Embed Size (px)
Citation preview
JOURNAL OF ADOLESCENT HEALTH CARE 1:309-312, 1981
BRIEF S C I E N T I F I C R E P O R T
Gallbladder Disease in Children and Adolescents
MARTIN FISHER, M.D., J O N A T H A N ROSENSTEIN, M.D., ARNOLD SCHUSSHEIM, M.D.,
I. RONALD SHENKER, M.D., AND MICHAEL NUSSBAUM, M.D. :! i
A 20-year experience with gallbladder disease in 85 chil- dren and adolescents was reviewed. Sixty-five patients had idiopathic cholelithiasis and cholecystitis (group I); 20 patients had cho!elithiasis and cholecystitis s@condary to a predisposing disease or other pathologic diagnoses (group II). For group I patients, 100% were gre~ter than age 12, 92.3% were female, 60% were overwei~t , 20% had a positive family history, and 27.7% had h~d a pre- vious pregnancy. For group II patients, 60% Were less than age 13, 45% were female, 15% were overweight, 5% had a positive family history, and none had p~viously been pregnant. Symptomatology in group I, ~but not group II, patients matched that seen in adults. ~roup I, but not group II, patients experienced delays in diag- nosis. These data indicate that children and adolescents with gallbladder disease constitute two distinct popula- tions and that idiopathic cholelithiasis and cholecystitis must be considered as a potential cause of chronic ab- dominal pain in otherwise healthy adolescents. ::~
KEY WORDS:
Cholelithiasis Cholecystitis
Traditional belief maintains that gallbladder disease is encountered only rarely in pediatric and adoles- cent patients and that predisposing hemat0~ogic or gastrointestinal factors are responsible for thpse few cases that do occur (1-4). Recent reports have cast doubts on the validity of such a belief (5-8). We have
From the Departmen t of Pediatrics, Division of Adolescent Medicine, Long Island Jewish-Hillside Medical Center, New Hyde Park and Health Sciences Center of the State University of New York at StOny Brook, Stony Brook, New York.
Direct reprint requests to: I. Ronald Shenker, M.D., Chief Adolescent Medicine, Long Island Jewish-Hillside Medical Center, NewHyde Park, New York 11042. ,:
Manuscript accepted November 28, 1980.
reviewed a 20-year experience with gallbladder dis- ease in children and adolescents in order to elucidate the clinical and demographic characteristics of this disease in the young.
Materials and Methods A retrospective review was performed on the rec- ords of all patients aged 21 years and younger on whom a cholecystectomy had been performed at Long Island Jewish-Hillside Medical Center from 1960 to 1979. The study group consisted of 85 pa- tients. Patients with biliary atresia were not in- cluded. Patient charts were reviewed for diagnostic findings, demographic data, predisposing factors, symptomatology, laboratory and radiographic find- ings, surgical procedures, and pathologic analyses.
Results Between the years 1960 and 1964, surgery had been performed on 11 patients; 1965-1969, 18 patients; 1970-1974, 30 patients; and 1975-1979, 26 patients. Sixty-five patients were found to have idiopathic cholelithiasis with no underlying disease. Thirteen patients had cholelithiasis and cholecystitis second- ary to a predisposing disease. Seven patients had a diagnosis of other than cholelithiasis and cholecys- tiffs at cholecystectomy. The pathologic diagnoses and underlying diseases are summarized in Table 1.
The 65 patients with idiopathic cholelithiasis and cholecystitis (group I) and the 20 patients with pre- disposing diseases or other gallbladder pathology (group II) are compared in Table 2. Group I patients, all adolescents (> age 12 years), were mostly over- weight (60%) and female (92.3%) and in some cases had a positive family history (20%) or a previous
© Society for Adolescent Medicine, 1981 309 Published by Elsevier North Holland, Inc., 52 Vanderbilt Ave., New York, NY 10017 ISSN 0197-0070/81/040309-04/$02.25
310 FISHER et al. JOURNAL OF ADOLESCENT HEALTH CARE Vol. 1, No. 4
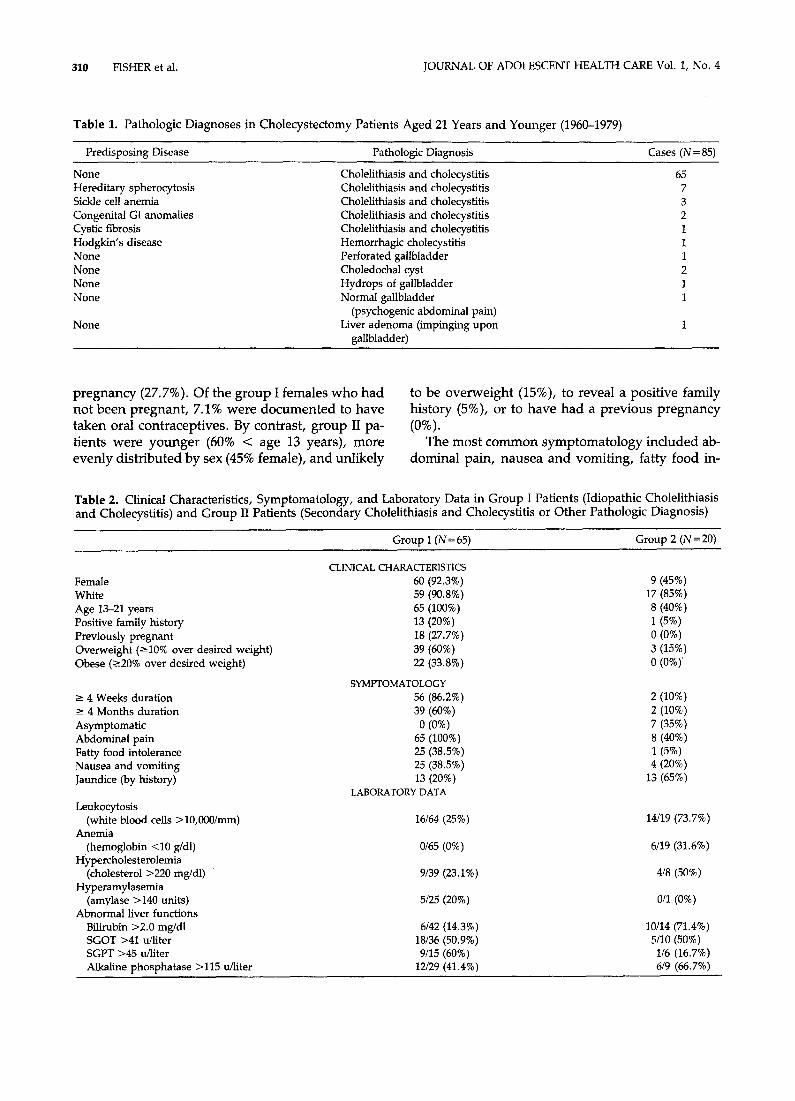
Table 1. Pathologic Diagnoses in Cholecystectomy Patients Aged 21 Years and Younger (1960-1979)
Predisposing Disease Pathologic Diagnosis Cases (N = 85)
None Cholelithiasis and cholecystitis 65 Hereditary spherocytosis Cholelithiasis and cholecystitis 7 Sickle cell anemia Cholelithiasis and cholecystitis 3 Congenital GI anomalies Cholelithiasis and cholecystitis 2 Cystic fibrosis Cholelithiasis and cholecystitis 1 Hodgkin's disease Hemorrhagic cholecystitis 1 None Perforated gallbladder 1 None Choledochal cyst 2 None Hydrops of gallbladder 1 None Normal gallbladder 1
(psychogenic abdominal pain) None Liver adenoma (impinging upon 1
gallbladder)
pregnancy (27.7%). Of the group I females who had not been pregnant, 7.1% were documented to have taken oral contraceptives. By contrast, group II pa- tients were younger (60% < age 13 years), more evenly distributed by sex (45% female), and unlikely
to be overweight (15%), to reveal a positive family history (5%), or to have had a previous pregnancy (0%).
The most common symptomatology included ab- dominal pain, nausea and vomiting, fatty food in-
Table 2. Clinical Characteristics, Symptomatology, and Laboratory Data in Group I Patients (Idiopathic Cholelithiasis and Cholecystitis) and Group II Patients (Secondary Cholelithiasis and Cholecystitis or Other Pathologic Diagnosis)
Group I (N= 65) Group 2 (N = 20)
CLINICAL CHARACTERISTICS Female 60 (92.3%) 9 (45%) White 59 (90.8%) 17 (85%) Age 13-21 years 65 (100%) 8 (40%) Positive family history 13 (20%) 1 (5%) Previously pregnant 18 (27.7%) 0 (0%) Overweight (-~10% over desired weight) 39 (60%) 3 (15%) Obese ('--20% over desired weight) 22 (33.8%) 0 (0%) '
SYMPTOMATOLOGY ----- 4 Weeks duration 56 (86.2%) 2 (10%) -> 4 Months duration 39 (60%) 2 (10%) Asymptomatic 0 (0%) 7 (35%) Abdominal pain 65 (100%) 8 (40%) Fatty food intolerance 25 (38.5%) 1 (5%) Nausea and vomiting 25 (38.5%) 4 (20%) Jaundice (by history) 13 (20%) 13 (65%)
LABORATORY DATA Leukocytosis
(white blood cells >10,000/mm) 16/64 (25%) 14/19 (73.7%) Anemia
(hemoglobin <10 g/dl) 0/65 (0%) 6/19 (31.6%) Hypercholesterolemia
(cholesterol >220 mg/dl) 9/39 (23.1%) 4/8 (50%) Hyperamylasemia
(amylase >140 units) 5/25 (20%) 0/1 (0%) Abnormal liver functions
Bflirubin >2.0 mg/dl 6/42 (14.3%) 10/14 (71.4%) SGOT >41 u/liter 18/36 (50.9%) 5/10 (50%) SGPT >45 u/liter 9/15 (60%) 1/6 (16.7%) Alkaline phosphatase >115 u/liter 12/29 (41.4%) 6/9 (66.7%)

June 1981 GALLBLADDER DISEASE IN CHILDREN AND ADOLESCENTS 311
tolerance, and jaundice (see Table 2). Abdominal pain, either alone (24.6%) or in combination with vomiting (20.0%) or fatty food intolerance (26.2%), was the most frequently reported symptom of group I patients. In 60% of group I patients, the onset of symptoms preceded surgery by at least 4 months. By comparison, 35% of group II patients were asymptomatic, and only 10% had symptoms of greater than I month duration at the time of surgery. Fever was conspicuously absent as a reported symp- tom in both groups (2.3%). Laboratory data revealed leukocytosis, anemia, hypercholesterolemia, hyper- amylasemia, and abnormalities of liver function in some patients (see Table 2).
Oral cholecystography was performed in 74 of the 85 patients. Stones were shown in 81% of cases. The gallbladder did not visualize on single- and double- dose studies in the remaining 19%. Radioopaque stones were detected on abdominal x-rays in one group I patient and in five (38.5%) of group II pa- tients with a predisposing disease. Surgery was per- formed during the course of an acute admission for abdominal pain or jaundice in 32 patients; interval cholecystectomy was performed in 53. Operating room cholecystogram was obtained for 30 patients, and common duct exploration with T-tube place- ment was necessary in 16 patients. As determined by fever patterns and length of hospital stay, no differences were noted postoperatively between those who had acute procedures and those who had interval procedures. Among group I patients, those who required T-tube placement had a greater av- erage postoperative length of stay (11.25 days) than those who did not require T-tube placement (7.86 days). Length of stay in group II patients varied with underlying disease and pathologic diagnosis.
Calculi were discovered on pathologic analysis in 64 of 65 group I patients and in 12 of 13 group II patients with a predisposing disease. The calculi were described grossly as cholesterol or mixed stones in all group I patients and as pigment stones in all group II patients with predisposing disease. Microscopic analysis of the gallbladder revealed cho- lecystitis (chronic, 92.3%; acute, 7.7%) in all patients.
Discussion Gallbladder disease in the young has been described as a complication of many diverse diseases. Chole- lithiasis is a well-known concomitant of hemolytic anemia and congenital bile duct malformations. Cys- tic fibrosis, Wilson's disease, metachromatic leuko- dystrophy, and regional enteritis are also docu-
mented causes (9-12). Acalculous cholecystitis has been reported to follow gastroenteritis, infectious hepatitis, scarlet fever, leptospirosis, cervical aden- opathy, familial Mediterranean fever, polyarteritis nodosa, and mucocutaneous Jymph node syndrome (13-15). Early reports stated that in children and ad- olescents, secondary gallbladder d~sease was the rule and idiopathic cholecystitis and cholelithiasis were the exception (1-4). Recent findings do not support these earlier reports (5-8).
Our study confirms that idiopathic cholelithiasis and cholecystitis is more common than secondary gallbladder disease in our study group of children and adolescents. Our results suggest that children and adolescents with gallbladder disease constitute two distinct populations. Of the 73 adolescents in this study, 65 (89%) had a diagnosis of idiopathic cholelithiasis and cholecystitis; of the 12 children in this study, none had this diagnosis. The adolescents in ou r study display characteristics similar to those noted in adult patients with gallbladder disease, They are predominantly female, frequently over- weight, and often have a positive family history of gallbladder disease or a history of Pregnancy. The children in the study, however, do not display the characteristics of adult gallbladder patients and may, in fact, be exhibiting different disease processes.
Although symptoms reported by the group I pa- tients in this study are consistent with those gen- erally reported by adults, the delays in diagnosis noted for some patients may indicate a low index of suspicion of gallbladder disease by physicians caring for adolescents. The short duration of symptoms in group II patients suggests an appropriate awareness of the predisposing causes of gallbladder disease. The frequency of asymptomatic cholelithiasis noted in group II patients has been described elsewhere (16).
Our laboratory data are consistent with those re- ported elsewhere (5-8). Leukocytosis correlates with the acute nature of the cholecystitis, while anemia is noted only in patients with underlying hemato- logic disease. Hypercholesterolemia does not spe- cifically correlate with cholelithiasis. Hyperamyla- semia may be seen in gallbladder disease with or without pancreatitis. Hyperbilirubinemia and other liver function abnormalities may serve as important indicators of gallbladder disease in group II and some group I patients. The pathologic findings of cholesterol or mixed stones in group I patients and of bilirubin pigment stones in group II patients with predisposing disease are as expected.
Recent reports indicate a rising incidence of gall-

312 FISHER et al. JOURNAL OF ADOLESCENT HEALTH CARE Vol. 1, No. 4
bladder disease among children and adolescents during the past two decades (7). A change in con- sumption patterns toward the use of more processed foods has been offered as an explanation for the apparent increased lithogenicity of bile at younger ages (17). We also found an increasing incidence of disease during t'he years 1960-1979. The authors suggest that a greater number of teenage pregnan- cies and more contraceptive usage may be additiona ! factors leading to ,increased bile lithogenicity in ad- olescent females (18).
In order to eliminate delays in diagnosis, it is nec- essary for physicians to appreciate that gallbladder disease must be considered as a potential cause of chronic abdominal pain in otherwise healthy ado- lescents, especially females. This study suggests that obesity, a positive family history for gallbladder dis- ease, pregnancy, and possibly oral contraceptive usage are predisposing factors. Right upper quad- rant or'mid-epigastic pain was found in all cases. Vomiting, fatty food intolerance, or jaundice may be a concomitant symptOm and liver function abnor- malities may be useful screening indicators. While abdominal x-rays are infrequently of help, ora! cho- lecystography yielded uniformly satisfactory results in this long-term study. Ultrasonography, not eval- uated in this study, is proving to be a useful adjunct. These clinical points should be kept in mind when evaluating young patients with abdominal pain, es- pecially if that patient is "female, fat, fertile, and fourteen."
References 1. Glenn F, Hill MR: Primary gallbladder disease in children.
Ann Surg 139:302-311, 1954 2. Seiler I: Gallbladder disease in children. Am J Dis Child
99:662-665, 1960
3. Hawkins PE, Graham FB, Halliday P: Gallbladder disease in children. Am J Surg 111:741-744, 1966
4. Graivier L, Dorman GW, Votteler TP: Gallbladder disease in infants and children. Surgery 63:690-696, 1968
5. Sears HF, Golden GT, Horsley S: Cholecystitis in childhood and adolescence. Arch Surg 106:651-653, 1973
6. Andrassy RJ, Treadwell TA, Ratner IA, et ah Gallbladder disease in children and adolescents. Am J Surg 132:19-2t, 1976
7. Grace N, Rodgers B: Cho!ecystitis in childhood: Clinical ob- servations based on 30 surgically treate d cases. Clin Pediatr (Philh) 16:179-181, 1977
8. Honore LH: Cholesterol cholelithiasis in adolescent females. Arch Surg 115:62-64, 1980
9. Rovsing H, Sloth K: Micro-gallbladder and biliary calculi in mucoviscidosis. Acta Radiol 14:588-592, 1973
10. Rosenfeld N, Grand RJ, Watkins JB, et al: Cholelithiasis and Wilson disease. J Pediatr 92:210-213, i978
11. Roy C, Silverman A, Cozzeto FJ: Pediatric Clinical Gastro- enterology, ed 2. St. Louis, C.V. Mosby, 1975, pp 605-614
12. Cohen S, Kaplan M, Gottlieb L, Patterson J: Liver disease and galMones in reg!onal enteritis. Gastroenterology 60:237-245, 1971
13. Kumari S, Lee WJ, Baron MG: Hydr0ps of the gallbladder in a child: Diagnosis bY ultrasonography. Pediatrics 63:295-297, 1979
14. Magilavy DB, Speert P, Silver TM, et al: Mucocutaneous lymph node syndrome: Report of two cases complicated by gallbladder hydrops and diagnosed by ultrasound. Pediatrics 61:699-702, 1968
15. Slovis TL, Hight DW, Philippart AI, et al: Sonography in the diagnosis and management of hydrops of the gallbladder in children with mucocutaneous lymph node syndrome. Pedi- atrics 65:789-794, 1980
16. Karayalcin G, Hassini N, Abrams M, et al: Cholelithiasis in children with sickle cell disease. Am J Dis Child 133:306-307, 1979
17. Plant JCD, Percy I, Bates T, et al: Incidence of gallbladder disease in Canada, England and France. Lancet 2:249-251, i973
18. Bennion L, Ginsberg RL, Garnick MB, et al: Effects of oral contraceptives on the gallbladder of normal women. N Engl J Med 294:189-192, 1976























![Approach to a Patient With Gallbladder Disease[1]](https://img.pdfslide.us/doc/110x75/577dacbe1a28ab223f8e5073/approach-to-a-patient-with-gallbladder-disease1.jpg)

