Embed Size (px)
Citation preview

Gastric Acid Secretion and Gastrointestinal Hormone Release
After Biliary Reconstruction Procedures
Toshio Sato, MD, FACS, Sendai, Japan
Mikio Imamura, MD, Sendai, Japan
lwao Sasaki, MD, Sendai, Japan
Jinichi Kameyama, MD, Sendai, Japan
The hypersecretion of gastric acid and the develop- ment of peptic ulcer after Roux-Y choledochojeju- nostomy have been pointed out by many surgeons. This tendency was also observed in our experiments using dogs subjected to Roux-Y cholecystojejunos- tomy [I]. Consequently, we have adopted jejunal interposition choledochoduodenostomy as another type of biliary reconstruction procedure and have been applying it in addition to Roux-Y choledocho- jejunostomy since 1977. In our previous study [2], we reported postoperative changes of gastric acid, plasma gastrin, and secretin secretion, by comparing patients undergoing Roux-Y choledochojejunostomy with those undergoing jejunal interposition chole- dochoduodenostomy. In this report, to further in- vestigate the mechanism of gastric acid hypersecre- tion after the Roux-Y procedure, more studies were carried out with regard to the changes of gastric acid secretion and gastrointestinal hormones.
Patients and Methods
Of the patients who underwent hiliary reconstruction procedures in our clinic for benign bile duct disorders during a 20 year period (from April 1961 to March 1981), a total of 36 patients, 10 with jejunal interposition chole- dochoduodenostomy and 26 with Roux-Y choledochoje- junostomy, were available for follow-up. The mean age of the patients was 47 years for the interposition group (range 19 to 66 years), and 36 years for the Roux-Y group (range 15 to 70 years). The male to female ratio was 2:8 for the interposition group and 8:18 for the Roux-Y group. The follow-up period ranged from 6 months to 3 years for the interposition group, averaging 1 year 8 months, and from 1 year 1 month to 15 years 4 months for the Roux-Y group,
From the Department of Surgery, Tohoku University School of Medicine, Sendai, Japan.
Requests for reprints should be addressed to Toshii Sato. MD, Department of Surgery, Tohoku University School of Medicine, Sendai, 980. Japan.
averaging 8 years. In both groups, the most common pri- mary diseases were congenital choledochal dilatation in 20 patients, followed by postoperative bile duct stricture in 9, stenosis of the bilioenteric anastomosis in 6, and intra- operative bile duct injury in 1.
In these patients, whenever possible, a gastric secretory test was performed after an overnight fast as follows: A Salem samp tube was inserted into the fundic area of the stomach. After the gastric contents were completely re- moved, gastric juice was collected during two 15 minute intervals; then, tetragastrin (4 pg/kg) was injected intra- muscularly as a stimulating agent, and gastric juice was collected during five periods at 15 minute intervals. The concentration of gastric acid was determined by titration with 0.1 normal NaOH using Topfer’s reagent as an indi- cator. The amount of gastric acid secretion was expressed in terms of basal acid output, which represents 1 hour acid output at a fasting state as well as maximum acid output, which represents 1 hour acid output after injection of te- tragastrin. Then, the preoperative level of maximum acid output was compared with the level at the time of follow-up in each group. Moreover, a comparison of the levels of maximum acid output at follow-up between the two groups was performed. At follow-up, a test meal of 300 g of rice gruel and an egg, (carbohydrate 70.9 percent, protein 16.4 percent, and fat 10.7 percent), was given to each patient. The blood was sampled from the peripheral vein at fasting and at 1530, and 60 minutes after test meal loading. The sampled blood was heparinized and drawn into ice-chilled glass tubes containing aprotinin 500 KIU per 1 ml of blood. Blood samples were centrifuged at 4°C immediately after the completion of the test and the plasma was then sepa- rated. The plasma was stored at -2OOC until the assay for gastrointestinal hormones was performed. Plasma im- munoreactive gastric inhibitory polypeptide was measured using a modified method of Sarson et al [3] with antiserum 312187 (supplied by S. R. Bloom, MD, Royal Postgraduate Medical School, London, UK). Plasma immunoreactive insulin was measured using an assay kit (Dainabot Ra- dioisotope Laboratory, Tokyo, Japan) [4]. The blood glu- cose level was determined from blood obtained from the
Volume 148, August lg83 245
Sat0 et al
TABLE I Changes In Basal Acid Output (mean f standard error of the mean)
Before At P Operation Follow-UQ Value
Jejunal interposition 0.82 f 0.69 1.67 f 0.73 NS choledochoduode- n= 10 n= 11 nostomy
Roux-Y choledochojeju- 0.29 f 0.25 0.92 f 0.49 NS nostomy n=8 n= 15
NS = not significant.
peripheral vein by the glucose oxidase method [5]. The levels of immunoreactive gastric inhibitory polypeptide, immunoreactive insulin, and blood glucose in the inter- position and the Roux-Y groups were compared. Because of a great difference in the follow-up period between the two groups, a comparative study of the changes in gastric acid secretion was also made selectively in the patients with approximately the same follow-up period. All results were expressed as the mean f: the standard error of the mean. The Student’s t test was used to analyse the data; p values less than 0.05 were considered statistically significant.
Results
Changes in basal acid output: The values of basal acid output in patients in the interposition group were 0.82 f 0.69 mEq/h before the operation and 1.67 f 0.73 mEq/h at follow-up, whereas in pa- tients in the Roux-Y group, the corresponding values were 0.29 f 0.25 mEq/h and 0.92 f 0.49 mEq/h, re- spectively (Table I). In both groups, there was no significant difference in the levels of basal acid out- put before surgery and at follow-up. Moreover, dur- ing follow-up, there was no significant difference in the levels of basal acid output between patients who underwent the interposition procedure and those who underwent the Roux-Y procedure.
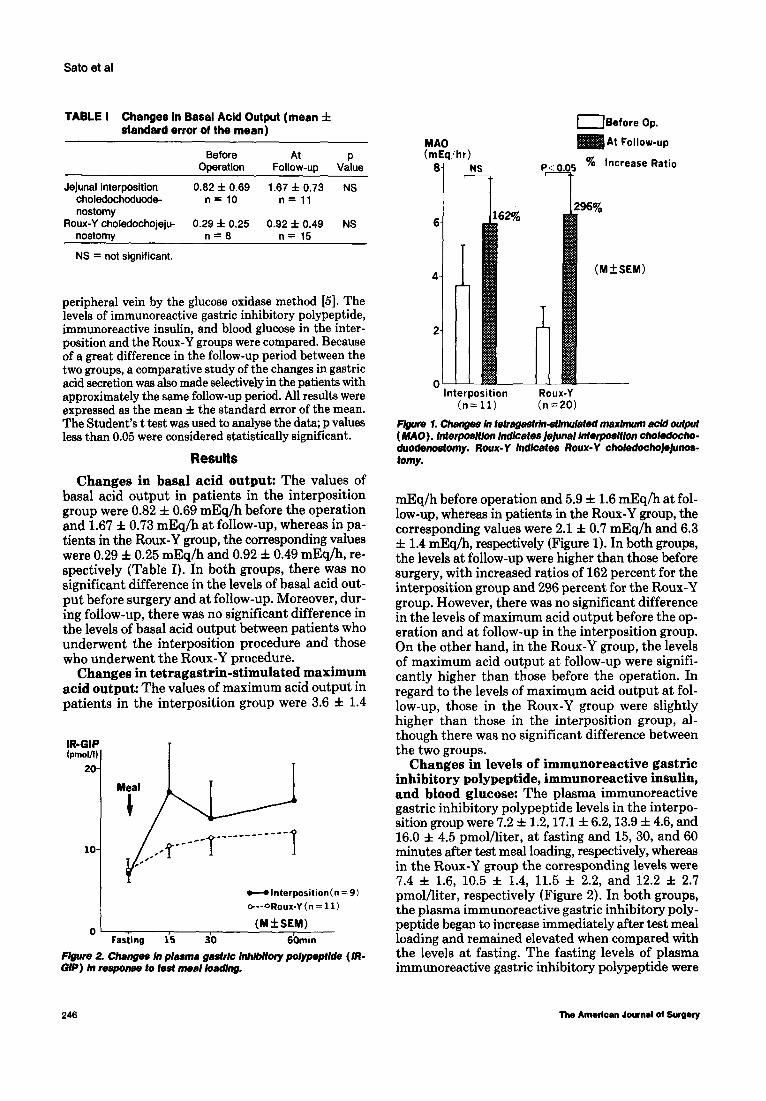
Changes in tetragastrin-stimulated maximum acid output: The values of maximum acid output in patients in the interposition group were 3.6 f 1.4
10
id
,/,,*___q------------ I
Fasting 15 30 60min
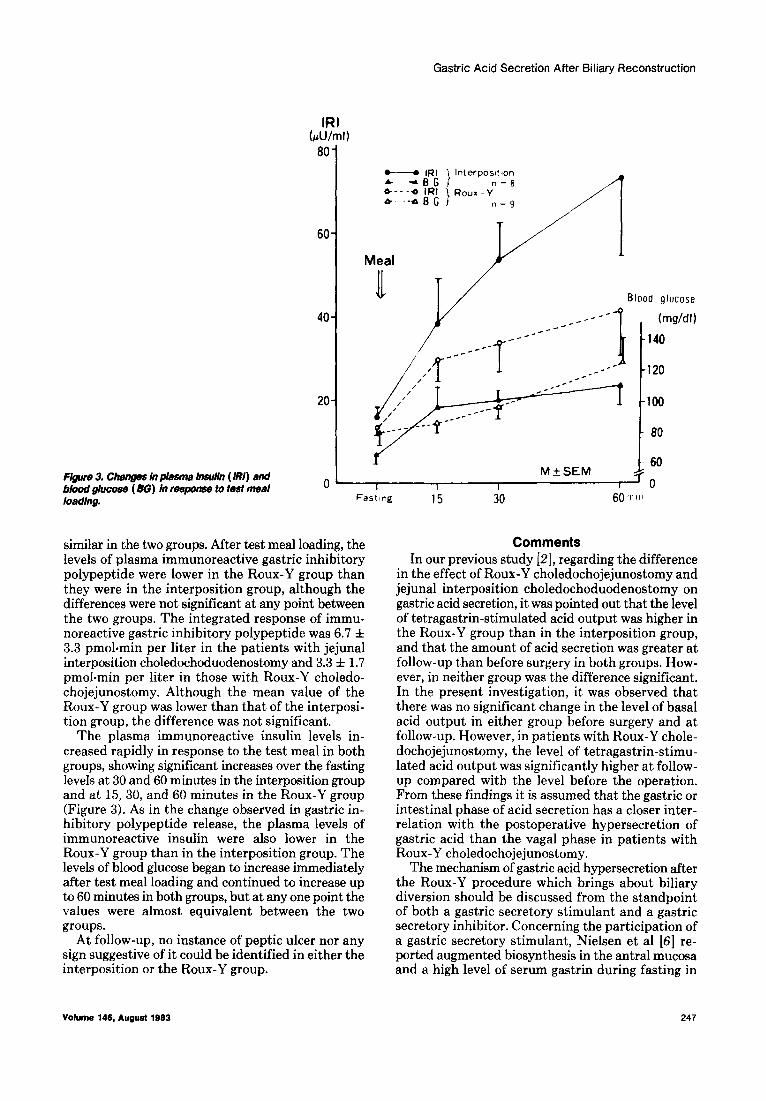
Figure 2. Changes ln p&ma gas&k Inhlbltory polypeptlde (IR- GIP) In response to test meal loading.
MAO (mEq :hr)
8
(Before Op.
At Follow-up
P < 0.05 % Increase Ratio
Interposition (n= 11)
Roux-Y (n=20)
F&we 1. Changes In tetragastrln-stlnwlafed maxmm acid output (MAO). InterposMon lndlcates)e)unal lntetposlilon choledocho- duodenostomy. Roux-Y M/cafes Roux-Y choledocho~@os- tomy.
mEq/h before operation and 5.9 f 1.6 mEq/h at fol- low-up, whereas in patients in the Roux-Y group, the corresponding values were 2.1 f 0.7 mEq/h and 6.3 f 1.4 mEq/h, respectively (Figure 1). In both groups, the levels at follow-up were higher than those before surgery, with increased ratios of 162 percent for the interposition group and 296 percent for the Roux-Y group. However, there was no significant difference in the levels of maximum acid output before the op- eration and at follow-up in the interposition group. On the other hand, in the Roux-Y group, the levels of maximum acid output at follow-up were signifi- cantly higher than those before the operation. In regard to the levels of maximum acid output at fol- low-up, those in the Roux-Y group were slightly higher than those in the interposition group, al- though there was no significant difference between the two groups.
Changes in levels of immunoreactive gastric inhibitory polypeptide, immunoreactive insulin, and blood glucose: The plasma immunoreactive gastric inhibitory polypeptide levels in the interpo- sition group were 7.2 f 1.2,17.1 f 6.2,13.9 f 4.6, and 16.0 f 4.5 pmolkter, at fasting and 15, 30, and 60 minutes after test meal loading, respectively, whereas in the Roux-Y group the corresponding levels were 7.4 f 1.6, 10.5 f 1.4, 11.5 f 2.2, and 12.2 f 2.7 pmol/liter, respectively (Figure 2). In both groups, the plasma immunoreactive gastric inhibitory poly- peptide began to increase immediately after test meal loading and remained elevated when compared with the levels at fasting. The fasting levels of plasma immunoreactive gastric inhibitory polypeptide were
246 The American Journal oi Surgery
Gastric Acid Secretion After Biliary Reconstruction
60
40
20
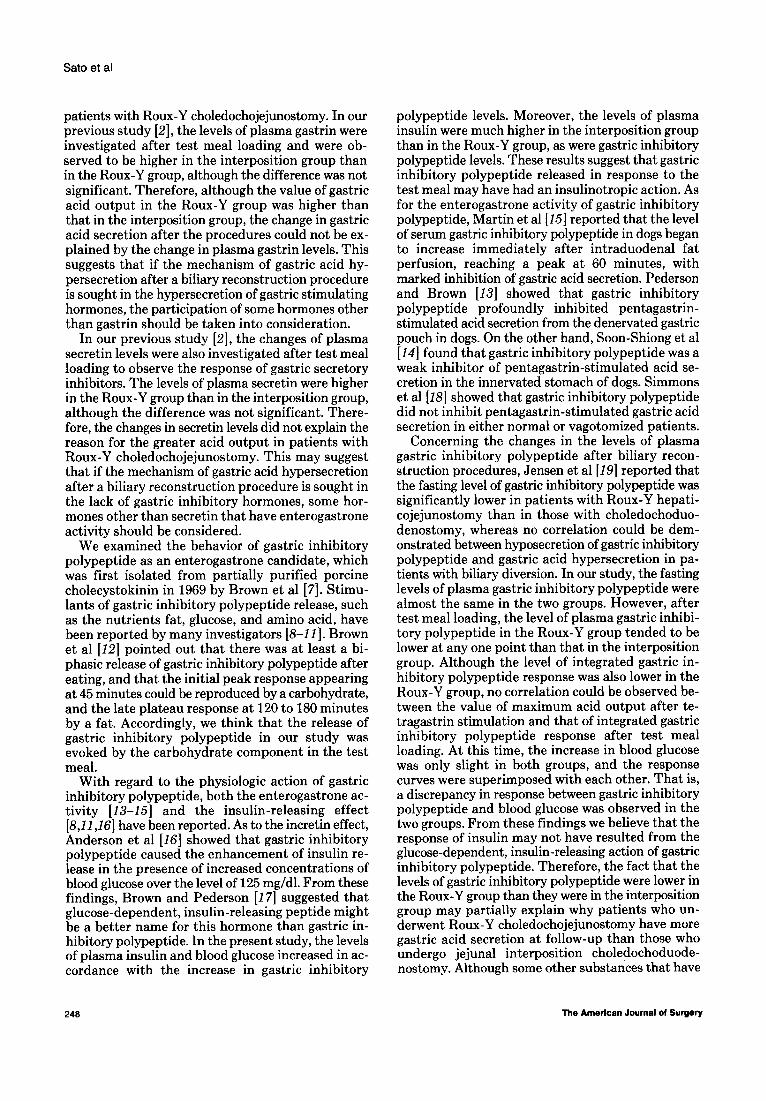
F@ue 3. Changes In plasma Insulin (MI) and blood glucose ( BG) in response to test meal
0
loading.
- IRI &-dBG *---o IRI & .-a B G
Meal
1 Int erposltlon n=R
i Roux-Y -
n=9
Blood glucose
similar in the two groups. After test meal loading, the levels of plasma immunoreactive gastric inhibitory polypeptide were lower in the Roux-Y group than they were in the interposition group, although the differences were not significant at any point between the two groups. The integrated response of immu- noreactive gastric inhibitory polypeptide was 6.7 f 3.3 pmohmin per liter in the patients with jejunal interposition choledochoduodenostomy and 3.3 f 1.7 pmol+min per liter in those with Roux-Y choledo- chojejunostomy. Although the mean value of the Roux-Y group was lower than that of the interposi- tion group, the difference was not significant.
The plasma immunoreactive insulin levels in- creased rapidly in response to the test meal in both groups, showing significant increases over the fasting levels at 30 and 60 minutes in the interposition group and at l&30, and 60 minutes in the Roux-Y group (Figure 3). As in the change observed in gastric in- hibitory polypeptide release, the plasma levels of immunoreactive insulin were also lower in the Roux-Y group than in the interposition group. The levels of blood glucose began to increase immediately after test meal loading and continued to increase up to 60 minutes in both groups, but at any one point the values were almost equivalent between the two groups.
At follow-up, no instance of peptic ulcer nor any sign suggestive of it could be identified in either the interposition or the Roux-Y group.
15 30
Comments In our previous study [2], regarding the difference
in the effect of Roux-Y choledochojejunostomy and jejunal interposition choledochoduodenostomy on gastric acid secretion, it was pointed out that the level of tetragastrin-stimulated acid output was higher in the Roux-Y group than in the interposition group, and that the amount of acid secretion was greater at follow-up than before surgery in both groups. How- ever, in neither group was the difference significant. In the present investigation, it was observed that there was no significant change in the level of basal acid output in either group before surgery and at follow-up. However, in patients with Roux-Y chole- dochojejunostomy, the level of tetragastrin-stimu- lated acid output was significantly higher at follow- up compared with the level before the operation. From these findings it is assumed that the gastric or intestinal phase of acid secretion has a closer inter- relation with the postoperative hypersecretion of gastric acid than the vagal phase in patients with Roux-Y choledochojejunostomy.
The mechanism of gastric acid hypersecretion after the Roux-Y procedure which brings about biliary diversion should be discussed from the standpoint of both a gastric secretory stimulant and a gastric secretory inhibitor. Concerning the participation of a gastric secretory stimulant, Nielsen et al [6] re- ported augmented biosynthesis in the antral mucosa and a high level of serum gastrin during fasting in
Volume 146, August 1863
Sat0 et al
patients with Roux-Y choledochojejunostomy. In our previous study [Z], the levels of plasma gastrin were investigated after test meal loading and were ob- served to be higher in the interposition group than in the Roux-Y group, although the difference was not significant. Therefore, although the value of gastric acid output in the Roux-Y group was higher than that in the interposition group, the change in gastric acid secretion after the procedures could not be ex- plained by the change in plasma gastrin levels. This suggests that if the mechanism of gastric acid hy- persecretion after a biliary reconstruction procedure is sought in the hypersecretion of gastric stimulating hormones, the participation of some hormones other than gastrin should be taken into consideration.
In our previous study [2], the changes of plasma secretin levels were also investigated after test meal loading to observe the response of gastric secretory inhibitors. The levels of plasma secretin were higher in the Roux-Y group than in the interposition group, although the difference was not significant. There- fore, the changes in secretin levels did not explain the reason for the greater acid output in patients with Roux-Y choledochojejunostomy. This may suggest that if the mechanism of gastric acid hypersecretion after a biliary reconstruction procedure is sought in the lack of gastric inhibitory hormones, some hor- mones other than secretin that have enterogastrone activity should be considered.
We examined the behavior of gastric inhibitory polypeptide as an enterogastrone candidate, which was first isolated from partially purified porcine cholecystokinin in 1969 by Brown et al [7]. Stimu- lants of gastric inhibitory polypeptide release, such as the nutrients fat, glucose, and amino acid, have been reported by many investigators [8-111. Brown et al [12] pointed out that there was at least a bi- phasic release of gastric inhibitory polypeptide after eating, and that the initial peak response appearing at 45 minutes could be reproduced by a carbohydrate, and the late plateau response at 120 to 180 minutes by a fat. Accordingly, we think that the release of gastric inhibitory polypeptide in our study was evoked by the carbohydrate component in the test meal.
With regard to the physiologic action of gastric inhibitory polypeptide, both the enterogastrone ac- tivity [13-1.51 and the insulin-releasing effect [8,11,26] have been reported. As to the incretin effect, Anderson et al [16] showed that gastric inhibitory polypeptide caused the enhancement of insulin re- lease in the presence of increased concentrations of blood glucose over the level of 125 mg/dl. From these findings, Brown and Pederson [17] suggested that glucose-dependent, insulin-releasing peptide might be a better name for this hormone than gastric in- hibitory polypeptide. In the present study, the levels of plasma insulin and blood glucose increased in ac- cordance with the increase in gastric inhibitory
polypeptide levels. Moreover, the levels of plasma insulin were much higher in the interposition group than in the Roux-Y group, as were gastric inhibitory polypeptide levels. These results suggest that gastric inhibitory polypeptide released in response to the test meal may have had an insulinotropic action. As for the enterogastrone activity of gastric inhibitory polypeptide, Martin et al [15] reported that the level of serum gastric inhibitory polypeptide in dogs began to increase immediately after intraduodenal fat perfusion, reaching a peak at 60 minutes, with marked inhibition of gastric acid secretion. Pederson and Brown [13] showed that gastric inhibitory polypeptide profoundly inhibited pentagastrin- stimulated acid secretion from the denervated gastric pouch in dogs. On the other hand, Soon-Shiong et al [14] found that gastric inhibitory polypeptide was a weak inhibitor of pentagastrin-stimulated acid se- cretion in the innervated stomach of dogs. Simmons et al [18] showed that gastric inhibitory polypeptide did not inhibit pentagastrin-stimulated gastric acid secretion in either normal or vagotomized patients.
Concerning the changes in the levels of plasma gastric inhibitory polypeptide after biliary recon- struction procedures, Jensen et al [19] reported that the fasting level of gastric inhibitory polypeptide was significantly lower in patients with Roux-Y hepati- cojejunostomy than in those with choledochoduo- denostomy, whereas no correlation could be dem- onstrated between hyposecretion of gastric inhibitory polypeptide and gastric acid hypersecretion in pa- tients with biliary diversion. In our study, the fasting levels of plasma gastric inhibitory polypeptide were almost the same in the two groups. However, after test meal loading, the level of plasma gastric inhibi- tory polypeptide in the Roux-Y group tended to be lower at any one point than that in the interposition group. Although the level of integrated gastric in- hibitory polypeptide response was also lower in the Roux-Y group, no correlation could be observed be- tween the value of maximum acid output after te- tragastrin stimulation and that of integrated gastric inhibitory polypeptide response after test meal loading. At this time, the increase in blood glucose was only slight in both groups, and the response curves were superimposed with each other. That is, a discrepancy in response between gastric inhibitory polypeptide and blood glucose was observed in the two groups. From these findings we believe that the response of insulin may not have resulted from the glucose-dependent, insulin-releasing action of gastric inhibitory polypeptide. Therefore, the fact that the levels of gastric inhibitory polypeptide were lower in the Roux-Y group than they were in the interposition group may partially explain why patients who un- derwent Roux-Y choledochojejunostomy have more gastric acid secretion at follow-up than those who undergo jejunal interposition choledochoduode- nostomy. Although some other substances that have
248 The American Journal of Surgery
Gastric Acid Secretion After Biliary Reconstruction
enterogastrone activity besides gastric inhibitory polypeptide should also be investigated, it is assumed that gastric inhibitory polypeptide released after test meal loading might have an influence on gastric acid secretion after a biliary reconstruction procedure.
Summary
5. Teller JD. Direct, quantative calorimetric determination of serum or plasma glucose. Abstracts of papers presented at 130th meeting of the American Chemical Society 1956;69C.
6. Nielsen ML, Jensen SL, MaImstram J. Gastrin and gastric acid secretion in hepaticojejunostomy Roux-en-Y. Surg Gynecol Obstet 1980;150:61-4.
7. Brown JC, Pederson RA, Jorpes JE, Mutt V. Preparation of highly active enterogastrone. Can J Physiol Pharmacol 1969;47: 113-4.
The changes in gastric acid secretion and gas- trointestinal hormone release were studied after biliary tract reconstruction to investigate the mechanism of gastric acid hypersecretion after a biliary diversion procedure. At follow-up, gastric acid output in patients with Roux-Y choledochojejunos- tomy was significantly higher than before the oper- ation. In contrast, in patients with jejunal interpo- sition choledochoduodenostomy, which does not bring about biliary diversion, acid output increased slightly after the operation. Moreover, at follow-up, acid output in the Roux-Y group was slightly higher than it was in the interposition group. Although the fasting levels of plasma gastric inhibitory polypeptide were almost the same in both groups, the loading of a test meal elicited a lower response of plasma gastric inhibitory polypeptide in patients with the Roux-Y procedure than in those with the interposition pro- cedure. Therefore, it is assumed that gastric inhibi- tory polypeptide, as an enterogastrone after a biliary reconstruction procedure, might have some influence on gastric acid secretion.
Acknowledgmenb We wish to thank Dr. S. R. Bloom for the kind gift of gastric inhibitory polypeptide anti- sera.
References
1. Sekine T, Tsukui H, Kameyama J, Sasaki I, Sato T. Influence of biliary diversion upon gastric acid secretion. Tohoku J Exp Med 1981;134:125-39.
2. Sato T, lmamura M, Sasaki I, Kameyama J. Effect of biliary reconstruction procedures upon gastric acid secretion. Am J Surg 1982; 144549-53.
3. Sarson DL, Bryant MG, Bloom SR. A radioimmunoassay of gastric inhibitory polypeptide in human plasma. J Endocrinol 1980;85:487-96.
4. Yalow RS, Berson SA. Immunoassay of endogenous plasma insulin in man. J Clin Invest 1960;39:1157-75.
8. Brown JC, Dryburgh JR, Ross SA, Dupre J. Identification and actions of gastric inhibitory polypeptide. Recent Prog Horm Res 1975;31:487-532.
9. Thomas F5, Mazzaferri E, Crockett SE, Mekhjiam HS, Cruemer HD. Cataland S. Stimulation of secretion of gastric inhibitory polypeptide and insulin by intraduodenal amino acid perfu- sion. Gastroenterology 1976;70:523-7.
10. Thomas FB, Shook DF, O’Dorisio TM, et al. Localization of gastric inhibitory polypeptide release by intestinal glucose perfusion in man. Gastroenterology 1977;72:49-54.
11. Walsh JH. Gastric inhibitory polypeptide. In: Johnson LR, Christensen JC, Grossman MI, Jacobson ED, Schultz SG, eds. Physiology of the gastrointestinal tract. Vol. 1. New York: Raven Press, 1981:93-g.
12. Brown JC, Dryburgh JR, Moccia P, Pederson RA. The current status of GIP. In: Thompson JC, ed. A symposium. Gas- trointestinal hormones. Austin: University of Texas Press, 1975:537-47.
13. Pederson RA, Brown JC. Inhibition of histamine-, pentagastrin-, and insulin-stimulated canine gastric secretion by pure “gastric inhibitory polypeptide.” Gastroenterology 1972; 62:393-400.
14. Soon-Shiong P, Debas HT, Brown JC. The evaluation of gastric inhibitory polypeptide (GIP) as the enterogastrone. J Surg Res 1979;26:681-6.
15. Martin EW, O’Dorisio TM, Spaeth J, Thomford NR, Cataland S. The association between endogenous gastric inhibitory polypeptide release and suppression of gastric acid output following intraduodenal fat stimulation. J Surg Res 1980; 29171-4.
16. Anderson DK, Elahi D, Brown JC, Tobin JD, Andres R. Oral glucose augmentation of insulin secretion. Interactions of gastric inhibitory polypeptide with ambient glucose and in- sulin levels. J Clin Invest 1978;62:152-61.
17. &own JC, Pederson RA. Endocrinology. Proceedings of the Fifth International Congress of Endocrinology. Vol. 2. Amsterdam: Excerpta Medica, 1977:568-70.
18. Simmons TC, Taylor IL. Maxwell V, Brown JC, Grossman Ml. Failure of gastric inhibitory polypeptide to inhibit pentagas- trin-stimulated acid secretion in vagotomized human subjects. Dig Dis Sci 1981;26:902-4.
19. Jensen SL, Lauritsen KB, Nielsen ML, Nielsen OV. Basal hy- posecretion of gastric inhibitory polypeptide after Roux-Y hepaticojejunostomy in man. Am J Surg 1981;142:328- 30.
Volume 146, August 1983 249





























