Embed Size (px)
Citation preview

International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:100989Z01MF2019. www.ijcasereportsandimages.com
Ferreira et al. 1
CASE SERIES PEER REVIEWED | OPEN ACCESS
Gallstone Ileus – A single center case series
Manuel Alexandre Viana Ferreira, Diogo Pinto, Francisco Fazeres, Alberto Midões
ABSTRACT
Introduction: Gallstone ileus is a rare complication of cholelithiasis that accounts for 1−3% of mechanic ileus of the small bowel. It is characterized by bowel obstruction secondary to gallstone impaction that results from a migration due to the existence of a bilioenteric fistula. Gallstone Ileus is more common in the elderly with more comorbidities which leads to a high morbidity rate. Consequently, a debate exists regarding the appropriate surgical strategy for emergency treatment of gallstone ileus. The aim of the present study was to evaluate different surgical approaches based on the authors’ recent experience and to analyze the clinical outcome. Case Series: Six patients were included, all females, with a mean age of 82 years. All patients had comorbidities, specially, cardiovascular diseases. Three of them had previous history of biliary pathology. Diagnosis was confirmed through computed tomography (CT) scan in five cases. The stone was in the ileum in three, jejunum in two, and duodenum in one patient; the mean stone size was 2.5 cm. Four patients were submitted proximal to enterotomy with the removal of the gallstone, one to gastrotomy and one to cholecystectomy
Manuel Alexandre Viana Ferreira1, Diogo Pinto1, Francisco Fazeres2, Alberto Midões3
Affiliations: 1MD, Resident, General Surgery Department, Hospital de Santa Lúzia, Viana do Castelo, Portugal; 2MD, Director, Department of Gastric Surgery, Hospital de Santa Lúzia, Viana do Castelo, Portugal; 3MD, Director, General Surgery Service in the Hospital de Santa Lúzia, Viana do Castelo, Portugal.Corresponding Author: Manuel Alexandre Viana Ferreira, Rua António De Mariz, nº22, 4715-279 Braga, Portugal; Email: [email protected]
Received: 17 October 2018Accepted: 11 December 2018Published: 08 January 2019
and a cholecystoduodenal fistula closure. During the postoperative period, complications were recorded in three subjects, one patient died due to cerebrovascular accident. Conclusion: The main key in guiding patients with gallstone ileus is the timely diagnosis which is currently facilitated with the support of the use of CT scan. Taking into consideration the age and comorbidities of these patients, the surgical management should be as conservative as possible.
Keywords: Bowel obstruction, Enterolithoto-my, Gallstone ileus, Intestinal obstruction
How to cite this article
Ferreira MAV, Pinto D, Fazeres F, Midões A. Gallstone Ileus – A single center case series. Int J Case Rep Images 2019;10:100989Z01MF2019.
Article ID: 100989Z01MF2019
*********
doi: 10.5348/100989Z01MF2019CS
INTRODUCTION
Gallstone Ileus described first in 1654 by Thomas Bartholin is a rare disease that results from intestinal obstruction due to the migration of gallstones into the intestine lumen [1]. Gallstone Ileus is an unusual complication of cholelithiasis, occurring in less than 3% of patients who present with mechanical obstruction of the small bowel [2].
The inflammatory process associated with acute cholecystitis promotes adhesion of the gallbladder to the intestinal wall, leading to the formation of a cholecystoenteric fistula. This fistula is the mechanism for passage of a large gallstone capable of obstruction [2]. The most frequent fistula location occurs between the duodenum and gallbladder, due to their proximity. The

International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:100989Z01MF2019. www.ijcasereportsandimages.com
Ferreira et al. 2
stomach, small bowel and the transverse portion of the colon may also be involved [1].
It is estimated that 80% of intraluminal stones will pass spontaneously [3]. Most of the gallstones smaller than 2 or 2.5 cm may pass spontaneously through the normal gastrointestinal tract and be excreted uneventfully in the stools [1]. Usually gallstones larger than 2.5 cm will most likely cause obstruction.
Gallstone Ileus is more common in the elderly, Halabi et al recently reported an age range from 60 to 84 years in American patients. The female sex is particularly affected [1].
Symptoms of Gallstone Ileus can be nonspecific, insidious, vague and intermittent which may interfere with the diagnosis. Patients usually do not seek immediate medical attention, presenting 4 to 8 days after the beginning of symptoms, and the diagnosis is usually made 3 to 8 days after the onset of symptoms [1], so this diagnosis is usually difficult to achieve and often delayed. Consequently, this is a condition with a high morbidity and mortality rate [4].
Up to 50% of cases diagnosis is only made during exploratory laparotomy. The mainstay of treatment is removal of the obstructing stone.Fluid and electrolyte imbalances and metabolic derangements may co-exist particularly in elderly patients with pre-existing co-morbidities and need prioritized addressing before surgical intervention [1]. Debate currently exists regarding the appropriate surgical strategy for emergency treatment of gallstone ileus. Most authors recommend enterolithotomy alone because of its lower morbidity, mortality and reports of spontaneous fistula closure [5]. However, an untreated biliary-enteric fistula may lead to recurrent events of Gallstone Ileus, the risk of recurrence has been reported in 5–8% of cases [3].
We describe case series of Gallstone ileus that occurred in our hospital, as well as the diagnostic procedures, treatments and follow-up of these patients.
CASE SERIES
Six patients with obstruction induced by gallstone were included in this case series. All patients were females with a median age was 82 (76–90) years. Patients were admitted to the emergency department with the symptoms of gastrointestinal obstruction such as abdominal pain, vomiting, abdominal distension and constipation.
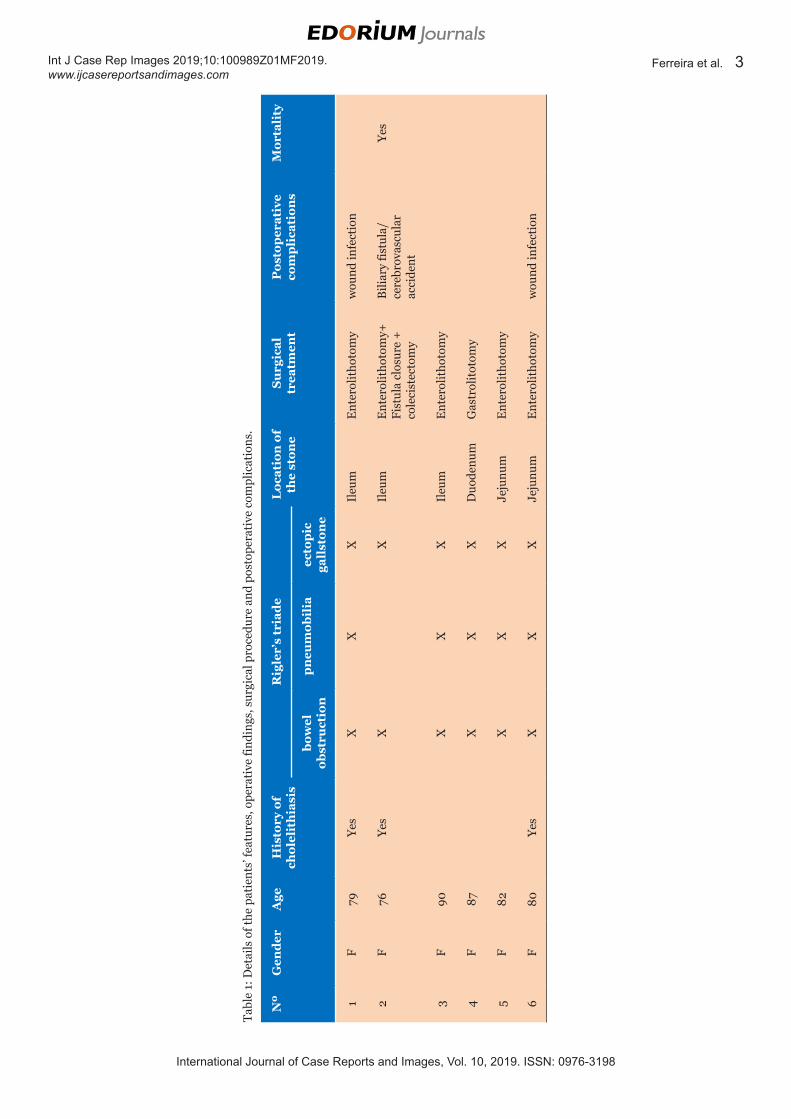
On admission, none had undergone previous biliary surgery, and only three cases (50%) had a known history of cholelithiasis. The diagnosis was successfully achieved in five patients (83.3%) before surgery, through CT scan (Figure 1), with all presenting a complete Rigler triad (Table 1).
During the surgical procedure, a stone was found in the ileum in three cases, jejunum in two (Figure 2), and duodenum in one patient; the mean stone size was 2.5
cm (2–3 cm). Four patients (66.7%) were submitted to enterotomy alone (without cholecystectomy and closure of the fistula), one (16.6%) to gastrotomy and one (16.6%) to enterotomy with cholecystectomy and a cholecystoduodenal fistula closure (Table 1).
The gallstone was manipulated in a retrograde manner into the distended proximal viscera and removed through a longitudinal enterotomy (Figure 3) or gastrotomy as previously pointed. The remaining small bowel was explored for other gallstones. When detected, they were also removed (which happened in one case). The incision was closed transversely using a single-layer suture to repair (Figure 4).
During the postoperative period, complications related to the procedure were recorded in four subjects. There was one (16.6%) perioperative mortality, due to cerebrovascular accident (details in Table 1).
Further biliary symptoms were observed in only one case (16.6%), with a patient presenting a case of cholecystitis eight months after surgery.
DISCUSSION
Gallstone ileus is an uncommon complication of gallstone disease. It is however, the most common cause of non-strangulating mechanical small bowel obstruction accounting for 1–4% of the cases [6]. As the western population continues to age, this condition will assume an increasing significance and impact, so the knowledge and revision of procedures taken, and the follow-up of the cases, that appear in our Hospital Unit is a much needed and important reflection to make, so that in the future we can perfect and enrich the service performance in this life-threatening condition [5].
As the diagnosis may be difficult additional information is required, therefore the use of plain abdominal X-ray and abdominal CT scan is a much-needed source of information.
Figure 1: (A) Axial plane of CT scan. The blue arrow shows the existence of a grossly triangular radiopaque structure in the distal portion of the jejunum, approximately 2 cm in diameter, from which an extensive collapse of the distal jejunal loops and especially of the ileum can be seen, with a marked upward gastrointestinal distension pointed by the green arrow. (B) Sagittal plane of CT scan. A moderate pneumobilia is observed, pointed by the yellow arrow. (C) Coronal plane of CT scan. The yellow arrow points the existence of pneumobilia associated with an irregularity of the lateral aspect of the first portion of the duodenum, where non-specific linear radiopaque structures were observed. Green arrow points the gastrointestinal distention proximal to the local of obstruction.
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:100989Z01MF2019. www.ijcasereportsandimages.com
Ferreira et al. 3
Tabl
e 1:
Det
ails
of t
he p
atie
nts’
feat
ures
, ope
rati
ve fi
ndin
gs, s
urgi
cal p
roce
dure
and
pos
tope
rati
ve c
ompl
icat
ions
.
Nº
Gen
der
Age
His
tory
of
chol
elit
hia
sis
Rig
ler’
s tr
iad
eL
ocat
ion
of
the
ston
eS
urg
ical
tr
eatm
ent
Pos
top
erat
ive
com
pli
cati
ons
Mor
tali
ty
bow
el
obst
ruct
ion
pn
eum
obil
iaec
top
ic
gall
ston
e
1F
79Ye
sX
XX
Ileu
mE
nter
olit
hoto
my
wou
nd in
fect
ion
2F
76Ye
sX
XIl
eum
Ent
erol
itho
tom
y+
Fist
ula
clos
ure
+
cole
cist
ecto
my
Bili
ary
fistu
la/
cere
brov
ascu
lar
acci
dent
Yes
3F
90X
XX
Ileu
mE
nter
olit
hoto
my
4F
87X
XX
Duo
denu
mG
astr
olit
otom
y
5F
82X
XX
Jeju
num
Ent
erol
itho
tom
y
6F
80Ye
sX
XX
Jeju
num
Ent
erol
itho
tom
yw
ound
infe
ctio
n

International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:100989Z01MF2019. www.ijcasereportsandimages.com
Ferreira et al. 4
Plain abdominal radiographs are of major importance in establishing the diagnosis. In 1941 Rigler et al described the signs found in gallstone ileus: partial or complete intestinal obstruction, pneumobilia and an aberrant gallstone [7]. The presence of two of the three first signs is considered pathognomonic. In later years, other signs have been added by different authors, however plain abdominal radiographs lack in specificity and sensibility for this condition [4].
Abdominal ultrasound is a complementary examination to the plain abdominal radiograph and is more sensitive at detecting pneumobilia and ectopic gallstones. The combination of abdominal ultrasound
and plain abdominal radiograph increases the sensitivity by 74% [8].
CT scan presents with a sensitivity of up to 93% in the detection of gallstone ileus cases [9]. In our series, the ectopic gallstone was observed in all the patients and a complete Rigler’s triad in 83.3%.
The frequency of Rigler’s triad detection is nowadays much superior, as for identifying a mechanical intestinal obstruction, small amount of air in the gallbladder and gallstone. As the CT scan can describe the location of the fistula, gallstones and obstruction with a higher precision, it allows better therapeutic decisions, assuming the position of the gold standard in the diagnosis, when a high index of suspicion is present [9].
When it comes to treatment there is no consensus. The main goal is to extract the offending gallstone. However, as most patients are elderly, and usually present several comorbidities, these reflect an increase in risk with surgery time, mortality and morbidity. The current surgical procedures in use are: simple enterolithomy; enterolithotomy cholecystectomy and fistula closure (one step procedure); and enterolithotomy with cholecystectomy performed in a two-step procedure [10].
Enterolithotomy is the most commonly surgical procedure performed. The main source of confusion comes from whether biliary surgery should be carried out at the same time as the relief of obstruction, performed latter, or not performed at all [11].
Enterolithotomy has been shown to be associated with lower morbidity and mortality, lower operative time and a shorter hospital stay. Reisner et al showed a mortality rate of 12% for simple enterolithotomy comparing with 17% for the one step procedure [6]. In our series, the only perioperatory mortality occured in the patient submitted to one step procedure, however in this case, patient died of cardiovascular complications, not directly associated to the surgical procedure.
Up to 50% of biliary enteric fistula closed spontaneously and biliary symptoms requiring surgery were seen in 10% of patients [6]. The report of recurrent gallstone ileus may be underestimated because figures are mainly based on case reports or small series [3].
A laparoscopic approach is still limited in experience with this condition, however in selected cases may help to reduce morbidity and mortality, with improvement in postoperative recovery [12].
CONCLUSION
Gallstone ileus is a rare entity, difficult to diagnose and requires a high index of suspicion. Abdominal CT scan is the diagnostic modality of choice due it’s high sensitivity. Since the majority of these patients are elderly, usually with multiple co-morbidities, the surgical treatment of choice should be as aggressive as possible and able to relieve the obstruction. In this sense, a
Figure 2: Jejunal obstruction caused by an ectopic gallstone.
Figure 3: Enterotomy performed proximal to the obstruction, with removal of the gallstone, measuring 2.5 cm.
Figure 4: The incision was closed transversely using a single layer suture.
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:100989Z01MF2019. www.ijcasereportsandimages.com
Ferreira et al. 5
simple enterolithotomy alone is the procedure of choice in the emergency context. The one-stage procedure with enterotomy plus cholecystectomy should be reserved for patients presenting in good general condition with a low degree of cholecystitis.
REFERENCES
1. de Alencastro MC, Cardoso KT, Mendes CA, Boteon YL, de Carvalho RB, Fraga GP. Acute intestinal obstruction due to gallstone ileus. [Article in Portuguese]. Rev Col Bras Cir 2013;40(4):275–80.
2. Pezzoli A, Maimone A, Fusetti N, Pizzo E. Gallstone ileus treated with non-surgical conservative methods: A case report. J Med Case Rep 2015;9:15.
3. Mir SA, Hussain Z, Davey CA, Miller GV, Chintapatla S. Management and outcome of recurrent gallstone ileus: A systematic review. World J Gastrointest Surg 2015;7(8):152–9.
4. Athwal TS, Howard N, Belfield J, Gur U. Large bowel obstruction due to impaction of a gallstone. BMJ Case Rep 2012;2012.
5. Saurabh S, Camerota A, Zavotsky J. Gallstone ileus: Diagnostic and therapeutic dilemma. International Journal of Case Reports and Images 2011;2(12):1–5.
6. Reisner RM, Cohen JR. Gallstone ileus: A review of 1001 reported cases. Am Surg 1994;60(6):441-6.
7. Lassandro F, Romano S, Ragozzino A, et al. Role of helical CT in diagnosis of gallstone ileus and related conditions. AJR Am J Roentgenol 2005;185(5):1159–65.
8. Ripollés T, Miguel-Dasit A, Errando J, Morote V, Gómez-Abril SA, Richart J. Gallstone ileus: Increased diagnostic sensitivity by combining plain film and ultrasound. Abdom Imaging 2001;26(4):401–5.
9. Yu CY, Lin CC, Shyu RY, et al. Value of CT in the diagnosis and management of gallstone ileus. World J Gastroenterol 2005;11(14):2142–7.
10. Martínez Ramos D, Daroca José JM, Escrig Sos J, Paiva Coronel G, Alcalde Sánchez M, Salvador Sanchís JL. Gallstone ileus: Management options and results on a series of 40 patients. [Article in Spanish]. Rev Esp Enferm Dig 2009;101(2):117–4.
11. Ayantunde AA, Agrawal A. Gallstone ileus: Diagnosis and management. World J Surg 2007;31(6):1292–7.
12. Moberg AC, Montgomery A. Laparoscopically assisted or open enterolithotomy for gallstone ileus. Br J Surg 2007;94(1):53–7.
*********
Author ContributionsManuel Alexandre Viana Ferreira – Substantial contributions to conception and design, Acquisition of data, Analysis and interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be publishedDiogo Pinto – Substantial contributions to conception and design, Acquisition of data, Analysis and interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be publishedFrancisco Fazeres – Substantial contributions to conception and design, Acquisition of data, Analysis and interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be publishedAlberto Midões – Substantial contributions to conception and design, Acquisition of data, Analysis and interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone.
Consent StatementWritten informed consent was obtained from the patient for publication of this case series.
Conflict of InterestAuthors declare no conflict of interest.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Copyright© 2019 Manuel Alexandre Viana Ferreira et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:100989Z01MF2019. www.ijcasereportsandimages.com
Ferreira et al. 6
Access full text article onother devices
Access PDF of article onother devices











![Clinical and radiological diagnosis of gallstone ileus: a ... · order to cause obstruction at an anatomically wide part of the gastrointestinal tract [40–42]. This is estimated](https://img.pdfslide.us/doc/110x75/5d62e92788c993e9588b86bc/clinical-and-radiological-diagnosis-of-gallstone-ileus-a-order-to-cause.jpg)



![Clinical and radiological diagnosis of gallstone ileus: a mini …...order to cause obstruction at an anatomically wide part of the gastrointestinal tract [40–42]. This is estimated](https://img.pdfslide.us/doc/110x75/608941363a06266b2e72bc06/clinical-and-radiological-diagnosis-of-gallstone-ileus-a-mini-order-to-cause.jpg)