Embed Size (px)
Citation preview

BIOMEDICAL AND ENVIRONMENTAL MASS SPECTROMETRY, VOL. 19, 453-458 (1990)
Gas Chromatography/Negative Ion Chemical Ionization/Tandem Mass Spectrometric Quantification of Indomethacin in Plasma and Synovial Fluid
Michael Dawson,? Michael D. Smith and C. M. McGee Department of Rheumatology, Royal North Shore Hospital, St Leonards, NSW 2065, Australia
A procedure for the quantification of sub-nanogram per millilitre concentrations of indomethacin in plasma and synovial fluid has been developed using gas chromatography/negative ion chemical ionization/tandem mass spec- trometry. The procedure is based on selected ion monitoring of the daughter ion at m/z 312 generated following decarboxylation of the "Cl isotope peak of the indomethacin anion (m/z 3%) formed from the pentafluorobenzyl ester of indomethacin in the ion source of the mass spectrometer. The internal standard, d,-indomethacin, has a daughter ion at m/z 316 formed from the corresponding "CI isotope peak. The limit of quantification was 0.1 ng ml- ' for both plasma and synovial fluid.
INTRODUCTION
Non-steroidal anti-inflammatory drugs (NSAIDs) are used to reduce the pain and swelling associated with a variety of inflammatory conditions such as osteo- and rheumatoid arthritis as well as soft tissue injury, but a common side effect of treatment with these drugs is gas- trointestinal upset.' NSAIDs exert their anti- inflammatory effect by inhibition of the formation of prostaglandins from arachidonic acid.2 However, whilst most prostaglandins are pro-inflammatory, some exert an anti-inflammatory action. This paradoxical action of prostaglandins is thought to be the basis for the gastrointestinal side effects of NSAID treatment and presents a dilemma for the physician.
One approach for resolving such problems is to deliver the drug directly to the site of action. This has been very successful in the treatment of asthma, where the cardiovascular side effects of brochodilating sub- stances (e.g. salbutamol) are minimized by direct inhala- tion of the drug. There is considerable clinical evidence to suggest that the topical application of NSAIDs is beneficial in the treatment of soft tissue injury and various arthropathies, and topical preparations contain- ing methyl salicylate have been used for centuries.
Clinical efficacy studies often need to be supported by reporting plasma and synovial fluid drug concentra- tions. But these concentrations are usually very low fol- lowing topical application of NSAIDS.~.~ Therefore a very sensitive monitoring technique is required.
The subject of this publication is the development of the analytical methodology required to quantify the plasma and synovial fluid concentrations of indometha- cin (1 -(4-chlorobenzoyl)-5-methoxy-2-methyl- lH-indole- 3-acetic acid (Fig. 1)) applied to the skin as an ethanolic solution. Literature methods for the quantification of
t Author to whom correspondence should be addressed.
0887-6134/90/080453-06 S05.00 0 1990 by John Wiley & Sons, Ltd.
Figure 1. lndomethacin (1 -(4-chlorobenzoyl)-5-methoxy-2- methyl-1 H- indole-3-acetic acid).
indomethacin in biological fluids usually involve high- performance liquid chromatography (HPLC) with ultra- violet (UV) detection5s6 or fluorescence detection3 None of the published methods provide the required level of sensitivity or selectivity for the study we wished to conduct.
Because indomethacin possesses a carboxylic acid functional group it is ideally suited to assay by negative ion chemical ionization mass spectrometry (NICI/MS), as the pentafluorobenzyl (PFB) ester. For certain com- pounds NICI/MS is orders of magnitude more sensitive than positive ion chemical ionization (PICI) or electron impact (EI)/MS.
The high sensitivity of NICI/MS and the selectivity offered by tandem mass spectrometry (MS/MS) have enabled us to develop an assay for indomethacin in plasma and synovial fluid with a lower limit of detec- tion of 0.1 ng ml-', using detuerium-labelled indo- methacin as the internal standard.
~
EXPERIMENTAL
Internal standard
Deuterium-labelled indomethacin was synthesized by an exchange reaction with D20, as reported pre- viously.8 This material contained less than 1% un- deuterated indomethacin. NQ loss of label occurred
Received 20 September 1989 Accepted (revised) 30 March 1990

454 M. DAWSON, M. D. SMITH AND C. M. McGEE
during the extraction or derivatization procedure. Simi- larly, no loss of label was observed in the standard solu- tion of deuterium-labelled indomethacin which was stored at - 20 "C for 4 months.
Gas chromatography/mass spectrometry/mass spectrometry (GCWSWS)
GC/MS/MS analyses were carried out on a Finnigan TSQ 46 triple-stage quadrupole gas chromatograph/ mass spectrometer operating in NICI mode. The BP5 fused-silica bonded-phase capillary column (12 m x 0.2 mm i.d., 0.1 pm film thickness) was inserted directly into the ion source of the mass spectrometer. Helium (2 ml min-') was the GC carrier gas and methane, the CI reactant gas, was introduced through the make-up valve to give a final source pressure of 130 Pa.
The effect of temperature on the ionization and rela- tive abundance of ions in the NICI mass spectrum of the PFB ester of indomethacin was observed over a range of ion source temperatures at an electron beam energy of I 0 0 eV.
The effects of collision pressure and collision energy on the collision-activated decomposition (CAD) spec- trum of the indomethacin anion were observed at three different pressures of argon and collision energies between 0 and 30 eV.
The capillary column was held at 150 "C for 2 min following splitless injection of 1 p1 aliquots of extracts, then programmed to 320 "C at 25 "C min-'. The injec- tion port and GC/MS interfaces were held at 250 "C and 300 "C, respectively. To minimize contamination of the injector, the septum sweep valve was kept open at all times, allowing a helium flow rate of 5 ml min-' across the septum. The split valve was closed imme- diately prior to injection and was opened after 1 min. Under these conditions the PFB esters of indomethacin and d,-indomethacin had retention times of 5.53 and 5.52 min, respectively.
Extraction and derivatization procedure
To 1 ml of the appropriate biological fluid was added 0.1 ml of water which contained nominally 6 ng d,-indomethacin. This solution was passed through a Sep-Pak C18 (Millipore-Waters) as per the manufac- turer's instructions. Synovial fluid was diluted with four volumes of distilled water before passing through the Sep-Pak C18. The Sep-Pak C18 was eluted with meth- anol and the methanol evaporated to dryness. The residue was dissolved in 5 p1 of dimethylformamide (DMF), treated with 5 p1 of 0.04 M tetra- ethylammonium hydroxide in methanol and 5 p1 of PFB bromide, vortex mixed for 60 s then evaporated to dryness. Water (100 pl) and hexane (200 pl) were added to the residue and vortex mixed for 60 s. Of the hexane layer 150 p1 were transferred to a clean vial and evapo- rated to approximately 10 pl, 1 p1 of this was injected onto the gas chromatograph/tandem mass spectrom- eter. Standard solutions of the PFB esters of indo- methacin and d,-indomethacin were prepared using the same derivatization procedure.
Collection of patient samples
Samples of synovial fluid were obtained by a 'no touch' technique through the contralateral side of the knee. A local anaesthetic was used to anaesthetize the area around the sampling site. Blood was collected by vene- puncture of an arm vein. Blood and synovial fluid samples were centrifuged and the supernatants (plasma in the case of blood) were transferred to sterile poly- propylene tubes, stored on ice and frozen within 4 h of collection at - 20 "C until assayed.
RESULTS AND DISCUSSION
The effect of source temperature on the ionization spectrum of the PFB ester of indomethacin
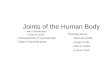
The mass spectrum of the PFB ester of indomethacin was studied at source temperatures of 100, 120, 140, 160 and 180°C. This derivative does not give a molecular ion in NICI but produces an abundant ion correspond- ing to loss of the PFB group. Ion abundance data for m/z 356 (the 35Cl indomethacin anion) and m/z 312 (loss of CO, from the indomethacin anion), plus total ion abundance in the range m/z 50-400, appears in Table 1. Figure 2 shows the NICI mass spectrum of the PFB ester of indomethacin at a source temperature of 140 "C.
As the source temperature was raised from 100 to 160°C the total ion abundance increased by a factor of 1.7. The abundance of m/z 356, the base peak (corresponding to the 35Cl isotope peak of the indo- methacin anion), increased slightly as the source tem- perature was raised to 140 "C and then decreased as the source temperature was raised further. The increase in total ion abundance observed with increasing source temperature was accounted for by fragmentation of m/z 356 to ions including m/z 312 which increased in abun- dance when the source temperature was raised. When the source temperature, reached 180 "C m/z 312 became the base peak. For further development of the assay 140 "C was selected as the optimum source temperature.
The effect of collision pressure and collision energy on ion abundance and fragmentation of the 35CI indomethacin anion
The mass spectrum of the daughter ions of m/z 356 was obtained at collision energies of 0, 5, 10, 15, 20, 25 and 30 eV with 0.15, 0.20 and 0.25 Pa collision pressure fol- lowing injection of 10 ng of the PFB ester of indo- methacin onto the GC column.
Table 1. The effect of source temperature on the abun- dance of selected ions in the methane NICI mass spectrum of the PFB ester of indometha- cin
Temperature ("C) m/z 31 2 m/z 356 Total ion abundance
100 6216 117504 237 824 120 9168 135468 283 136 140 17888 139008 340 480
406 01 6 160 54336 130944 180 120576 80384 410112

QUANTITATION OF INDOMETHACIN
m e -
58.8-
455
r
-
181 312 . 218
111 196 I
Figure 2. The NlCl mass spectrum of the PFB ester of indomethacin.
Tables 2, 3 and 4 show the total ion abundance and the ion abundances of m/z 356 (the parent ion) and m/z 312 (the daughter ion of m/z 356 formed by loss of CO,) under each set of CAD conditions studied.
Figure 3 shows the ion abundances for mlz 312 under the different collision conditions studied.
Figure 4 shows the daughter spectrum of m/z 356 at a collision pressure of 0.20 Pa and 5 eV. Under these con- ditions the fragmentation of m/z 356 is incomplete and the major ion formed is m/z 312.
Table 2. The effect of collision energy on ion abundance at a collision pressure of 0.15 Pa
Collision energy (eV) mlz 312 m p 356 Total ion abundance
0 86917 68809 165 581 5 156398 93404 267 760
10 226161 25129 291 111 15 146790 5000 193 759 20 61 667 2038 121 418 25 35 282 900 103 677 30 11 744 0 72 843
Table 3. The effect of collision energy on ion abundance at a collision pressure of 0.20 Pa
Collision energy (eV) m/z 312 m/z 356 Total ion abundance
0 111044 34816 171 150 5 248451 65536 351 947
10 316166 24477 403 284 15 115637 800 22 160 20 29 805 0 1 35 080 25 4 320 0 90912 30 1560 0 57 236
Table 4. The effect of collision energy on ion abundances at a collision pressure of 0.25 Pa
Collision energy (eV) m/z 312 mlz 356 Total ion abundance
0 103837 28480 155 724 5 216060 46720 303 31 5
10 284574 14416 390 603 15 139 963 400 311 149 20 24 389 0 197 833 25 1799 0 118158 30 0 0 67 486
3
0 0.15 b o 0.20 Pa x 0.25Pa
Collision energy W )
Figure 3. The ion abundance for m/z 312 at different collision energies and pressures.

456
100.8 -
50.0 -
M. DAWSON, M. D. SMITH AND C. M. McGEE
-
-
312 lee.8-
50.8-
356 297 278
255 I 282
Figure 5 shows the daughter spectrum of m/z 356 at a collision pressure of 0.20 Pa and 30 eV. Under these conditions no parent at m/z 356 is observed and the peak at m/z 312 accounts for less than 3% of the total ion abundance. The ions at m/z 297 and m/z 282 corre- spond to successive losses of CH, from the decarboxyl- ated indomethacin anion, m/z 158 to loss of C,H,03'C1 and CH, from the decarboxylated indomethacin anion and m/z 11 1 to C6H,35C1.
Although complete fragmentation occurs at high col- lision energies and collision pressures, these conditions do not provide the optimum sensitivity for CAD quan- titative analyses for indomethacin. Inspection of Fig. 3
r
-
lm-.I 50.0
100.0
1
1
M/Z 50 100 282 282
2r
shows that the most sensitivity is obtained at a collision energy of 10 eV and a collision pressure of 0.2 Pa.
Analyses were performed by selected ion monitoring of the ions at m/z 312 and m/z 316 formed by CAD of [M3'Cl - PFBI- and [(2H2)-M37C1 - PFBl-, respec- tively, at 10 eV and 0.2 Pa.
Assay validation
The assay was validated by assaying five replicates at concentrations of 0.1, 1.0 and 10 ng ml-', for both the biological fluids studied.
c
Figure 5. The daughter spectrum of m/z 356 at 30 eV and 0.20 Pa.

QUANTITATION OF INDOMETHACIN
lee.&
312 -
457
13599. 16116. 7328.
312.893 f 8.588
227 1274.
I 72 274 87. 174. 1p. I I . - - A 211. - ,
_ I _ & . . 1 - 1 - 8 , I
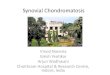
Figure& I n chr
258 55616. 1191a7. I 55616.
matograrns for m/z 312 and 316 obtained following analysis of a plasma sample containing 0.1 ng ml-’ of indornethacin asdescribed in the text.
The coefficients of variation at the three concentra- tions were 16.1%, 6.1% and 6.4%, respectively, for plasma, and 18.1%, 3.2% and 8.9%, respectively, for synovial fluid. The limit of quantification was set at that defined by the Australian Department of Community Services and Health for the minimum quantifiable con- centration in bioavailability studies, i.e. ‘the lowest con- centration which has a coefficient of variation of < 20%’.
sample analyses
Calibration curves were constructed for each run by assaying six indomethacin-spiked standards for both plasma and synovial fluid. Concentrations used were 2.0, 1.5, 1.0, 0.5, 0.25, 0.1 and 0 ng ml-’. For each run, three quality-control samples spiked at 1.0 ng ml- ’ were also extracted and assayed during the run. Every tenth injection was a standard containing indomethacin and the internal standard. A typical regression line was y = 0.7298~ + 0.0303, r = 0.9983. Ion ratios for m/z 312/316 varied by less than 4% between analytical runs for each standard concentration examined. Figure 6 shows the ion chromatograms for m/z 312 and m/z 316 obtained when a sample of plasma containing 0.1 ng ml- of indomethacin was assayed using the method- ology described above; the peaks eluting at scan number 258 in the traces shown correspond to indo- methacin and the internal standard.
Data treatment
Least-squares regression analysis (using an Apple Macintosh program) was used to construct the standard curve. The concentration of indomethacin in the plasma and synovial fluid samples was obtained by inter- polation.
Table 5. Plasma and synovial fluid indG metbacin concentrations following application of Indospray@’ to an inflamed knee
lndomethacin con- lndomethacin con- Time centration (ng rn-’). centratdon (ng ml-‘), (h) synovial fluid plasma
0 ND ND 2 ND 0.3 5.0 0.1 0.7 6.92 1 .o
12.5 0.4 1.3 24.5 2.2 4.9
ND = less than the timit of quantification; - = no sample.
-
Assay of patient plasma and synovial fluid samples
The assay methodology proved satisfactory for the quantitative analysis of indomethacin in 84 plasma and 84 synovial fluid samples from patients who had been treated with 1 ml of a 3% indomethacin solution which was applied to an area of the knee of approximately 50 cm’. The plasma and synovial fluid concentrations detected in one of the subjects enrolled in the study are shown in Table 5.
A detailed description of the plasma and synovial fluid concentrations of indomethacin following topical administration of the solution to seven subjects will be presented elsewhere.
CONCLUSION
The stable isotope dilution GC/NICI/MS/MS assay described here is a sensitive and specific means of quan- tifying indomethacin in plasma and synovial fluid fol- lowing topical administration of the drug.

458 M. DAWSON, M. D. SMITH AND C. M. McGEE
The concentrations of indomethacin detected in the plasma and synovial fluid in this study were much lower than concentrations found in these biological fluids fol- lowing oral administration of the drug.9 The most sensi- tive assay reported in the literature has a detection limit of 2 ng ml - I , which would not have been suitable for the quantification of indomethacin in the plasma and synovial samples analysed in this study.
The processes involved in MS/MS analyses are more complex than in single-stage mass spectrometry, so to achieve optimum sensitivity in quantitative analyses, it
is important to ascertain the most appropriate MS/MS conditions for each analyte. In structure determination MS/MS studies a high degree of collision-induced disso- ciation may be desirable to facilitate the assignment of a proposed structure to an unknown compound. However, for quantitative analyses it is important to select those MS/MS conditions which yield the greatest sensitivity and, as shown in this study and our previous study,’ those conditions do not necessarily coincide with complete dissociation of the parent ion.
REFERENCES
1. P. L. Boardman and D. L. Hart, Side effects of indomethacin, Ann. Rheum. Dis. 26,127 (1976).
2. J. R. Vane, Inhibition of prostaglandin synthesis as a mecha- nism of action for asprin-like drugs, Nature 231,232 (1 971).
3. H. Pratzel, P. Dittrich and W. Kukovetz, Spontaneous and forced cutaneous absorption of indomethacin in pigs and humans, J. Rheumatol. 13,1122 (1986).
4. M. Dawson, C. M. McGee, J. H. Vine, P. Nash, T. R. Watson and P. M. Brooks, The disposition of biphenylacetic acid fol- lowing topical administration, Eur. J. Clin. Pharmacol. 33, 639 (1 988).
5. I. W. Beringer, D. A. Darsh and D. R. Fulton, The use of reversed phase cartridges (C18) in processing plasma for analysis of indomethacin by high performance liquid chroma- tography, J. Clin. Chem. Biochem. 24, 227 (1986).
6. R. J. Suhbs, M. S. Schwartz, R. Chiou, L. A. Entwistle and M.
F. Bayne, Improved method for the determination of indo- methacin in plasma and urine by reversed phase high per- formance liquid chromatography, J. Chromatogr. 383, 432 (1 986).
7. M. Dawson, J. H. Vine, C. M. McGee, P. M. Brooks and T. R. Watson, The quantitation of leukotriene 64 in synovial fluid by gas chromatography/mass spectrometry/mass spectrometry, Biomed. Environ. Mass Spectrom. 17. 205 (1 988).
8. M. Dawson, C. M. McGee, M. D. Smith and J. H. Vine, The synthesis of exchange deuterium labelled non-steroidal anti- inflammatory drugs using aluminium chloride and deuterium oxide, J. Labelled Compd. Radiopharm. 27,707 (1989).
9. H. W. Emori, G. D. Champion, R. Bluestone and H. E. Paulus, Simultaneous pharmacokinetics of indomethacin in serum and synovial fluid.Ann. Rheum. Dis. 32,433 (1 973).