Embed Size (px)
Citation preview

IJCRI – International Journal of Case Reports and Images, Vol. 2, No. 1 2, December 2011 . ISSN – [0976-31 98]
Gallstone ileus:Diagnostic and therapeutic dilemmaShireesh Saurabh, Andrew Camerota, Jeffrey Zavotsky
ABSTRACTIntroduction: Gallstone ileus is a rarecomplication of cholelithiasis but an establishedcause of mechanical bowel obstruction in theelderly. Concomitant co–morbidities arefrequent in older patients and responsible forthe high mortality rate. The aim of the presentstudy was to evaluate and discuss differentsurgical approaches and to analyze the clinicaloutcome. Case Series: Over a period of twoyears, three patients with a mean age of 78 yearspresented with complains of abdominal pain,nausea and vomiting of approximately two daysduration. Diagnosis of gallstone ileus was madeon computed tomography (CT) scan, whichshowed cholecystoenteric fistula and smallbowel obstruction at the point of impaction ofthe gallstone. All the patients underwententerolithotomy without a follow up biliary tractsurgery. The postoperative course wasuneventful in all the cases. Conclusion:Gallstone ileus is a rare condition, occurring inelderly with multiple comorbidities. Theappropriate surgical intervention remains
controversial. Enterolithotomy alone wasperformed in all the patients with favorableoutcome.Keywords: Gallstone ileus, Cholelithiasis,Gallbladder
*********Saurabh S, Camerota A, Zavotsky J. Gallstone ileus:diagnostic and therapeutic dilemma. InternationalJournal of Case Reports and Images 2011;2(12):15.
*********doi:10.5348/ijcri20111271CS1
INTRODUCTIONGallstone ileus was first described by Bartholin in1654 [1]. It is defined as a mechanical obstruction of thegastrointestinal tract caused by the presence of agallstone in its lumen. It accounts for 1 – 4 % of all casesof mechanical intestinal obstruction and upto 25 % ofthose in patients over 65 years of age [2]. Acute orchronic cholecystitis results in extensive inflammationand adhesion between the gallbladder and thegastrointestinal tract, resulting in formation of biliaryenteric fistula [3].Gallstone ileus is associated with high morbidity andmortality as most patients are elderly with multiple comorbidities. Delay in diagnosis secondary to vaguesymptoms and signs is another reason for highmorbidity. Debate currently exists regarding theappropriate surgical strategy for emergency treatmentof gallstone ileus. Most authors recommendenterolithotomy alone on account of its lower morbidity,mortality and reports of spontaneous fistula closure [1,2, 3, 4, 5, 6].
CASE SERIES OPEN ACCESS
Shireesh Saurabh1 , Andrew Camerota2, Jeffrey Zavotsky2
Affi l iations: 1Shireesh Saurabh, Drexel University Collegeof Medicine, Broad and Vine street, Philadelphia, PA1 91 02, USA; 2St Peter’s University Hospital, 254Easton avenue, New Brunswick, NJ 08901 , USA; StPeter’s University Hospital, 254 Easton avenue, NewBrunswick, NJ 08901 , USA.Corresponding Author: Shireesh Saurabh, DrexelUniversity College of Medicine, Broad and Vinestreet, Philadelphia, PA 1 91 02, USA; Email :[email protected]
Received: 1 4 May 2011Accepted: 24 August 2011Published: 31 December 2011
IJCRI 2011 ;2(1 2):1 -5.www.ijcasereportsandimages.com Saurabh et al. 1

IJCRI – International Journal of Case Reports and Images, Vol. 2, No. 1 2, December 2011 . ISSN – [0976-31 98]
Saurabh et al. 2
CASE REPORTPatient 1: A 75yearold female presented with athree day history of diffuse abdominal pain, distension,nausea and vomiting. Past history was significant fordiabetes mellitus, hypertension, anemia andappendectomy. There was no history of biliarysymptoms. On examination patient appeareddehydrated, however her vitals were stable. Abdomenwas soft, mildly distended, diffusely tender with noperitoneal signs. Laboratory work up revealed a whiteblood count of 13,200/mm3 and liver enzymes werefound to be in the normal range. Abdominal radiographwas inconclusive and diagnosis was made on computedtomography (CT) scan, which demonstratedcholelithiasis, cholecystoduodenal fistula and smallbowel obstruction with transition point at the level ofimpaction of gallstone in distal ileum. Patient was takento the operating room for exploratory laparotomy andenterolithotomy alone was performed. Longitudinalenterotomy was closed transversely in two layers.Postoperative course was uneventful.Patient 2: A 74–yearold male presented with aone day history of diffuse abdominal pain, nausea andvomiting. Past history was significant for diabetesmellitus, hypertension, diverticulitis, total colectomyfor lower gastrointestinal bleeding and ventral hernia.On examination patient was afebrile, his vitals werestable, his abdomen was soft, mildly distended, mildlytender in right upper quadrant with no peritonealsigns.White blood count was 25,000/mm3 and liverfunction tests was within normal limits. Diagnosis ofgallstone ileus was made on abdominal CT scan, whichshowed pneumobilia, small bowel obstruction andimpacted gallstone in small bowel. Assuming that thepatient had significant adhesions from previoussurgery, a exploratory laparotomy was performed.Gallstone was found to be impacted at the site ofangulation of small bowel caused by adhesions.Enterolithotomy alone was performed to remove a 5 cmx 3 cm gallstone from proximal ileum. Postoperativecourse was uneventful.Patient 3: A 84–yearold male presented with atwo day history of abdominal pain, distension, nauseaand vomiting. Past history included coronary arterydisease, stroke, hypertension, diabetes mellitus,dementia and right hemicolectomy for colon cancer. Onexamination patients abdomen was mildly tender in theperiumblical region.Laboratory findings showed a white cell count of15,900/mm3. Electrolytes and liver enzymes werewithin the normal limits. Abdominal CT scan was usedto make the diagnosis of gallstone ileus. Patient wasadequately hydrated and taken to the operating roomfor exploratory laparotomy. Considering the longhistory of medical problems the patient had, a decisionto perform enterolithotomy alone was taken.Postoperative course was uneventful.
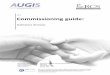
Figure 1: A) Abdominal computed tomography scan of patientshowing, cholecystoduodenal fistula (arrow) and, B) anectopic gallstone (arrow) impacting the distal ileum lumenand accompanying dilated proximal small bowel loops.
DISCUSSIONGallstone ileus as a complication of gallstone diseaseis a diagnostic as well as therapeutic challenge. It isassuming an increasing significance because of the
IJCRI 2011 ;2(1 2):1 -5.www.ijcasereportsandimages.com

IJCRI – International Journal of Case Reports and Images, Vol. 2, No. 1 2, December 2011 . ISSN – [0976-31 98]
Saurabh et al. 3
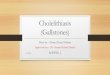
Figure 2: Demonstrates 5x3 cm gallstone within distal ileum.
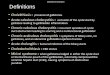
Table 1: Demographics (number of patients, mean age) and mortality rates of different operative approaches.
References Onestage (n) Mortality (%) Enterolithotomy (n) Mortality (%) Mean age1. Ramos DM, et al. (2009) 4 25 27 15 78.32. Reisner RM, et al. (1994) 13 17 801 12 _
3. Ayantunde AA, et al. (2007) 2 50 20 20 77
4. Doko M, et al. (2003) 19 11.1 11 9.1 _
5. Tan YM, et al. (2004) 12 0 7 0 74.66. Riaz N, et al. (2008) 5 0 5 0 61.87. Muthukumarasamy G, et al. (2008) 3 0 10 0 74.3
8. RodriguezSanjuan JC, et al. (1997) 9 33 16 19 75
9. Sfairi A, et al. (1997) 8 0 2 0 74.5
10. Clavien PA, et al. (1990) 8 25 6 0 78
progressive rise in the proportion of aging population inthe western world. The mean age of these patients inour study was 78 years. The median duration ofsymptoms prior to surgical intervention was three days.Most authors report a period of 3 – 5 days in averagebetween first symptoms and the time of admission [5,7]. Nonspecific symptoms are the primary cause ofdelayed diagnosis, which in turn leads to high morbidityand mortality associated with this condition. Plain
abdominal radiographs are not always conclusive,because some gallstones are not dense enough to bedetected radiologically. The classical rigler’s triad ofpneumobilia, small bowel obstruction and an ectopicgallstones are seen in less than 50 % of cases onabdominal film [5, 8, 9]. Ripolles et al. showed thatpreoperative diagnosis of gallstone ileus is increased to74 % by combining plain abdominal radiograph withultrasound [10]. An ultrasound may detect impactedstone and the site of fistula, in addition to confirmingthe presence of cholelithiasis. The use of computedtomography (CT) scan has widely been accepted as theinvestigation of choice for detection of gallstone ileus [8,9, 11]. In our case series abdominal radiograph wasinconclusive and diagnosis in all three patients wasmade by abdominal CT scan. It provides informationregarding the exact number, size and location of thegallstone. It also helps in direct visualization of thebiliary enteric fistula. Yu et al. showed an overallsensitivity, specificity and accuracy of CT scan indiagnosis of gallstone ileus to be 93%, 100% and 99%respectively [9]. CT scan helps in recognizingintraluminal stones that are nonobstructing atpresentation but can lead to recurrent gallstone ileus ona later date. Abdominal CT scan offer prompt and rapiddiagnosis of gallstone ileus, and also helps in decisionmaking for management strategy.The surgical procedure continues to be a matter ofdebate. The one stage procedure includesenterolithotomy, cholecystectomy and fistula repair. Thetwo stage procedure involves initial emergententerolithotomy followed by cholecystectomy and fistulaclosure in 4–6 weeks. However, most authors favor
IJCRI 2011 ;2(1 2):1 -5.www.ijcasereportsandimages.com

IJCRI – International Journal of Case Reports and Images, Vol. 2, No. 1 2, December 2011 . ISSN – [0976-31 98]
Saurabh et al. 4
enterolithotomy alone without a follow up biliary tractsurgery [1, 2, 3, 4, 5, 6]. In table 1 the different operativeapproaches, one stage procedure and enterolithotomyalone are compared regarding incidence and mortality.Enterolithotomy has been shown to be associated withlower morbidity and mortality, lower operative time andshorter hospital stay. A large metaanalysis by Reisner etal. showed a mortality rate of 12% for simpleenterolithotomy in comparison to 17% for one stageprocedure. Upto 50% of the biliary enteric fistula closedspontaneously and postoperative biliary symptomsrequiring surgery were seen in only 10 % patients [2].Ayantunde et al. reported lower morbidity and mortalityrate in simple enterolithotomy group, but Riaz et al.showed no difference between the two groups [3, 6].Doko et al. showed that postoperative complicationslike wound infection, wound dehiscence, myocardialinfarction, pneumonia are more likely to occur with onestage procedure when compared with simpleenterolithotomy (61.1% to 27.3%) [4]. However, fewauthors like Sfairi et al. recommend one stage procedurefor gallstone ileus to prevent future recurrence. Most ofthe patients in their study underwent one stageprocedure with no mortality. Enterolithotomy alonegroup had one mortality secondary to biliarycomplication [12].There have been several recent publicationsregarding the use of laparoscopic approach in gallstoneileus [13, 14, 15]. Moberg et al. comparedlaparoscopically assisted enterolithotomy with openshorter hospital stay for the laparoscopic group. Therewas no difference in the duration of operation betweenthe two groups [13]. However, experience withlaparoscopic enterolithotomy is limited to a very smallnumber of patients. Whether this approach will help inreducing morbidity and mortality rates requires furtherinvestigation.Based on our results and the results of other
published studies, we believe that simpleenterolithotomy should be the procedure of choice forpatients with gallstone ileus. Complications related tothe fistula are rare as most of them undergospontaneous closure and only 10% of these patients willhave postoperative biliary symptoms. One stageprocedure should be reserved only for highly selectedpatients with absolute indications like acutecholecystitis and/or gangrene of the gallbladder.
CONCLUSIONGallstone ileus is a difficult clinical entity to diagnoseand requires a high index of suspicion. Abdominal CTscan is the diagnostic modality of choice. Majority ofthese patients are elderly with multiple comorbiditiesand will benefit from relief of obstruction byenterolithotomy alone in the emergency setting. The onestage procedure should be reserved for highly selectedpatients with absolute indications.
*********
AcknowledgmentAndrew Camerota, M.D. – Provided guidance duringthe management of these patients and general supportduring writing of this paperJeffrey Zavotsky, M.D. – Provided guidance during themanagement of these patients and general supportduring writing of this paperAuthor ContributionsShireesh Saurabh – Substantial contributions toconception and design, Acquisition of data, Drafting thearticle, Revising it critically for important intellectualcontent, Final approval of the version to be publishedAndrew Camerota – Acquisition of data, Drafting thearticle, Final approval of the version to be publishedJeffrey Zavotsky – Acquisition of data, Drafting thearticle, Final approval of the version to be publishedGuarantorThe corresponding author is the guarantor ofsubmission.Conflict of InterestAuthors declare no conflict of interest.Copyright© Shireesh Saurabh et al. 2011; This article isdistributed under the terms of Creative Commonsattribution 3.0 License which permits unrestricted use,distribution and reproduction in any means providedthe original authors and original publisher are properlycredited. (Please see www.ijcasereportsandimages.com/copyrightpolicy.php for more information.)
REFERENCES1. Ramos DM, Jose JM et al: Gallstone ileus:Management options and results on a series of 40patients. Rev Esp Enferm Dig 2009; 101(2):117124.2. Reisner RM, Cohen JR: Gallstone ileus: a review of1001 reported case; Am Surg. 1994 Jun;60(6):4416.3. Ayantunde AA, Agarwal A: Gallstone Ileus:Diagnosis and Management. World J Surg 2007;31:12921297.4. Doko M, Zovak M, Kopljar M, et al. Comparison ofsurgical treatments of gallstone ileus: preliminaryreport. World J Surg 2003; 27: 400404.5. Tan YM, Wong WK. A comparision of 2 surgicalstrategies for the emergency treatment of gallstoneileus. Singapore Med J 2004; 45(2):6972.6. Riaz N, Khan MR, Tayeb M. Gallstone ileus:retrospective review of a single center’s experienceusing two surgical procedures. Singapore Med J2008; 49(8):624626.7. Haesselfeldt P, Jess P. Gallstone ileus. Acta Chir.Scand 1982; 148:431433.8. Lassandro F, Gaglardi N et al. Gallstone ileus:analysis of radiological findings in 27 patients. Eur JRadiol 2004; 50(1):232.9. Yu CV, Linn CC et al. Value of CT in diagnosis andmanagement of gallstone ileus: World JGastroenterol 2005; 11:21422147.
IJCRI 2011 ;2(1 2):1 -5.www.ijcasereportsandimages.com

IJCRI – International Journal of Case Reports and Images, Vol. 2, No. 1 2, December 2011 . ISSN – [0976-31 98]
Saurabh et al. 5IJCRI 2011 ;2(1 2):1 -5.www.ijcasereportsandimages.com
10. Ripolles T, MiguelDasit A, Errando J et al.Gallstone ileus: increased diagnostic sensitivity bycombining plain film and ultrasound. AbdomImaging 2001; 26:401405.11. Lassandro F, Romano S, Ragozzino A et al. Role ofhelical CT in diagnosis of gallstone ileus and relatedconditions. AJR 2005; 185:11591165.12. Sfairi A, Patel JC. Gallstone ileus: plea forsimultaneous treatment of obstruction and gallstonedisease. J Chir (Paris) 1997; 134(2):5964.13. Moberg AC, Montgomery A: Laparoscopicallyassisted or open enterolithotomy for gallstone ileus:Br J Surg 2007; 94(1):5357.14. Owera A, Low J: Laparoscopic Enterolithotomy forGallstone Ileus: Surg Laparosc Endosc PercutanTech 2008; 18(5):4502.15. Allen JW, McCurry T, Rivas H et al. Totallaparoscopic management of gallstone ileus. SurgEndosc 2003; 17:352.