, Coy D, Chey WY. Inhibition of gastric acid secretion in rat stomachby PACAP is mediated by secretin, somatostatin, and PGE2. Am J Physiol GastrointestLiver Physiol 278: G121–G127, 2000.
658. Li XF, Kraev AS, Lytton J. Molecular cloning of a fourth member of the potassium-dependent sodium-calcium exchanger gene family, NCKX4. J Biol Chem 277:48410–48417, 2002.
659. Li Y, Wu X, Yao H, Owyang C. Secretin activates vagal primary afferent neurons inthe rat: evidence from electrophysiological and immunohistochemical studies. Am JPhysiol Gastrointest Liver Physiol 289: G745–G752, 2005.
660. Li YC. Vitamin D regulation of the renin-angiotensin system. J Cell Biochem 88:327–331, 2003.
661. Li YC, Amling M, Pirro AE, Priemel M, Meuse J, Baron R, Delling G, Demay MB.Normalization of mineral ion homeostasis by dietary means prevents hyperparathy-roidism, rickets, osteomalacia, but not alopecia in vitamin D receptor-ablated mice.Endocrinology 139: 4391–4396, 1998.
662. Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25-Dihydroxyvitamin D3 is anegative endocrine regulator of the renin-angiotensin system. J Clin Invest 110: 229–238, 2002.
663. Li YC, Pirro AE, Demay MB. Analysis of vitamin D-dependent calcium-binding pro-tein messenger ribonucleic acid expression in mice lacking the vitamin D receptor.Endocrinology 139: 847–851, 1998.
664. Li YY. Mechanisms for regulation of gastrin and somatostatin release from isolatedrat stomach during gastric distention. World J Gastroenterol 9: 129–133, 2003.
665. Lian J, Stewart C, Puchacz E, Mackowiak S, Shalhoub V, Collart D, Zambetti G, SteinG. Structure of the rat osteocalcin gene and regulation of vitamin D-dependentexpression. Proc Natl Acad Sci USA 86: 1143–1147, 1989.
666. Lieben L, Benn BS, Ajibade D, Stockmans I, Moermans K, Hediger MA, Peng JB,Christakos S, Bouillon R, Carmeliet G. Trpv6 mediates intestinal calcium absorptionduring calcium restriction and contributes to bone homeostasis. Bone 47: 301–308,2010.
667. Liedman B, Bosaeus I, Mellstrom D, Lundell L. Osteoporosis after total gastrectomy.Results of a prospective, clinical study. Scand J Gastroenterol 32: 1090–1095, 1997.
668. Liedman B, Henningsson A, Mellstrom D, Lundell L. Changes in bone metabolismand body composition after total gastrectomy: results of a longitudinal study. Dig DisSci 45: 819–824, 2000.
SASCHA KOPIC AND JOHN P. GEIBEL
254 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

669. Lin HY, Harris TL, Flannery MS, Aruffo A, Kaji EH, Gorn A, Kolakowski LF Jr, LodishHF, Goldring SR. Expression cloning of an adenylate cyclase-coupled calcitonin re-ceptor. Science 254: 1022–1024, 1991.
670. Lindberg P, Nordberg P, Alminger T, Brandstrom A, Wallmark B. The mechanism ofaction of the gastric acid secretion inhibitor omeprazole. J Med Chem 29: 1327–1329,1986.
671. Lindsay R, Nieves J, Formica C, Henneman E, Woelfert L, Shen V, Dempster D,Cosman F. Randomised controlled study of effect of parathyroid hormone on ver-tebral-bone mass and fracture incidence among postmenopausal women on oestro-gen with osteoporosis. Lancet 350: 550–555, 1997.
672. Lindstrom E, Bjorkqvist M, Boketoft A, Chen D, Zhao CM, Kimura K, Hakanson R.Neurohormonal regulation of histamine and pancreastatin secretion from isolatedrat stomach ECL cells. Regul Pept 71: 73–86, 1997.
673. Lindstrom E, Eliasson L, Bjorkqvist M, Hakanson R. Gastrin and the neuropeptidePACAP evoke secretion from rat stomach histamine-containing (ECL) cells by stim-ulating influx of Ca2� through different Ca2� channels. J Physiol 535: 663–677, 2001.
674. Lindstrom E, Hakanson R. Neurohormonal regulation of secretion from isolated ratstomach ECL cells: a critical reappraisal. Regul Pept 97: 169–180, 2001.
675. Lipecka J, Bali M, Thomas A, Fanen P, Edelman A, Fritsch J. Distribution of ClC-2chloride channel in rat and human epithelial tissues. Am J Physiol Cell Physiol 82:C805–C816, 2002.
676. Liu C, Chen J, Guo Y, Yang L, Zhao C, Bai L. The expression of PTHLH in humangastric mucosa enterochromaffin-like cells. Dig Dis Sci 56: 993–998, 2011.
677. Lloyd KC, Amirmoazzami S, Friedik F, Heynio A, Solomon TE, Walsh JH. Candidatecanine enterogastrones: acid inhibition before and after vagotomy. Am J PhysiolGastrointest Liver Physiol 272: G1236–G1242, 1997.
678. Lo CW, Paris PW, Clemens TL, Nolan J, Holick MF. Vitamin D absorption in healthysubjects and in patients with intestinal malabsorption syndromes. Am J Clin Nutr 42:644–649, 1985.
679. Locklin RM, Khosla S, Turner RT, Riggs BL. Mediators of the biphasic responses ofbone to intermittent and continuously administered parathyroid hormone. J CellBiochem 89: 180–190, 2003.
680. Loffing J, Loffing-Cueni D, Valderrabano V, Klausli L, Hebert SC, Rossier BC, Hoen-derop JG, Bindels RJ, Kaissling B. Distribution of transcellular calcium and sodiumtransport pathways along mouse distal nephron. Am J Physiol Renal Physiol 281:F1021–F1027, 2001.
681. Lorenz S, Frenzel R, Paschke R, Breitwieser GE, Miedlich SU. Functional desensiti-zation of the extracellular calcium-sensing receptor is regulated via distinct mecha-nisms: role of G protein-coupled receptor kinases, protein kinase C and beta-arres-tins. Endocrinology 148: 2398–2404, 2007.
682. Lotscher M, Scarpetta Y, Levi M, Halaihel N, Wang H, Zajicek HK, Biber J, Murer H,Kaissling B. Rapid downregulation of rat renal Na/Pi cotransporter in response toparathyroid hormone involves microtubule rearrangement. J Clin Invest 104: 483–494, 1999.
683. Lu P, Boros S, Chang Q, Bindels RJ, Hoenderop JG. The �-glucuronidase klothoexclusively activates the epithelial Ca2� channels TRPV5 and TRPV6. Nephrol Dial-ysis Transplantation 23: 3397–3402, 2008.
684. Luiz de Freitas PH, Li M, Ninomiya T, Nakamura M, Ubaidus S, Oda K, Udagawa N,Maeda T, Takagi R, Amizuka N. Intermittent PTH administration stimulates pre-osteoblastic proliferation without leading to enhanced bone formation in osteoclast-less c-fos(�/�) mice. J Bone Miner Res 24: 1586–1597, 2009.
685. Lund B, Selnes A. Plasma 1,25-dihydroxyvitamin D levels in pregnancy and lactation.Acta Endocrinol 92: 330–335, 1979.
686. Lund J, DeLuca HF. Biologically active metabolite of vitamin D3 from bone, liver, andblood serum. J Lipid Res 7: 739–744, 1966.
687. Lytton J. Na�/Ca2� exchangers: three mammalian gene families control Ca2� trans-port. Biochem J 406: 365–382, 2007.
688. Lytton J, Li XF, Dong H, Kraev A. K�-dependent Na�/Ca2� exchangers in the brain.Ann NY Acad Sci 976: 382–393, 2002.
689. Ma YL, Cain RL, Halladay DL, Yang X, Zeng Q, Miles RR, Chandrasekhar S, MartinTJ, Onyia JE. Catabolic effects of continuous human PTH (1–38) in vivo is associatedwith sustained stimulation of RANKL and inhibition of osteoprotegerin and gene-associated bone formation. Endocrinology 142: 4047–4054, 2001.
690. MacCallum WG, Voegtlin C. On the regulation of the parathyroid to calcium metab-olism and the nature of tetany. Bull Johns Hopkins Hosp 19: 91, 1908.
691. Maccarinelli G, Sibilia V, Torsello A, Raimondo F, Pitto M, Giustina A, Netti C, CocchiD. Ghrelin regulates proliferation and differentiation of osteoblastic cells. J Endocrinol184: 249–256, 2005.
692. Mace OJ, Morgan EL, Affleck JA, Lister N, Kellett GL. Calcium absorption by Cav1.3induces terminal web myosin II phosphorylation and apical GLUT2 insertion in ratintestine. J Physiol 580: 605–616, 2007.
693. MacGregor RR, Cohn DV, Hamilton JW. The content of carboxyl-terminal frag-ments of parathormone in extracts of fresh bovine parathyroids. Endocrinology 112:1019–1025, 1983.
694. Madaus S, Bender H, Schusdziarra V, Kehe K, Munzert G, Weber G, Classen M.Vagally induced release of gastrin, somatostatin and bombesin-like immunoreactivityfrom perfused rat stomach. Effect of stimulation frequency and cholinergic mecha-nisms. Regul Pept 30: 179–192, 1990.
695. Madaus S, Schusdziarra V, Seufferlein T, Classen M. Effect of galanin on gastrin andsomatostatin release from the rat stomach. Life Sci 42: 2381–2387, 1988.
696. Madhok TC, DeLuca HF. Characteristics of the rat liver microsomal enzyme systemconverting cholecalciferol into 25-hydroxycholecalciferol. Evidence for the partici-pation of cytochrome p-450. Biochem J 184: 491–499, 1979.
697. Maeda M, Oshiman K, Tamura S, Futai M. Human gastric-ATPase gene. Similarity to(Na� � K�)-ATPase genes in exon/intron organization but difference in controlregion. J Biol Chem 265: 9027–9032, 1990.
698. Mahon MJ, Donowitz M, Yun CC, Segre GV. Na�/H� exchanger regulatory factor 2directs parathyroid hormone 1 receptor signalling. Nature 417: 858–861, 2002.
699. Mahoney AW, Holbrook RS, Hendricks DG. Effects of calcium solubility on adsorp-tion by rats with induced achlorhydria. Nutr Metab 18: 310–317, 1975.
700. Maier GW, Kreis ME, Zittel TT, Becker HD. Calcium regulation and bone mass lossafter total gastrectomy in pigs. Ann Surg 225: 181–192, 1997.
701. Maislos M, Silver J, Fainaru M. Intestinal absorption of vitamin D sterols: differentialabsorption into lymph and portal blood in the rat. Gastroenterology 80: 1528–1534,1981.
702. Maiti A, Beckman MJ. Extracellular calcium is a direct effecter of VDR levels inproximal tubule epithelial cells that counter-balances effects of PTH on renal VitaminD metabolism. J Steroid Biochem Mol Biol 103: 504–508, 2007.
703. Makin G, Lohnes D, Byford V, Ray R, Jones G. Target cell metabolism of 1,25-dihydroxyvitamin D3 to calcitroic acid. Evidence for a pathway in kidney and boneinvolving 24-oxidation. Biochem J 262: 173–180, 1989.
704. Makishima M, Lu TT, Xie W, Whitfield GK, Domoto H, Evans RM, Haussler MR,Mangelsdorf DJ. Vitamin D receptor as an intestinal bile acid sensor. Science 296:1313–1316, 2002.
705. Malinowska DH. Cl� channel blockers inhibit acid secretion in rabbit parietal cells.Am J Physiol Cell Physiol 259: C536–C543, 1990.
706. Malinowska DH, Kupert EY, Bahinski A, Sherry AM, Cuppoletti J. Cloning, functionalexpression, and characterization of a PKA-activated gastric Cl� channel. Am J PhysiolCell Physiol 268: C191–C200, 1995.
707. Malinowska DH, Sherry AM, Tewari KP, Cuppoletti J. Gastric parietal cell secretorymembrane contains PKA- and acid-activated Kir2.1 K� channels. Am J Physiol CellPhysiol Cell Physiol 286: C495–C506, 2004.
708. Manela FD, Ren J, Gao J, McGuigan JE, Harty RF. Calcitonin gene-related peptidemodulates acid-mediated regulation of somatostatin and gastrin release from ratantrum. Gastroenterology 109: 701–706, 1995.
709. Manolagas SC, Burton DW, Deftos LJ. 1,25-Dihydroxyvitamin D3 stimulates thealkaline phosphatase activity of osteoblast-like cells. J Biol Chem 256: 7115–7117,1981.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
255Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

710. Marcus CS, Lengemann FW. Absorption of Ca45 and Sr85 from solid and liquid foodat various levels of the alimentary tract of the rat. J Nutr 77: 155–160, 1962.
711. Marie PJ. The calcium-sensing receptor in bone cells: a potential therapeutic target inosteoporosis. Bone 46: 571–576, 2010.
712. Marks HD, Fleet JC, Peleg S. Transgenic expression of the human Vitamin D recep-tor (hVDR) in the duodenum of VDR-null mice attenuates the age-dependent declinein calcium absorption. J Steroid Biochem Mol Biol 103: 513–516, 2007.
713. Martin DL, DeLuca HF. Influence of sodium on calcium transport by the rat smallintestine. Am J Physiol 216: 1351–1359, 1969.
714. Martin SR, Linse S, Johansson C, Bayley PM, Forsen S. Protein surface charges andCa2� binding to individual sites in calbindin D9k: stopped-flow studies. Biochemistry29: 4188–4193, 1990.
715. Martinez V, Curi AP, Torkian B, Schaeffer JM, Wilkinson HA, Walsh JH, Tache Y.High basal gastric acid secretion in somatostatin receptor subtype 2 knockout mice.Gastroenterology 114: 1125–1132, 1998.
716. Martz A, Forte LR, Langeluttig SG. Renal cAMP and 1,25(OH)2D3 synthesis in es-trogen-treated chick embryos and hens. Am J Physiol Endocrinol Metab 249: E626–E633, 1985.
717. Massheimer V, Boland R, de Boland AR. Rapid 1,25(OH)2-vitamin D3 stimulation ofcalcium uptake by rat intestinal cells involves a dihydropyridine-sensitive cAMP-dependent pathway. Cell Signal 6: 299–304, 1994.
718. Massry SG, Coburn JW, Chapman LW, Kleeman CR. Role of serum Ca, parathyroidhormone, NaCl infusion on renal Ca and Na clearances. Am J Physiol 214: 1403–1409, 1968.
719. Masuda Y, Tanaka T, Inomata N, Ohnuma N, Tanaka S, Itoh Z, Hosoda H, Kojima M,Kangawa K. Ghrelin stimulates gastric acid secretion and motility in rats. BiochemBiophys Res Commun 276: 905–908, 2000.
720. Mate L, Sakamoto T, Greeley GH Jr, Thompson JC. Regulation of gastric acid secre-tion by secretin and serotonin. Am J Surg 149: 40–45, 1985.
721. Matloff DS, Kaplan MM, Neer RM, Goldberg MJ, Bitman W, Wolfe HJ. Osteoporosisin primary biliary cirrhosis: effects of 25-hydroxyvitamin D3 treatment. Gastroenter-ology 83: 97–102, 1982.
722. Matsumoto M, Park J, Sugano K, Yamada T. Biological activity of progastrin post-translational processing intermediates. Am J Physiol Gastrointest Liver Physiol 252:G315–G319, 1987.
723. Matsuoka LY, Ide L, Wortsman J, MacLaughlin JA, Holick MF. Sunscreens suppresscutaneous vitamin D3 synthesis. J Clin Endocrinol Metab 64: 1165–1168, 1987.
724. Mawer EB, Taylor CM, Backhouse J, Lumb GA, Stanbury SW. Failure of formation of1,25-dihydroxycholecalciferol in chronic renal insufficiency. Lancet 1: 626–628,1973.
725. Mayer G, Arnold R, Feurle G, Fuchs K, Ketterer H, Track NS, Creutzfeldt W.Influence of feeding and sham feeding upon serum gastrin and gastric acid secretionin control subjects and duodenal ulcer patients. Scand J Gastroenterol 9: 703–710,1974.
726. Mayer GP, Keaton JA, Hurst JG, Habener JF. Effects of plasma calcium concentrationon the relative proportion of hormone and carboxyl fragments in parathyroid venousblood. Endocrinology 104: 1778–1784, 1979.
727. McCollum EV, Simmonds N, Becker JE, Shipley PG. Studies on experimental rickets.XXI. An experimental demonstration of the existence of a vitamin which promotescalcium deposition. J Biol Chem 53: 293–312, 1922.
728. McGehee DS, Aldersberg M, Liu KP, Hsuing S, Heath MJ, Tamir H. Mechanism ofextracellular Ca2� receptor-stimulated hormone release from sheep thyroid para-follicular cells. J Physiol 502: 31–44, 1997.
729. McLaughlin JT, Ai W, Sinclair NF, Colucci R, Raychowdhury R, Koh TJ, Wang TC.PACAP and gastrin regulate the histidine decarboxylase promoter via distinct mech-anisms. Am J Physiol Gastrointest Liver Physiol 286: G51–G59, 2004.
730. Mee AP, Hoyland JA, Braidman IP, Freemont AJ, Davies M, Mawer EB. Demonstra-tion of vitamin D receptor transcripts in actively resorbing osteoclasts in bone sec-tions. Bone 18: 295–299, 1996.
731. Melander T, Hokfelt T, Rokaeus A, Fahrenkrug J, Tatemoto K, Mutt V. Distributionof galanin-like immunoreactivity in the gastro-intestinal tract of several mammalianspecies. Cell Tissue Res 239: 253–270, 1985.
732. Melick RA, Benson JA Jr. Osteomalacia following partial gastrectomy. N Engl J Med260: 976–978, 1959.
733. Mellanby E. An experimental investigation on rickets. Lancet 193: 407–412, 1919.
734. Mentaverri R, Yano S, Chattopadhyay N, Petit L, Kifor O, Kamel S, Terwilliger EF,Brazier M, Brown EM. The calcium sensing receptor is directly involved in bothosteoclast differentiation and apoptosis. FASEB J 20: 2562–2564, 2006.
735. Meredith SC, Bolt MJ, Rosenberg IH. The supramolecular structure of vitamin D3 inwater. J Colloid Interface Sci 99: 244–255, 1984.
736. Meyer MB, Watanuki M, Kim S, Shevde NK, Pike JW. The human transient receptorpotential vanilloid type 6 distal promoter contains multiple vitamin D receptor bind-ing sites that mediate activation by 1,25-dihydroxyvitamin D3 in intestinal cells. MolEndocrinol 20: 1447–1461, 2006.
737. Miampamba M, Germano PM, Arli S, Wong HH, Scott D, Tache Y, Pisegna JR.Expression of pituitary adenylate cyclase-activating polypeptide and PACAP type 1receptor in the rat gastric and colonic myenteric neurons. Regul Pept 105: 145–154,2002.
738. Michelangeli F, Ruiz MC, Fernandez E, Ciarrocchi A. Role of Ca2� in H� transport byrabbit gastric glands studied with A23187 and BAPTA, an incorporated Ca2� chela-tor. Biochim Biophys Acta 983: 82–90, 1989.
739. Millen AE, Dodd KW, Subar AF. Use of vitamin, mineral, nonvitamin, and nonmineralsupplements in the United States: The 1987, 1992, and 2000 National Health Inter-view Survey results. J Am Diet Assoc 104: 942–950, 2004.
740. Miller A 3rd, Bronner F. Calcium uptake in isolated brush-border vesicles from ratsmall intestine. Biochem J 196: 391–401, 1981.
741. Milne ML, Baran DT. End product inhibition of hepatic 25-hydroxyvitamin D pro-duction in the rat: specificity and kinetics. Arch Biochem Biophys 242: 488–492, 1985.
742. Mircheff AK, Wright EM. Analytical isolation of plasma membranes of intestinalepithelial cells: identification of Na, K-ATPase rich membranes and the distributionof enzyme activities. J Membr Biol 28: 309–333, 1976.
743. Mitchell HH, Hamiltom TS, Steggerda FR, Bean HW. The chemical composition ofthe adult human body and its bearing on the biochemistry of growth. J Biol Chem 158:625–637, 1945.
744. Mitsuma T, Rhue N, Kayama M, Mori Y, Adachi K, Yokoi Y, Ping J, Nogimori T,Hirooka Y. Distribution of calcium sensing receptor in rats: an immunohistochemicalstudy. Endocr Regul 33: 55–59, 1999.
745. Miyake N, Hoshi K, Sano Y, Kikuchi K, Tadano K, Koshihara Y. 1,25-Dihydroxyvita-min D3 promotes vitamin K2 metabolism in human osteoblasts. Osteoporos Int 12:680–687, 2001.
746. Mizobuchi M, Ogata H, Hatamura I, Saji F, Koiwa F, Kinugasa E, Koshikawa S,Akizawa T. Activation of calcium-sensing receptor accelerates apoptosis in hyper-plastic parathyroid cells. Biochem Biophys Res Commun 362: 11–16, 2007.
747. Mogard MH, Maxwell V, Sytnik B, Walsh JH. Regulation of gastric acid secretion byneurotensin in man. Evidence against a hormonal role. J Clin Invest 80: 1064–1067,1987.
748. Monkawa T, Yoshida T, Wakino S, Shinki T, Anazawa H, Deluca HF, Suda T, HayashiM, Saruta T. Molecular cloning of cDNA and genomic DNA for human 25-hydroxyvi-tamin D3 1 alpha-hydroxylase. Biochem Biophys Res Commun 239: 527–533, 1997.
749. Monstein HJ, Nylander AG, Salehi A, Chen D, Lundquist I, Hakanson R. Cholecysto-kinin-A and cholecystokinin-B/gastrin receptor mRNA expression in the gastrointes-tinal tract and pancreas of the rat and man. A polymerase chain reaction study. ScandJ Gastroenterol 31: 383–390, 1996.
750. Morgan EL, Mace OJ, Affleck J, Kellett GL. Apical GLUT2 and Cav1.3: regulation ofrat intestinal glucose and calcium absorption. J Physiol 580: 593–604, 2007.
751. Morgan EL, Mace OJ, Helliwell PA, Affleck J, Kellett GL. A role for Ca(v)1.3 in ratintestinal calcium absorption. Biochem Biophys Res Commun 312: 487–493, 2003.
SASCHA KOPIC AND JOHN P. GEIBEL
256 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

752. Morii H, Lund J, Neville PF, DeLuca HF. Biological activity of a vitamin D metabolite.Arch Biochem Biophys 120: 508–512, 1967.
753. Mosekilde L, Sogaard CH, Danielsen CC, Torring O. The anabolic effects of humanparathyroid hormone (hPTH) on rat vertebral body mass are also reflected in thequality of bone, assessed by biomechanical testing: a comparison study betweenhPTH-(1–34) and hPTH-(1–84). Endocrinology 129: 421–428, 1991.
754. Motoyama HI, Friedman PA. Calcium-sensing receptor regulation of PTH-depen-dent calcium absorption by mouse cortical ascending limbs. Am J Physiol Renal Physiol283: F399–F406, 2002.
755. Muallem S, Fimmel CJ, Pandol SJ, Sachs G. Regulation of free cytosolic Ca2� in thepeptic and parietal cells of the rabbit gastric gland. J Biol Chem 261: 2660–2667,1986.
756. Muallem S, Karlish SJ. Studies on the mechanism of regulation of the red-cell Ca2�
pump by calmodulin and ATP. Biochim Biophys Acta 647: 73–86, 1981.
757. Muhe L, Lulseged S, Mason KE, Simoes EA. Case-control study of the role of nutri-tional rickets in the risk of developing pneumonia in Ethiopian children. Lancet 349:1801–1804, 1997.
758. Mulderry PK, Ghatei MA, Spokes RA, Jones PM, Pierson AM, Hamid QA, Kanse S,Amara SG, Burrin JM, Legon S. Differential expression of alpha-CGRP and beta-CGRP by primary sensory neurons and enteric autonomic neurons of the rat. Neu-roscience 25: 195–205, 1988.
759. Mun HC, Franks AH, Culverston EL, Krapcho K, Nemeth EF, Conigrave AD. TheVenus Fly Trap domain of the extracellular Ca2�-sensing receptor is required forL-amino acid sensing. J Biol Chem 279: 51739–51744, 2004.
760. Mungan Z, Hammer RA, Akarca US, Komaki G, Ertan A, Arimura A. Effect of PACAPon gastric acid secretion in rats. Peptides 16: 1051–1056, 1995.
761. Munson K, Garcia R, Sachs G. Inhibitor and ion binding sites on the gastric H�-K�-ATPase. Biochemistry 44: 5267–5284, 2005.
762. Munson K, Law RJ, Sachs G. Analysis of the gastric H,K ATPase for ion pathways andinhibitor binding sites. Biochemistry 46: 5398–5417, 2007.
763. Murayama A, Takeyama K, Kitanaka S, Kodera Y, Hosoya T, Kato S. The promoterof the human 25-hydroxyvitamin D3 1 alpha-hydroxylase gene confers positive andnegative responsiveness to PTH, calcitonin, and 1 alpha,25(OH)2D3. Biochem Bio-phys Res Commun 249: 11–16, 1998.
764. Murayama A, Takeyama K, Kitanaka S, Kodera Y, Kawaguchi Y, Hosoya T, Kato S.Positive and negative regulations of the renal 25-hydroxyvitamin D3 1alpha-hydrox-ylase gene by parathyroid hormone, calcitonin, and 1alpha,25(OH)2D3 in intactanimals. Endocrinology 140: 2224–2231, 1999.
765. Murer H, Hernando N, Forster I, Biber J. Proximal tubular phosphate reabsorption:molecular mechanisms. Physiol Rev 80: 1373–1409, 2000.
766. Murray CB, Morales MM, Flotte TR, McGrath-Morrow SA, Guggino WB, Zeitlin PL.CIC-2: a developmentally dependent chloride channel expressed in the fetal lung anddownregulated after birth. Am J Respir Cell Mol Biol 12: 597–604, 1995.
767. Mutt V, Jorpes JE. Structure of porcine cholecystokinin-pancreozymin. 1. Cleavagewith thrombin and with trypsin. Eur J Biochem 6: 156–162, 1968.
768. Nakajima K, Nohtomi K, Sato M, Takano K, Sato K. PTH(7–84) inhibits PTH(1–34)-induced 1,25-(OH)2D3 production in murine renal tubules. Biochem Biophys ResCommun 381: 283–287, 2009.
769. Nakajima T, Konda Y, Izumi Y, Kanai M, Hayashi N, Chiba T, Takeuchi T. Gastrinstimulates the growth of gastric pit cell precursors by inducing its own receptors. AmJ Physiol Gastrointest Liver Physiol 282: G359–G366, 2002.
770. Nakamura E, Hasumura M, Gabriel AS, Uneyama H, Torii K. Functional role ofcalcium-sensing receptor on somatostatin release from rat gastric mucosa (Ab-stract). Gastroenterology 138: S404, 2010.
771. Nakamura K, Zhou CJ, Parente J, Chew CS. Parietal cell MAP kinases: multipleactivation pathways. Am J Physiol Gastrointest Liver Physiol 271: G640 –G649,1996.
772. Nakata H, Matsui T, Ito M, Taniguchi T, Naribayashi Y, Arima N, Nakamura A,Kinoshita Y, Chihara K, Hosoda S. Cloning and characterization of gastrin receptor
from ECL carcinoid tumor of Mastomys natalensis. Biochem Biophys Res Commun187: 1151–1157, 1992.
773. Nandi J, Bosche MC, Levine RA. Effects of a phorbol ester and isoquinoline sulfon-amides on rabbit parietal cell function. J Pharmacol Exp Ther 279: 97–105, 1996.
774. Nandi J, Loo A, Kim SW, Levine RA. Expression and characterization of proteinkinase C in isolated rabbit parietal cells. Int J Mol Med 3: 521–526, 1999.
775. Napoli N, Pedone C, Pozzilli P, Lauretani F, Bandinelli S, Ferrucci L, Incalzi RA. Effectof ghrelin on bone mass density: the InChianti study. Bone 49: 257–263, 2011.
776. Naro F, Perez M, Migliaccio S, Galson DL, Orcel P, Teti A, Goldring SR. Phospho-lipase D- and protein kinase C isoenzyme-dependent signal transduction pathwaysactivated by the calcitonin receptor. Endocrinology 139: 3241–3248, 1998.
777. Natalucci G, Riedl S, Gleiss A, Zidek T, Frisch H. Spontaneous 24-h ghrelin secretionpattern in fasting subjects: maintenance of a meal-related pattern. Eur J Endocrinol152: 845–850, 2005.
778. Naveh-Many T, Rahamimov R, Livni N, Silver J. Parathyroid cell proliferation innormal and chronic renal failure rats. The effects of calcium, phosphate, and vitaminD. J Clin Invest 96: 1786–1793, 1995.
779. Nemere I. The 1,25D3-MARRS protein: contribution to steroid stimulated calciumuptake in chicks and rats. Steroids 70: 455–457, 2005.
780. Nemere I, Norman AW. 1,25-Dihydroxyvitamin D3-mediated vesicular transport ofcalcium in intestine: time-course studies. Endocrinology 122: 2962–2969, 1988.
781. Nemere I, Norman AW. Parathyroid hormone stimulates calcium transport in per-fused duodena from normal chicks: comparison with the rapid (transcaltachic) effectof 1,25-dihydroxyvitamin D3. Endocrinology 119: 1406–1408, 1986.
782. Nemere I, Safford SE, Rohe B, DeSouza MM, Farach-Carson MC. Identification andcharacterization of 1,25D3-membrane-associated rapid response, steroid (1,25D3-MARRS) binding protein. J Steroid Biochem Mol Biol 89–90: 281–285, 2004.
783. Nemere I, Szego CM. Early actions of parathyroid hormone and 1,25-dihydroxy-cholecalciferol on isolated epithelial cells from rat intestine. I. Limited lysosomalenzyme release and calcium uptake. Endocrinology 108: 1450–1462, 1981.
784. Nemere I, Szego CM. Early actions of parathyroid hormone and 1,25-dihydroxy-cholecalciferol on isolated epithelial cells from rat intestine. II. Analyses of additivity,contribution of calcium, and modulatory influence of indomethacin. Endocrinology109: 2180–2187, 1981.
785. Nemere I, Yoshimoto Y, Norman AW. Calcium transport in perfused duodena fromnormal chicks: enhancement within fourteen minutes of exposure to 1,25-dihy-droxyvitamin D3. Endocrinology 115: 1476–1483, 1984.
786. Nguyen-Yamamoto L, Rousseau L, Brossard JH, Lepage R, D’Amour P. Syntheticcarboxyl-terminal fragments of parathyroid hormone (PTH) decrease ionized cal-cium concentration in rats by acting on a receptor different from the PTH/PTH-related peptide receptor. Endocrinology 142: 1386–1392, 2001.
787. Nguyen TM, Lieberherr M, Fritsch J, Guillozo H, Alvarez ML, Fitouri Z, Jehan F,Garabedian M. The rapid effects of 1,25-dihydroxyvitamin D3 require the vitamin Dreceptor and influence 24-hydroxylase activity: studies in human skin fibroblastsbearing vitamin D receptor mutations. J Biol Chem 279: 7591–7597, 2004.
788. Niall HD, Keutmann H, Sauer R, Hogan M, Dawson B, Aurbach G, Potts J Jr. Theamino acid sequence of bovine parathyroid hormone I. Hoppe-Seylers Z Physiol Chem351: 1586–1588, 1970.
789. Nicar MJ, Pak CY. Calcium bioavailability from calcium carbonate and calcium ci-trate. J Clin Endocrinol Metab 61: 391–393, 1985.
790. Nicholson GC, Moseley JM, Sexton PM, Mendelsohn FA, Martin TJ. Abundant cal-citonin receptors in isolated rat osteoclasts. Biochemical and autoradiographic char-acterization. J Clin Invest 78: 355–360, 1986.
791. Niemeyer BA, Bergs C, Wissenbach U, Flockerzi V, Trost C. Competitive regulationof CaT-like-mediated Ca2� entry by protein kinase C and calmodulin. Proc Natl AcadSci USA 98: 3600–3605, 2001.
792. Nijenhuis T, Hoenderop JG, van der Kemp AW, Bindels RJ. Localization and regula-tion of the epithelial Ca2� channel TRPV6 in the kidney. J Am Soc Nephrol 14:2731–2740, 2003.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
257Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

793. Nilas L, Christiansen C. Vitamin D deficiency after highly selective vagotomy. ActaMed Scand 221: 303–306, 1987.
794. Nilas L, Christiansen C, Christiansen J. Regulation of vitamin D and calcium metab-olism after gastrectomy. Gut 26: 252–257, 1985.
795. Nilsson BE, Westlin NE. The fracture incidence after gastrectomy. Acta Chir Scand137: 533–534, 1971.
796. Nishimura M, Yaguti H, Yoshitsugu H, Naito S, Satoh T. Tissue distribution of mRNAexpression of human cytochrome P450 isoforms assessed by high-sensitivity real-time reverse transcription PCR. Yakugaku Zasshi 123: 369–375, 2003.
797. Nordin BE. Measurement and meaning of calcium absorption. Gastroenterology 54:294–301, 1968.
798. Norlen P, Bernsand M, Konagaya T, Hakanson R. ECL-cell histamine mobiliza-tion in conscious rats: effects of locally applied regulatory peptides, candidateneurotransmitters and inflammatory mediators. Br J Pharmacol 134: 1767–1777,2001.
799. Norman AW, Lund J, Deluca HF. Biologically active forms of vitamin D3 in kidney andintestine. Arch Biochem Biophys 108: 12–21, 1964.
800. Norman AW, Myrtle JF, Midgett RJ, Nowicki HG, Williams V, Popjak G. 1,25-Dihydroxycholecalciferol: identification of the proposed active form of vitamin D3 inthe intestine. Science 173: 51–54, 1971.
801. Norman AW, Okamura WH, Hammond MW, Bishop JE, Dormanen MC, Bouil-lon R, van Baelen H, Ridall AL, Daane E, Khoury R, Farach-Carson MC. Com-parison of 6-s-cis- and 6-s-trans-locked analogs of 1alpha,25-dihydroxyvitaminD3 indicates that the 6-s-cis conformation is preferred for rapid nongenomicbiological responses and that neither 6-s-cis- nor 6-s-trans-locked analogs arepreferred for genomic biological responses. Mol Endocrinol 11: 1518 –1531,1997.
802. Norman AW, Olivera CJ, Barreto Silva FR, Bishop JE. A specific binding protein/receptor for 1alpha,25-dihydroxyvitamin D(3) is present in an intestinal caveolaemembrane fraction. Biochem Biophys Res Commun 298: 414–419, 2002.
803. Noto T, Nagasaki M, Endo T. Role of vagus nerves and gastrin in the gastric phase ofacid secretion in male anesthetized rats. Am J Physiol Gastrointest Liver Physiol 272:G335–G339, 1997.
804. Nuttall ME, Patton AJ, Olivera DL, Nadeau DP, Gowen M. Human trabecular bonecells are able to express both osteoblastic and adipocytic phenotype: implications forosteopenic disorders. J Bone Miner Res 13: 371–382, 1998.
805. Nykjaer A, Dragun D, Walther D, Vorum H, Jacobsen C, Herz J, Melsen F, Chris-tensen EI, Willnow TE. An endocytic pathway essential for renal uptake and activa-tion of the steroid 25-(OH) vitamin D3. Cell 96: 507–515, 1999.
806. Nykjaer A, Fyfe JC, Kozyraki R, Leheste JR, Jacobsen C, Nielsen MS, Verroust PJ,Aminoff M, de la Chapelle A, Moestrup SK, Ray R, Gliemann J, Willnow TE, Chris-tensen EI. Cubilin dysfunction causes abnormal metabolism of the steroid hormone25(OH) vitamin D(3). Proc Natl Acad Sci USA 98: 13895–13900, 2001.
807. O’Connell MB, Madden DM, Murray AM, Heaney RP, Kerzner LJ. Effects of protonpump inhibitors on calcium carbonate absorption in women: a randomized cross-over trial. Am J Med 118: 778–781, 2005.
808. Offermanns S, Iida-Klein A, Segre GV, Simon MI. G alpha q family members coupleparathyroid hormone (PTH)/PTH-related peptide and calcitonin receptors to phos-pholipase C in COS-7 cells. Mol Endocrinol 10: 566–574, 1996.
809. Oginni LM, Worsfold M, Oyelami OA, Sharp CA, Powell DE, Davie MW. Etiology ofrickets in Nigerian children. J Pediatr 128: 692–694, 1996.
810. Oh DS, Lieu SN, Yamaguchi DJ, Tachiki K, Lambrecht N, Ohning GV, Sachs G,Germano PM, Pisegna JR. PACAP regulation of secretion and proliferation of purepopulations of gastric ECL cells. J Mol Neurosci 26: 85–97, 2005.
811. Oh KW, Lee WY, Rhee EJ, Baek KH, Yoon KH, Kang MI, Yun EJ, Park CY, Ihm SH,Choi MG, Yoo HJ, Park SW. The relationship between serum resistin, leptin, adi-ponectin, ghrelin levels and bone mineral density in middle-aged men. Clin Endocrinol63: 131–138, 2005.
812. Ohyama Y, Ozono K, Uchida M, Yoshimura M, Shinki T, Suda T, Yamamoto O.Functional assessment of two vitamin D-responsive elements in the rat 25-hy-droxyvitamin D3 24-hydroxylase gene. J Biol Chem 271: 30381–30385, 1996.
813. Okamoto CT, Karam SM, Jeng YY, Forte JG, Goldenring JR. Identification of clathrinand clathrin adaptors on tubulovesicles of gastric acid secretory (oxyntic) cells. Am JPhysiol Cell Physiol 274: C1017–C1029, 1998.
814. Okunade GW, Miller ML, Pyne GJ, Sutliff RL, O’Connor KT, Neumann JC, AndringaA, Miller DA, Prasad V, Doetschman T, Paul RJ, Shull GE. Targeted ablation of plasmamembrane Ca2�-ATPase (PMCA) 1 and 4 indicates a major housekeeping functionfor PMCA1 and a critical role in hyperactivated sperm motility and male fertility forPMCA4. J Biol Chem 279: 33742–33750, 2004.
815. Olesen C, Picard M, Winther AML, Gyrup C, Morth JP, Oxvig C, Moller JV, NissenP. The structural basis of calcium transport by the calcium pump. Nature 450:1036–1042, 2007.
816. Oscarson J, Hakanson R, Liedberg G, Lundqvist G, Sundler F, Thorell J. Variatedserum gastrin concentration: trophic effects on the gastrointestinal tract of the rat.Acta Physiol Scand Suppl 475: 2–27, 1979.
817. Owen TA, Aronow MS, Barone LM, Bettencourt B, Stein GS, Lian JB. Pleiotropiceffects of vitamin D on osteoblast gene expression are related to the proliferativeand differentiated state of the bone cell phenotype: dependency upon basal levels ofgene expression, duration of exposure, and bone matrix competency in normal ratosteoblast cultures. Endocrinology 128: 1496–1504, 1991.
818. Owyang C, Miller LJ, DiMagno EP, Brennan LA Jr, Go VL. Gastrointestinal hormoneprofile in renal insufficiency. Mayo Clin Proc 54: 769–773, 1979.
819. Paillard F, Ardaillou R, Malendin H, Fillastre JP, Prier S. Renal effects of salmoncalcitonin in man. J Lab Clin Med 80: 200–216, 1972.
820. Pan Q, Ma J, Zhou Q, Li J, Tang Y, Liu Y, Yang Y, Xiao J, Peng L, Li P, Liang D, ZhangH, Chen YH. KCNQ1 loss-of-function mutation impairs gastric acid secretion inmice. Mol Biol Rep 37: 1329–1333, 2010.
821. Panda DK, Miao D, Bolivar I, Li J, Huo R, Hendy GN, Goltzman D. Inactivation of the25-hydroxyvitamin D 1alpha-hydroxylase and vitamin D receptor demonstrates in-dependent and interdependent effects of calcium and vitamin D on skeletal andmineral homeostasis. J Biol Chem 279: 16754–16766, 2004.
822. Panda DK, Miao D, Tremblay ML, Sirois J, Farookhi R, Hendy GN, Goltzman D.Targeted ablation of the 25-hydroxyvitamin D 1alpha-hydroxylase enzyme: evi-dence for skeletal, reproductive, and immune dysfunction. Proc Natl Acad Sci USA 98:7498–7503, 2001.
823. Pannabecker TL, Chandler JS, Wasserman RH. Vitamin-D-dependent transcriptionalregulation of the intestinal plasma membrane calcium pump. Biochem Biophys ResCommun 213: 499–505, 1995.
824. Pansu D, Bellaton C, Bronner F. Effect of Ca intake on saturable and nonsaturablecomponents of duodenal Ca transport. Am J Physiol Gastrointest Liver Physiol 240:G32–G37, 1981.
825. Pansu D, Bellaton C, Roche C, Bronner F. Duodenal and ileal calcium absorption inthe rat and effects of vitamin D. Am J Physiol Gastrointest Liver Physiol 244: G695–G700, 1983.
826. Parhon C, Ureche CS. Untersuchungen uber den Einfluss den die Calcium undSodiumsalze auf den Verlauf der experimentellen Tetanie ausuben. Neurol Centr 26:1099, 1907.
827. Park J, Chiba T, Yamada T. Mechanisms for direct inhibition of canine gastric parietalcells by somatostatin. J Biol Chem 262: 14190–14196, 1987.
828. Parkinson DB, Thakker RV. A donor splice site mutation in the parathyroid hormonegene is associated with autosomal recessive hypoparathyroidism. Nat Genet 1: 149–152, 1992.
829. Parthemore JG, Deftos LJ. Calcitonin secretion in normal human subjects. J ClinEndocrinol Metab 47: 184–188, 1978.
830. Patterson EK, Hodsman AB, Hendy GN, Canaff L, Bringhurst FR, Fraher LJ. Func-tional analysis of a type 1 parathyroid hormone receptor intracellular tail mutant[KRK(484–6)AAA]: effects on second messenger generation and cellular targeting.Bone 46: 1180–1187, 2010.
831. Patton MB. Further experiments on the utilization of calcium from salts by collegewomen. J Nutr 55: 519–526, 1955.
832. Patton MB, Sutton TS. The utilization of calcium from lactate, gluconate, sulfate andcarbonate salts by young college women. J Nutr 48: 443–452, 1952.
SASCHA KOPIC AND JOHN P. GEIBEL
258 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

833. Pawlow JP, Schumowa-Simanowskaja EO. Beitrage zur Physiologie der Absonder-ungen. Die Innervation der Magendrusen beim Hunde. Arch Anat Physiol 54–69,1895.
834. Pearce SH, Bai M, Quinn SJ, Kifor O, Brown EM, Thakker RV. Functional character-ization of calcium-sensing receptor mutations expressed in human embryonic kidneycells. J Clin Invest 98: 1860–1866, 1996.
835. Pedersen JI, Holmberg I, Bjorkhem I. Reconstitution of vitamin D3 25-hydroxylaseactivity with a cytochrome P-450 preparation from rat liver mitochondria. FEBS Lett98: 394–398, 1979.
836. Peng JB, Brown EM, Hediger MA. Structural conservation of the genes encodingCaT1, CaT2, and related cation channels. Genomics 76: 99–109, 2001.
837. Peng JB, Chen XZ, Berger UV, Vassilev PM, Brown EM, Hediger MA. A rat kidney-specific calcium transporter in the distal nephron. J Biol Chem 275: 28186–28194,2000.
838. Peng JB, Chen XZ, Berger UV, Vassilev PM, Tsukaguchi H, Brown EM, Hediger MA.Molecular cloning and characterization of a channel-like transporter mediating in-testinal calcium absorption. J Biol Chem 274: 22739–22746, 1999.
839. Peng JB, Zhuang L, Berger UV, Adam RM, Williams BJ, Brown EM, Hediger MA,Freeman MR. CaT1 expression correlates with tumor grade in prostate cancer.Biochem Biophys Res Commun 282: 729–734, 2001.
840. Perez JF, Ruiz MC, Michelangeli F. Simultaneous measurement and imaging of intra-cellular Ca2� and H� transport in isolated rabbit gastric glands. J Physiol 537: 735–745, 2001.
841. Persson P, Gagnemo-Persson R, Chen D, Axelson J, Nylander AG, Johnell O, Ha-kanson R. Gastrectomy causes bone loss in the rat: is lack of gastric acid responsible?Scand J Gastroenterol 28: 301–306, 1993.
842. Persson P, Gagnemo-Persson R, Orberg J, Chen D, Hakanson R. Effects of gastrin oncalcium homeostasis in chickens. Endocrinology 129: 1162–1166, 1991.
843. Persson P, Grunditz T, Axelson J, Sundler F, Hakanson R. Cholecystokinins but notgastrin-17 release calcitonin from thyroid C-cells in the rat. Regul Pept 21: 45–56,1988.
844. Persson P, Hakanson R, Axelson J, Sundler F. Gastrin releases a blood calcium-lowering peptide from the acid-producing part of the rat stomach. Proc Natl Acad SciUSA 86: 2834–2838, 1989.
845. Petrovic S, Wang Z, Ma L, Seidler U, Forte JG, Shull GE, Soleimani M. Colocalizationof the apical Cl�/HCO3
� exchanger PAT1 and gastric H�-K�-ATPase in stomachparietal cells. Am J Physiol Gastrointest Liver Physiol 283: G1207–G1216, 2002.
846. Pfeiffer A, Rochlitz H, Noelke B, Tacke R, Moser U, Mutschler E, Lambrecht G.Muscarinic receptors mediating acid secretion in isolated rat gastric parietal cells areof M3 type. Gastroenterology 98: 218–222, 1990.
847. Pfister MF, Lederer E, Forgo J, Ziegler U, Lotscher M, Quabius ES, Biber J, Murer H.Parathyroid hormone-dependent degradation of type II Na�/Pi cotransporters. J BiolChem 272: 20125–20130, 1997.
848. Phelps CB, Huang RJ, Lishko PV, Wang RR, Gaudet R. Structural analyses of theankyrin repeat domain of TRPV6 and related TRPV ion channels. Biochemistry 47:2476–2484, 2008.
849. Pi M, Chen L, Huang M, Luo Q, Quarles LD. Parathyroid-specific interaction of thecalcium-sensing receptor and G alpha q. Kidney Int 74: 1548–1556, 2008.
850. Pi M, Chen L, Huang MZ, Zhu W, Ringhofer B, Luo J, Christenson L, Li B, Zhang J,Jackson PD, Faber P, Brunden KR, Harrington JJ, Quarles LD. GPRC6A null miceexhibit osteopenia, feminization and metabolic syndrome. PLoS One 3: e3858, 2008.
851. Pi M, Faber P, Ekema G, Jackson PD, Ting A, Wang N, Fontilla-Poole M, Mays RW,Brunden KR, Harrington JJ, Quarles LD. Identification of a novel extracellular cation-sensing G-protein-coupled receptor. J Biol Chem 280: 40201–40209, 2005.
852. Pi M, Garner SC, Flannery P, Spurney RF, Quarles LD. Sensing of extracellularcations in CasR-deficient osteoblasts. Evidence for a novel cation-sensing mecha-nism. J Biol Chem 275: 3256–3263, 2000.
853. Pi M, Oakley RH, Gesty-Palmer D, Cruickshank RD, Spurney RF, Luttrell LM, Quar-les LD. Beta-arrestin- and G protein receptor kinase-mediated calcium-sensing re-ceptor desensitization. Mol Endocrinol 19: 1078–1087, 2005.
854. Pi M, Zhang L, Lei SF, Huang MZ, Zhu W, Zhang J, Shen H, Deng HW, Quarles LD.Impaired osteoblast function in GPRC6A null mice. J Bone Miner Res 25: 1092–1102,2010.
855. Picard N, Capuano P, Stange G, Mihailova M, Kaissling B, Murer H, Biber J, WagnerCA. Acute parathyroid hormone differentially regulates renal brush border mem-brane phosphate cotransporters. Pflügers Arch 460: 677–687, 2010.
856. Pickard BW, Hodsman AB, Fraher LJ, Watson PH. Type 1 parathyroid hormonereceptor (PTH1R) nuclear trafficking: association of PTH1R with importin alpha1and beta. Endocrinology 147: 3326–3332, 2006.
857. Pickard BW, Hodsman AB, Fraher LJ, Watson PH. Type 1 parathyroid hormonereceptor (PTH1R) nuclear trafficking: regulation of PTH1R nuclear-cytoplasmicshuttling by importin-alpha/beta and chromosomal region maintenance 1/exportin 1.Endocrinology 148: 2282–2289, 2007.
858. Pidasheva S, Grant M, Canaff L, Ercan O, Kumar U, Hendy GN. Calcium-sensingreceptor dimerizes in the endoplasmic reticulum: biochemical and biophysical char-acterization of CASR mutants retained intracellularly. Hum Mol Genet 15: 2200–2209, 2006.
859. Pines M, Fukayama S, Costas K, Meurer E, Goldsmith PK, Xu X, Muallem S, Behar V,Chorev M, Rosenblatt M, Tashjian AH Jr, Suva LJ. Inositol 1-,4-,5-trisphosphate-dependent Ca2� signaling by the recombinant human PTH/PTHrP receptor stablyexpressed in a human kidney cell line. Bone 18: 381–389, 1996.
860. Pioszak AA, Harikumar KG, Parker NR, Miller LJ, Xu HE. Dimeric arrangement ofthe parathyroid hormone receptor and a structural mechanism for ligand-induceddissociation. J Biol Chem 285: 12435–12444, 2010.
861. Pioszak AA, Xu HE. Molecular recognition of parathyroid hormone by its G protein-coupled receptor. Proc Natl Acad Sci USA 105: 5034–5039, 2008.
862. Piqueras L, Tache Y, Martinez V. Peripheral PACAP inhibits gastric acid secretionthrough somatostatin release in mice. Br J Pharmacol 142: 67–78, 2004.
863. Polak JM, Sullivan SN, Bloom SR, Buchan AM, Facer P, Brown MR, Pearse AG.Specific localisation of neurotensin to the N cell in human intestine by radioimmu-noassay and immunocytochemistry. Nature 270: 183–184, 1977.
864. Ponchon G, DeLuca HF. The role of the liver in the metabolism of vitamin D. J ClinInvest 48: 1273–1279, 1969.
865. Ponchon G, Kennan AL, DeLuca HF. “Activation” of vitamin D by the liver. J ClinInvest 48: 2032–2037, 1969.
866. Popielski L. Beta-imidazolylathylamin und die Organextrakte. Erster Teil: beta-imi-dazolylathylamin als machtiger Erreger der Magendrusen. Pflügers Arch 178: 214–236, 1920.
867. Potts JT Jr, Tregear GW, Keutmann HT, Niall HD, Sauer R, Deftos LJ, Dawson BF,Hogan ML, Aurbach GD. Synthesis of a biologically active N-terminal tetratriacon-tapeptide of parathyroid hormone. Proc Natl Acad Sci USA 68: 63–67, 1971.
868. Pouwels S, Lalmohamed A, Souverein P, Cooper C, Veldt BJ, Leufkens HG, DeBoer A, Van Staa T, De Vries F. Use of proton pump inhibitors and risk ofhip/femur fracture: A population-based case-control study. Osteoporosis Int 22:903–910, 2011.
869. Prader A, Illig R, Heierli E. Eine besondere Form der primären Vitamin D resistentenTachitis mit Hypocalcemie und autosomal dominantem Erbgang: die hereditärePseudomangelrachitis. Helv Paediatr Acta 16: 452–468, 1961.
870. Prince CW, Butler WT. 1,25-Dihydroxyvitamin D3 regulates the biosynthesis ofosteopontin, a bone-derived cell attachment protein, in clonal osteoblast-like osteo-sarcoma cells. Coll Relat Res 7: 305–313, 1987.
871. Prinz C, Kajimura M, Scott DR, Mercier F, Helander HF, Sachs G. Histamine secre-tion from rat enterochromaffinlike cells. Gastroenterology 105: 449–461, 1993.
872. Prinz C, Neumayer N, Mahr S, Classen M, Schepp W. Functional impairment of ratenterochromaffin-like cells by interleukin 1 beta. Gastroenterology 112: 364–375,1997.
873. Prinz C, Sachs G, Walsh JH, Coy DH, Wu SV. The somatostatin receptor subtype onrat enterochromaffinlike cells. Gastroenterology 107: 1067–1074, 1994.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
259Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

874. Prosser DE, Guo Y, Jia Z, Jones G. Structural motif-based homology modeling ofCYP27A1 and site-directed mutational analyses affecting vitamin D hydroxylation.Biophys J 90: 3389–3409, 2006.
875. Prunier JH, Bearn AG, Cleve H. Site of formation of the group-specific componentand certain other serum proteins. Proc Soc Exp Biol Med 115: 1005–1007, 1964.
876. Pyrah LN, Smith IB. Osteomalacia following gastrectomy. Lancet 270: 935–937,1956.
877. Quamme GA. Effect of calcitonin on calcium and magnesium transport in ratnephron. Am J Physiol Endocrinol Metab 238: E573–E578, 1980.
878. Quinn JM, Morfis M, Lam MH, Elliott J, Kartsogiannis V, Williams ED, Gillespie MT,Martin TJ, Sexton PM. Calcitonin receptor antibodies in the identification of oste-oclasts. Bone 25: 1–8, 1999.
879. Quinn SJ, Bai M, Brown EM. pH Sensing by the calcium-sensing receptor. J Biol Chem279: 37241–37249, 2004.
880. Quinn SJ, Ye CP, Diaz R, Kifor O, Bai M, Vassilev P, Brown E. The Ca2�-sensingreceptor: a target for polyamines. Am J Physiol Cell Physiol 273: C1315–C1323, 1997.
881. Raczynski J. Recherches expérimentales sur le manque d’action du soleil commecause du rachitisme. In: C R Assoc Internat Pediatrie. Paris: 1912, p. 308–309.
882. Rakopoulos M, Ikegame M, Findlay DM, Martin TJ, Moseley JM. Short treatment ofosteoclasts in bone marrow culture with calcitonin causes prolonged suppression ofcalcitonin receptor mRNA. Bone 17: 447–453, 1995.
883. Rasmussen H, Anast C, Arnaud C. Thyrocalcitonin, EGTA, and urinary electrolyteexcretion. J Clin Invest 46: 746–752, 1967.
884. Rautureau M, Rambaud JC. Aqueous solubilisation of vitamin D3 in normal man. Gut22: 393–397, 1981.
885. Ravazzola M, Benoit R, Ling N, Orci L. Prosomatostatin-derived antrin is present ingastric D cells and in portal blood. J Clin Invest 83: 362–366, 1989.
886. Ray JM, Squires PE, Curtis SB, Meloche MR, Buchan AM. Expression of the calcium-sensing receptor on human antral gastrin cells in culture. J Clin Invest 99: 2328–2333,1997.
887. Ray K, Clapp P, Goldsmith PK, Spiegel AM. Identification of the sites of N-linkedglycosylation on the human calcium receptor and assessment of their role in cellsurface expression and signal transduction. J Biol Chem 273: 34558–34567, 1998.
888. Ray K, Hauschild BC, Steinbach PJ, Goldsmith PK, Hauache O, Spiegel AM. Identifi-cation of the cysteine residues in the amino-terminal extracellular domain of thehuman Ca2� receptor critical for dimerization. Implications for function of mono-meric Ca2� receptor. J Biol Chem 274: 27642–27650, 1999.
889. Raychowdhury R, Fleming JV, McLaughlin JT, Bulitta CJ, Wang TC. Identification andcharacterization of a third gastrin response element (GAS-RE3) in the human histi-dine decarboxylase gene promoter. Biochem Biophys Res Commun 297: 1089–1095,2002.
890. Raychowdhury R, Zhang Z, Hocker M, Wang TC. Activation of human histidinedecarboxylase gene promoter activity by gastrin is mediated by two distinct nuclearfactors. J Biol Chem 274: 20961–20969, 1999.
891. Recker RR. Calcium absorption and achlorhydria. N Engl J Med 313: 70–73, 1985.
892. Reddy GS, Norman AW, Willis DM, Goltzman D, Guyda H, Solomon S, Philips DR,Bishop JE, Mayer E. Regulation of vitamin D metabolism in normal human pregnancy.J Clin Endocrinol Metab 56: 363–370, 1983.
893. Reddy GS, Tserng KY. Calcitroic acid, end product of renal metabolism of 1,25-dihydroxyvitamin D3 through C-24 oxidation pathway. Biochemistry 28: 1763–1769,1989.
894. Reed JS, Meredith SC, Nemchausky BA, Rosenberg IH, Boyer JL. Bone disease inprimary biliary cirrhosis: reversal of osteomalacia with oral 25-hydroxyvitamin D.Gastroenterology 78: 512–517, 1980.
895. Reenstra WW, Forte JG. Characterization of K� and Cl� conductances in apicalmembrane vesicles from stimulated rabbit oxyntic cells. Am J Physiol GastrointestLiver Physiol 259: G850–G858, 1990.
896. Reerink EH, Van Wijk W. The vitamin D problem. Biochem J 25: 1001–1009, 1931.
897. Reeve J, Meunier PJ, Parsons JA, Bernat M, Bijvoet OL, Courpron P, Edouard C,Klenerman L, Neer RM, Renier JC, Slovik D, Vismans FJ, Potts JT Jr. Anabolic effectof human parathyroid hormone fragment on trabecular bone in involutional osteo-porosis: a multicentre trial. Br Med J 280: 1340–1344, 1980.
898. Reiss AB, Martin KO, Rojer DE, Iyer S, Grossi EA, Galloway AC, Javitt NB. Sterol27-hydroxylase: expression in human arterial endothelium. J Lipid Res 38: 1254–1260, 1997.
899. Remy C, Kirchhoff P, Hafner P, Busque SM, Mueller MK, Geibel JP, Wagner CA.Stimulatory pathways of the Calcium-sensing receptor on acid secretion in freshlyisolated human gastric glands. Cell Physiol Biochem 19: 33–42, 2007.
900. Rengifo-Cam W, Umar S, Sarkar S, Singh P. Antiapoptotic effects of progastrin onpancreatic cancer cells are mediated by sustained activation of nuclear factor-�B.Cancer Res 67: 7266–7274, 2007.
901. Renkema KY, Velic A, Dijkman HB, Verkaart S, van der Kemp AW, Nowik M,Timmermans K, Doucet A, Wagner CA, Bindels RJ, Hoenderop JG. The calcium-sensing receptor promotes urinary acidification to prevent nephrolithiasis. J Am SocNephrol 20: 1705–1713, 2009.
902. Repa JJ, Lund EG, Horton JD, Leitersdorf E, Russell DW, Dietschy JM, Turley SD.Disruption of the sterol 27-hydroxylase gene in mice results in hepatomegaly andhypertriglyceridemia. Reversal by cholic acid feeding. J Biol Chem 275: 39685–39692,2000.
903. Resnick RH, Adelardi CF, Gray SJ. Stimulation of gastric secretion in man by aserotonin antagonist. Gastroenterology 42: 22–25, 1962.
904. Reubi JC, Waser B, Horisberger U, Halter F, Soroka CJ, Kumar RR, Goldenring JR,Modlin IM. Identification of somatostatin and gastrin receptors on enterochromaffin-like cells from Mastomys gastric tumors. Endocrinology 131: 166–172, 1992.
905. Reubi JC, Waser B, Laderach U, Stettler C, Friess H, Halter F, Schmassmann A.Localization of cholecystokinin A and cholecystokinin B-gastrin receptors in thehuman stomach. Gastroenterology 112: 1197–1205, 1997.
906. Riccardi D, Brown EM. Physiology and pathophysiology of the calcium-sensing re-ceptor in the kidney. Am J Physiol Renal Physiol 298: F485–F499, 2010.
907. Riccardi D, Hall AE, Chattopadhyay N, Xu JZ, Brown EM, Hebert SC. Localization ofthe extracellular Ca2�/polyvalent cation-sensing protein in rat kidney. Am J PhysiolRenal Physiol 274: F611–F622, 1998.
908. Riccardi D, Lee WS, Lee K, Segre GV, Brown EM, Hebert SC. Localization of theextracellular Ca2�-sensing receptor and PTH/PTHrP receptor in rat kidney. Am JPhysiol Renal Fluid Electrolyte Physiol 271: F951–F956, 1996.
909. Riccardi D, Traebert M, Ward DT, Kaissling B, Biber J, Hebert SC, Murer H. Dietaryphosphate and parathyroid hormone alter the expression of the calcium-sensingreceptor (CaR) and the Na�-dependent Pi transporter (NaPi-2) in the rat proximaltubule. Pflügers Arch 441: 379–387, 2000.
910. Richardson CT, Walsh JH, Cooper KA, Feldman M, Fordtran JS. Studies on the roleof cephalic-vagal stimulation in the acid secretory response to eating in normalhuman subjects. J Clin Invest 60: 435–441, 1977.
911. Ridefelt P, Hellman P, Stridsberg M, Akerstrom G, Rastad J. Different secretoryactions of pancreastatin in bovine and human parathyroid cells. Biosci Rep 14: 221–229, 1994.
912. Robert A, Olafsson AS, Lancaster C, Zhang WR. Interleukin-1 is cytoprotective,antisecretory, stimulates PGE2 synthesis by the stomach, retards gastric emptying.Life Sci 48: 123–134, 1991.
913. Robinson CJ, Spanos E, James MF, Pike JW, Haussler MR, Makeen AM, Hillyard CJ,MacIntyre I. Role of prolactin in vitamin D metabolism and calcium absorption duringlactation in the rat. J Endocrinol 94: 443–453, 1982.
914. Rochel N, Wurtz JM, Mitschler A, Klaholz B, Moras D. The crystal structure of thenuclear receptor for vitamin D bound to its natural ligand. Mol Cell 5: 173–179, 2000.
915. Rodriguez L, Tu C, Cheng Z, Chen TH, Bikle D, Shoback D, Chang W. Expressionand functional assessment of an alternatively spliced extracellular Ca2�-sensing re-ceptor in growth plate chondrocytes. Endocrinology 146: 5294–5303, 2005.
916. Rodriguez ME, Almaden Y, Canadillas S, Canalejo A, Siendones E, Lopez I, Aguilera-Tejero E, Martin D, Rodriguez M. The calcimimetic R-568 increases vitamin D
SASCHA KOPIC AND JOHN P. GEIBEL
260 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

receptor expression in rat parathyroid glands. Am J Physiol Renal Physiol 292: F1390–F1395, 2007.
917. Roepke TK, Anantharam A, Kirchhoff P, Busque SM, Young JB, Geibel JP, Lerner DJ,Abbott GW. The KCNE2 potassium channel ancillary subunit is essential for gastricacid secretion. J Biol Chem 281: 23740–23747, 2006.
918. Rosen H, Reshef A, Maeda N, Lippoldt A, Shpizen S, Triger L, Eggertsen G, Bjork-hem I, Leitersdorf E. Markedly reduced bile acid synthesis but maintained levels ofcholesterol and vitamin D metabolites in mice with disrupted sterol 27-hydroxylasegene. J Biol Chem 273: 14805–14812, 1998.
919. Rosenblatt M, Segre GV, Tyler GA, Shepard GL, Nussbaum SR, Potts JT Jr. Identifi-cation of a receptor-binding region in parathyroid hormone. Endocrinology 107:545–550, 1980.
920. Ross TK, Darwish HM, Moss VE, DeLuca HF. Vitamin D-influenced gene expressionvia a ligand-independent, receptor-DNA complex intermediate. Proc Natl Acad SciUSA 90: 9257–9260, 1993.
921. Rost CR, Bikle DD, Kaplan RA. In vitro stimulation of 25-hydroxycholecalciferol 1alpha-hydroxylation by parathyroid hormone in chick kidney slices: evidence for arole for adenosine 3=,5=-monophosphate. Endocrinology 108: 1002–1006, 1981.
922. Roth J, Thorens B, Hunziker W, Norman AW, Orci L. Vitamin D-dependent calciumbinding protein: immunocytochemical localization in chick kidney. Science 214: 197–200, 1981.
923. Roux C, Briot K, Gossec L, Kolta S, Blenk T, Felsenberg D, Reid DM, Eastell R, GlüerCC. Increase in vertebral fracture risk in postmenopausal women using omeprazole.Calcified Tissue Int 84: 13–19, 2009.
924. Rovner AJ, Stallings VA, Schall JI, Leonard MB, Zemel BS. Vitamin D insufficiency inchildren, adolescents, and young adults with cystic fibrosis despite routine oral sup-plementation. Am J Clin Nutr 86: 1694–1699, 2007.
925. Rowe DW, Kream BE. Regulation of collagen synthesis in fetal rat calvaria by 1,25-dihydroxyvitamin D3. J Biol Chem 257: 8009–8015, 1982.
926. Rowling MJ, Kemmis CM, Taffany DA, Welsh J. Megalin-mediated endocytosis ofvitamin D binding protein correlates with 25-hydroxycholecalciferol actions in hu-man mammary cells. J Nutr 136: 2754–2759, 2006.
927. Rumenapf G, Schwille PO, Erben RG, Schreiber M, Berge B, Fries W, Schmiedl A,Koroma S, Hohenberger W. Gastric fundectomy in the rat: effects on mineral andbone metabolism, with emphasis on the gastrin-calcitonin-parathyroid hormone-vitamin D axis. Calcif Tissue Int 63: 433–441, 1998.
928. Rumenapf G, Schwille PO, Wagner W, Tiecks FP, Fries W, Galewski D. Highlyselective vagotomy in the rat: effects on bone and mineral metabolism. Scand JGastroenterol 29: 232–237, 1994.
929. Rune SJ. Acid-base parameters of duodenal contents in man. Gastroenterology 62:533–539, 1972.
930. Russell J, Bar A, Sherwood LM, Hurwitz S. Interaction between calcium and 1,25-dihydroxyvitamin D3 in the regulation of preproparathyroid hormone and vitamin Dreceptor messenger ribonucleic acid in avian parathyroids. Endocrinology 132: 2639–2644, 1993.
931. Russell J, Lettieri D, Sherwood LM. Suppression by 1,25(OH)2D3 of transcription ofthe pre-proparathyroid hormone gene. Endocrinology 119: 2864–2866, 1986.
932. Rutten MJ, Bacon KD, Marlink KL, Stoney M, Meichsner CL, Lee FP, Hobson SA,Rodland KD, Sheppard BC, Trunkey DD, Deveney KE, Deveney CW. Identificationof a functional Ca2�-sensing receptor in normal human gastric mucous epithelialcells. Am J Physiol Gastrointest Liver Physiol 277: G662–G670, 1999.
933. Saarem K, Pedersen JI. Sex differences in the hydroxylation of cholecalciferol and of5 beta-cholestane-3 alpha,7 alpha,12 alpha-triol in rat liver. Biochem J 247: 73–78,1987.
934. Sabbieti MG, Agas D, Xiao L, Marchetti L, Coffin JD, Doetschman T, Hurley MM.Endogenous FGF-2 is critically important in PTH anabolic effects on bone. J CellPhysiol 219: 143–151, 2009.
935. Saccomani G, Psarras CG, Smith PR, Kirk KL, Shoemaker RL. Histamine-inducedchloride channels in apical membrane of isolated rabbit parietal cells. Am J Physiol CellPhysiol 260: C1000–C1011, 1991.
936. Sachs G, Shin JM, Briving C, Wallmark B, Hersey S. The pharmacology of the gastricacid pump: the H�,K� ATPase. Annu Rev Pharmacol Toxicol 35: 277–305, 1995.
937. Safadi FF, Thornton P, Magiera H, Hollis BW, Gentile M, Haddad JG, Liebhaber SA,Cooke NE. Osteopathy and resistance to vitamin D toxicity in mice null for vitaminD binding protein. J Clin Invest 103: 239–251, 1999.
938. Sakurada T, Ro S, Onouchi T, Ohno S, Aoyama T, Chinen K, Takabayashi H, Kato S,Takayama K, Yakabi K. Comparison of the actions of acylated and desacylatedghrelin on acid secretion in the rat stomach. J Gastroenterol 45: 1111–1120, 2010.
939. Salvesen HA. The function of the parathyroids. J Biol Chem 56: 443–456, 1923.
940. Sandle GI, Fraser G, Long S, Warhurst G. A cAMP-activated chloride channel in theplasma membrane of cultured human gastric cells (HGT-1). Pflügers Arch 417: 259–263, 1990.
941. Sandor A, Kidd M, Lawton GP, Miu K, Tang LH, Modlin IM. Neurohormonal mod-ulation of rat enterochromaffin-like cell histamine secretion. Gastroenterology 110:1084–1092, 1996.
942. Sands JM, Flores FX, Kato A, Baum MA, Brown EM, Ward DT, Hebert SC, HarrisHW. Vasopressin-elicited water and urea permeabilities are altered in IMCD inhypercalcemic rats. Am J Physiol Renal Physiol 274: F978–F985, 1998.
943. Sands JM, Naruse M, Baum M, Jo I, Hebert SC, Brown EM, Harris HW. Apicalextracellular calcium/polyvalent cation-sensing receptor regulates vasopressin-elic-ited water permeability in rat kidney inner medullary collecting duct. J Clin Invest 99:1399–1405, 1997.
944. Sandvik AK, Cui G, Bakke I, Munkvold B, Waldum HL. PACAP stimulates gastric acidsecretion in the rat by inducing histamine release. Am J Physiol Gastrointest LiverPhysiol 281: G997–G1003, 2001.
945. Sandvik AK, Dimaline R, Forster ER, Evans D, Dockray GJ. Differential control ofsomatostatin messenger RNA in rat gastric corpus and antrum. Role of acid, food,and capsaicin-sensitive afferent neurons. J Clin Invest 91: 244–250, 1993.
946. Sandvik AK, Kleveland PM, Waldum HL. Muscarinic M2 stimulation releases hista-mine in the totally isolated, vascularly perfused rat stomach. Scand J Gastroenterol 23:1049–1056, 1988.
947. Saperas E, Cominelli F, Tache Y. Potent inhibition of gastric acid secretion by intra-venous interleukin-1 beta and -1 alpha in rats. Peptides 13: 221–226, 1992.
948. Saperas E, Yang H, Tache Y. Interleukin-1 beta acts at hypothalamic sites to inhibitgastric acid secretion in rats. Am J Physiol Gastrointest Liver Physiol 263: G414–G418,1992.
949. Saperas ES, Yang H, Rivier C, Tache Y. Central action of recombinant interleukin-1to inhibit acid secretion in rats. Gastroenterology 99: 1599–1606, 1990.
950. Sawada N, Sakaki T, Ohta M, Inouye K. Metabolism of vitamin D3 by humanCYP27A1. Biochem Biophys Res Commun 273: 977–984, 2000.
951. Schachter D. Toward a molecular description of active transport. In: Biological Mem-branes, edited by Dowben RM. Boston: Little, Brown, 1969, p. 157–176.
952. Schachter D, Dowdle EB, Schenker H. Active transport of calcium by the smallintestine of the rat. Am J Physiol 198: 263–268, 1960.
953. Schachter D, Finkelstein JD, Kowarski S. Metabolism of vitamin D. I. Preparation ofradioactive vitamin D and its intestinal absorption in the rat. J Clin Invest 43: 787–796,1964.
954. Schachter D, Rosen SM. Active transport of Ca45 by the small intestine and itsdependence on vitamin D. Am J Physiol 196: 357–362, 1959.
955. Schaffalitzky de Muckadell OB, Fahrenkrug J. Secretion pattern of secretin in man:regulation by gastric acid. Gut 19: 812–818, 1978.
956. Schatzmann HJ. ATP-dependent Ca2�-extrusion from human red cells. Experientia22: 364–365, 1966.
957. Schayer RW. Formation and binding of histamine by rat tissues in vitro. Am J Physiol187: 63–65, 1956.
958. Schepp W, Dehne K, Herrmuth H, Pfeffer K, Prinz C. Identification and functionalimportance of IL-1 receptors on rat parietal cells. Am J Physiol Gastrointest LiverPhysiol 275: G1094–G1105, 1998.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
261Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

959. Schepp W, Dehne K, Riedel T, Schmidtler J, Schaffer K, Classen M. Oxyntomodulin:a cAMP-dependent stimulus of rat parietal cell function via the receptor for gluca-gon-like peptide-1 (7–36)NH2. Digestion 57: 398–405, 1996.
960. Schepp W, Prinz C, Hakanson R, Schusdziarra V, Classen M. Bombesin-like peptidesstimulate gastrin release from isolated rat G-cells. Regul Pept 28: 241–253, 1990.
961. Schepp W, Prinz C, Tatge C, Hakanson R, Schusdziarra V, Classen M. Galanin inhibitsgastrin release from isolated rat gastric G-cells. Am J Physiol Gastrointest Liver Physiol258: G596–G602, 1990.
962. Schiller LR, Walsh JH, Feldman M. Distention-induced gastrin release: effects ofluminal acidification and intravenous atropine. Gastroenterology 78: 912–917, 1980.
963. Schinke T, Schilling AF, Baranowsky A, Seitz S, Marshall RP, Linn T, Blaeker M,Huebner AK, Schulz A, Simon R, Gebauer M, Priemel M, Kornak U, Perkovic S,Barvencik F, Beil FT, Del Fattore A, Frattini A, Streichert T, Pueschel K, Villa A,Debatin KM, Rueger JM, Teti A, Zustin J, Sauter G, Amling M. Impaired gastricacidification negatively affects calcium homeostasis and bone mass. Nature Med 15:674–681, 2009.
964. Schipani E, Karga H, Karaplis AC, Potts JT Jr, Kronenberg HM, Segre GV, Abou-Samra AB, Juppner H. Identical complementary deoxyribonucleic acids encode ahuman renal and bone parathyroid hormone (PTH)/PTH-related peptide receptor.Endocrinology 132: 2157–2165, 1993.
965. Schjoldager BT, Baldissera FG, Mortensen PE, Holst JJ, Christiansen J. Oxyntomodu-lin: a potential hormone from the distal gut. Pharmacokinetics and effects on gastricacid and insulin secretion in man. Eur J Clin Invest 18: 499–503, 1988.
966. Schmidt WE, Schenk S, Nustede R, Holst JJ, Folsch UR, Creutzfeldt W. Cholecysto-kinin is a negative regulator of gastric acid secretion and postprandial release ofgastrin in humans. Gastroenterology 107: 1610–1620, 1994.
967. Schmitz F, Goke MN, Otte JM, Schrader H, Reimann B, Kruse ML, Siegel EG, PetersJ, Herzig KH, Folsch UR, Schmidt WE. Cellular expression of CCK-A and CCK-B/gastrin receptors in human gastric mucosa. Regul Pept 102: 101–110, 2001.
968. Schmorl G. (Editor). Verhandlungen der Deutschen Pathologischen Gesellschaft. Jena:Gustav Fischer, 1909.
969. Schnoke M, Midura SB, Midura RJ. Parathyroid hormone suppresses osteoblastapoptosis by augmenting DNA repair. Bone 45: 590–602, 2009.
970. Schoeber JP, Topala CN, Wang X, Diepens RJ, Lambers TT, Hoenderop JG, BindelsRJ. RGS2 inhibits the epithelial Ca2� channel TRPV6. J Biol Chem 281: 29669–29674,2006.
971. Schoeber JPH, Topala CN, Lee KP, Lambers TT, Ricard G, Van Der Kemp AWCM,Huynen MA, Hoenderop JGJ, Bindels RJM. Identification of Nipsnap1 as a novelauxiliary protein inhibiting TRPV6 activity. Pflügers Arch 457: 91–101, 2008.
972. Schoen MS, Lindenbaum J, Roginsky MS, Holt PR. Significance of serum level of25-hydroxycholecalciferol in gastrointestinal disease. Am J Dig Dis 23: 137–142,1978.
973. Schofield GC, Ito S, Bolender RP. Changes in membrane surface areas in mouseparietal cells in relation to high levels of acid secretion. J Anat 128: 669–692, 1979.
974. Scholz D, Schwille PO, Schley HW, Hanisch E, Bieger D, Zeuner E, Engelhardt W.Mineral metabolism and vitamin D status before and up to five years following highlyselective vagotomy in duodenal ulcer patients. Hepatogastroenterology 30: 102–106,1983.
975. Schubert ML, Edwards NF, Makhlouf GM. Regulation of gastric somatostatin secre-tion in the mouse by luminal acidity: a local feedback mechanism. Gastroenterology94: 317–322, 1988.
976. Schubert ML, Jong MJ, Makhlouf GM. Bombesin/GRP-stimulated somatostatin se-cretion is mediated by gastrin in the antrum and intrinsic neurons in the fundus. AmJ Physiol Gastrointest Liver Physiol 261: G885–G889, 1991.
977. Schubert ML, Makhlouf GM. Gastrin secretion induced by distention is mediated bygastric cholinergic and vasoactive intestinal peptide neurons in rats. Gastroenterology104: 834–839, 1993.
978. Schubert ML, Saffouri B, Walsh JH, Makhlouf GM. Inhibition of neurally mediatedgastrin secretion by bombesin antiserum. Am J Physiol Gastrointest Liver Physiol 248:G456–G462, 1985.
979. Schuessler M, Astecker N, Herzig G, Vorisek G, Schuster I. Skin is an autonomousorgan in synthesis, two-step activation and degradation of vitamin D(3): CYP27 inepidermis completes the set of essential vitamin D(3)-hydroxylases. Steroids 66:399–408, 2001.
980. Schulak JA, Kaplan EL. Gastrin-induced hypocalcemia in thyroparathyroidectomizedrats. Metabolism 23: 1103–1106, 1974.
981. Schulak JA, Kaplan EL. The importance of the stomach in gastrin-induced hypocal-cemia in the rat. Endocrinology 96: 1217–1220, 1975.
982. Schusdziarra V, Harris V, Conlon JM, Arimura A, Unger R. Pancreatic and gastricsomatostatin release in response to intragastric and intraduodenal nutrients and HClin the dog. J Clin Invest 62: 509–518, 1978.
983. Schwab M, Klotz U, Hofmann U, Schaeffeler E, Leodolter A, Malfertheiner P,Treiber G. Esomeprazole-induced healing of gastroesophageal reflux disease is un-related to the genotype of CYP2C19: evidence from clinical and pharmacokineticdata. Clin Pharmacol Ther 78: 627–634, 2005.
984. Schwartz GG, Wang MH, Zang M, Singh RK, Siegal GP. 1�,25-Dihydroxyvitamin D(calcitriol) inhibits the invasiveness of human prostate cancer cells. Cancer EpidemiolBiomarkers Prev 6: 727–732, 1997.
985. Seal A, Liu E, Buchan A, Brown J. Immunoneutralization of somatostatin and neuro-tensin: effect on gastric acid secretion. Am J Physiol Gastrointest Liver Physiol 255:G40–G45, 1988.
986. Segawa H, Kaneko I, Takahashi A, Kuwahata M, Ito M, Ohkido I, Tatsumi S, Miy-amoto K. Growth-related renal type II Na/Pi cotransporter. J Biol Chem 277: 19665–19672, 2002.
987. Segawa H, Yamanaka S, Onitsuka A, Tomoe Y, Kuwahata M, Ito M, Taketani Y,Miyamoto K. Parathyroid hormone-dependent endocytosis of renal type IIc Na-Pi
cotransporter. Am J Physiol Renal Physiol 292: F395–F403, 2007.
988. Segev H, Honigman A, Rosen H, Leitersdorf E. Transcriptional regulation of thehuman sterol 27-hydroxylase gene (CYP27) and promoter mapping. Atherosclerosis156: 339–347, 2001.
989. Segre GV, D’Amour P, Hultman A, Potts JT Jr. Effects of hepatectomy, nephrec-tomy, nephrectomy/uremia on the metabolism of parathyroid hormone in the rat. JClin Invest 67: 439–448, 1981.
990. Selye H. Anesthetic effect of steroid hormones. Proc Soc Exp Biol Med 46: 116, 1941.
991. Serfaty-Lacrosniere C, Wood RJ, Voytko D, Saltzman JR, Pedrosa M, Sepe TE,Russell RR. Hypochlorhydria from short-term omeprazole treatment does not in-hibit intestinal absorption of calcium, phosphorus, magnesium or zinc from food inhumans. J Am Coll Nutr 14: 364–368, 1995.
992. Seroussi E, Pan HQ, Kedra D, Roe BA, Dumanski JP. Characterization of the humanNIPSNAP1 gene from 22q12: a member of a novel gene family. Gene 212: 13–20,1998.
993. Setoguchi T, Salen G, Tint GS, Mosbach EH. A biochemical abnormality in cerebro-tendinous xanthomatosis. Impairment of bile acid biosynthesis associated with in-complete degradation of the cholesterol side chain. J Clin Invest 53: 1393–1401,1974.
994. Seva C, Dickinson CJ, Yamada T. Growth-promoting effects of glycine-extendedprogastrin. Science 265: 410–412, 1994.
995. Shareghi GR, Stoner LC. Calcium transport across segments of the rabbit distalnephron in vitro. Am J Physiol Renal Fluid Electrolyte Physiol 235: F367–F375, 1978.
996. Sheikh MS, Ramirez A, Emmett M, Santa Ana C, Schiller LR, Fordtran JS. Role ofvitamin D-dependent and vitamin D-independent mechanisms in absorption of foodcalcium. J Clin Invest 81: 126–132, 1988.
997. Sheikh MS, Santa Ana CA, Nicar MJ, Schiller LR, Fordtran JS. Gastrointestinal ab-sorption of calcium from milk and calcium salts. N Engl J Med 317: 532–536, 1987.
998. Sheinin Y, Kallay E, Wrba F, Kriwanek S, Peterlik M, Cross HS. Immunocytochemicallocalization of the extracellular calcium-sensing receptor in normal and malignanthuman large intestinal mucosa. J Histochem Cytochem 48: 595–602, 2000.
999. Shen L, Weber CR, Raleigh DR, Yu D, Turner JR. Tight junction pore and leakpathways: a dynamic duo. Annu Rev Physiol 73: 283–309, 2011.
SASCHA KOPIC AND JOHN P. GEIBEL
262 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

1000. Shen LP, Pictet RL, Rutter WJ. Human somatostatin I: sequence of the cDNA. ProcNatl Acad Sci USA 79: 4575–4579, 1982.
1001. Sherry AM, Malinowska DH, Morris RE, Ciraolo GM, Cuppoletti J. Localization ofClC-2 Cl� channels in rabbit gastric mucosa. Am J Physiol Cell Physiol 280: C1599–C1606, 2001.
1002. Shibata N, Matsui H, Yokota T, Matsuura B, Maeyama K, Onji M. Direct effects ofnitric oxide on histamine release from rat enterochromaffin-like cells. Eur J Pharmacol535: 25–33, 2006.
1003. Shimizu T, Yoshitomi K, Nakamura M, Imai M. Effects of PTH, calcitonin, cAMP oncalcium transport in rabbit distal nephron segments. Am J Physiol Renal Fluid Electro-lyte Physiol 259: F408–F414, 1990.
1004. Shimoi K, Saka N, Nozawa R, Sato M, Amano I, Nakayama T, Kinae N. Deglucuroni-dation of a flavonoid, luteolin monoglucuronide, during inflammation. Drug MetabDispos 29: 1521–1524, 2001.
1005. Shin JM, Besancon M, Prinz C, Simon A, Sachs G. Continuing development of acidpump inhibitors: site of action of pantoprazole. Aliment Pharmacol Ther 8 Suppl 1:11–23, 1994.
1006. Shin JM, Besancon M, Simon A, Sachs G. The site of action of pantoprazole in thegastric H�/K�-ATPase. Biochim Biophys Acta 1148: 223–233, 1993.
1007. Shin JM, Cho YM, Sachs G. Chemistry of covalent inhibition of the gastric (H�,K�)-ATPase by proton pump inhibitors. J Am Chem Soc 126: 7800–7811, 2004.
1008. Shin JM, Homerin M, Domagala F, Ficheux H, Sachs G. Characterization of theinhibitory activity of tenatoprazole on the gastric H�,K�-ATPase in vitro and in vivo.Biochem Pharmacol 71: 837–849, 2006.
1009. Shinki T, Ueno Y, DeLuca HF, Suda T. Calcitonin is a major regulator for theexpression of renal 25-hydroxyvitamin D3-1alpha-hydroxylase gene in normocalce-mic rats. Proc Natl Acad Sci USA 96: 8253–8258, 1999.
1010. Shoback DM, Membreno LA, McGhee JG. High calcium and other divalent cationsincrease inositol trisphosphate in bovine parathyroid cells. Endocrinology 123: 382–389, 1988.
1011. Shulkes A, Read M. Regulation of somatostatin secretion by gastrin- and acid-depen-dent mechanisms. Endocrinology 129: 2329–2334, 1991.
1012. Shyjan AW, Canfield VA, Levenson R. Evolution of the Na,K- and H�-K�-ATPasebeta subunit gene family: structure of the murine Na�-K�-ATPase beta 2 subunitgene. Genomics 11: 435–442, 1991.
1013. Sidani SM, Kirchhoff P, Socrates T, Stelter L, Ferreira E, Caputo C, Roberts KE, BellRL, Egan ME, Geibel JP. DeltaF508 mutation results in impaired gastric acid secre-tion. J Biol Chem 282: 6068–6074, 2007.
1014. Silve C, Petrel C, Leroy C, Bruel H, Mallet E, Rognan D, Ruat M. Delineating a Ca2�
binding pocket within the venus flytrap module of the human calcium-sensing recep-tor. J Biol Chem 280: 37917–37923, 2005.
1015. Silver J, Fainaru M. Transport of vitamin D sterols in human plasma: effect of excessvitamin D, 25 hydroxyvitamin D and 1,25 dihydroxyvitamin D. Eur J Clin Invest 9:433–438, 1979.
1016. Singer FR, Foster GV, Jpolin GF, Nadarajah A, Parkinson DK, Thalassinos N, Wood-house NJ, Clark MB, Fraser TR, MacIntyre I. Acute effects of administered calcitoninin man. Calcif Tissue Res Suppl: 20, 1968.
1017. Singh P, Velasco M, Given R, Varro A, Wang TC. Progastrin expression predisposesmice to colon carcinomas and adenomas in response to a chemical carcinogen.Gastroenterology 119: 162–171, 2000.
1018. Sitrin MD, Bengoa JM. Intestinal absorption of cholecalciferol and 25-hydroxychole-calciferol in chronic cholestatic liver disease. Am J Clin Nutr 46: 1011–1015, 1987.
1019. Sitrin MD, Pollack KL, Bolt MJ, Rosenberg IH. Comparison of vitamin D and 25-hydroxyvitamin D absorption in the rat. Am J Physiol Gastrointest Liver Physiol 242:G326–G332, 1982.
1020. Sizemore GW, Go VL, Kaplan EL, Sanzenbacher LJ, Holtermuller KH, Arnaud CD.Relations of calcitonin and gastrin in the Zollinger-Ellison syndrome and medullarycarcinoma of the thyroid. N Engl J Med 288: 641–644, 1973.
1021. Slepchenko BM, Bronner F. Modeling of transcellular Ca transport in rat duodenumpoints to coexistence of two mechanisms of apical entry. Am J Physiol Cell Physiol 281:C270–C281, 2001.
1022. Sneddon WB, Syme CA, Bisello A, Magyar CE, Rochdi MD, Parent JL, Weinman EJ,Abou-Samra AB, Friedman PA. Activation-independent parathyroid hormone re-ceptor internalization is regulated by NHERF1 (EBP50). J Biol Chem 278: 43787–43796, 2003.
1023. Soejima M, Tachida H, Koda Y. Sequence analysis of human TRPV6 suggests positiveselection outside Africa. Biochem Genet 47: 147–153, 2009.
1024. Soll AH. The interaction of histamine with gastrin and carbamylcholine on oxygenuptake by isolated mammalian parietal cells. J Clin Invest 61: 381–389, 1978.
1025. Soll AH. Potentiating interactions of gastric stimulants on [14C]aminopyrine accu-mulation by isolated canine parietal cells. Gastroenterology 83: 216–223, 1982.
1026. Soll AH, Wollin A. Histamine and cyclic AMP in isolated canine parietal cells. Am JPhysiol Endocrinol Metab Gastrointest Physiol 237: E444–E450, 1979.
1027. Sone T, Kerner S, Pike JW. Vitamin D receptor interaction with specific DNA.Association as a 1,25-dihydroxyvitamin D3-modulated heterodimer. J Biol Chem 266:23296–23305, 1991.
1028. Song P, Groos S, Riederer B, Feng Z, Krabbenhoft A, Manns MP, Smolka A, Hagen SJ,Neusch C, Seidler U. Kir4.1 channel expression is essential for parietal cell control ofacid secretion. J Biol Chem 286: 14120–14128, 2011.
1029. Song P, Groos S, Riederer B, Feng Z, Krabbenhoft A, Smolka A, Seidler U. KCNQ1is the luminal K� recycling channel during stimulation of gastric acid secretion. JPhysiol 587: 3955–3965, 2009.
1030. Song Y, Peng X, Porta A, Takanaga H, Peng JB, Hediger MA, Fleet JC, Christakos S.Calcium transporter 1 and epithelial calcium channel messenger ribonucleic acid aredifferentially regulated by 1,25 dihydroxyvitamin D3 in the intestine and kidney ofmice. Endocrinology 144: 3885–3894, 2003.
1031. Sopjani M, Kunert A, Czarkowski K, Klaus F, Laufer J, Föller M, Lang F. Regulation ofthe Ca2� Channel TRPV6 by the Kinases SGK1, PKB/Akt, and PIKfyve. J Membr Biol233: 35–41, 2010.
1032. Sowa H, Kaji H, Iu MF, Tsukamoto T, Sugimoto T, Chihara K. Parathyroid hormone-SmaD3 axis exerts anti-apoptotic action and augments anabolic action of transform-ing growth factor beta in osteoblasts. J Biol Chem 278: 52240–52252, 2003.
1033. St-Arnaud R. The direct role of vitamin D on bone homeostasis. Arch Biochem Biophys473: 225–230, 2008.
1034. St-Arnaud R, Messerlian S, Moir JM, Omdahl JL, Glorieux FH. The 25-hydroxyvita-min D 1-alpha-hydroxylase gene maps to the pseudovitamin D-deficiency rickets(PDDR) disease locus. J Bone Miner Res 12: 1552–1559, 1997.
1035. Stamp TC, Round JM. Seasonal changes in human plasma levels of 25-hydroxyvitaminD. Nature 247: 563–565, 1974.
1036. Stedman CA, Barclay ML. Review article: comparison of the pharmacokinetics, acidsuppression and efficacy of proton pump inhibitors. Aliment Pharmacol Ther 14:963–978, 2000.
1037. Steenbock H, Black A. Fat-soluble vitamins. XVII. The induction of growth-promot-ing and calcifying properties in a ration by exposure to ultra-violet light. J Biol Chem61: 405–422, 1924.
1038. Steggerda FR, Mitchell HH. The effect of the citrate ion on the calcium metabolismof adult human subjects. J Nutr 31: 423–438, 1946.
1039. Stepan V, Pausawasdi N, Ramamoorthy S, Todisco A. The Akt and MAPK signal-transduction pathways regulate growth factor actions in isolated gastric parietal cells.Gastroenterology 127: 1150–1161, 2004.
1040. Stepan V, Sugano K, Yamada T, Park J, Dickinson CJ. Gastrin biosynthesis in canine Gcells. Am J Physiol Gastrointest Liver Physiol 282: G766–G775, 2002.
1041. Sternfeld L, Anderie I, Schmid A, Al-Shaldi H, Krause E, Magg T, Schreiner D, HoferHW, Schulz I. Identification of tyrosines in the putative regulatory site of the Ca2�
channel TRPV6. Cell Calcium 42: 91–102, 2007.
1042. Sternfeld L, Krause E, Schmid A, Anderie I, Latas A, Al-Shaldi H, Kohl A, Evers K,Hofer HW, Schulz I. Tyrosine phosphatase PTP1B interacts with TRPV6 in vivo and
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
263Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

plays a role in TRPV6-mediated calcium influx in HEK293 cells. Cell Signal 17: 951–960, 2005.
1043. Strehler EE, Zacharias DA. Role of alternative splicing in generating isoform diversityamong plasma membrane calcium pumps. Physiol Rev 81: 21–50, 2001.
1044. Strong TV, Boehm K, Collins FS. Localization of cystic fibrosis transmembrane con-ductance regulator mRNA in the human gastrointestinal tract by in situ hybridization.J Clin Invest 93: 347–354, 1994.
1045. Strushkevich N, Usanov SA, Plotnikov AN, Jones G, Park HW. Structural analysis ofCYP2R1 in complex with vitamin D3. J Mol Biol 380: 95–106, 2008.
1046. Stumpf T, Zhang Q, Hirnet D, Lewandrowski U, Sickmann A, Wissenbach U, DorrJ, Lohr C, Deitmer JW, Fecher-Trost C. The human TRPV6 channel protein isassociated with cyclophilin B in human placenta. J Biol Chem 283: 18086–18098,2008.
1047. Su HC, Bishop AE, Power RF, Hamada Y, Polak JM. Dual intrinsic and extrinsicorigins of CGRP- and NPY-immunoreactive nerves of rat gut and pancreas. J Neu-rosci 7: 2674–2687, 1987.
1048. Su P, Rennert H, Shayiq RM, Yamamoto R, Zheng YM, Addya S, Strauss JF 3rd,Avadhani NG. A cDNA encoding a rat mitochondrial cytochrome P450 catalyzingboth the 26-hydroxylation of cholesterol and 25-hydroxylation of vitamin D3: go-nadotropic regulation of the cognate mRNA in ovaries. DNA Cell Biol 9: 657–667,1990.
1049. Suda J, Zhu L, Okamoto CT, Karvar S. Rab27b localizes to the tubulovesicle mem-branes of gastric parietal cells and regulates acid secretion. Gastroenterology 140:868–878, 2011.
1050. Sudo Y, Matsuo K, Tetsuo T, Tsutsumi S, Ohkura M, Nakai J, Uezono Y. Derived(mutated)-types of TRPV6 channels elicit greater Ca2� influx into the cells thanancestral-types of TRPV6: evidence from Xenopus oocytes and mammalian cell ex-pression system. J Pharmacol Sci 114: 281–291, 2010.
1051. Sugano K, Park J, Dobbins WO, Yamada T. Glycine-extended progastrin processingintermediates: accumulation and cosecretion with gastrin. Am J Physiol GastrointestLiver Physiol 253: G502–G507, 1987.
1052. Suki WN, Eknoyan G, Rector FC Jr, Seldin DW. The renal diluting and concentratingmechanism in hypercalcemia. Nephron 6: 50–61, 1969.
1053. Sulimovici S, Roginsky MS, Duffy JL, Pfeifer RF. Calciferol 25-hydroxylase activity insmooth and rough endoplasmic reticulum of rat liver. Arch Biochem Biophys 195:45–52, 1979.
1054. Sundler F, Ekblad E, Absood A, Hakanson R, Koves K, Arimura A. Pituitary adenylatecyclase activating peptide: a novel vasoactive intestinal peptide-like neuropeptide inthe gut. Neuroscience 46: 439–454, 1992.
1055. Sunthornthepvarakul T, Churesigaew S, Ngowngarmratana S. A novel mutation ofthe signal peptide of the preproparathyroid hormone gene associated with auto-somal recessive familial isolated hypoparathyroidism. J Clin Endocrinol Metab 84:3792–3796, 1999.
1056. Suva LJ, Winslow GA, Wettenhall RE, Hammonds RG, Moseley JM, Diefenbach-Jagger H, Rodda CP, Kemp BE, Rodriguez H, Chen EY. A parathyroid hormone-related protein implicated in malignant hypercalcemia: cloning and expression. Sci-ence 237: 893–896, 1987.
1057. Suzuki H, Nakamura I, Takahashi N, Ikuhara T, Matsuzaki K, Isogai Y, Hori M, SudaT. Calcitonin-induced changes in the cytoskeleton are mediated by a signal pathwayassociated with protein kinase A in osteoclasts. Endocrinology 137: 4685–4690, 1996.
1058. Suzuki M, Ishibashi K, Ooki G, Tsuruoka S, Imai M. Electrophysiologic characteristicsof the Ca-permeable channels, ECaC and CaT, in the kidney. Biochem Biophys ResCommun 274: 344–349, 2000.
1059. Tache Y, Saperas E. Potent inhibition of gastric acid secretion and ulcer formation bycentrally and peripherally administered interleukin-1. Ann NY Acad Sci 664: 353–368,1992.
1060. Takahashi N, Yamana H, Yoshiki S, Roodman GD, Mundy GR, Jones SJ, Boyde A,Suda T. Osteoclast-like cell formation and its regulation by osteotropic hormones inmouse bone marrow cultures. Endocrinology 122: 1373–1382, 1988.
1061. Takahashi S, Goldring S, Katz M, Hilsenbeck S, Williams R, Roodman GD. Down-regulation of calcitonin receptor mRNA expression by calcitonin during human os-teoclast-like cell differentiation. J Clin Invest 95: 167–171, 1995.
1062. Takeuchi Y, Pausawasdi N, Todisco A. Carbachol activates ERK2 in isolated gastricparietal cells via multiple signaling pathways. Am J Physiol Gastrointest Liver Physiol276: G1484–G1492, 1999.
1063. Takeuchi Y, Yamada J, Yamada T, Todisco A. Functional role of extracellular signal-regulated protein kinases in gastric acid secretion. Am J Physiol Gastrointest LiverPhysiol 273: G1263–G1272, 1997.
1064. Talmage RV, Neuenschwander J, Kraintz L. Evidence for the existence of thyrocal-citonin in the rat. Endocrinology 76: 103–107, 1965.
1065. Tam CS, Heersche JN, Murray TM, Parsons JA. Parathyroid hormone stimulates thebone apposition rate independently of its resorptive action: differential effects ofintermittent and continuous administration. Endocrinology 110: 506–512, 1982.
1066. Tanaka S, Hamada K, Yamada N, Sugita Y, Tonai S, Hunyady B, Palkovits M, Falus A,Watanabe T, Okabe S, Ohtsu H, Ichikawa A, Nagy A. Gastric acid secretion inL-histidine decarboxylase-deficient mice. Gastroenterology 122: 145–155, 2002.
1067. Tanaka Y, Castillo L, Wineland MJ, DeLuca HF. Synergistic effect of progesterone,testosterone, estradiol in the stimulation of chick renal 25-hydroxyvitamin D3-1al-pha-hydroxylase. Endocrinology 103: 2035–2039, 1978.
1068. Tanaka Y, Deluca HF. The control of 25-hydroxyvitamin D metabolism by inorganicphosphorus. Arch Biochem Biophys 154: 566–574, 1973.
1069. Tanaka Y, DeLuca HF. Measurement of mammalian 25-hydroxyvitamin D3 24R-and1 alpha-hydroxylase. Proc Natl Acad Sci USA 78: 196–199, 1981.
1070. Tang LH, Stoch SA, Modlin IM, Goldenring JR. Identification of rab2 as a tubulo-vesicle-membrane-associated protein in rabbit gastric parietal cells. Biochem J 285:715–719, 1992.
1071. Tanrattana C, Charoenphandhu N, Limlomwongse L, Krishnamra N. Prolactin di-rectly stimulated the solvent drag-induced calcium transport in the duodenum offemale rats. Biochim Biophys Acta 1665: 81–91, 2004.
1072. Tatemoto K, Efendic S, Mutt V, Makk G, Feistner GJ, Barchas JD. Pancreastatin,a novel pancreatic peptide that inhibits insulin secretion. Nature 324: 476 – 478,1986.
1073. Taylor AN, Wasserman RH. Vitamin D3-induced calcium-binding protein: partialpurification, electrophoretic visualization, and tissue distribution. Arch Biochem Bio-phys 119: 536–540, 1967.
1074. Taylor IL, Byrne WJ, Christie DL, Ament ME, Walsh JH. Effect of individual L-aminoacids on gastric acid secretion and serum gastrin and pancreatic polypeptide releasein humans. Gastroenterology 83: 273–278, 1982.
1075. Taylor IL, Sells RA, McConnell RB, Dockray GJ. Serum gastrin in patients withchronic renal failure. Gut 21: 1062–1067, 1980.
1076. Teranishi H, Kasuya M, Aoshima K, Kato T, Migita S. Demonstration of vitaminD-binding protein (Gc-globulin) in the urine of Itai-itai disease patients. Toxicol Lett15: 7–12, 1983.
1077. Thamsborg G, Jensen JE, Kollerup G, Hauge EM, Melsen F, Sorensen OH. Effect ofnasal salmon calcitonin on bone remodeling and bone mass in postmenopausal os-teoporosis. Bone 18: 207–212, 1996.
1078. Theodoropoulos C, Demers C, Petit JL, Gascon-Barre M. High sensitivity of rathepatic vitamin D3-25 hydroxylase CYP27A to 1,25-dihydroxyvitamin D3 adminis-tration. Am J Physiol Endocrinol Metab 284: E138–E147, 2003.
1079. Thomas WC Jr, Morgan HG, Connor TB, Haddock L, Bills CE, Howard JE. Studies ofantiricketic activity in sera from patients with disorders of calcium metabolism andpreliminary observations on the mode of transport of vitamin D in human serum. JClin Invest 38: 1078–1085, 1959.
1080. Thompson GR, Lewis B, Booth CC. Absorption of vitamin D3-3H in control subjectsand patients with intestinal malabsorption. J Clin Invest 45: 94–102, 1966.
1081. Thompson GR, Lewis B, Booth CC. Vitamin-D absorption after partial gastrectomy.Lancet 1: 457–458, 1966.
SASCHA KOPIC AND JOHN P. GEIBEL
264 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

1082. Thompson GR, Ockner RK, Isselbacher KJ. Effect of mixed micellar lipid on theabsorption of cholesterol and vitamin D3 into lymph. J Clin Invest 48: 87–95, 1969.
1083. Thompson PD, Jurutka PW, Haussler CA, Whitfield GK, Haussler MR. Heterodi-meric DNA binding by the vitamin D receptor and retinoid X receptors is enhancedby 1,25-dihydroxyvitamin D3 and inhibited by 9-cis-retinoic acid. Evidence for allo-steric receptor interactions. J Biol Chem 273: 8483–8491, 1998.
1084. Thunberg R. Localization of cells containing and forming histamine in the gastricmucosa of the rat. Exp Cell Res 47: 108–115, 1967.
1085. Tian XQ, Chen TC, Matsuoka LY, Wortsman J, Holick MF. Kinetic and thermody-namic studies of the conversion of previtamin D3 to vitamin D3 in human skin. J BiolChem 268: 14888–14892, 1993.
1086. Tian XQ, Holick MF. A liposomal model that mimics the cutaneous production ofvitamin D3. Studies of the mechanism of the membrane-enhanced thermal isomer-ization of previtamin D3 to vitamin D3. J Biol Chem 274: 4174–4179, 1999.
1087. Tinel N, Diochot S, Borsotto M, Lazdunski M, Barhanin J. KCNE2 confers back-ground current characteristics to the cardiac KCNQ1 potassium channel. EMBO J19: 6326–6330, 2000.
1088. Tishkoff DX, Nibbelink KA, Holmberg KH, Dandu L, Simpson RU. Functional vita-min D receptor (VDR) in the t-tubules of cardiac myocytes: VDR knockout cardio-myocyte contractility. Endocrinology 149: 558–564, 2008.
1089. Tondapu P, Provost D, Adams-Huet B, Sims T, Chang C, Sakhaee K. Comparison ofthe absorption of calcium carbonate and calcium citrate after Roux-en-Y gastricbypass. Obes Surg 19: 1256–1261, 2009.
1090. Topala CN, Schoeber JP, Searchfield LE, Riccardi D, Hoenderop JG, Bindels RJ.Activation of the Ca2�-sensing receptor stimulates the activity of the epithelial Ca2�
channel TRPV5. Cell Calcium 45: 331–339, 2009.
1091. Tovey FI, Karamanolis DG, Godfrey J, Clark CG. Post-gastrectomy nutrition: meth-ods of outpatient screening for early osteomalacia. Hum Nutr Clin Nutr 39: 439–446,1985.
1092. Toyoshima C, Nomura H. Structural changes in the calcium pump accompanying thedissociation of calcium. Nature 418: 605–611, 2002.
1093. Toyoshima C, Nomura H, Sugita Y. Crystal structures of Ca2�-ATPase in variousphysiological states. Ann NY Acad Sci 986: 1–8, 2003.
1094. Tregear GW, Van Rietschoten J, Greene E, Keutmann HT, Niall HD, Reit B, ParsonsJA, Potts JT Jr. Bovine parathyroid hormone: minimum chain length of syntheticpeptide required for biological activity. Endocrinology 93: 1349–1353, 1973.
1095. Tsunoda Y, Funasaka M, Modlin IM, Hidaka H, Fox LM, Goldenring JR. An inhibitorof Ca2�/calmodulin-dependent protein kinase II, KN-62, inhibits cholinergic-stimu-lated parietal cell secretion. Am J Physiol Gastrointest Liver Physiol 262: G118–G122,1992.
1096. Tu Q, Pi M, Karsenty G, Simpson L, Liu S, Quarles LD. Rescue of the skeletalphenotype in CasR-deficient mice by transfer onto the Gcm2 null background. J ClinInvest 111: 1029–1037, 2003.
1097. Tucker G 3rd, Gagnon RE, Haussler MR. Vitamin D3-25-hydroxylase: tissue occur-rence and apparent lack of regulation. Arch Biochem Biophys 155: 47–57, 1973.
1098. Tudpor K, Teerapornpuntakit J, Jantarajit W, Krishnamra N, Charoenphandhu N.1,25-Dihydroxyvitamin D(3) rapidly stimulates the solvent drag-induced paracellularcalcium transport in the duodenum of female rats. J Physiol Sci 58: 297–307, 2008.
1099. Tzaneva MA. Ultrastructural immunohistochemical localization of gastrin, soma-tostatin and serotonin in endocrine cells of human antral gastric mucosa. Acta His-tochem 105: 191–201, 2003.
1100. Uchida M, Teranishi H, Aoshima K, Katoh T, Kasuya M, Inadera H. Elevated urinarylevels of vitamin D-binding protein in the inhabitants of a cadmium polluted area,Jinzu River basin, Japan. Tohoku J Exp Med 211: 269–274, 2007.
1101. Uehara A, Okumura T, Sekiya C, Okamura K, Takasugi Y, Namiki M. Interleukin-1inhibits the secretion of gastric acid in rats: possible involvement of prostaglandin.Biochem Biophys Res Commun 162: 1578–1584, 1989.
1102. Usatii M, Rousseau L, Demers C, Petit JL, Brossard JH, Gascon-Barre M, Lavigne JR,Zahradnik RJ, Nemeth EF, D’Amour P. Parathyroid hormone fragments inhibit ac-
tive hormone and hypocalcemia-induced 1,25(OH)2D synthesis. Kidney Int 72:1330–1335, 2007.
1103. Usui E, Noshiro M, Okuda K. Molecular cloning of cDNA for vitamin D3 25-hydrox-ylase from rat liver mitochondria. FEBS Lett 262: 135–138, 1990.
1104. Vagin O, Denevich S, Munson K, Sachs G. SCH28080, a K�-competitive inhibitor ofthe gastric H�-K�-ATPase, binds near the M5–6 luminal loop, preventing K� accessto the ion binding domain. Biochemistry 41: 12755–12762, 2002.
1105. Vagin O, Denevich S, Sachs G. Plasma membrane delivery of the gastric H�-K�-ATPase: the role of beta-subunit glycosylation. Am J Physiol Cell Physiol 285: C968–C976, 2003.
1106. Vagin O, Munson K, Lambrecht N, Karlish SJ, Sachs G. Mutational analysis of theK�-competitive inhibitor site of gastric H�-K�-ATPase. Biochemistry 40: 7480–7490, 2001.
1107. Vagne M, Andre C. The effect of secretin on gastric emptying in man. Gastroenter-ology 60: 421–424, 1971.
1108. Van Abel M, Hoenderop JG, van der Kemp AW, Friedlaender MM, van Leeuwen JP,Bindels RJ. Coordinated control of renal Ca2� transport proteins by parathyroidhormone. Kidney Int 68: 1708–1721, 2005.
1109. Van Abel M, Hoenderop JG, van der Kemp AW, van Leeuwen JP, Bindels RJ. Regu-lation of the epithelial Ca2� channels in small intestine as studied by quantitativemRNA detection. Am J Physiol Gastrointest Liver Physiol 285: G78–G85, 2003.
1110. Van Cromphaut SJ, Dewerchin M, Hoenderop JG, Stockmans I, Van Herck E, Kato S,Bindels RJ, Collen D, Carmeliet P, Bouillon R, Carmeliet G. Duodenal calcium ab-sorption in vitamin D receptor-knockout mice: functional and molecular aspects.Proc Natl Acad Sci USA 98: 13324–13329, 2001.
1111. Van de Graaf SF, Chang Q, Mensenkamp AR, Hoenderop JG, Bindels RJ. Directinteraction with Rab11a targets the epithelial Ca2� channels TRPV5 and TRPV6 tothe plasma membrane. Mol Cell Biol 26: 303–312, 2006.
1112. Van de Graaf SF, Hoenderop JG, Gkika D, Lamers D, Prenen J, Rescher U, Gerke V,Staub O, Nilius B, Bindels RJ. Functional expression of the epithelial Ca2� channels(TRPV5 and TRPV6) requires association of the S100A10-annexin 2 complex. EMBOJ 22: 1478–1487, 2003.
1113. Van de Graaf SF, Hoenderop JG, van der Kemp AW, Gisler SM, Bindels RJ. Interac-tion of the epithelial Ca2� channels TRPV5 and TRPV6 with the intestine- andkidney-enriched PDZ protein NHERF4. Pflügers Arch 452: 407–417, 2006.
1114. Van Leeuwen JP, van Driel M, van den Bemd GJ, Pols HA. Vitamin D control ofosteoblast function and bone extracellular matrix mineralization. Crit Rev EukaryotGene Expr 11: 199–226, 2001.
1115. Varrault A, Pena MS, Goldsmith PK, Mithal A, Brown EM, Spiegel AM. Expression ofG protein alpha-subunits in bovine parathyroid. Endocrinology 136: 4390–4396,1995.
1116. Varro A, Green T, Holmes S, Dockray GJ. Calcitonin gene-related peptide in visceralafferent nerve fibres: quantification by radioimmunoassay and determination of ax-onal transport rates. Neuroscience 26: 927–932, 1988.
1117. Velluz L, Amirad G. Chimie organique-equilibre de reaction entre precalciferol etcalciferol. Compt Rend Assoc Anat 288: 853–855, 1949.
1118. Velluz L, Amirad G. Chimie organique-le precalciferol. Compt Rend Assoc Anat 228:692–694, 1949.
1119. Velluz L, Amirad G. Chimie organique-nouveau precursor de la vitamine D3. ComptRend Assoc Anat 228: 1037–1038, 1949.
1120. Velluz L, Amirad G, Petit A. Le precalciferol: ses relations d’equilibre avec le calcif-erol. Bull Soc Chim France 16: 501–507, 1949.
1121. Verboven C, Rabijns A, De Maeyer M, Van Baelen H, Bouillon R, De Ranter C. Astructural basis for the unique binding features of the human vitamin D-bindingprotein. Nat Struct Biol 9: 131–136, 2002.
1122. Vertino AM, Bula CM, Chen JR, Almeida M, Han L, Bellido T, Kousteni S, NormanAW, Manolagas SC. Nongenotropic, anti-apoptotic signaling of 1alpha,25(OH)2-vitamin D3 and analogs through the ligand binding domain of the vitamin D receptorin osteoblasts and osteocytes. Mediation by Src, phosphatidylinositol 3-, and JNKkinases. J Biol Chem 280: 14130–14137, 2005.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
265Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

1123. Vilardaga JP, Krasel C, Chauvin S, Bambino T, Lohse MJ, Nissenson RA. Internaliza-tion determinants of the parathyroid hormone receptor differentially regulate beta-arrestin/receptor association. J Biol Chem 277: 8121–8129, 2002.
1124. Villa-Bellosta R, Ravera S, Sorribas V, Stange G, Levi M, Murer H, Biber J, Forster IC.The Na�-Pi cotransporter PiT-2 (SLC20A2) is expressed in the apical membrane ofrat renal proximal tubules and regulated by dietary Pi. Am J Physiol Renal Physiol 296:F691–F699, 2009.
1125. Vinik AI, Gaginella TS, O’Dorisio TM, Shapiro B, Wagner L. The distribution andcharacterization of somatostatin-like immunoreactivity in epithelial cells, submu-cosa, muscle of the rat stomach and intestine. Endocrinology 109: 1921–1926, 1981.
1126. Voets T, Janssens A, Prenen J, Droogmans G, Nilius B. Mg2�-dependent gating andstrong inward rectification of the cation channel TRPV6. J Gen Physiol 121: 245–260,2003.
1127. Vogelsang H, Schofl R, Tillinger W, Ferenci P, Gangl A. 25-Hydroxyvitamin D ab-sorption in patients with Crohn’s disease and with pancreatic insufficiency. Wien KlinWochenschr 109: 678–682, 1997.
1128. Wada M, Furuya Y, Sakiyama J, Kobayashi N, Miyata S, Ishii H, Nagano N. Thecalcimimetic compound NPS R-568 suppresses parathyroid cell proliferation in ratswith renal insufficiency. Control of parathyroid cell growth via a calcium receptor. JClin Invest 100: 2977–2983, 1997.
1129. Wada S, Martin TJ, Findlay DM. Homologous regulation of the calcitonin receptor inmouse osteoclast-like cells and human breast cancer T47D cells. Endocrinology 136:2611–2621, 1995.
1130. Wada S, Udagawa N, Nagata N, Martin TJ, Findlay DM. Calcitonin receptor down-regulation relates to calcitonin resistance in mature mouse osteoclasts. Endocrinology137: 1042–1048, 1996.
1131. Waldum HL, Sandvik AK, Brenna E, Petersen H. Gastrin-histamine sequence in theregulation of gastric acid secretion. Gut 32: 698–701, 1991.
1132. Wallace JL, Cucala M, Mugridge K, Parente L. Secretagogue-specific effects of inter-leukin-1 on gastric acid secretion. Am J Physiol Gastrointest Liver Physiol 261: G559–G564, 1991.
1133. Walling MW, Rothman SS. Apparent increase in carrier affinity for intestinal calciumtransport following dietary calcium restriction. J Biol Chem 245: 5007–5011, 1970.
1134. Walling MW, Rothman SS. Phosphate-independent, carrier-mediated active trans-port of calcium by rat intestine. Am J Physiol 217: 1144–1148, 1969.
1135. Wallmark B, Brandstrom A, Larsson H. Evidence for acid-induced transformation ofomeprazole into an active inhibitor of (H� � K�)-ATPase within the parietal cell.Biochim Biophys Acta 778: 549–558, 1984.
1136. Walters JR. Calbindin-D9k stimulates the calcium pump in rat enterocyte basolateralmembranes. Am J Physiol Gastrointest Liver Physiol 256: G124–G128, 1989.
1137. Walters JR, Howard A, Charpin MV, Gniecko KC, Brodin P, Thulin E, Forsen S.Stimulation of intestinal basolateral membrane calcium-pump activity by recombi-nant synthetic calbindin-D9k and specific mutants. Biochem Biophys Res Commun170: 603–608, 1990.
1138. Walters JR, Howard A, Lowery LJ, Mawer EB, Legon S. Expression of genes involvedin calcium absorption in human duodenum. Eur J Clin Invest 29: 214–219, 1999.
1139. Wang B, Bisello A, Yang Y, Romero GG, Friedman PA. NHERF1 regulates parathy-roid hormone receptor membrane retention without affecting recycling. J Biol Chem282: 36214–36222, 2007.
1140. Wang B, Yang Y, Abou-Samra AB, Friedman PA. NHERF1 regulates parathyroidhormone receptor desensitization: interference with beta-arrestin binding. MolPharmacol 75: 1189–1197, 2009.
1141. Wang DH, Hu YS, Du JJ, Hu YY, Zhong WD, Qin WJ. Ghrelin stimulates proliferationof human osteoblastic TE85 cells via NO/cGMP signaling pathway. Endocrine 35:112–117, 2009.
1142. Wang L, Gantz I, DelValle J. Histamine H2 receptor activates adenylate cyclase andPLC via separate GTP-dependent pathways. Am J Physiol Gastrointest Liver Physiol271: G613–G620, 1996.
1143. Wang LD, Hoeltzel M, Gantz I, Hunter R, Del Valle J. Characterization of the hista-mine H2 receptor structural components involved in dual signaling. J Pharmacol ExpTher 285: 573–578, 1998.
1144. Wang Q, Curran ME, Splawski I, Burn TC, Millholland JM, VanRaay TJ, Shen J,Timothy KW, Vincent GM, de Jager T, Schwartz PJ, Toubin JA, Moss AJ, AtkinsonDL, Landes GM, Connors TD, Keating MT. Positional cloning of a novel potassiumchannel gene: KVLQT1 mutations cause cardiac arrhythmias. Nat Genet 12: 17–23,1996.
1145. Wang TC, Koh TJ, Varro A, Cahill RJ, Dangler CA, Fox JG, Dockray GJ. Processingand proliferative effects of human progastrin in transgenic mice. J Clin Invest 98:1918–1929, 1996.
1146. Wang TJ, Zhang F, Richards JB, Kestenbaum B, van Meurs JB, Berry D, Kiel DP, StreetenEA, Ohlsson C, Koller DL, Peltonen L, Cooper JD, O’Reilly PF, Houston DK, Glazer NL,Vandenput L, Peacock M, Shi J, Rivadeneira F, McCarthy MI, Anneli P, de Boer IH,Mangino M, Kato B, Smyth DJ, Booth SL, Jacques PF, Burke GL, Goodarzi M, CheungCL, Wolf M, Rice K, Goltzman D, Hidiroglou N, Ladouceur M, Wareham NJ, Hocking LJ,Hart D, Arden NK, Cooper C, Malik S, Fraser WD, Hartikainen AL, Zhai G, MacdonaldHM, Forouhi NG, Loos RJ, Reid DM, Hakim A, Dennison E, Liu Y, Power C, Stevens HE,Jaana L, Vasan RS, Soranzo N, Bojunga J, Psaty BM, Lorentzon M, Foroud T, Harris TB,Hofman A, Jansson JO, Cauley JA, Uitterlinden AG, Gibson Q, Jarvelin MR, Karasik D,Siscovick DS, Econs MJ, Kritchevsky SB, Florez JC, Todd JA, Dupuis J, Hypponen E,Spector TD. Common genetic determinants of vitamin D insufficiency: a genome-wide association study. Lancet 376: 180–188, 2010.
1147. Wang W, Lu M, Balazy M, Hebert SC. Phospholipase A2 is involved in mediating theeffect of extracellular Ca2� on apical K� channels in rat TAL. Am J Physiol RenalPhysiol 273: F421–F429, 1997.
1148. Wang WH, Lu M, Hebert SC. Cytochrome P-450 metabolites mediate extracellularCa2�-induced inhibition of apical K� channels in the TAL. Am J Physiol Cell Physiol271: C103–C111, 1996.
1149. Wasserman RH, Corradino RA, Taylor AN. Vitamin D-dependent calcium-bindingprotein. Purification and some properties. J Biol Chem 243: 3978–3986, 1968.
1150. Wasserman RH, Kallfelz FA, Comar CL. Active transport of calcium by rat duode-num in vivo. Science 133: 883–884, 1961.
1151. Wasserman RH, Taylor AN. Vitamin D3-induced calcium-binding protein in chickintestinal mucosa. Science 152: 791–793, 1966.
1152. Wasserman RH, Taylor AN. Vitamin D-dependent calcium-binding protein. Re-sponse to some physiological and nutritional variables. J Biol Chem 243: 3987–3993,1968.
1153. Watanabe S, Chey WY, Lee KY, Chang TM. Secretin is released by digestive prod-ucts of fat in dogs. Gastroenterology 90: 1008–1017, 1986.
1154. Watson F, Kiernan RS, Deavall DG, Varro A, Dimaline R. Transcriptional activation ofthe rat vesicular monoamine transporter 2 promoter in gastric epithelial cells: reg-ulation by gastrin. J Biol Chem 276: 7661–7671, 2001.
1155. Watson PH, Fraher LJ, Hendy GN, Chung UI, Kisiel M, Natale BV, Hodsman AB.Nuclear localization of the type 1 PTH/PTHrP receptor in rat tissues. J Bone MinerRes 15: 1033–1044, 2000.
1156. Webb AR, Kline L, Holick MF. Influence of season and latitude on the cutaneoussynthesis of vitamin D3: exposure to winter sunlight in Boston and Edmonton will notpromote vitamin D3 synthesis in human skin. J Clin Endocrinol Metab 67: 373–378,1988.
1157. Weiss LA, Langenberg C, Barrett-Connor E. Ghrelin and bone: is there an associa-tion in older adults?: the Rancho Bernardo study. J Bone Miner Res 21: 752–757, 2006.
1158. Weitkamp LR, Rucknagel DL, Gershowitz H. Genetic linkage between structural locifor albumin and group specific component (Gc). Am J Hum Genet 18: 559–571, 1966.
1159. Wettschureck N, Lee E, Libutti SK, Offermanns S, Robey PG, Spiegel AM. Parathy-roid-specific double knockout of Gq and G11 alpha-subunits leads to a phenotyperesembling germline knockout of the extracellular Ca2�-sensing receptor. Mol En-docrinol 21: 274–280, 2007.
1160. Whalen EJ, Rajagopal S, Lefkowitz RJ. Therapeutic potential of beta-arrestin- and Gprotein-biased agonists. Trends Mol Med 17: 126–139, 2011.
SASCHA KOPIC AND JOHN P. GEIBEL
266 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

1161. Wiborg O, Berglund L, Boel E, Norris F, Norris K, Rehfeld JF, Marcker KA, Vuust J.Structure of a human gastrin gene. Proc Natl Acad Sci USA 81: 1067–1069, 1984.
1162. Wikvall K. Hydroxylations in biosynthesis of bile acids. Isolation of a cytochromeP-450 from rabbit liver mitochondria catalyzing 26-hydroxylation of C27-steroids. JBiol Chem 259: 3800–3804, 1984.
1163. Wilkes JM, Kajimura M, Scott DR, Hersey SJ, Sachs G. Muscarinic responses of gastricparietal cells. J Membr Biol 122: 97–110, 1991.
1164. Windaus A. The chemistry of irradiated ergosterol. Proc R Soc Lond 108: 568–575,1931.
1165. Windaus A, Bock F. über das Provitamin aus dem Sterin der Schweineschwarte.Hoppe-Seyler’s Zeitschr physiol Chem 245: 168–170, 1936.
1166. Windaus A, Hess A. Sterine und antirachitisches Vitamin. In: Nachrichten von derGesellschaft der Wissenschaften zu Göttingen aus dem Jahre 1926. Berlin: Weidma-nnsche Buchhandlung, 1927, p. 175–184.
1167. Windaus A, Lüttringhaus A, Deppe M. über das krystallisierte Vitamin D1. Just LiebAnn Chem 489: 252–269, 1931.
1168. Wissenbach U, Niemeyer BA, Fixemer T, Schneidewind A, Trost C, Cavalie A, ReusK, Meese E, Bonkhoff H, Flockerzi V. Expression of CaT-like, a novel calcium-selective channel, correlates with the malignancy of prostate cancer. J Biol Chem 276:19461–19468, 2001.
1169. Wolosin JM, Forte JG. Stimulation of oxyntic cell triggers K� and Cl� conductancesin apical H�-K�-ATPase membrane. Am J Physiol Cell Physiol 246: C537–C545, 1984.
1170. Woodrow JP, Sharpe CJ, Fudge NJ, Hoff AO, Gagel RF, Kovacs CS. Calcitonin playsa critical role in regulating skeletal mineral metabolism during lactation. Endocrinology147: 4010–4021, 2006.
1171. Wortsman J, Pak CY, Bartter FC, Deftos L, Delea CS. Pathogenesis of osteomalaciain secondary hyperparathyroidism after gastrectomy. Am J Med 52: 556–564, 1972.
1172. Wrenn RW, Biddulph DM. Parathyroid hormone-induced calcium efflux from iso-lated renal cortical tubules: evidence for cyclic AMP mediation. Mol Cell Endocrinol15: 29–40, 1979.
1173. Wright MJ, Sullivan RR, Gaffney-Stomberg E, Caseria DM, O’Brien KO, Proctor DD,Simpson CA, Kerstetter JE, Insogna KL. Inhibiting gastric acid production does notaffect intestinal calcium absorption in young, healthy individuals: a randomized,crossover, controlled clinical trial. J Bone Miner Res 25: 2205–2211, 2010.
1174. Wu G, Burzon DT, di Sant’Agnese PA, Schoen S, Deftos LJ, Gershagen S, CockettAT. Calcitonin receptor mRNA expression in the human prostate. Urology 47: 376–381, 1996.
1175. Wu S, Grieff M, Brown AJ. Regulation of renal vitamin D-24-hydroxylase by phos-phate: effects of hypophysectomy, growth hormone and insulin-like growth factor I.Biochem Biophys Res Commun 233: 813–817, 1997.
1176. Wuster C, Raue F, Meyer C, Bergmann M, Ziegler R. Long-term excess of endoge-nous calcitonin in patients with medullary thyroid carcinoma does not affect bonemineral density. J Endocrinol 134: 141–147, 1992.
1177. Wyatt MA, Jarvie E, Feniuk W, Humphrey PP. Somatostatin sst2 receptor-mediatedinhibition of parietal cell function in rat isolated gastric mucosa. Br J Pharmacol 119:905–910, 1996.
1178. Xu H, Zhao H, Tian W, Yoshida K, Roullet JB, Cohen DM. Regulation of a transientreceptor potential (TRP) channel by tyrosine phosphorylation. SRC family kinase-dependent tyrosine phosphorylation of TRPV4 on TYR-253 mediates its response tohypotonic stress. J Biol Chem 278: 11520–11527, 2003.
1179. Xu J, Henriksnas J, Barone S, Witte D, Shull GE, Forte JG, Holm L, Soleimani M.SLC26A9 is expressed in gastric surface epithelial cells, mediates Cl�/HCO3
� ex-change, is inhibited by NH4
�. Am J Physiol Cell Physiol 289: C493–C505, 2005.
1180. Xu J, Song P, Miller ML, Borgese F, Barone S, Riederer B, Wang Z, Alper SL, Forte JG,Shull GE, Ehrenfeld J, Seidler U, Soleimani M. Deletion of the chloride transporterSlc26a9 causes loss of tubulovesicles in parietal cells and impairs acid secretion in thestomach. Proc Natl Acad Sci USA 105: 17955–17960, 2008.
1181. Xue Y, Fleet JC. Intestinal vitamin D receptor is required for normal calcium andbone metabolism in mice. Gastroenterology 136: 1317–1327, e1311–1312, 2009.
1182. Yamada T, Soll AH, Park J, Elashoff J. Autonomic regulation of somatostatin release:studies with primary cultures of canine fundic mucosal cells. Am J Physiol GastrointestLiver Physiol 247: G567–G573, 1984.
1183. Yamaguchi T, Chattopadhyay N, Kifor O, Brown EM. Extracellular calcium[Ca2�(o)]-sensing receptor in a murine bone marrow-derived stromal cell line(ST2): potential mediator of the actions of Ca2�(o) on the function of ST2 cells.Endocrinology 139: 3561–3568, 1998.
1184. Yamaguchi T, Chattopadhyay N, Kifor O, Butters RR Jr, Sugimoto T, Brown EM.Mouse osteoblastic cell line (MC3T3–E1) expresses extracellular calcium (Ca2�o)-sensing receptor and its agonists stimulate chemotaxis and proliferation ofMC3T3-E1 cells. J Bone Miner Res 13: 1530–1538, 1998.
1185. Yamaguchi T, Chattopadhyay N, Kifor O, Ye C, Vassilev PM, Sanders JL, Brown EM.Expression of extracellular calcium-sensing receptor in human osteoblastic MG-63cell line. Am J Physiol Cell Physiol 280: C382–C393, 2001.
1186. Yamauchi M, Yamaguchi T, Kaji H, Sugimoto T, Chihara K. Involvement of calcium-sensing receptor in osteoblastic differentiation of mouse MC3T3–E1 cells. Am JPhysiol Endocrinol Metab 288: E608–E616, 2005.
1187. Yang F, Brune JL, Naylor SL, Cupples RL, Naberhaus KH, Bowman BH. Humangroup-specific component (Gc) is a member of the albumin family. Proc Natl Acad SciUSA 82: 7994–7998, 1985.
1188. Yang F, Luna VJ, McAnelly RD, Naberhaus KH, Cupples RL, Bowman BH. Evolution-ary and structural relationships among the group-specific component, albumin andalpha-fetoprotein. Nucleic Acids Res 13: 8007–8017, 1985.
1189. Yang W, Friedman PA, Kumar R, Omdahl JL, May BK, Siu-Caldera ML, Reddy GS,Christakos S. Expression of 25(OH)D3 24-hydroxylase in distal nephron: coordinateregulation by 1,25(OH)2D3 and cAMP or PTH. Am J Physiol Endocrinol Metab 276:E793–E805, 1999.
1190. Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapyand risk of hip fracture. JAMA 296: 2947–2953, 2006.
1191. Yao X, Karam SM, Ramilo M, Rong Q, Thibodeau A, Forte JG. Stimulation of gastricacid secretion by cAMP in a novel alpha-toxin-permeabilized gland model. Am JPhysiol Cell Physiol 271: C61–C73, 1996.
1192. Ye CP, Yamaguchi T, Chattopadhyay N, Sanders JL, Vassilev PM, Brown EM. Extra-cellular calcium-sensing-receptor (CaR)-mediated opening of an outward K� chan-nel in murine MC3T3-E1 osteoblastic cells: evidence for expression of a functionalCaR. Bone 27: 21–27, 2000.
1193. Yergey AL, Abrams SA, Vieira NE, Aldroubi A, Marini J, Sidbury JB. Determination offractional absorption of dietary calcium in humans. J Nutr 124: 674–682, 1994.
1194. Yoshizawa T, Handa Y, Uematsu Y, Takeda S, Sekine K, Yoshihara Y, Kawakami T,Arioka K, Sato H, Uchiyama Y, Masushige S, Fukamizu A, Matsumoto T, Kato S. Micelacking the vitamin D receptor exhibit impaired bone formation, uterine hypoplasiaand growth retardation after weaning. Nat Genet 16: 391–396, 1997.
1195. Yu EW, Bauer SR, Bain PA, Bauer DC. Proton pump inhibitors and risk of fractures:a meta-analysis of 11 international studies. Am J Med 124: 519–526, 2011.
1196. Yu PL, Fujimura M, Hayashi N, Nakamura T, Fujimiya M. Mechanisms in regulatingthe release of serotonin from the perfused rat stomach. Am J Physiol Gastrointest LiverPhysiol 280: G1099–G1105, 2001.
1197. Yue L, Peng JB, Hediger MA, Clapham DE. CaT1 manifests the pore properties ofthe calcium-release-activated calcium channel. Nature 410: 705–709, 2001.
1198. Zacharias DA, Kappen C. Developmental expression of the four plasma membranecalcium ATPase (Pmca) genes in the mouse. Biochim Biophys Acta 1428: 397–405,1999.
1199. Zaidi M, Chambers TJ, Gaines Das RE, Morris HR, MacIntyre I. A direct action ofhuman calcitonin gene-related peptide on isolated osteoclasts. J Endocrinol 115:511–518, 1987.
1200. Zanello LP, Norman AW. Rapid modulation of osteoblast ion channel responses by1alpha,25(OH)2-vitamin D3 requires the presence of a functional vitamin D nuclearreceptor. Proc Natl Acad Sci USA 101: 1589–1594, 2004.
1201. Zanner R, Hapfelmeier G, Gratzl M, Prinz C. Intracellular signal transduction duringgastrin-induced histamine secretion in rat gastric ECL cells. Am J Physiol Cell Physiol282: C374–C382, 2002.
GASTRIC ACID, CALCIUM ABSORPTION, AND BONE HEALTH
267Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

1202. Zavros Y, Fleming WR, Hardy KJ, Shulkes A. Regulation of fundic and antral soma-tostatin secretion by CCK and gastrin. Am J Physiol Gastrointest Liver Physiol 274:G742–G750, 1998.
1203. Zavros Y, Shulkes A. Cholecystokinin (CCK) regulates somatostatin secretion through boththe CCK-A and CCK-B/gastrin receptors in sheep. J Physiol 505: 811–821, 1997.
1204. Zehnder D, Bland R, Chana RS, Wheeler DC, Howie AJ, Williams MC, Stewart PM,Hewison M. Synthesis of 1,25-dihydroxyvitamin D3 by human endothelial cells isregulated by inflammatory cytokines: a novel autocrine determinant of vascular celladhesion. J Am Soc Nephrol 13: 621–629, 2002.
1205. Zehnder D, Bland R, Williams MC, McNinch RW, Howie AJ, Stewart PM, HewisonM. Extrarenal expression of 25-hydroxyvitamin d(3)-1 alpha-hydroxylase. J Clin En-docrinol Metab 86: 888–894, 2001.
1206. Zehnder D, Evans KN, Kilby MD, Bulmer JN, Innes BA, Stewart PM, Hewison M.The ontogeny of 25-hydroxyvitamin D(3) 1alpha-hydroxylase expression in humanplacenta and decidua. Am J Pathol 161: 105–114, 2002.
1207. Zeng N, Athmann C, Kang T, Lyu RM, Walsh JH, Ohning GV, Sachs G, Pisegna JR.PACAP type I receptor activation regulates ECL cells and gastric acid secretion. J ClinInvest 104: 1383–1391, 1999.
1208. Zeng N, Kang T, Lyu RM, Wong H, Wen Y, Walsh JH, Sachs G, Pisegna JR. Thepituitary adenylate cyclase activating polypeptide type 1 receptor (PAC1-R) is ex-pressed on gastric ECL cells: evidence by immunocytochemistry and RT-PCR. AnnNY Acad Sci 865: 147–156, 1998.
1209. Zeng N, Kang T, Wen Y, Wong H, Walsh J, Sachs G. Galanin inhibition of entero-chromaffin-like cell function. Gastroenterology 115: 330–339, 1998.
1210. Zeng N, Walsh JH, Kang T, Wu SV, Sachs G. Peptide YY inhibition of rat gastricenterochromaffin-like cell function. Gastroenterology 112: 127–135, 1997.
1211. Zhang JX, Fasciotto BH, Darling DS, Cohn DV. Pancreastatin, a chromogranin A-derived peptide, inhibits transcription of the parathyroid hormone and chromo-granin A genes and decreases the stability of the respective messenger ribonucleicacids in parathyroid cells in culture. Endocrinology 134: 1310–1316, 1994.
1212. Zhang W, Na T, Wu G, Jing H, Peng JB. Down-regulation of intestinal apical calcium entrychannel TRPV6 by ubiquitin E3 ligase Nedd4–2. J Biol Chem 285: 36586–36596, 2010.
1213. Zhang Z, Sun S, Quinn SJ, Brown EM, Bai M. The extracellular calcium-sensingreceptor dimerizes through multiple types of intermolecular interactions. J Biol Chem276: 5316–5322, 2001.
1214. Zhao CM, Chen D, Yamada H, Dornonville de la Cour C, Lindstrom E, Persson L,Hakanson R. Rat stomach ECL cells: mode of activation of histidine decarboxylase.Regul Pept 114: 21–27, 2003.
1215. Zhao CM, Jacobsson G, Chen D, Hakanson R, Meister B. Exocytotic proteins inenterochromaffin-like (ECL) cells of the rat stomach. Cell Tissue Res 290: 539–551,1997.
1216. Zhao G, Simpson RU. Membrane localization, Caveolin-3 association and rapidactions of vitamin D receptor in cardiac myocytes. Steroids 75: 555–559,2010.
1217. Zhong Y, Armbrecht HJ, Christakos S. Calcitonin, a regulator of the 25-hydroxyvi-tamin D3 1alpha-hydroxylase gene. J Biol Chem 284: 11059–11069, 2009.
1218. Zhou AT, Assil I, Abou-Samra AB. Role of asparagine-linked oligosaccharides in thefunction of the rat PTH/PTHrP receptor. Biochemistry 39: 6514–6520, 2000.
1219. Zhou C, Lu F, Cao K, Xu D, Goltzman D, Miao D. Calcium-independent and1,25(OH)2D3-dependent regulation of the renin-angiotensin system in 1alpha-hy-droxylase knockout mice. Kidney Int 74: 170–179, 2008.
1220. Zhuang L, Peng JB, Tou L, Takanaga H, Adam RM, Hediger MA, Freeman MR.Calcium-selective ion channel, CaT1, is apically localized in gastrointestinal tractepithelia and is aberrantly expressed in human malignancies. Lab Invest 82: 1755–1764, 2002.
1221. Zhuang X, Adipietro KA, Datta S, Northup JK, Ray K. Rab1 small GTP-bindingprotein regulates cell surface trafficking of the human calcium-sensing receptor.Endocrinology 151: 5114–5123, 2010.
1222. Zierold C, Mings JA, DeLuca HF. Parathyroid hormone regulates 25-hydroxyvitaminD(3)-24-hydroxylase mRNA by altering its stability. Proc Natl Acad Sci USA 98:13572–13576, 2001.
1223. Zietkiewicz E, Labuda M, Sinnett D, Glorieux FH, Labuda D. Linkage mapping bysimultaneous screening of multiple polymorphic loci using Alu oligonucleotide-di-rected PCR. Proc Natl Acad Sci USA 89: 8448–8451, 1992.
1224. Zornitzer AE, Bronner F. In situ studies of calcium absorption in rats. Am J Physiol220: 1261–1266, 1971.
1225. Zuo Q, Claveau D, Hilal G, Leclerc M, Brunette MG. Effect of calcitonin on calciumtransport by the luminal and basolateral membranes of the rabbit nephron. Kidney Int51: 1991–1999, 1997.
SASCHA KOPIC AND JOHN P. GEIBEL
268 Physiol Rev • VOL 93 • JANUARY 2013 • www.prv.org
on Decem
ber 8, 2014D
ownloaded from

doi:10.1152/physrev.00015.2012 93:189-268, 2013.Physiol RevSascha Kopic and John P. Geibelon Bone HealthGastric Acid, Calcium Absorption, and Their Impact
You might find this additional info useful...
1211 articles, 454 of which can be accessed free at:This article cites /content/93/1/189.full.html#ref-list-1
1 other HighWire hosted articlesThis article has been cited by
[PDF] [Full Text] [Abstract]
, August 19, 2014; .Gastroenterol. Rep.James Wei Tatt Toh, Evonne Ong and Robert WilsonHypomagnesaemia associated with long-term use of proton pump inhibitors
including high resolution figures, can be found at:Updated information and services /content/93/1/189.full.html
can be found at:Physiological Reviewsabout Additional material and information http://www.the-aps.org/publications/prv
This information is current as of December 8, 2014.
website at http://www.the-aps.org/.MD 20814-3991. Copyright © 2013 by the American Physiological Society. ISSN: 0031-9333, ESSN: 1522-1210. Visit ourpublished quarterly in January, April, July, and October by the American Physiological Society, 9650 Rockville Pike, Bethesda
provides state of the art coverage of timely issues in the physiological and biomedical sciences. It isPhysiological Reviews
on Decem
ber 8, 2014D
ownloaded from