Embed Size (px)
Citation preview
G A M E C H A N G E R :
Preparing for Success With
MACRA
UPDATED WITH F INAL RULE NOVEMBER 11 , 2016

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 2
Overview
Table of contents
The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) dramatically impacts the way Medicare payments will be made as the healthcare industry continues to shift from fee-for-service to value-based care. Here, we shed light on MACRA’s key components and explore with CareSync’s founder and CEO Travis Bond how establishing compliant, full-service care coordination today can create success with MACRA tomorrow.
3How did we get here?Improved Care Through the Sharing of Health Information
14Where are we headed?Connecting CCM, Care Coordination and MACRA
6Where are we now?MACRA: A Law Paved With Good Intentions
Updated November 11, 2016

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 3
How did we get here?
IMPROVED CARE THROUGH THE
SHARING OF HEALTH
INFORMATION
In 2009, technology was improving productivity in ways we’d never imagined. Mobile devices were becoming the norm, family and friends could video conference each other from continents away, and Facebook users had already been oversharing for three years. Software solutions were so prevalent that Apple trademarked the phrase, “There’s an app for that®.” It’s amazing to think that while the most mundane details about personal lives were being shared electronically, the most important details that could save lives were not.
In a very connected world, the healthcare industry was largely disconnected. Physician offices and even hospitals weren’t adequately wired for the exchange of health information and creating a health IT infrastructure was a costly
consideration. For many physicians, the act of shifting data from paper to paperless seemed too daunting a task, let alone finding a way to pay for it. And with patient information spread among so many different providers at once, it was hard for some in healthcare to get on board with a move toward electronic health records (EHRs) or even picture how it could be accomplished.
However, as CareSync’s Founder and Chief Executive Officer Travis Bond explains, “It was becoming increasingly clear that sharing health information was vital to patient care and leveraging technology that added productivity and value to our personal lives could do the same for healthcare. To help prompt physicians out of paper silos and into EHRs, CMS did what had worked in the past: they dangled a carrot.”
Medicare EHR Incentive ProgramsThe carrot came in the form of Medicare EHR Incentive Programs. These programs were launched in stages to help providers move from Stage 1, creating the information, to Stage 2, exchanging health information, to Stage 3, focusing on improved outcomes and using
what we learned in Stage 2 to inform policy decisions for Stage 3.
The first stage established the requirements for electronically capturing clinical data and providing patients with electronic copies of their health information. Referred to

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 4
as “Meaningful Use,” the programs encouraged the adoption of new technology and gave eligible providers and hospitals incentives for using certified EHR technology to:
Improve healthcare quality, safety, and efficiency
Reduce health disparities
Engage patients and their family members
Improve care coordination and public health
Maintain the privacy and security of patient health information
As we moved into Stage 2, focus shifted to patient engagement, interoperability and health information exchange. Measures were put in place to ensure that the meaningful use of EHRs supported national interests, such as:
Achieving continuous quality improvement at the point of care
Increasing interoperable health data sharing among providers
Improving patient health outcomes and overall public health outcomes
Providing structure to how health information is exchanged
Increasing transparency and efficiency
Empowering individuals and encouraging them to be active participants in their healthcare
Providing more robust research data on health systems
There were plenty of growing pains associated with adopting EHR technology and there will continue to be pain points as we move into Stage 3. However, since that pivotal point in 2009, we’ve made a lot of progress.
Now, more than 97 percent of all hospitals and three-quarters of physician offices use EHRs, according to the Center for Medicare and Medicaid Services (CMS). Increased use of EHRs has led to many benefits, including doctors getting a more accurate picture of a patient’s overall health, the ability to swiftly and safely transmit prescriptions electronically to pharmacies, patients having direct access to their health information, and more.
The next steps with EHR technology involve transitioning from the staged Meaningful Use phase to the new program as it will look under MACRA.
EHR use as of April 2016
97% OF HOSPITALS
3/4 OF PHYSICIAN OFFICES

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 5
“When you read the list of goals associated with the meaningful use of EHR technology, you can see how they are closely tied to patient engagement, improved care, and public health outcomes,” said Bond. “These are all goals HHS has outlined for MACRA. Achieving the full potential of health IT is just one of those goals.”
According to the Office of the National Coordinator for Health Information Technology, “Having the right information at the right time supports team-based care, strong care coordination, and effective
patient and family engagement, which many provider communities have recognized are fundamental to an efficient and effective care delivery system.”
Widespread EHR adoption has, indeed, dramatically improved our ability to get the right information, into the right hands, at the right time. It has also paved the way for new programs, codes, and reimbursement models to be implemented, not the least of which are CPT Code 99490 for Chronic Care Management (CCM) and now MACRA.
WHEN YOU READ THE LIST OF GOALS ASSOCIATED WITH THE MEANINGFUL USE OF EHR TECHNOLOGY, YOU CAN SEE HOW THEY ARE CLOSELY TIED TO PATIENT ENGAGEMENT, IMPROVED CARE, AND PUBLIC HEALTH OUTCOMES — TRAVIS BOND

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 6
Where are we now?
MACRA: A LAW PAVED WITH GOOD INTENTIONS
According to HHS, MACRA “ended more than a decade of last-minute fixes and potential payment cliffs for Medicare doctors and clinicians, while making numerous improvements to America’s healthcare system.”
At the heart of this bipartisan legislation is the desire to achieve truly patient-centered care by improving the relevancy and depth of Medicare’s quality-based payments.
Under the fee-for-service approach MACRA replaces, physicians would provide a service and get paid. The more services they provided, the more money they would make. Results of patient care, good or bad, were not a factor in payment as it was about quantity rather than quality. MACRA shifts the focus from volume to value. Physicians provide a service and their payment varies based on how well they meet certain quality measures and create value for their patients.
APM
01.01.17
MIPS

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 7
MACRA FOCUS ON THREE KEY AREAS
ACHIEVE THREE HEALTHCARE GOALS
INCENTIVES
BETTER CARE
CARE DELIVERY
SMARTER SPENDING
INFORMATION SHARING
HEALTHIER PEOPLE
“There is legitimate concern that healthcare spending in the U.S. puts our national economy in jeopardy,” said Bond. “Currently, we spend 18 cents of every dollar on the delivery of healthcare and we’re on track for that number to reach 34 cents by 20401. When you consider the impact of healthcare spend reaching 34 percent of GDP with 86 percent of that spend already going to the treatment of chronic conditions2, it’s clear the trajectory we’re on can’t possibly work” and CMS is recognizing that.
By emphasizing quality over quantity, the new system pays physicians for doing what they already want to do: provide the best possible care for their patients. Care
becomes increasingly focused and individualized, health information is more easily shared (which supports the healthcare decisions of both doctors and patients), and patients get healthier and stay healthier longer. Additionally, Medicare pays for what works in the hope that we all benefit from a more enduring Medicare, and that we use the lessons we learn to turn the tide on healthcare spending.
“At CareSync, we think this shift represents the alignment of doing well by doing good, meaning that if a provider does the best thing in the interest of the patient — doing good — they’ll also do financially well,” said Bond. “I think that’s the essence and purpose of what CMS is doing here.”
At CareSync, we think this
shift represents the alignment
of doing well by doing good
1 The Economic Case for Health Care Reform, Council of Economic Advisers, Executive Office of the President, 2009 2 Total U.S. Healthcare Spending by Number of Chronic Conditions in 2010, Agency for Healthcare Research and Quality, 2010

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 8
Advanced APMs are a subset
of APMs, and let practices
earn more for taking on some
risk related to their patients’
outcomes
The Quality Payment Program (QPP)Aligned with CMS’ effort to reward better care, smarter spending, and healthier people, MACRA repeals Medicare’s flawed Sustainable Growth Rate (SGR) formula and replaces it with a new value-based reimbursement system called the Quality Payment Program (QPP).
Additionally, it streamlines physician reporting and gives providers two paths to choose from for determining how the value and quality of their care will be measured. These two paths are the Merit-Based Incentive Payment System (MIPS) and Advanced Alternative Payment Models (APMs).
Reporting as an Advanced APMAccording to CMS, “an APM is a payment approach that gives added incentive payments to provide high-quality and cost-efficient care. APMs can apply to a specific clinical condition, a care episode, or a population. Advanced APMs are a subset of APMs, and let practices earn more for taking on some risk related to their patients’ outcomes.”
In the case of reporting through the QPP as an Advanced APM, providers can earn a 5% incentive payment in 2019 for Advanced APM participation in 2017 if they receive 25% of their Medicare Part B payments through an Advanced APM or see 20% of their Medicare patients through an Advanced APM.
Reporting through MIPSThe term CMS uses for Medicare Part B providers subject to participation in MIPS is “MIPS eligible clinicians.” During the first performance year, this group includes physicians (MD/DO and DMD/DDS), physician assistants, nurse practitioners, clinical nurse specialists, and certified registered nurse anesthetists.
In future years, the HHS Secretary may expand the eligibility net to include other providers, such as physical or occupational therapists, speech-language pathologists, audiologists, nurse midwives, clinical social workers,
clinical psychologists, and dieticians and nutritional professionals.
At least initially, most Medicare providers (CMS estimates between 592,000 and 642,000 for the first performance year) will participate in the QPP by reporting through MIPS.
Eligible clinicians who do so can participate in MIPS as an individual or as a group billing through a common tax ID. If participating as a group, they would be assessed as a group practice across all four MIPS performance categories (three in 2017).

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 9
Reporting MIPS score as an individual:
If you send MIPS data in as an individual, your payment adjustment will be based on your performance.
An individual is defined as a single National Provider Identifier (NPI) tied to a single Tax Identification Number.
You’ll send your individual data for each of the MIPS categories through an electronic health record, registry, or a qualified clinical data registry.
You may also send in quality data through your routine Medicare claims process.
Reporting MIPS score as a group:
If you send your MIPS data with a group, the group will get one payment adjustment based on the group’s performance.
A group is defined as a set of clinicians (identified by their NPIs) sharing a common Tax Identification Number, no matter the specialty or practice site.
Your group will send in group-level data for each of the MIPS categories through the CMS web interface or an electronic health record, registry, or a qualified clinical data registry.
To submit data through the CMS web interface, you must register as a group by June 30, 2017.
Some providers will be exempt from MIPS:
Clinicians who are in their first year of participation in Medicare Part B
Clinicians who fall under the low-volume threshold: Clinicians who see less than or equal to 100 Medicare patients in a year or accrue less than or equal to $30,000 in Medicare Part B allowed charges in a year
Clinicians who are significantly participating in an Advanced Alternative Payment Model (APM), Qualifying APM Participants (QPs), and certain Partial Qualifying APM Participants (Partial QPs)
TO SUBMIT DATA
THROUGH THE CMS WEB
INTERFACE, YOU MUST
REGISTER AS A GROUP BY
JUNE 30, 2017

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 1 0
MIPS Performance Categories and ScoresMIPS improves and consolidates the Physician Quality Reporting System (PQRS), the Value-Based Modifier (VBM) Program, and the Medicare EHR Incentive Program into one scoring system designed to measure the care given to Medicare patients.
When reporting through MIPS, payments are determined by how well providers demonstrate success in four performance categories:
Quality, Improvement Activities, Advancing Care Information, and Cost. These four categories are weighted to determine a provider’s MIPS Composite Performance Score (CPS) of up to 100 points. This score will be used to measure a provider’s overall care delivery and compute a positive, negative, or neutral adjustment to their future Medicare payments as appropriate.
Payment Adjustments Based on MIPS ScoresMACRA requires MIPS to be budget neutral so total upward and downward adjustments will be balanced to make the average change equal 0%.
The swing in percentage for those payment adjustments is based on the relationship between the provider’s MIPS CPS and the MIPS performance threshold. If the CPS is below the performance threshold, the provider will see a negative payment adjustment, or proportional penalty. A CPS at the performance threshold will result in a neutral payment adjustment, or 0%. A CPS above the performance threshold will result in a positive payment adjustment, or incentive. The amount of adjustment will depend on how much the CPS exceeds the threshold and the overall CPS distribution.
The MIPS performance threshold will be set annually by CMS. The threshold will be based on the mean or median of the MIPS scores from all MIPS-eligible providers during a prior period (as defined by CMS). In 2019, no historical MIPS scores will be available to determine the performance threshold. In 2020, historical MIPS scores will only reflect the first year of measurement, which may or may not be very representative of the norm. So in 2019 and 2020, the first two payment years, the plan is to base the performance threshold on historical data related to the previous reporting categories and any additional factors as determined by CMS.
MIPS payment adjustments are applied to Medicare Part B payments
MIPS PAYMENT
ADJUSTMENTS ARE APPLIED
TO MEDICARE PART B
PAYMENTS TWO YEARS AFTER THE
PERFORMANCE YEAR

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 1 1
two years after the performance year. The first performance year will be 2017, with 2019 being the payment adjustment year. This means CMS will begin measuring a physician’s performance and the care data they report through MIPS from January 1, 2017 to December 31, 2017, to determine their Medicare payments beginning in 2019.
In that first payment adjustment year, 2019, depending on the variation of MIPS scores, negative adjustments can be no more than -4 percent, and positive adjustments can be no more than +4 percent.
The stakes get higher each year after that as both positive and negative adjustments will increase as follows:
Additionally, in the first five payment years of the program, the law allows for up to $500 million per year in an “exceptional performance bonus” to reward progressively high performers.
9% IN 2022
5% IN 2020
7% IN 2021
CMS ESTIMATES THAT BETWEEN 592,000 AND 642,000 ELIGIBLE CLINICIANS WILL PARTICIPATE IN MIPS DURING THE FIRST PERFORMANCE YEAR

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 1 2
Quality (60%)
Advancing Care Information (25%)
Improvement Activities (15%)
The Quality category, which replaces the PQRS, will count for 60 percent in Calendar Year (CY) 2017. Depending on how much the clinician wants to participate, they can report on
as few as one quality measure for partial credit, or on six measures or one speciality-specific set for full credit if submitting quality data as an individual physician.
For full participation in the Advancing Care Information category, which replaces the Medicare EHR Incentive Program also known as Meaningful
Use, there are five required measures. Reporting on other measures is optional.
To receive full credit in Improvement Activities, a new category, clinicians who report as an individual are required to complete four medium-weighted or two high-weighted activities.
For small practices, rural practices, or practices located in geographic health professional shortage areas (HPSAs), and non-patient facing MIPS
eligible clinicians, CMS reduces the requirement for this category to only two medium-weighted activities or one high-weighted activity.
Because improving care often involves deploying EHR technology, CMS has indicated it will designate some improvement activities as also qualifying for the Advancing Care Information score.
How MIPS Categories Will Be Weighted the First Performance Year
THE QUALITY CATEGORY,
WHICH REPLACES THE PQRS,
WILL COUNT FOR 60% IN CALENDAR YEAR 2017
DURING THE FIRST PERFORMANCE YEAR, DESIGNATED A “TRANSITION” YEAR BY CMS, THE COST CATEGORY WILL BE EXCLUDED AND THE MIPS CATEGORIES WILL BE WEIGHTED AS FOLLOWS:

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 1 3
In 2017, clinicians can earn a bonus score for improvement activities that make use of certified electronic health record technology (CEHRT) and for reporting to public health or clinical data registries. CMS
stated this reflects “the belief that the Advancing Care Information performance category should align with the other performance categories to achieve the unified goal of quality improvement.”
Cost (0%)A note about the Cost category, which replaces the VBM: Beginning with performance year 2018, the Cost performance category’s contribution to the final score will gradually increase from 0 to 30
percent by the third MIPS payment year of 2021, as required by MACRA, and the Quality category weight will decrease from 60 percent to 30 percent at the same time and by the same increments.
Pick Your Pace Options for the First Performance YearAlso during the first performance year, CMS is allowing clinicians to pick their pace for reporting through MIPS in an effort to ease the transition. The options include:
Report nothing in 2017: Receive the full negative 4 percent adjustment.
Report under MIPS for a full 90-day period or, ideally, the full year. This will maximize chances to qualify for a positive payment adjustment and the possibility to earn a bonus for “exceptional performance” (available for years 2019 through 2024, with $500 million allotted annually for this purpose). Clinicians could start collecting performance data January 1, 2017, but if they are not ready and plan to participate for at least part of the year, they can choose to start any time between January 1 and October 2, 2017. Whenever they choose to start, they will need to send in their performance data by March 31, 2018.
Report under MIPS for less than the full year, but for at least a full 90-day period, and report more than one quality measure, more than one improvement activity, or more than the required measures under the Advancing Care Information category in order to avoid a negative MIPS payment adjustment and possibly receive a positive MIPS payment adjustment if reporting MIPS score as an individual.
Report one quality measure, one improvement activity, or report the required measures of the Advancing Care Information category and avoid a negative MIPS payment adjustment if reporting MIPS score as an individual.
Participate in an Advanced Alternative Payment Model (APM) and possibly qualify for a 5 percent bonus incentive payment in 2019.
CLINICIANS COULD START
COLLECTING PERFORMANCE DATA JANUARY
1, 2017

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 1 4
Where are we headed?
CONNECTING CCM, CARE
COORDINATION AND MACRA
What began with the adoption of EHR technology, boosted by incentivizing its meaningful use, and the adoption of CCM, boosted by creating reimbursement through CPT Code 99490, now brings us to the next evolution in patient care: MACRA.
Moving into MACRA won’t be easy, instant or an immediate fix for some of the frustrations that have been built along the way.
“Change is painful,” acknowledged Bond. “In fact, many practices are still in pain from the EHR implementation phase. But the good news is there are already programs in place that can help you compliantly bridge the gap between fee-for-service and value-based care.”
As we’ve repeatedly seen in the healthcare industry, when new incentives, reimbursement models, or codes are announced, there is generally a bigger purpose behind such moves.
“If you get too focused on the protocols, you miss the purpose,” said Bond. “But when you truly understand the intention behind something, it’s a lot easier to
anticipate and appreciate the continued direction.”
Bond believes part of the reason CMS created CPT Code 99490 was to help ease providers out of the fee-for-service environment they have been operating in their entire careers into the new outcomes-based environment of MACRA.
“The spirit of what CMS is trying to accomplish with MACRA is paying providers for the value and quality of care they provide to significantly improve the value and quality of care patients receive,” said Bond. ”If that sounds like chronic care management or any other care coordination service, you’re right.”
Consider any aspect of care coordination — from creating a comprehensive care plan, implementing CCM in your practice or ensuring you’ve got compliant, shareable EHR capabilities — and you’ll see it has the potential to impact all four MIPS performance categories.
To that end, the following specifically illustrates how robust CCM and other care coordination services can be leveraged the first performance year.
G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 1 5
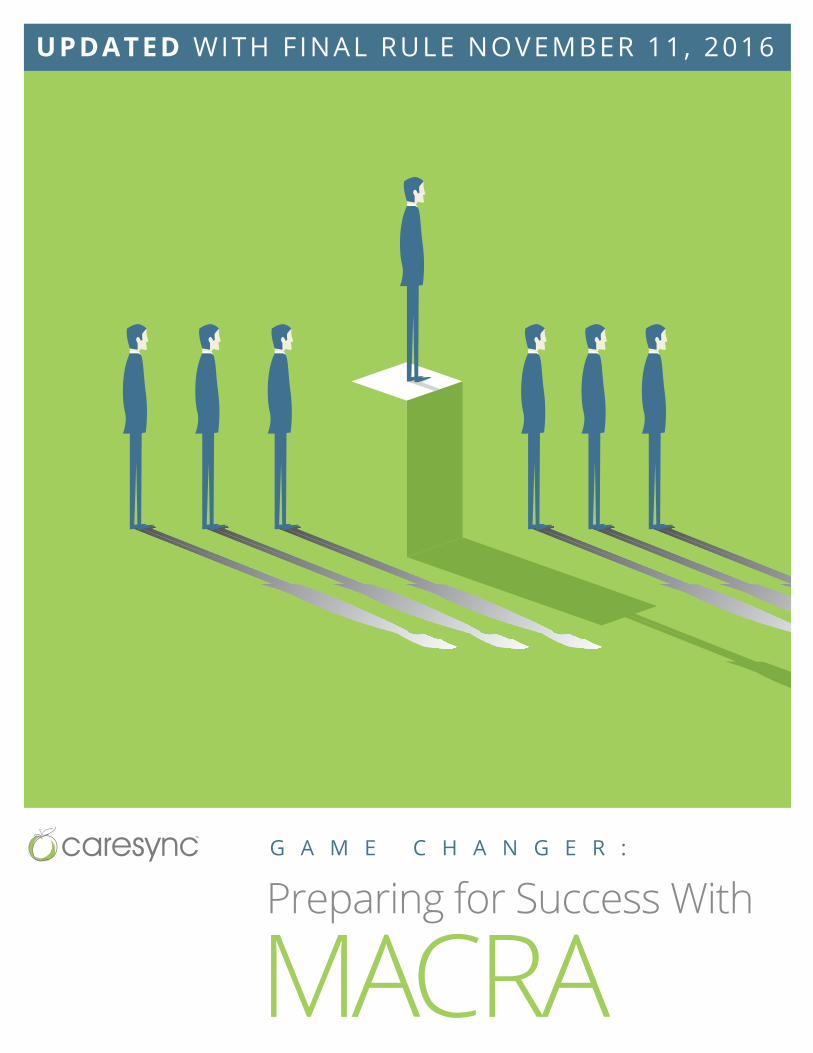
How is the MIPS journey supported by CareSync?
Quality Measures are 60% of MIPS score
CareSync can help support your practice in 16 Quality Measures
You only need 6 for full participation via the MIPS pathway
Advancing Care Information is 25% of MIPS score (replaces Meaningful Use)
CareSync can help support 3 out of 5 required measures
Security Risk Analysis and e-Prescribing are to be completed within the practice
CareSync provides 4 additional measures which can be used for additional credit
Improvement Activities are 15% of MIPS score
CareSync can help support 13 Medium-Weighted Activities and 1 High-Weighted Activity
You only need 4 Medium or 2 High-Weighted Activities for full participation via the MIPS pathway
To implement your measures and activitiesEngage your patients to help achieve better resultsNotify you of measurement and activity progressSustain the progress through ongoing CCM support
For a clinician reporting as an individual, CareSync can support you in the following ways:
If you are a group participating in MIPS or if you are participating in an Advanced APM, please contact us to learn how we can support you.
G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 1 6
ConclusionClearly, care coordination is at the core of MACRA. As a physician, you want to ask yourself if it’s at the core of your practice. How you answer that question will speak volumes about whether or not you’re prepared for what’s to come next.
Providers who delay participation in value-based care and are not prepared for the shift will face significant reductions in payment. And smaller practices, particularly those with single practitioners, could feel the biggest impact. If their low scores lead to low enough reimbursements, they could be forced to choose between joining larger groups or closing their doors.
Alternatively, providers who understand care coordination, embrace proactive between-visit care, and engage patients to become active participants in their health will be well-prepared for the changes and challenges ahead.
As Bond explained, “We like to think of it this way: Making deposits in the bank of care coordination today will build equity for success with MACRA tomorrow. If you’re looking for a smooth transition into MACRA, partnering with CareSync is a smart bet for the future.”

G A M E C H A N G E R : P R E P A R I N G F O R S U C C E S S W I T H M A C R A I 1 7
Disclaimer
At the time this white paper was published or uploaded to the web, the information, sources and links
included were current. This white paper was written to provide you with a general summary of policy and is
not intended to take the place of written laws or specific statutes as they evolve. CareSync encourages you to
visit CareSync.com and CMS.gov for updates regarding MACRA. Note: Generally, we use the term providers or
physicians in this white paper, but the terminology used in the legislation uses the phrase “eligible clinicians.”
Originally published July 14, 2016. Last updated November 11, 2016.
© CareSync 2016. All Rights Reserved.
Don’t leave your Medicare
reimbursments to chance
Choose a trusted partner with the experience, resources and proven capabilities to deliver truly compliant chronic care management and other care coordination services to your patients.
Leverage our expertise to give your organization a smooth and successful transition into CCM and MACRA. Contact us today to discuss your options and learn the many ways we can be of assistance to your practice.