Embed Size (px)
Citation preview

ctin. exp. Immunot. (t99l) 85, 109-113 ADONIS 000991049100202S
Gamma/delta T cells and the diagnosis of coeliac disease
J. SPENCER, P. G. ISAACSON, T. T. MACDONALDt, A. J. THOMAS* & J. A. WALKER-SMITH*Department of Histopathologv. University College and Middle.sex School of Medicine. Bland Sutton Institute. London.
* Academic Unit of Paediatric Gastroenterology. Queen Elizabeth Ho.spital For Children, London, andfSt Bartholomew's Hospital. London. England
(Acceptedfor publieation 28 January 1991 j
SUMMARY
Gamma/delta T cells are increased in the gut epithelium ofpatients with coeliac disease comparedwith normal controls. The aim of this study was to determine whether the inerease in yS intraepitheliallymphocytes (lEL) is specific for coeliac disease, in which ease it could be of diagnostic importance.Biopsies were obtained from children with no intestinal disease, coeliac disease, cow-milk-sensitiveenteropathy/post-enteritis syndrome (CMSE/PES) and miscellaneous other enteropathies (« = 67).Intraepithelial CD3 * and yd T cells were identified in frozen sections using peroxidase immunohisto-chemistry. In normal biopsies there were 0-7 y5 IEL/100 cells in ihe epithelium. In untreated coeliacpatients this increased to 9-22 yS IEL/100 cells in the epithelium (P = 0()t)0004). Of 27 patients withmorphologic intestinal damage which was not due to coeliac disease, four with CMSE/PES had y6IEL/100 cells in the epithelium in the same range as the patients with coeliac disease. Of these, two hadhigh densities of CD3 * IEL in the epithelium and were indistinguishable from patients with untreatedcoeliac disease. The other two could be excluded as possible coeliacs because their CD3 ^ IEL/100epithelial cells were in the normal range. Thus an increase in yS IEL is not specific for coeliac disease.However, enumeration of both of yS IEL and CD3 ' IEL densities will be useful in the exclusion ofcoeliac disease as a diagnosis In some children.
Keywords intraepithelial lymphocytes coeliac disease T eell receptors yS T cells
INTRODUCTION
The diagnosis of coeliac disease in childhood, as defined by theoriginal ESPGAN criteria (Meeuwisse. 1970). is a time-consum-ing process. Il involves an initial small intestinal biopsy, asecond small intestinal biopsy following clinical remission on agluten-free diet, and at least a third biopsy to show smallintestinal mucosal damage after gluten challenge. Such damagemay take many months to develop, so fourth and even fifthbiopsies may be required to finally establish the diagnosis. Thusan alternative means of diagnosing coeliac disease would be ofparticular advantage to obviate the need for repeat invasiveprocedures in ehildren. Definitive diagnosis of coeliac disease isof particular importance in children under 2 years of agebecause there are several other causes of small intestinalenteropathy apart from coeliac disease, including cow-milk-sensitive enteropathy. post-enteritis syndrome and a variety ofinfectious agents (Walker-Smith et al. 1990). Previously pro-posed methods of differentially diagnosing coeliac disease haveincluded analysis of IgA anti-gliadin antibodies (Savilahti et al..
Correspondence: Dr Jo Spencer, Departmenl of Histopathology.University College and Middlesex School of Medicine. Bland SuttonInstitute. Riding House Si, London WCIP 7PN. UK.
1983), anti-retieuHn (Unsworth, Walker-Smith & Holborow,1983) and IgA anti-endomysium antibodies (Chozelski et al.,1984). bui these are not specific for coeliac disease. A recentproposal is that glulen challenge be made rectally, where it iseasier to take biopsies (Loft. Marsh & Crowe, 1990). However.the effectiveness of using this technique to diagnose coeliacdisease in children is not known.
The possibility of diagnosing coeliac disease by studying theintraepithelial lymphocyte (IEL) population was studied, and ilwas shown that milolic figures are more commonly seen in thejejunal lELof patients with coeliac disease than those with non-coeliac enteropathies (Marsh, 1982; Marsh & Haeney. 1983).However, this technique has failed to gain general acceptance. Ithas recently been shown by several groups that yd T cells areincreased in frequency in the IEL population ofpatients withcoeliac disease (Spencer et al., 1989; Halstensen, Scott &Brandtzaeg, 1989; Savilahti, Arato & Verkasalo, 1990). It hasbeen suggested thai if the increase in yS T cells is specific forcoeliac disease, this could be a significant aid to diagnosis(Walker-Smilh et al.. 1990). Previous studies have comparedcoeliac disease with normal biopsies or inappropriate diseasecontrols (e.g. infiammatory bowel disease) so that it has nolbeen established whether enumeration of yd T cells wouldindeed be diagnostically useful.
109

10 J. Spencer et al.
The aim of this study was therefore to compare yd T eells inthe gul epithelium in a large series of biopsies from children inwiom subsequent clinical diagnoses were made, to determineW'lcther this would enable an early and reliable diagnosis ofcceliae disease to be made using a single initial biopsy.
SUBJECT AND METHODS
Tissue cottection and ProcessingSmall intestinal biopsies were obtained using a double-portpaediatrie Crosby eapsule from patients with a elinieal historysuggestive of eoeliae disease. Unless otherwise stated, paiientswi:re on normal diets at the time of biopsy. Half of eaeh biopsywas fixed and processed for routine histology and half was snapfrozen and stored in liquid nitrogen for study of surfacemarkers.
Patients wtth coetiac disease {n = 12)Ail patients in this group were diagnosed as having coeliacdisease aecording to the revised ESPGAN criteria (Walker-Smith ('/ at., 1990), Eight were on normal diets and four were ongluten-free diets at the time of biopsy. The mean age of thepatients on normal diets was 4 years and 7 months {range I yearard 1 month-9 years and 11 months) and of patients on gluten-free diets, 4 years and 2 months (range 1 year and 5 months-8 years and 6 months).
Patients with htstotogicatly normal biopsies (n = 2S).H stologically, normality was defined in paraffin sections asvi4us:crypt ratio of 3:1 or more, and no abnormality of thebrush border at the villous tips. Ten patients were diagnosed ashaving toddlers' diarrhoea, four post-enteritis syndrome(resolved), 10 failure to thrive (unknown cause), one multiplefood allergy, one egg allergy, one lactose intolerance and oneilcal stenosis. The mean age of the patients was 2 years andK! months (range 4 months-13 years).
Patients with cow-milk-sensitiie enteropathy and post-enteritissyndrome (CMSEjPES) (n = !8)Fifteen of these biopsies showed partial villous atrophy, twoshowed patehy partial villous atrophy, and one showed severevillous atrophy. It was impossible to separate the patients in thisgroup into those sensitive to cows' milk and those with PESbecause both conditions may be transient and indeed may co-exist, preeluding accurate clinical diagnosis (Walker-Smith,1988), All were treated with and responded to a cow-milk-freediet but in none were serial biopsies related to milk eliminationor challenge performed (Walker-Smith et al.., 1978). Crypto-sporidia were isolated from the stools and biopsies of two ofthese patients. The mean age of patients in this group was 10months (range 3 months-4 years and 7 months).
Pi'tients with miscettaneous idiopathie enteropathies {n = 9)Six biopsies showed partial villous atrophy and three biopsiesshowed patchy partial villous atrophy. Two patients weredi:ignosed as having idiopathic colitis, three idiopathic entero-ptithy. one intractable diarrhoea of infancy, one eosinophilicgastroenteritis, one failure to thrive (unknown eause),, onegluten allergy (Rudd, Manuel & Walker-Smith, 1981). Meanage was 3 years and 1 month (range 3 months-12 years and6 months).
ImmunocytochemistryImmunohistological studies were carried out on 8 /im acetone-fixed sections of snap-frozen jejunal biopsies. The followingprimary antibodies were used: CD3 (Dako, High Wyeombe,UK) whieh is expressed on all T cells and TCR^I (T CellSeiences, Cambridge, MA) whieh reeognizes all yd T cells.Following incubation in primary anlibody. peroxidase-con-jugated rabbii anti-mouse immunoglobulin was applied to thesections and the peroxidase activity was visualized usingdiamino benzidine substrate.
Quantification of I ELThe density ofcells expressing CD3 or TCR^I in the epitheliumwas determined by counting Ihe number of stained cells as apercentage ofthe total eells in the epithelium, both lymphoidand epithelial. Counts were made on serial sections, in triplicate.using x400 total magnifieation. [EL per IOO total celts in theepithelium were quantified, because in frozen sections it is notalways possible to tell whether a negative cell is epithelial orlymphoid. Only cells in the surface epithelium were eounted.Based on the densities of CD3 * lEL and y6 IEL/100 cells in theepithehum. the frequency of v<5 lEL in the CD3 population wasdeduced.
Statistical analysisData from all groups were tested to determine whether (heyeonformed to samples taken from a normally distributedpopulation. Data from the group of normal biopsies were notnormally distributed and thus statistical comparisons weremade using the Mann-Whitney f/-tesl.
RESULTS
The density of CD3 * IEL in eaeh patient was determined(Fig. la). As expected, patients with eoeliae disease had a higherdensity of CD3* IEL than any other group (coeliac diseasever.sus normal. /* = 4 3xlO ^ eoeliae disease ler.sus CMSE/PES, /• — I 9 X 10 ; eoeliae disease rersus miseellanous biopsiesP ^ 3-8 X 10 •'). However, there was some overlap in that four ofthe normal patients and four of the patients with CMSE/PEShad CD3* IEL densities within the range seen in the eoeliaepatients.
The density oCyS IEL was next determined (Fig. Ib). Thedensity o( yS IEL was increased in untreated eoeliae patientscompared with all other groups (coeliac disease versus normal.P=4 IX 10 *; eoeliae disease t^er.sus CMSE/PES. P=4 3 X 10 *; eoeliae disease versus miscellaneous enteropathies.P — 2-7x lO""""), There was no overlap between either the normalbiopsies or the miseellaneous enteropathies with the untreatedcoeliacs. However, four ofthe 18 patients with CMSE/PES werein the range of the treated eoeliacs and details of theCD3* andyS IEL densities, and the frequency of yS CD3 ' IEL of thesefour patients are shown in Table I. In the two wilh the highestvalues. CD3 * IEL were also high, thus these were indistinguish-able from untreated coeliac disease. In the other two wilh onlyslightly raised values, the CD3+ IEL density was normal thusexcluding coeliac disease.
Four patients with treated eoeliae disease were studied. Inthe two with the highest densities of CD3 ' IEL, the density of"/(')IEL was in the range seen in untreated coeliaes. In the two wilhIhe lowest densities of CD3 + IEL the density of yd IEL was inthe range seen in the nonnal biopsies (Fig. 2).

yS T ceiis and the diagnosis of eoeliae disease 111
70
60
50
40
30
20
10
0
( Q )
25-
20
15
10
5
(b)
IOO,
80
60
40
20
(c)
Normal Untreoiedcoeliac
Treatedcoeltac
CMSE/PES Miscellaneous
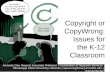
Fig. I. Scatter-plots showing (a) CD3+ intra-epiihelial lymphocytes(IEL)/100 cells in the epitheliutn; (b) TCR^I* IEL/100 cells in theepi[helium;and(c)TCR<*r IEL/100 CD3^- cells in ihe epithelium, innormal biopsies (n = 28), biopsies from untreated coeliacs (n = 8),treated coeiiacs (H = 4) . cow-m ilk-sensitive enteropathies and/or post-enteritis syndrome (CMSE/PES) (n=18), and miscellaneous otherenteropathies (« = 9).
Table I. Densities of CD3+ and TCRtil + intra-epithelial lymphocytes(IEL) and the frequency or CD3+ IEL expressing TCRtil in Tourpatienis with cow-milk-scnsitivc enteropathy/post-enteritis syndrome(CMSE/PES) with y6 T cell densities within the range seen in coeliac
disease
Palient withCMSE/PES
I234
C D 3 ' IEL/100 cells inepithelium
17-617-731-7326
TC:R(Jr IEL/IOO cells inepithelium
9 381
166149
TCR51I00CD3 +
52-845'852'445-7
VIEL
The frequency of CD3' IEL expressing yd was then deduced(Fig, lc). The frequency in untreated coeliac disease wasincreased compared with normal biopsies {P = 0Q02). CMSE/PES (P = 0047) and miscellaneous enteropathies (^ = 0002).Patients with CMSE/PES had a higher frequency of CD3+ IELexpressing yd than did normal controls (P=003). It was alsonoticeable that this measurement did not distinguish betweencoeliacs and normals since seven of the normal biopsies had afrequency of yd !EL as high or even higher than the untreatedcoeliacs. These patients, however, had a low densities of bothCD3+IEL/100 cells in the epithelium and v<5 IEL/100 cells in theepithelium, and nonnal mucosal morphology. By deduction,therefore, these patients must be relatively lacking in lELexpressing cxji T cell receptor. Eight ofthe patienis with CMSE/PES also had frequencies of i'(5 IEL/100 CD3 ' cells comparableto untreated coeliacs.
DISCUSSION
This study shows, as we and others have shown previously, thatthere is an increase in yS IEL in small intestinal biopsies ofpatients with untreated coeliac disease compared with patientswith normal biopsies (Spencer et al., 1989; Halstensen et al.,1989; Savilhati et al.. 1990), This is apparent both in lerms ofdensity of y^ IEL in the epithelium and in the frequency of ydIEL in theCD3 ' IEL populalion. We now show that y<S IEL arealso increased in the biopsies of some patienis with CMSE/PES,which also have high densities of IEL and which histologicallymost closely resemble coeliac disease, Ofthe 27 patients studiedwith CMSE/PES or miscellaneous other entcropathies, all ofwhom had various degrees of histotogical abnormality, two inthe CMSE/PES group had an increased density of CD3 ' IEL,an increased density of )'( IEL, and a high frequency ofyS IEL inthe CD3' IEL population. Both of these biopsies were thusindistinguishable from biopsies from patients with coeliacdisease. One of these paiienis had cryptosporidiosis and theother improved on a cow-milk-free diet. Since CMSE/PES is themost important dilferential diagnosis of coeliac disease inchildren, the failure of yS T cells to distinguish Ihese childrenfrom true coeliacs is disappointing. Nevertheless, the fact that 25out of 27 patients with morphologic intestinal damage could beexcluded as coeliacs demonstrates that yd T cells can be used toexclude coeliac disease in most cases-
Other investigators have reported that patients wilh coeliacdisease on gluten-free diets retain a high density of yd IEL(Halstensen et al.. 1989; Savilhati et al.. 1990). Ofthe patientswith coeliac disease on gluten-free diels in this study, tworetained a high density of yti IEL. However, these patients alsohad high densities of CD3' lEL/IOOcells in the epithelium. Thetwo coeliac patients on gluten-free diets in this study with IELdensities within normal range also had normal densities of ydIEL, We therefore propose that if the IEL density ofa coeliacpatient decreases, then the yS IEL density also decreases. Usingdouble immunofluorescence, Halstensen et al. (1990) showeddirectly thai the population of CD3' IEL expressing ydincreases in coeliac disease. The increase in yS T cells in coeliacdisease exceeds the increase in a/J T cells so that the increase in ydIEL observed in coeliac disease is disproportionate and does nolmerely reflect an increase in the density of IEL. The reasons forthis are unknown.

;. 2. Pluiui iniciographsof nuiiiial siiuill inicstinc (a. b). untreated cut-liaCMiiiail iiilcbline (t'- »J). treated coeliac small inlesiini; (e. t ) iijideow-milk-sensitive enteropathies and/or post-enleritis syndrome (CMSE/PES) small intestine with a high density or CD.1' andTC"R,51 + IEL (g. h). stained with CD3 (a. c. e. g) and TCR<^ 1 {b. d, f. h), lEL expressing JCK61 are increased in density and iti Trcquencywithin the CD3-^ IEL populalion in both coeliac disease and the case of CMSE/PES illustrated. The case of treated coeliac diseaseillustrated has normal levels ol CD3+ and TCR< I * IEL. Sections cand d and e and fare frotn biopsies taken from the same patient onnormal and giuten-free diet, respectively, Immunoperoxidase staining; magnification x 160.

yS Tcells and the diagnosis of coeliac disease 113
Enumeration of y^* and CD3 ••" IEL in a single initial biopsywill be of use in the diagnosis ofcoeliac disease. A low density ofyd IEL in a patient with a high CD3* IEL density will enablecoeliac disease to be excluded, A high density of^yS IEL will notallow a positive diagnosis of coeliac disease to be made,however, as this is occasionally seen in other enteropathies.
ACKNOWLEDGMENTSWe are grateful to Mr Alan Phillips for his help in collecting biopsyspecimens. This work was supported by the Medical Research Councilof Great Britain and the Wellcome Trust,
REFERENCESCHOZELSKI, T ,P . , BEUTNER, D , H . , SULEJ, J,, TCHORZEWSKA, H. , JAB-
LONSKA. S,. KUMAR, V, & KAPUSCINSKA, A,, (1984) IgA anti-endomysium antibody, Br. J. Dermalol. I l l , 395.
HALSTENSEN, T.S.. SCOTT, H , & BRANDTZAEG, P, (1989) Intraepithelial
Tcells of the TcR y5-i-. C D 8 ~ and Vdl/JdI-l- phenotypes areincreased in coeliac disaease, Scand. J. Immunol. 30, 665.
LOFT. D.E,, MARSH. M , N , . & CROWE. P.T. (1990) Rectal glutenchallenge and the diagnosis ofcoeliac disease. Lancet, i. 1293.
MARSH. M.N, (1982) Studies of intestinal lymphoid tissue, IV. Thepredictive value of raised mitotic indices among jejunal epitheliallymphocytes in the diagnosis of gluten sensitive entcropiithy, J. clin.Ptiihoi 35, 517.
MARSH. M.N. & HAENEY, M.N. (1983) Studies of intestinal lymphoidtissue. VI. Proliferative response of small intestinal epithelial lym-
phocytes distinguishes glutcn-from non-gluten-induced entropathy,J. clin. Pathol. 36, 149.
MEEUWISSE, G . W , (1970) Diagnostic criteria in coeliac disease. Actapaedialr. Scand. 59. 461,
RUDi), P, MANUI-I,. P, & WALKER-SMITH. J. (1981) Anaphylactic shockin an infant after feeding wilh a wheat rusk, A transient phenomenon.Postgrad, med. J. 57, 794.
SAVILAHTI, E., ARATA. A, & VERKA.SAL(), M . (1990) Increased numbersof gamma/delta bearing lymphtx:ytes In the epithelium of coeliacpatients. In Advances in Mucosal Immunology (Ed. by T. T. Mac-Donald, S. J. Challacombe. P, W, Bland, C. R, Stokes. R, V. Healley& A. McI. Mowat) p,6l. Kluwer. Dordrecht,
SAVILAHTI. E,. VIANDER. M , . PERKKIO. M , . VIANIO. E,. KALIMO. K, &
REUNALA. T . (1983) IgA gliadin antibodies: a marker of mucosaidamage in childhood coeliac disease. Lancet. '\, 320,
SPENCER. J.. ISAACSON. PG,. Diss. T C , & MACLTONALD, TT , (1989)
Expression of disulphide linked and non-disulphide linked forms ofthe T eel! receptor gamma/delta heterodimer in human intestinalintraepithelial lymphocytes. Eur. J. Immunol. 19, 1335,
UNSWORTH, D.J., WALKER-SMITH, J.A. & HOLBOROW, E.J. (1983)
Gliadin and reticulin antibodies in childhood coeliac disease. Lancet,i, 874,
WALKER-SMITH, J.A. (1988) Diseases of the Small Iniesiine in ChiklhoocI3rd edn. Butterworth, London.
WALKER-SMITH. J ,A . . GUANDALINI. S,, SCHMITZ. J., SCHMERLING. D , H ,
& ViSAKORPi. J,K. (1990) Revised criteria for the diagnosis of coeliacdisease. Arch. Di.\. Cluhi 65. 909,
WALKER-SMITH. J.A-. HARRISON. M , . KILBY. A,. PHILLIPS. A.D. &
FRANCE. N , (1978) COWS milk sensitive enteropalhy. Arch. Dis. Child.53, 375.