Embed Size (px)
Citation preview

European Journal of Pharmacology 668 (2011) 225–232
Contents lists available at ScienceDirect
European Journal of Pharmacology
j ourna l homepage: www.e lsev ie r.com/ locate /e jphar
Cardiovascular Pharmacology
Gap junctions and hydrogen peroxide are involved in endothelium-derivedhyperpolarising responses to bradykinin in omental arteries and veins isolated frompregnant women
Stephanie Hammond a, Alastair M. Mathewson a, Philip N. Baker b, Terry M. Mayhew a, William R. Dunn a,⁎a Cardiovascular Research Group, School of Biomedical Sciences, University of Nottingham, Nottingham, NG7 2UH, United Kingdomb Faculty of Medicine and Dentistry, University of Alberta, Canada
⁎ Corresponding author at: School of Biomedical ScienNottingham, NG7 2UH, United Kingdom. Tel.: +44 1150142.
E-mail address: [email protected] (W
0014-2999/$ – see front matter © 2011 Elsevier B.V. Aldoi:10.1016/j.ejphar.2011.06.050
a b s t r a c t
a r t i c l e i n f oArticle history:Received 14 April 2011Received in revised form 9 June 2011Accepted 23 June 2011Available online 8 July 2011
Keywords:EDHFGap junctionsH2O2
EndotheliumPregnancyConnexin
Altered endothelial function may underlie human cardiovascular diseases, including hypertension, diabetesand pre-eclampsia. While much is known about endothelial function in small arteries, very little is knownabout endothelial responses in small veins isolated from humans. Therefore, we assessed endothelium-dependent responses in omental arteries and veins isolated from healthy pregnant women, focussing onendothelium-dependent hyperpolarising (EDH) mechanisms. Human omental arteries and veins wereobtained from women undergoing elective caesarean sections and examined using pressure myography. Inpressurised vessels, the effects of proposed inhibitors of EDH production/function were examined onresponses to bradykinin. The expression of connexins Cx37, 40 and 43 was assessed using immunohisto-chemistry. Bradykinin caused vasodilatation in human pressurised omental arteries and veins. In both vessels,responses to bradykinin were partially blocked in the presence of the gap junction uncoupler, carbenoxolone,and reduced further with the addition of catalase, which acts to degrade H2O2. The effect of catalase alone wasmore pronounced in venous preparations. All three connexins were expressed in both arteries and veins, witha similar distribution pattern, where Cx37 and Cx40were locatedmainly in the endothelium and Cx43 locatedmostly in the media. These data show that, in human omental vessels, an EDH mechanism is produced inresponse to bradykinin that involves gap junction communication and the production of H2O2. Thesemechanisms may be involved in the haemodynamic alterations that take place during pregnancy, and anyaberration in their function could contribute to raised blood pressure in hypertensive disorders of pregnancy,such as pre-eclampsia.
ces, University of Nottingham,823 0188; fax: +44 115 823
.R. Dunn).
l rights reserved.
© 2011 Elsevier B.V. All rights reserved.
1. Introduction
A number of factors are released from the vascular endotheliumincluding, prostacyclin, nitric oxide (NO) and a mechanism thatresults in hyperpolarisation of the underlying vascular smoothmusclecells (endothelium-derived hyperpolarisation, EDH). Several factorshave been proposed to be a transferable endothelium-derivedhyperpolarising factor (EDHF) including arachidonic acid metabolites(Campbell et al., 1996), K+ ions (Edwards et al., 1998) and hydrogenperoxide (H2O2) (Matoba et al., 2002), while there are many reportsindicating that the EDH response involves the passage of current viagap junctions (Chaytor et al., 1998; Griffith, 2004).
A role for EDHF in the human vasculature has been shown inseveral isolated arterial preparations, generally using pharmacologicaltools. In particular, raising extracellular potassium to functionally
antagonise hyperpolarising mechanisms has implicated an EDHresponse in human omental (Ohlmann et al., 1997; (Wallerstedt &Bodelsson, 1997); Wareing et al., 2006), subcutaneous (Coats et al.,2001; Lang et al., 2007; McIntyre et al., 2001) and myometrial arteries(Kenny et al., 2002a,b). In addition, sharp microelectrodes have beenused to directly measure hyperpolarisation responses in coronary(Miura and Gutterman, 1998; Nakashima et al., 1993), gastroepiploic(Urakami-Harasawa et al., 1997), subcutaneous (Buus et al., 2000)and omental arteries (Suzuki et al., 2002).
Although the pathophysiological role of EDHF remains to be fullydetermined, a lack of EDHF responses has been shown in ageing(Urakami-Harasawa et al., 1997), diabetes (Fitzgerald et al., 2005),pre-eclampsia (Kenny et al., 2002a) and in hypertension (Sunano etal., 1999). This has led to an interest in defining the factor responsiblefor mediating the EDH response in human arteries. Several candidatemolecules have been reported including, cytochrome P450 metabo-lites in subcutaneous arteries isolated from elderly volunteers (Coatset al., 2001), potassium ions in larger renal arteries (Bussemaker et al.,2003) and H2O2 in mesenteric arteries (Matoba et al., 2002). In smallmyometrial and subcutaneous arteries from pregnant women, the

-9 -8 -7 -6 -5
-9 -8 -7 -6 -5
-9 -8 -7 -6 -5
-20
0
20
40
60
80
100
120controlL-NAME
*
log [bradykinin] (M)
log [bradykinin] (M)
log [bradykinin] (M)
% m
axim
umva
sodi
lata
tion
% m
axim
umva
sodi
lata
tion
% m
axim
umva
sodi
lata
tion
-20
0
20
40
60
80
100
120controlraised extracellular K+
*
-20
0
20
40
60
80
100
120 control
L-NAME+raised extracellular K+
+
*+
+++
A
B
C
*
ARTERY
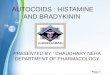
Fig. 1. Effect of, A) L-NAME (100 μM), B) raised extracellular K+ (25 mM) and C) thecombination of L-NAMEand raisedextracellularK+onvasodilator responses tobradykinininhumanpressurisedomental arteries. Eachpoint represents themean±S.E.M. (n=5–6).Statistically significant differences between the curves are indicated by * Pb0.05 (twowayANOVA). + represents a statistically significant difference (Pb0.05) between individualpoints on each curve (Bonferroni post hoc test).
226 S. Hammond et al. / European Journal of Pharmacology 668 (2011) 225–232
EDH response is mediated by gap junction communication (Kenny etal., 2002b; Lang et al., 2007; Luksha et al., 2004). Indeed, gap junctionsmay be the predominant EDH mechanism in many arterial prepara-tions, mediated by different connexin (Cx) proteins. The connexinsmost widely expressed in blood vessels are Cx37, Cx40 and Cx43 (seede Wit et al., 2006), although Cx45 and Cx32 have been reported insome blood vessels (Li and Simard, 2001; Okamoto et al., 2009).
Although a picture is emerging about the role of EDHF in humanarteries, much less is known about the nature of EDHF responses inhuman veins. This is surprising since altered endothelial function inveins will profoundly influence venous return, cardiac output andsubsequently blood pressure. An EDHFmechanism has been shown topartly mediate responses to substance P in omental veins isolatedfrom aged patients although the underlying mechanism was notcharacterised (Wallerstedt and Bodelsson, 1997). Therefore, thepresent study assessed endothelial function and the associatedmechanisms in human omental veins and to compare these responseswith the function of small arteries isolated from the same vascularbed.
2. Materials and methods
2.1. Ethical permission
Ethical permission for the study was obtained from the Notting-ham Regional Ethics Committee and all subjects had given informedwritten consent to participation.
The study included 72 normotensive women, who deliveredsingleton foetuses by elective lower segment Caesarean section atterm, shown subsequently to be above the tenth centile of birthweight for gestational age. The women were undergoing Caesareansection for reasons such as breech or transverse presentation, placentapraevia, previous Caesarean section or maternal request.
Following the delivery of the baby and placenta, a 1 cm3 biopsy ofomentumwas taken and placed in freshly-prepared physiological saltsolution (PSS) at 4 °C. With the use of a stereomicroscope, arteries ofdiameter ranging from 100 to 400 μm, and veins of diameter rangingfrom 300 to 600 μm were dissected free of the surrounding tissue.
2.2. Pressure myography
Dissected vessels were cleaned of any connective tissue andsecured between two glass cannulae of a pressure myograph (LivingSystems Instrumentation, Burlington, VT, USA). One end of the vesselwas mounted on a cannula which was attached to a pressure-servosystem containing PSS, allowing the precise control of the intralum-inal pressure and thus the measurement of diameter changes underisobaric conditions. Any blood was flushed from the lumen and thevessel was mounted on the other cannula and checked for leaks.Vessels were superfused with PSS gassed with 5% CO2 95% O2 and thetemperature of the organ bath was maintained at 37 °C. The vesselswere imaged using a video camera and the diameter was measuredwith the use of a dimension analyser (Living Systems Instrumenta-tion, Burlington, VT, USA), which was linked to a PowerLab dataacquisition system. All experiments were performed in the presenceof indomethacin (10−6 M).
The intraluminal pressurewas set at 40 mm Hg for arteries (a valueapproximately 40–50% of mean arterial pressure) and 10 mm Hg forveins, and vessels were allowed to equilibrate for 60 min. Neitherveins nor arteries developed myogenic tone under these conditions.Thereafter, vessel diameter was reduced to approximately 50% of theoriginal diameter by exposure to the thromboxane mimetic U46619.Following the development of stable contractile tone, cumulativeconcentration response curves to bradykinin were constructed byadding it to the external superfusing solution. Responses to bradykininwere assessed in the absence and presence of L-nitro arginine methyl
ester (L-NAME, 100 μM) in consecutive concentration response curves.L-NAME was present for at least 30 min before vessels were pre-constricted with U46619 and responses to bradykinin were obtained.In some experiments, the effects of inducing tone (50% reduction indiameter) with raised extracellular K+ (25 mM in arteries, 40 mM inveins) on responses to bradykinin were determined 45 min aftergenerating an initial concentration-response curve to bradykinin inthe presence of U46619-induced tone.
All subsequent experiments were carried out in the presence of L-NAME (100 μM). Thereafter, responses to bradykinin were obtainedbefore and 45 min after exposure to raised extracellular K+,carbenoxolone (100 μM) (Kenny et al., 2002b) or catalase (3000–4000 U/ml (arteries and veins respectively)) (Matoba et al., 2002). Ina further set of experiments, responses to bradykinin were assessedfollowing combined treatment with carbenoxolone (100 μM) andcatalase (3000–4000 U/ml). All drugs were added to the externalsuperfusing solution. At the end of each experiment, the maximumvessel diameter was determined in arteries exposed to calcium-freePSS.

ARTERY
-20
0
20
40
60
80
100
120
++ +
L-NAME
*
VEIN
-20
0
20
40
60
80
100
120
L-NAME
L-NAME+carbenoxolone
*
-9 -8 -7 -6 -5
log [bradykinin] (M)
-9 -8 -7 -6 -5
log [bradykinin] (M)%
max
imum
vaso
dila
tatio
n%
max
imum
vaso
dila
tatio
n
A
B
L-NAME + Carbenoxolone
Fig. 3. Effect of the gap junction uncoupler, carbenoxolone (100 μM) on the vasodilatorresponse to bradykinin, in the presence of L-NAME, in human pressurised omental A)arteries andB)veins, pre-constrictedwithU46619. Eachpoint represents themean±S.E.M.(n=5–6). Statistically significant differences between the curves are indicated by * Pb0.05(two way ANOVA). + represents a statistically significant difference (Pb0.05) betweenindividual points on each curve (Bonferroni post hoc test).
-20
0
20
40
60
80
100
120control
L-NAME
*
++
control
raised extracellular K +
control
L-NAME+raised extracellular K+
++++
+
-9 -8 -7 -6 -5
log [bradykinin] (M)
% m
axim
umva
sodi
lata
tion
-20
0
20
40
60
80
100
120
-9 -8 -7 -6 -5
log [bradykinin] (M)
-9 -8 -7 -6 -5
log [bradykinin] (M)
% m
axim
umva
sodi
lata
tion
-20
0
20
40
60
80
100
120
% m
axim
umva
sodi
lata
tion
*
A
B
C
VEIN
Fig. 2. Effect of, A) L-NAME (100 μM), B) raised extracellular K+ (40 mM) and C) thecombination of L-NAMEand raisedextracellularK+onvasodilator responses to bradykininin human pressurised omental veins. Each point represents the mean±S.E.M. (n=5–6).Statistically significant differences between the curves are indicated by * Pb0.05 (twowayANOVA). + represents a statistically significant difference (Pb0.05) between individualpoints on each curve (Bonferroni post hoc test).
227S. Hammond et al. / European Journal of Pharmacology 668 (2011) 225–232
2.3. Immunostaining
The vessels were frozen in optimum cutting compound (OCT)using isopentane that had been super-cooled to −40 °C using liquidnitrogen. The frozen samples were cut into sections approximately 5–10 μm thick using a cryostat (Leica) with the cutting arm set to−18°,and the surrounding air to −15 °C.
The sections were washed using phosphate-buffered salinesolution (PBS), and 4% paraformaldehyde (PFA) was applied for5 min to fix the tissue. The PFA was then washed off using PBS. Ablocking solution composed of fish skin gelatine and Triton X100 wasapplied for 30 min to prevent non-specific staining and then drainedoff. The primary antibodies were diluted in the blocking solution tothe following dilutions: 1:200 (Cx37), 1:50 (Cx40) and 1:100 (Cx43).The slides were then placed in a humidity chamber and the primaryantibodies were applied to the sections and left to bind overnight(17 h). No primary antibody was applied to the negative control. Theexcess primary antibody was removed the following day by washing
with PBS. The secondary antibody, biotinylated goat anti-rabbit, wasdiluted to 1:100 or 1:50 (depending on the batch) in blocking solutionand applied to the sections for 1 h. The excess secondary antibodywasthen removed by washing with PBS. The fluorescent tertiary antibodycomplex, Streptavidin TRITC, was diluted to 1:500 or 1:200 (depend-ing on the batch) using blocking solution. The diluted tertiaryantibody was applied to the sections and the slides placed in ahumidity chamber which was then covered in aluminium foil toprevent bleaching of the TRITC marker. After 1 h, the excess antibodywas removed by washing with PBS. Coverslips were applied usingmounting medium containing the nuclear stain, DAPI, and anti-fade.
2.4. Confocal microscopy
The immunostained sections were viewed using a filter-freeconfocal microscope (Leica TCS SPZ AOBS). Sections were viewed ateither ×20, ×40 or ×63 magnification depending on the size of thevessel section. A wavelength of 410 nm to 520 nm was used to viewDAPI, which fluoresces blue, and a wavelength of 570 nm to 620 nmwas used to view TRITC, which fluoresces red. Images were recordedfrom approximately 20 planes through the section and thenreconstructed to form the final image.
2.5. Drugs and solutions
The composition of PSS was as follows: NaCl 118 mM, NaHCO3
25 mM, glucose 11.1 mM, KCl 4.8 mM, MgSO4 2.5 mM, KH2PO4
1.2 mM and CaCl2 1.25 mM. The composition of Ca2+-free PSS wasas above with the omission of CaCl2 and the addition of EGTA(0.5 mM). High-K+ PSS was prepared by equimolar replacement of

ARTERY
L
SM
E
E
S
L
L
E
S
a
b
c
d
Fig. 4. Representative cross-sections of human omental arteries (HOA) labelled with secondary antibody and tertiary complex viewed using Leica TCS SP2 AOBS confocal microscope(one of six repeats). Endothelial cell nuclei and SM cells stain blue with Hoechst dye and with antibodies against b) Cx37 (1:100), c) Cx40 (1:50) and d) Cx43 (1:100) in comparisonto tissues that were not exposed to a primary Cx antibody, control a). E = endothelium, L = lumen, SM = smooth muscle, small arrows indicate endothelial cell nuclei.
228 S. Hammond et al. / European Journal of Pharmacology 668 (2011) 225–232
NaCl with KCl. Bradykinin, L-NAME, carbenoxolone, catalase andindomethacin were obtained from Sigma, UK. All drugs were freshlyprepared in PSS from stock solutions on the day of use and thendiscarded. Catalase was prepared directly in PSS at the finalconcentration (3000 U/ml or 4000 U/ml respectively). Indomethacinwas prepared in ethanol. The final bath concentration of ethanol didnot exceed 0.01% (v/v) and did not affect vascular function.
PBS (Oxoid Ltd, Basingstoke, Hampshire, England): 1 tablet per100 ml distilled water. 4% PFA: paraformaldehyde, sodium hydroxide(BHD, VWR International Ltd, Poole, England) and distilled water.Blocking solution: 1% fish skin gelatine and 0.2% Triton X100 (Sigma-Aldrich, Poole, Dorset, UK) in 100 ml PBS.
Primary antibodies: (rabbit polyclonal) Cx37-rabbit anti-mouse16aa peptide C-terminal cytoplasmic (AlphaDiagnostics, CX37A11-A).Cx40-rabbit anti-mouse 19aa C-terminal cytoplasmic (Chemicon,AB1726). Cx43-rabbit anti-rat 3rd cytoplasmic domain C-terminal(Zymed, 71-0700). Secondary antibody: biotinylated goat anti-rabbitIgG (H+L) conjugate (Zymed, 81-6140). Tertiary antibody: strepta-vidin TRITC (Zymed, 43-4314). Mounting medium: Vectashield withDAPI (Vector Laboratories, H-1200).
2.6. Data analysis
Vasoconstrictor tonewas calculated as the % reduction in the initialvessel diameter. Vasodilator responses to bradykinin were expressedas percentages of the maximum possible vasodilator range i.e. the
difference in vessel diameter in Ca2+-free PSS and after thedevelopment of stable vasoconstrictor tone. Results are presented asmean±standard error of mean (S.E.M.). Rmax refers to the maximumvasodilator response obtained to bradykinin. Statistical analysis wasperformed using GraphPad Prism (GraphPad Software Inc, La Jolla,USA). LogEC50's were calculated for individual concentration responsecurves using nonlinear regression (sigmoidal dose–response). Differ-ences in logEC50's and maximum vasodilator response (Rmax) werecompared using a paired Student's t-test. Differences in thebradykinin concentration-response curves before and after drugintervention were assessed using a repeated measures two-wayanalysis of variance (ANOVA) with the Bonferroni post-hoc test. Aprobability level of Pb0.05 was considered as statistically significant.
3. Results
3.1. Vasodilator responses
Bradykinin caused a concentration-dependent vasodilator re-sponse in pre-constricted human omental arteries (Fig. 1). Consecu-tive concentration-response curves were reproducible (data notshown). The NO synthase inhibitor, L-NAME (100 μM) significantlyattenuated responses to bradykinin (Fig. 1A), while raising extracel-lular potassium (+25 mM) caused a modest inhibition of bradykinin-induced vasodilatation (Fig. 1B). The combination of L-NAME andraised extracellular potassium virtually abolished responses to

229S. Hammond et al. / European Journal of Pharmacology 668 (2011) 225–232
bradykinin (Fig. 1C). Responses to bradykinin were reproducible withtime (data not shown).
Similarly, bradykinin caused a concentration-dependent vasodila-tor response in pre-constricted human omental veins, with a similarsensitivity to that seen in arteries (Fig. 2). Venous responses werepartly sensitive to L-NAME (Fig. 2A), but unaffected by the raisedextracellular potassium alone (+40 mM) (Fig. 2B). The combinationof L-NAME and raised extracellular potassium virtually abolishedresponses to bradykinin (Fig. 2C).
To assess the potential role of gap junctions in mediating the L-NAME resistant (EDHF-mediated) response in omental arteries andveins, responses to bradykinin were examined in the presence of L-NAME with or without carbenoxolone (100 μM). Carbenoxolonesignificantly decreased the size of the maximum response tobradykinin, mediated by EDHF, from 67±4% to 41±11% (Pb0.05;n=5; Fig. 3A) and in omental veins from 42±2% to 30±3% (Fig. 3B).
3.2. Immunostaining
Fig. 4a shows a representative example of a confocal image of thenegative control sample for connexin staining in a human omentalartery. The blue staining shows the location of cell nuclei using DAPI,allowing localisation of endothelial cells (closest to the lumen) andsmooth muscle cells in the media, of which there are between 3 and 4layers. Cx37 staining is shown by bright red staining (Fig. 4b). Thebrightest staining was localised around the cells closest to the lumen,reflecting expression in endothelial cells with the brightest staininglocated on the media side of these cells (inset). There was a morediffuse pattern of fluorescence in the media. Cx40 staining was alsomost apparent in endothelial rather than smooth muscle cells(Fig. 4c). The punctate nature of this staining was apparent in most
Fig. 5. Representative cross-sections of human omental veins (HOV) labelled with secondar(one of six repeats). Endothelial cell nuclei and SM cells stain blue with Hoechst dye and withto tissues that were not exposed to a primary Cx antibody, control a). E = endothelium, L
endothelial cells and localised to the external part of the cell, mostprobably at the membrane. Cx43 staining was more evident in themedia of omental arteries (Fig. 4d). The bright staining surroundingthe nuclei suggests a cytosolic location for this connexin (Fig. 4d,inset). In some, but not all endothelial cells, there was a modestamount of red fluorescence.
Detailed assessment of connexin staining was less easy to performin the omental veins since they tended to collapse and lose shapeduring processing. However, the pattern of connexin expressionfollowed a similar distribution to that observed in arteries with Cx37and Cx40 predominantly located in the endothelium and Cx43 locatedprincipally in the media (Fig. 5).
3.3. Effect of combined inhibition of gap junctions and H2O2 productionon vasodilator responses to bradykinin
In the presence of L-NAME (100 μM), catalase (3000 U/ml) did notsignificantly affect the sensitivity (log EC50 : control,−7.54±0.21 M;catalase, −7.07±0.32 M; n=5; Fig. 6A) or maximum response tobradykinin in human omental artery. In the presence of carbenox-olone in addition to catalase, responses to bradykinin were virtuallyabolished (Fig. 6B). In human omental veins, catalase significantlyattenuated responses to bradykinin (Fig. 6C), while the combinationof catalase and carbenoxolone was more effective at reducing EDHF-mediated responses to bradykinin than either agent alone (Fig. 6D).
4. Discussion
The present study examined vasodilator responses to bradykinin inpressurised omental arteries and veins isolated from pregnant women.In both arteries and veins, the results indicate that bradykinin can cause
y antibody and tertiary complex viewed using Leica TCS SP2 AOBS confocal microscopeantibodies against b) Cx37 (1:100), c) Cx40 (1:50) and d) Cx43 (1:100) in comparison
= lumen, SM = smooth muscle, small arrows indicate endothelial cell nuclei.

ARTERY VEIN
L-NAMEL-NAME+Catalase
L-NAME
L-NAME+catalase
++
*
L-NAMEL-NAME+Catalase+CBX
+ + ++
*
L-NAME
L-NAME+catalase+CBX
++
+ *
-9 -8 -7 -6 -5
log [bradykinin] (M)-9 -8 -7 -6 -5
log [bradykinin] (M)
-9 -8 -7 -6 -5
log [bradykinin] (M)-9 -8 -7 -6 -5
log [bradykinin] (M)
% m
axim
umva
sodi
lata
tion
-20
0
20
40
60
80
100
120%
max
imum
vaso
dila
tatio
n
-20
0
20
40
60
80
100
120
% m
axim
umva
sodi
lata
tion
-20
0
20
40
60
80
100
120
% m
axim
umva
sodi
lata
tion
-20
0
20
40
60
80
100
120A
B D
C
Fig. 6. Effect of catalase (3000–4000 U/ml) alone (A and C) and the combination of catalase and carbenoxolone (100 μM) (B and D) on vasodilator responses to bradykinin, in thepresence of L-NAME, in human pressurised omental arteries (A and B) and veins (C and D) pre-constricted with U46619. Each point represents themean±S.E.M. (n=4). Statisticallysignificant differences between the curves are indicated by * Pb0.05 (twoway ANOVA). + represents a statistically significant difference (Pb0.05) between individual points on eachcurve (Bonferroni post hoc test).
230 S. Hammond et al. / European Journal of Pharmacology 668 (2011) 225–232
the release of NO and cause hyperpolarisation via an EDH mechanism.The EDH response involves both gap junction communication and theproduction of H2O2. The former mechanismmay involve the connexinsCx37, Cx40 or Cx43 which are present in these blood vessels.
Pharmacologically, EDHF responses are defined by their resistanceto combined inhibition of the NO synthase and cyclo-oxygenaseenzymes. In the current study, all the functional experiments wereconducted in the presence of indomethacin, to exclude any influenceof cyclo-oxygenase products. Human omental arteries and veinsshowed a similar pattern of responses after inhibition of NO synthaseand after functionally inhibiting hyperpolarising mechanisms byraising the level of extracellular potassium. In both vessels, L-NAMEreduced responses to bradykinin indicating the involvement of NO.However, a large residual response remained. Raising extracellularpotassium produced only a modest attenuation of the response tobradykinin in human omental arteries and veins but the combinationof raising extracellular potassium and L-NAME virtually abolishedbradykinin-mediated vasodilatation. These observations indicate thatresponses to bradykinin were mediated by the combination of bothNO and an EDHmechanism. The large residual response to bradykininin the presence of raised extracellular potassium alone or L-NAMEalone indicates that either NO or EDH is capable of generating a largeresponse in the absence of the other endothelium-dependentvasodilator mechanism. A NO synthase-resistant response to brady-kinin or acetylcholine has been reported previously in isometrically-mounted omental arteries from pregnant women (Knock and Poston,1996; Pascoal and Umans, 1996; Suzuki et al., 2000).
EDH-type responses in small arteries isolated from pregnantwomen have been shown to involve gap junction communication asdetermined by the effects of gap junction uncouplers such as 18-α-GA
and carbenoxolone in myometrial and subcutaneous arteries (Kennyet al., 2002b; Luksha et al., 2004) and the use of more specific peptideinhibitors of connexins in subcutaneous arteries (Lang et al., 2007). Inthe present study, the gap junctional inhibitor, carbenoxoloneproduced a partial inhibition of the concentration-response curve tobradykinin in both omental arteries and veins. These observationsindicate some involvement of gap junctions in mediating EDHresponses in both omental arteries and veins as has been reportedin myometrial and subcutaneous arteries from pregnant women,respectively (Kenny et al., 2002b; Lang et al., 2007; Luksha et al.,2004) and in non pregnant human mesenteric arteries (Matoba et al.,2002).
There is a high degree of variability in the distribution of Cxsubtypes in blood vessels isolated from animals, although in generalCx37 and Cx40 tend to be associated with the endothelium, and thelatter has been localised to myoendothelial gap junctions andproposed to mediate EDH responses (de Wit et al., 2006; Mather etal., 2005). Few studies have mapped the expression of connexins insmall blood vessels isolated from humans. However, Lang et al. (2007)have shown that Cx37, Cx40 and Cx43 are expressed in humansubcutaneous arteries isolated from pregnant women. Each connexinwas found in both the endothelium and media, although Cx40 wasprincipally found on the endothelium as was Cx37 and there wasabundant expression of Cx43 in the media. In the present study, theconnexin distribution in omental arteries was similar with Cx37 andCx40mostly located in the endothelium and Cx43mostly found in themedia. The Cx43 also seemed to be in the cell cytosol rather thandiscretely located on the plasmamembrane. It is possible that the Cx43is undergoing vesicular trafficking in our vessels as has been reportedin rat aortic A7r5 smooth muscle cells (Martin et al., 2004).

231S. Hammond et al. / European Journal of Pharmacology 668 (2011) 225–232
Interestingly, Lang et al. (2007) concluded that Cx43was the dominantconnexin subtype involved in mediating the myoendothelial gap-junction-mediated EDHF response in subcutaneous arteries on thebasis that EDHF-responses were more sensitive to putatively selectivegap junction inhibitors of Cx43, compared to inhibitors generatedagainst Cx37 or Cx40. We have additionally shown that Cx37, 40 and43 are expressed in human omental small veins with a similardistribution to that seen in small omental arteries.
The relatively small inhibitory effects of carbenoxolone in omentalarteries and veins could be taken as evidence that gap junctions arenot particularly important in mediating the EDH response in thesevessels. However, the true extent of the involvement of gap junctionswasmore evident when carbenoxolone was used in combination withcatalase, which degrades H2O2, since inhibition of both mechanismsproduced a larger effect than either alone, suggesting that they cancompensate for one another.
H2O2 was first proposed to be an EDHF in mouse mesenteric smallarteries on the basis that the EDHF-mediated relaxant response andhyperpolarisation were abolished by catalase. In these vessels, AChwas shown to stimulate the production of H2O2 from endothelial cellsand exogenous H2O2was shown to cause a hyperpolarisation (Matobaet al., 2000). Since then, H2O2 has been proposed to be an EDHF inseveral blood vessels isolated from humans including mesenteric(Matoba et al., 2002) and coronary arterioles (Miura et al., 2003). In thepresent study, catalase alone did not affect the vasodilator response tobradykinin in omental arteries. This could indicate that H2O2 is notinvolved in mediating endothelium-dependent responses in humanomental arteries isolated from pregnantwomen. However, when usedin combination with the gap junction uncoupler, carbenoxolone, thevasodilatation produced by bradykinin was abolished. By contrast,catalase alone reduced responses to bradykinin in omental veins,while the combination of catalase and carbenoxolone was moreeffective than either agent alone. These data indicate that both gapjunctions and H2O2 are involved in mediating the hyperpolarisationresponse to bradykinin in these vessels but that H2O2 may play a moreimportant role in small veins. When either gap junctions or H2O2 areinactive, then the alternative hyperpolarising mechanism remainsintact to mediate the vasodilator response. While our observationsmay indicate that H2O2 acts as an EDHF in human omental smallarteries, it has been suggested that H2O2 causes the release of anunidentified substance from the endothelium of human submucosalintestinal microvessels, which then acts to cause hyperpolarisation,rather than H2O2 being an EDHF itself (Hatoum et al., 2005).
In summary, in human omental arteries and veins isolated frompregnant women, bradykinin can cause the release of NO and causeEDH. The EDH response involves both gap junction communicationand the production of H2O2. The formermechanismmay be associatedwith gap junctions formed by the connexins Cx37, Cx40 or Cx43whichare present in these blood vessels. A lack of expression of connexinsmay be associated with the reduced gap junction-mediated EDHresponse seen in arteries isolated from women with pre-eclampsia(Kenny et al., 2002a; Luksha et al., 2008; Pascoal et al., 1998).
Acknowledgements
This work was supported, in part, by a grant from the WellcomeTrust (069781). SH gratefully acknowledges receipt of an ASGBI PhDstudentship. The authors thank Kelly-Ann Vere for expert technicalsupport with confocal microscopy.
References
Bussemaker, E., Popp, R., Binder, J., Busse, R., Fleming, I., 2003. Characterization of theendothelium-derived hyperpolarizing factor (EDHF) response in the humaninterlobular artery. Kidney Int. 63, 1749–1755.
Buus, N.H., Simonsen, U., Pilegaard, H.K., Mulvany, M.J., 2000. Nitric oxide, prostanoidand non-NO, non-prostanoid involvement in acetylcholine relaxation of isolatedhuman small arteries. Br. J. Pharmacol. 129, 184–192.
Campbell, W.B., Gebremedhin, D., Pratt, P.F., Harder, D.R., 1996. Identification of epoxy-eicosatrienoic acids as endothelium-derived hyperpolarizing factors. Circ. Res. 78,415–423.
Chaytor, A.T., Evans, W.H., Griffith, T.M., 1998. Central role of heterocellular gapjunctional communication in endothelium-dependent relaxations of rabbitarteries. J. Physiol. 508, 561–573.
Coats, P., Johnston, F., MacDonald, J., McMurray, J.J., Hillier, C., 2001. Endothelium-derived hyperpolarizing factor : identification and mechanisms of action in humansubcutaneous resistance arteries. Circulation 103, 1702–1708.
de Wit, C., Hoepfl, B., Wölfle, S.E., 2006. Endothelial mediators and communicationthrough vascular gap junctions. Biol. Chem. 387, 3–9.
Edwards, G., Dora, K.A., Gardener, M.J., Garland, C.J., Weston, A.H., 1998. K+ is anendothelium-derived hyperpolarizing factor in rat arteries. Nature 396, 269–272.
Fitzgerald, S.M., Kemp-Harper, B.K., Tare, M., Parkington, H.C., 2005. Role ofendothelium-derived hyperpolarizing factor in endothelial dysfunction duringdiabetes. Clin. Exp. Pharmacol. Physiol. 32, 482–487.
Griffith, T., 2004. Endothelium-dependent smooth muscle hyperpolarization: do gapjunctions provide a unifying hypothesis? Br. J. Pharmacol. 141, 881–903.
Hatoum, O.A., Binion, D.G., Miura, H., Telford, G., Otterson, M.F., Gutterman, D.D., 2005.Role of hydrogen peroxide in ACh-induced dilation of human submucosal intestinalmicrovessels. Am. J. Physiol. 288, H48–H54.
Kenny, L.C., Baker, P.N., Kendall, D.A., Randall, M.D., Dunn, W.R., 2002a. Differentialmechanisms of endothelium-dependent vasodilator responses in humanmyometrialsmall arteries in normal pregnancy and pre-eclampsia. Clin. Sci. (Lond.) 103, 67–73.
Kenny, L.C., Baker, P.N., Kendall, D.A., Randall, M.D., Dunn, W.R., 2002b. The role of gapjunctions in mediating endothelium-dependent responses to bradykinin inmyometrial small arteries isolated from pregnant women. Br. J. Pharmacol. 136,1085–1088.
Knock, G.A., Poston, L., 1996. Bradykinin-mediated relaxation of isolated maternalresistance arteries in normal pregnancy and preeclampsia. Am. J. Obstet. Gynecol.175, 1668–1674.
Lang, N.N., Luksha, L., Newby, D.E., Kublickiene, K., 2007. Connexin 43mediates endothelium-derived hyperpolarising factor-induced vasodilatation in subcutaneous resistancearteries from healthy pregnant women. Am. J. Physiol. 292, H1026–H1032.
Li, X., Simard, J.M., 2001. Connexin45 gap junction channels in rat cerebral vascularsmooth muscle cells. Am. J. Physiol. 281, H1890–H1898.
Luksha, L., Nisell, H., Kublickiene, K., 2004. Themechanism of EDHF-mediated responsesin subcutaneous small arteries from healthy pregnant women. Am. J. Physiol. 286,R1102–R1109.
Luksha, L., Nisell, H., Luksha, N., Kublickas, M., Hultenby, K., Kublickiene, K., 2008.Endothelium-derived hyperpolarizing factor in pre-eclampsia: heterogeneouscontribution, mechanisms, and morphological prerequisites. Am. J. Physiol. 294,R510–R519.
Martin, P.E.M., Hill, N.S., Kristensen, B., Errington, R.J., Griffith, T.M., 2004. Ouabainexerts biphasic effects on connexin functionality and expression in vascular smoothmuscle cells. Br. J. Pharmacol. 141, 374–384.
Mather, S., Dora, K.A., Sandow, S.L., Winter, P., Garland, C.J., 2005. Rapid endothelial cell-selective loading of connexin 40 antibody blocks endothelium-derived hyperpo-larizing factor dilation in rat small mesenteric arteries. Circ. Res. 97, 399–407.
Matoba, T., Shimokawa, H., Nakishima, M., Hirakawa, Y., Mukai, Y., Hirano, K., Kanaide,H., Takeshita, A., 2000. Hydrogen peroxide is an endothelium-derived hyperpolar-ising factor in mice. J. Clin. Invest. 106, 1521–1530.
Matoba, T., Shimokawa, H., Kubota, H., Morikawa, K., Fujiki, T., Kunihiro, I., Mukai, Y.,Hirakawa, Y., Takeshita, A., 2002. Hydrogen peroxide is an endothelium-derivedhyperpolarizing factor in human mesenteric arteries. Biochem. Biophys. Res.Commun. 290, 909–913.
McIntyre, C.A., Buckley, C.H., Jones, G.C., Sandeep, T.C., Andrews, R.C., Elliot, A.I., Gray, G.A.,Williams, B.C., McKnight, J.A., Walker, B.R., Hadoke, P.W., 2001. Endothelium-derivedhyperpolarizing factor and potassium use different mechanisms to induce relaxation ofhuman subcutaneous resistance arteries. Br. J. Pharmacol. 133, 902–908.
Miura, H., Gutterman, D.D., 1998. Human coronary arteriolar dilation to arachidonicacid depends on cytochrome P450 monooxygenase and Ca2+-activated K+
channels. Circ. Res. 83, 501–507.Miura, H., Bosnjak, J.J., Ning, G., Saito, T., Miura, M., Gutterman, D.D., 2003. Role for
hydrogen peroxide in flow-induced dilation of human coronary arterioles. Circ. Res.92, e31–e40.
Nakashima, M., Mombouli, J.V., Taylor, A.A., Vanhoutte, P.M., 1993. Endothelium-dependent hyperpolarization caused by bradykinin in human coronary arteries. J.Clin. Invest. 92, 2867–2871.
Ohlmann, P., Martinez, M.C., Schneider, F., Stoclet, J.C., Andriantsitohaina, R., 1997.Characterization of endothelium-derived relaxing factors released by bradykinin inhuman resistance arteries. Br. J. Pharmacol. 121, 657–664.
Okamoto, T., Akiyama,M., Takeda,M., Gabazza, E.C., Hayashi, T., Suzuki, K., 2009. Connexin32is expressed in vascular endothelial cells and participates in gap-junction intercellularcommunication. Biochem. Biophys. Res. Commun. 382, 264–268.
Pascoal, I.F., Umans, J.G., 1996. Effect of pregnancy on mechanisms of relaxation inhuman omental microvessels. Hypertension 28, 183–187.
Pascoal, I.F., Lindheimer, M.D., Nalbantian-Brandt, C., Umans, J.G., 1998. Preeclampsiaselectively impairs endothelium-dependent relaxation and leads to oscillatoryactivity in small omental arteries. J. Clin. Invest. 101, 464–470.
Sunano, S., Watanabe, H., Tanaka, S., Sekiguchi, F., Shimmura, K., 1999. Endothelium-derived relaxing, contracting and hyperpolarizing factors of mesenteric arteries ofhypertensive and normotensive rats. Br. J. Pharmacol. 126, 709–716.

232 S. Hammond et al. / European Journal of Pharmacology 668 (2011) 225–232
Suzuki, Y., Kajikuri, J., Suzumori, K., Itoh, T., 2000. Mechanisms underlying the reducedendothelium-dependent relaxation in human omental resistance artery in pre-eclampsia. J. Physiol. 527, 163–174.
Suzuki, Y., Hattori, T., Kajikuri, J., Yamamoto, T., Suzumori, K., Itoh, T., 2002. Reducedfunction of endothelial prostacyclin in human omental resistance arteries in pre-eclampsia. J. Physiol. 545, 269–277.
Urakami-Harasawa, L., Shimokawa, H., Nakashima, M., Egashira, K., Takeshita, A., 1997.Importance of endothelium-derived hyperpolarizing factor in human arteries. J.Clin. Invest. 100, 2793–2799.
Wallerstedt, S.M., Bodelsson, M., 1997. Endothelium-dependent relaxation by sub-stance P in human isolated omental arteries and veins: relative contribution ofprostanoids, nitric oxide and hyperpolarization. Br. J. Pharmacol. 120, 25–30.
Wareing, M., Myers, J.E., O'Hara, M., Kenny, L.C., Taggart, M.J., Skillern, L., Machin, I.,Baker, P.N., 2006. Phosphodiesterase-5 inhibitors and omental and placental smallartery function in normal pregnancy and pre-eclampsia. Eur. J. Obstet. Gynecol.Reprod. Biol. 127, 41–49.