Embed Size (px)
Citation preview

Gut 1994; 35: 117-121
Gall stone pulverisation strategy in patients treatedwith extracorporeal lithotripsy and follow up resultsof maintenance treatment with ursodeoxycholic acid
M Boscaini, M Piccinni-Leopardi, F Andreotti, A Montori
AbstractBetween November 1988 and July 199270 patients with radiolucent gall stones were
treated with extracorporeal lithotripsy (ESL)and ursodeoxycholic acid (UDCA; mean (SD)dose 11-2 (1-9) mg/kg/day). Fifty three patientshave been followed for one year. One weekafter lithotripsy, 30-6% had completely elimi-nated all stone fragments from the gall bladderand one year later 93*9% were free of stones.Three factors were considered important inachieving these results. 'Pulverisation' of thestone - that is, its fragmentation into echo-genic dust (crystalline aggregates, some fewhundred > in size) or particles similar to grainsof sand, smaller than 1 mm in diameter, or
both, is required. Secondly, dust and particleswere rapidly eliminated, strongly suggestinga mechanical elimination process by physio-logical gall bladder contractions. Thirdly,there must be chemical dissolution with biliaryacids. This therapeutic approach gave excel-lent results without causing any clinicallyrelevant side effects. The first 20 patients whobecame free of stones after ESL were givenoral bile acid maintenance treatment - 300 mg/day of UDCA at bedtime, for two years. Allwere asymptomatic and none had suffered a
recurrence after two years. In four patients,crystalline aggregates, detected in gall bladderbile by ultrasound, were subsequently dis-solved between one and three months afterresuming a full dose regimen ofUDCA.(Gut 1994; 35: 117-12 1)
Third Department ofSurgery, University ofRome 'La Sapienza'M BoscainiA Montori
ExtracorporealLithotripsy Unit, Pio XIClinic, RomeM Piccinni-LeopardiF AndreottiCorrespondence to:Dr M Boscaini, Clinica Pio XI,Unita di Litotrissia, ViaAurelia 559, 00165 Rome,Italy.Accepted for publication8 June 1993
Results of studies on extracorporeal lithotripsy(ESL) of gall stones in which patients have beenfollowed up for seven years have often provedto be unsatisfactory and at times discordant.Despite this we believe that ESL is an extremelyeffective method of treating gall stones and thatthese negative results may result from the follow-ing factors that are unrelated to the procedure:(1) Use of equipment developed for kidney stonedissolution and improperly adapted to gall stonetreatment; (2) Use of shock waves that are toolow in pressure and too few in number;(3) Therapeutic strategy tending towards stonefragmentation followed by chemical dissolu-tion with bile acids lasting even long periods oftime.
This trial aimed to determine whether byperfecting the technique of biliary lithotripsy,the procedure would prove to be an effectivemethod of treating gall stones. For this purposeit was necessary to verify:
(1) Whether by using shock waves adequate inpressure and in number it would be possible toachieve 'pulverisation' of stones into crystallineaggregates or particles the size of grains of sand,or both.
(2) Whether by achieving this pulverisation itwould be possible to achieve safer and morerapid elimination of the resulting microfrag-ments.
(3) Eliminating stones followed by mainten-ance treatment while preserving the gall bladderwould be sufficient to avoid stone recurrence.
Methods
PATIENTSBetween November 1988 and July 1992, 70patients with radiolucent gall stones were treatedwith a lithotripter equipped with an underwaterspark-gap for shock wave generation (DornierMPL 9000, Germany). The first 53 patients (24men and 29 women; mean (SD) age 48 (12)(range 24-74 years) and mean (SD) body weight148-9 (27) (range 108-234) lb) were followed upover one year by monthly clinical and ultrasoundexaminations. Thirty nine (73 6%) were con-sidered to be 'symptomatic' (having had at leastone attack of biliary pain lasting more than 30minutes in the three years before the treatment),while 14 (26-4%) were considered 'asympto-matic' (either having suffered from biliary painmore than three years before treatment or havinghad an attenuated painful symptomatology). Allpatients were admitted to hospital: 45 patients(85%) for one day and 8 (15%) for two days.No patient required anaesthesia and 17 (32%)required intravenous analgesia (fentanyl 0 1 mgand diazepam 20 mg). Four ofthe 53 patients didnot complete follow up, leaving only 49 for thefull study.
STONESThirty four patients had single stones (sevenof which had a diameter >20 mm), while 19had multiple stones (up to eight stones). Fivepatients had calcified stones: two had a centralcalcification 2mm in diameter, one had a calcifiedrim <2 mm, and two had completely calcifiedstones. The smallest single stone had a diameterof 7 mm and the largest 40 mm. The mean (SD)stone diameter was 14-3 (7- 1 mm). The smallestsingle stone volume was 0- 18 cm3 and the largestwas 33-4 cm3. Mean (SD) stone volume was 4-4(6) cm3. The number and diameter of the stoneswere measured by ultrasound scan (3 75 MHz
117
on Decem
ber 22, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.35.1.117 on 1 January 1994. Dow
nloaded from
Boscaini, Piccinni-Leopardi, Andreotti, Montori
convex array probe PVB-358M, SAL 38BToshiba, Japan). These measurements weredetermined by oral cholecystography whenevernecessary.
ESL TREATMENTSThirty nine patients (79 6%) required a singletreatment, five required two, two required three,two required four, and one required five for atotal of 68 treatments. The mean number oftreatments per patient was 1-4, and the percent-age that required retreatment was 20-4%. Theminimum voltage used was 14 kV, maximum 23kV, mean 18 8 (1) kV. The minimum number ofshock waves per treatment was 700, the maxi-mum 2600, and the mean (SD) 1972 (482).
MEDICAL TREATMENTMedical treatment consisting of daily doses ofursodeoxycholic acid (UDCA) at bed time (mean(SD) dose 11-2 (1-9) mg/kg/day) started twoweeks before ESL treatment and continuedfor up to three months after patients hadbeen considered 'stone-free'. All patients whowere confirmed to be 'stone-free' after threemonths continued with maintenance therapy(UDCA 300 mg/day at bedtime for up to twoyears).
ANALYSESAll patients underwent double contrast oralcholecystography to determine the patency ofthe cystic duct, ultrasonography of the upperabdomen, plain film x ray of the gall bladder areato detect any stone calcification, chest x ray,electrocardiogram, and urinalysis. In addition,the following blood tests were performed:erythrocyte sedimentation rate, full blood count,prothrombin time, bilirubin, partial thrombintime, aspartate transaminase, alanine aminotransferase, lactate dehydrogenase, creatinephosphokinase, gamma glutamyl transferase,alkaline phosphatase, serum amylase and lipase,fasting blood glucose, blood urea nitrogen,creatinine, and pregnancy test in women. Bloodtests were repeated the day after treatment.Biochemical variations were considered signifi-cant only if they were 20% or more above orbelow normal values.
CRITERIA FOR TREATMENTInclusion criteria for treatment were as follows:
a 100U)
a)
I0
ce
0
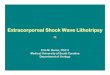
93-9
81-6
959-2 737'..........
49
7 Day 1 2 3 4 6 8 1 YearMonths
Time
(1) solitary radiolucent stone, maximum dia-meter -40 mm; (2) multiple radiolucent stonesnot exceeding 50% of total gall bladder volumeand not exceeding the volume of a stone 40 mmin diameter; (3) radiolucent stones with rimcalcification <2 mm; (4) radiolucent stones withcentral calcification <5 mm; (5) proof of cysticduct patency by oral cholecystography; (6) cleardetection of stone by ultrasound and possibilityof positioning in shock wave focus.The exclusion criteria for treatment were as
follows: (1) obstructive jaundice; (2) cholangitis;(3) acute cholecystitis; (4) acute pancreatitis; (5)bleeding disorders; (6) cardiac pacemaker; (7)pregnancy.
FRAGMENTATION RESULTSFragmentation results were reported one weekafter ESL and were defined by ultrasonographyby the same operator as follows: (1) Completefragmentation: echogenic dust (crystallineaggregates, some few hundred [t in size) or smallparticles similar to grains ofsand with a diameter<1 mm, or both. The authors call this type offragmentation 'pulverisation'. (2) Satisfactoryfragmentation: remaining particles diameter s:5mm. (3) Partial fragmentation: remainingparticles diameter >5 mm.
STRATEGY FOR RETREATMENTSReassessment was performed once a month byultrasonography. If this showed remaining frag-ments --5 mm, medical treatment was continuedwith UDCA. Fragments larger than 5 mmindicated the need for retreatment. This thera-peutic approach was followed up to December1989 (first 25 patients), after which fragmentslarger than 1 mm were also retreated at onemonth intervals in order to achieve pulverisa-tion.
'STONE-FREE' DEFINITIONOnly where there was complete disappearance ofstone fragments and also ofcrystalline aggregateswas the patient considered 'stone-free'. Thisstage had to be confirmed ultrasonographicallyby the same operator after three months.
STATISTICAL ANALYSESTo verify whether the attacks of biliary painsuffered after lithotripsy were a side effect oftreatment as has been reported,' controls wereperformed to detect any statistically significantdifference between the mean number of attackssuffered after treatment up to the stone-freestage compared with those suffered for an equalperiod of time before treatment. Statisticalanalyses were carried out by using paired twotailed Student's t test. A value of p<0 05 wasconsidered to be statistically significant.
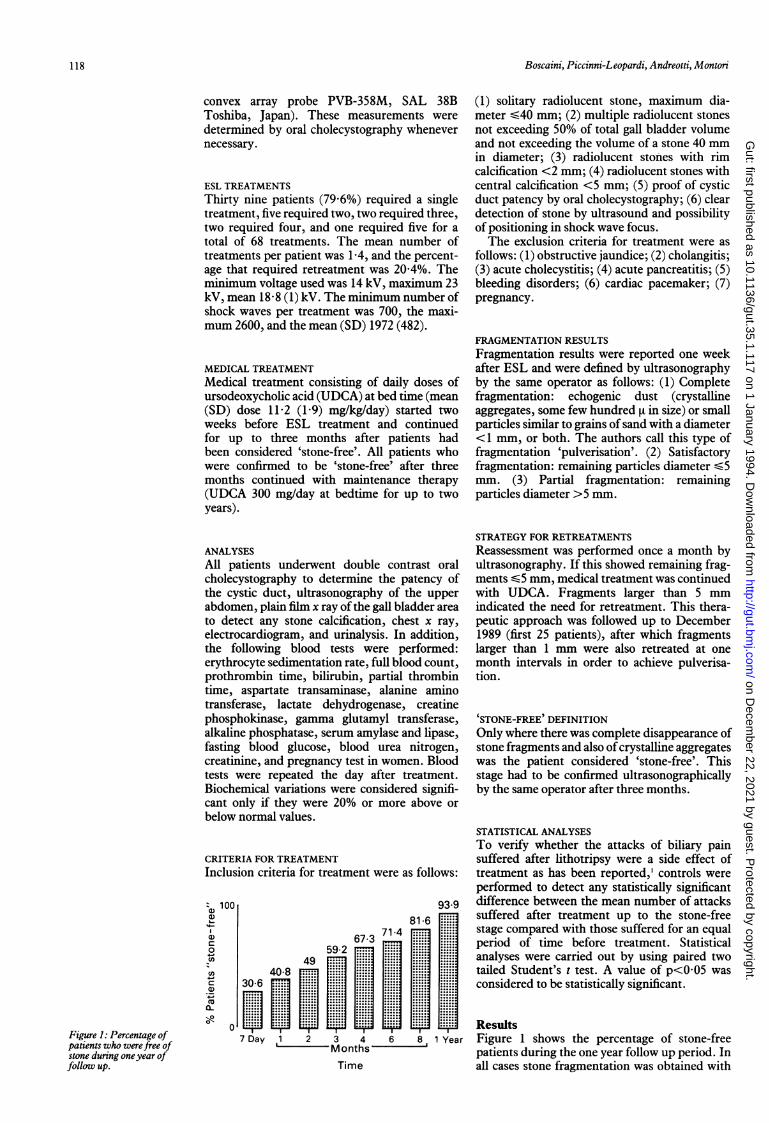
ResultsFigure 1 shows the percentage of stone-freepatients during the one year follow up period. Inall cases stone fragmentation was obtained with
Figure 1: Percentage ofpatients who werefree ofstone during oneyear offollow up.
118
on Decem
ber 22, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.35.1.117 on 1 January 1994. Dow
nloaded from
Gall stone pulverisation strategy in patients treated with extracorporeal lithotripsy andfollow up results ofmaintenance treatment with ursodeoxycholic acid
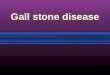
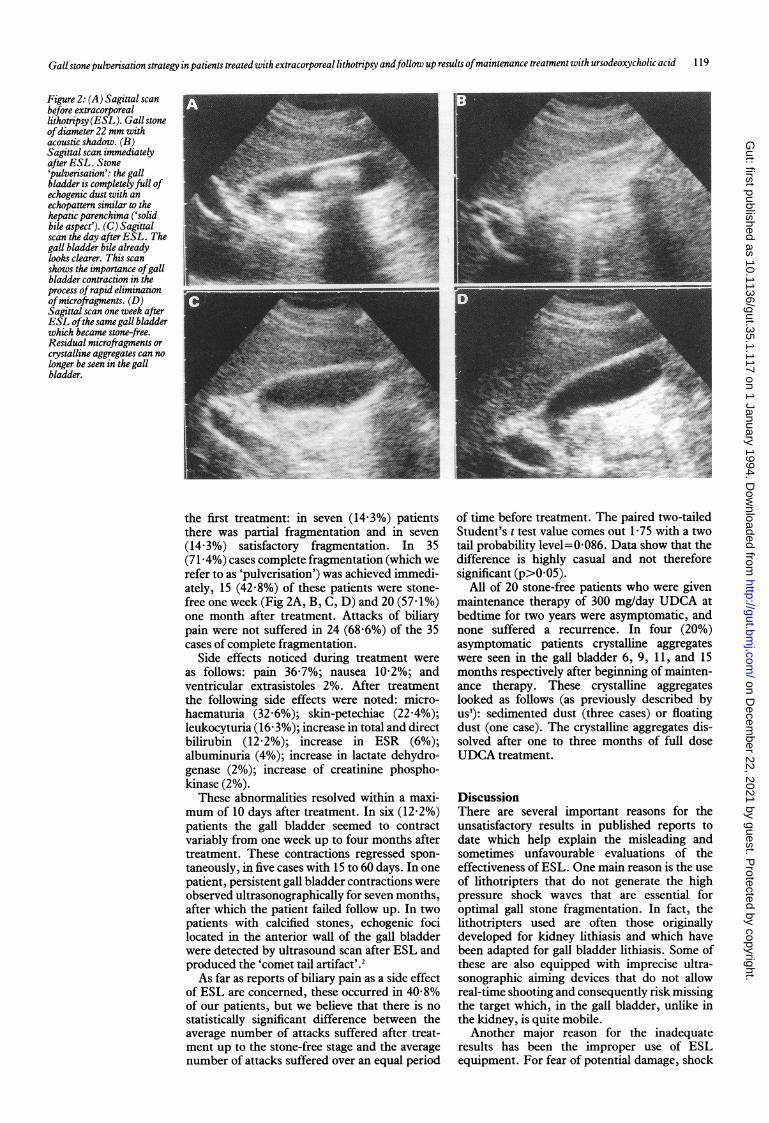
Figure 2: (A) Sagittal scanbefore extracorporeallithotripsy(ESL). Gallstoneofdiameter 22 mm withacoustic shadow. (B)Sagittal scan immediatelyafter ESL. Stone'pulverisation': the gallbladder is completely full ofechogenic dust with anechopattern similar to thehepatic parenchima ('solidbile aspect'). (C) Sagittalscan the day after ESL. Thegall bladder bile alreadylooks clearer. This scanshows the importance ofgallbladder contraction in theprocess ofrapid eliminationofmicrofragments. (D)Sagittal scan one week afterESL ofthe same gall bladderwhich became stone-free.Residual microfragments orcrystalline aggregates can nolonger be seen in the gallbladder.
the first treatment: in seven (14-3%) patientsthere was partial fragmentation and in seven(14-3%) satisfactory fragmentation. In 35(71-4%) cases complete fragmentation (which werefer to as 'pulverisation') was achieved immedi-ately, 15 (42 8%) of these patients were stone-free one week (Fig 2A, B, C, D) and 20 (57dI%)one month after treatment. Attacks of biliarypain were not suffered in 24 (68 6%) of the 35cases of complete fragmentation.
Side effects noticed during treatment wereas follows: pain 36-7%; nausea 10-2%; andventricular extrasistoles 2%. After treatmentthe following side effects were noted: micro-haematuria (32 6%); skin-petechiae (22 4%);leukocyturia (16 3%); increase in total and directbilirubin (12-2%); increase in ESR (6%);albuminuria (4%); increase in lactate dehydro-genase (2%); increase of creatinine phospho-kinase (2%).
These abnormalities resolved within a maxi-mum of 10 days after treatment. In six (12-2%)patients the gall bladder seemed to contractvariably from one week up to four months aftertreatment. These contractions regressed spon-taneously, in five cases with 15 to 60 days. In onepatient, persistent gall bladder contractions wereobserved ultrasonographically for seven months,after which the patient failed follow up. In twopatients with calcified stones, echogenic focilocated in the anterior wall of the gall bladderwere detected by ultrasound scan after ESL andproduced the 'comet tail artifact'.2As far as reports of biliary pain as a side effect
of ESL are concerned, these occurred in 40-8%of our patients, but we believe that there is nostatistically significant difference between theaverage number of attacks suffered after treat-ment up to the stone-free stage and the averagenumber of attacks suffered over an equal period
of time before treatment. The paired two-tailedStudent's t test value comes out 1-75 with a twotail probability level=0 086. Data show that thedifference is highly casual and not thereforesignificant (p>0O05).
All of 20 stone-free patients who were givenmaintenance therapy of 300 mg/day UDCA atbedtime for two years were asymptomatic, andnone suffered a recurrence. In four (20%)asymptomatic patients crystalline aggregateswere seen in the gall bladder 6, 9, 11, and 15months respectively after beginning of mainten-ance therapy. These crystalline aggregateslooked as follows (as previously described byus3): sedimented dust (three cases) or floatingdust (one case). The crystalline aggregates dis-solved after one to three months of full doseUDCA treatment.
DiscussionThere are several important reasons for theunsatisfactory results in published reports todate which help explain the misleading andsometimes unfavourable evaluations of theeffectiveness of ESL. One main reason is the useof lithotripters that do not generate the highpressure shock waves that are essential foroptimal gall stone fragmentation. In fact, thelithotripters used are often those originallydeveloped for kidney lithiasis and which havebeen adapted for gall bladder lithiasis. Some ofthese are also equipped with imprecise ultra-sonographic aiming devices that do not allowreal-time shooting and consequently risk missingthe target which, in the gall bladder, unlike inthe kidney, is quite mobile.
Another major reason for the inadequateresults has been the improper use of ESLequipment. For fear of potential damage, shock
119
on Decem
ber 22, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.35.1.117 on 1 January 1994. Dow
nloaded from
Boscaini, Piccinni-Leopardi, Andreotti, Montori
waves too low in pressure and too few in numberhave been applied. This concern is unwarrentedsince we have shown that biliary lithotripsy, withhigher pressure and more shock waves, will giveexcellent results without causing clinicallyrelevant side effects.A further problem has been the implementa-
tion of a therapeutic strategy. Up to now this hasaimed at creating fragments which have then hadto be dissolved chemically. Because of this it hastaken longer for patients to become stone-freeand, consequently, they have risked 'residual'symptomatic lithiasis.The most interesting results, which up to now
have never been published, are that 306% ofourpatients became free of stones after only sevendays and 93-9% were stone-free after one year.
Achieving this stone-free condition in such ashort time strongly suggests something new andimportant - how effective gall bladder contrac-tions are in eliminating microfragments rapidly.The difference in strategy may be substitution ofthe binomial 'fragmentation-chemical dissolu-tion' for 'pulverisation-mechanical expulsion'.The stone should not be fragmented, but'pulverised'. This term, which describes the finalaim of lithotripsy better, is intended by us tomean reduction of the stone into echogenic dust(crystalline aggregates some few hundred [t insize) or small particles similar to grains of sandand with a diameter <1 mm, or both. As hasbeen observed, it is probable that these particlesare mainly eliminated by physiological gallbladder contractions. In cases where pulverisa-tion was achieved, the length of time taken toexpel particles was extremely short. Some 42 8%patients were stone-free after one week and57-1% at the end of a month. In 68-6% of thecases elimination occurred without attacks ofbiliary pain.Another point we would like to stress is that
pulverisation must be achieved in the shortesttime possible, even if this requires more treat-ments at shorter intervals (one month). Reportedside effects (mild biliary pancreatitis in 1 8% ofthe cases, cholestasis in 1%, and endoscopicsphincterotomy in 0-6%)' have actually been theresult of fragments remaining in the gall bladderfor long periods, and thus the consequentialresidual lithiasis. Damage caused by shockwaves has never created any clinically relevantproblems except in the rare case of a subcapsularhaematoma of the liver in 0 1% of patients.'A therapeutic strategy aimed at fragment
pulverisation should further reduce the risks ofcommon bile duct obstruction and acute biliarypancreatitis. The American National Multi-center Study (MEDSTONE) data indicate thatfragments can pass spontaneously or are dis-solved, or both, without causing major sideeffects4 and Greiner' has already indicated thefeasibility and innocuousness of the passagethrough the main biliary duct of fragments up to3 mm in size.We emphasise that to obtain stone pulverisa-
tion, underwater spark-gap lithotripters able toproduce high pressure shock waves and equip-ped with precision ecographic aiming devicesallowing real-time shooting are essential. Inaddition, an adequate number of shock waves
must be applied. While published reports showthat this number is usually limited to 1500 onspark-gap equipment, we used a mean (SD) of1972 (482) waves, up to a maximum of 2600.As far as side effects are concerned, we show
that biliary colic cannot be considered as such,since in our patients there was not a significantdifference between the number of episodes ofcolic suffered before and after treatment.Having proved that lithotripsy is valid in
freeing the gall bladder from stones, we still needto determine whether it is methodologicallycorrect to use this therapeutic technique inpatients with a gall bladder that is susceptible tostone recurrences. Ruppin6 and Toulet7 over-estimated the percentage of recurrences, accord-ing to Lanzini,8 because patients were followedup exclusively by cholecystography and theresults were not statistically correct. In the pastfew years, reports of recurrence after chemicaldissolution are in agreement. Each year, theincidence of recurrences is about 10%,8-'3 but therisk falls after the first two and a half years'4 anddoes not seem to persist after five years.8 13 AfterESL and with ultrasound control the risk ofrecurrence seems to be reduced by about half, asthe rate becomes 5% annually.'5 According todata on recurrence after bile acid treatment,approximately 50% of patients remain stone-freeafter 10 years'3 and according to data after ESL,approximately 80% of patients should remainstone-free after four years."' In these patients,the aetiopathogenetic defect responsible for theformation of calculi seems to be transitory only,and cholcystectomy in these cases would be anunnecessary as well as a drastic means ofprevent-ing stone recurrences. Hence, ESL together withUDCA treatment seems to be appropriate. Thisis further confirmed by results published in thepast few years on the efficacy of maintenancetherapy with UDCA in preventing recurrence.Cases where low doses of CDCA (375 mg/day)'0or UDCA (3 mg/kg/day)'6 were given along withfollow up consisting exclusively of cholecysto-graphy or cholecystography plus ultrasoundshow no reduction in the percentage of recur-rences. Other more recent studies show that therisk of recurrence is reduced by using higherdoses ofUDCA during maintenance therapy." 12We would like to add to these results our
preliminary data on the absence of lithiasicrecurrences at two years in patients given main-tenance therapy with UDCA (300 mg/day atbedtime). We believe that these successfulresults are largely due to the use of preciseparameters in ultrasound determination of whena patient can be considered stone-free. If thisstage is not evaluated correctly, new lithiasicformations will be inaccurately diagnosed asrecurrences whereas, in fact, they represent noneother than the volumetric increase of residualmicroformations (risk of overestimating recur-rences). Moreover, if the stone-free condition isnot assessed under very rigorous criteria, crystal-line aggregates that were not completely elimi-nated and were not recognised by ultrasono-graphy could become responsible for anaccelerated nucleation process (risk of more fre-quent and earlier recurrences).
Ultrasonographic recognition of crystals in
120
on Decem
ber 22, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.35.1.117 on 1 January 1994. Dow
nloaded from
Gall stone pulverisation strategy in patients treated with extracorporeal lithotripsy andfollow up results ofmaintenance treatment with ursodeoxycholic acid 121
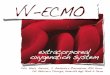
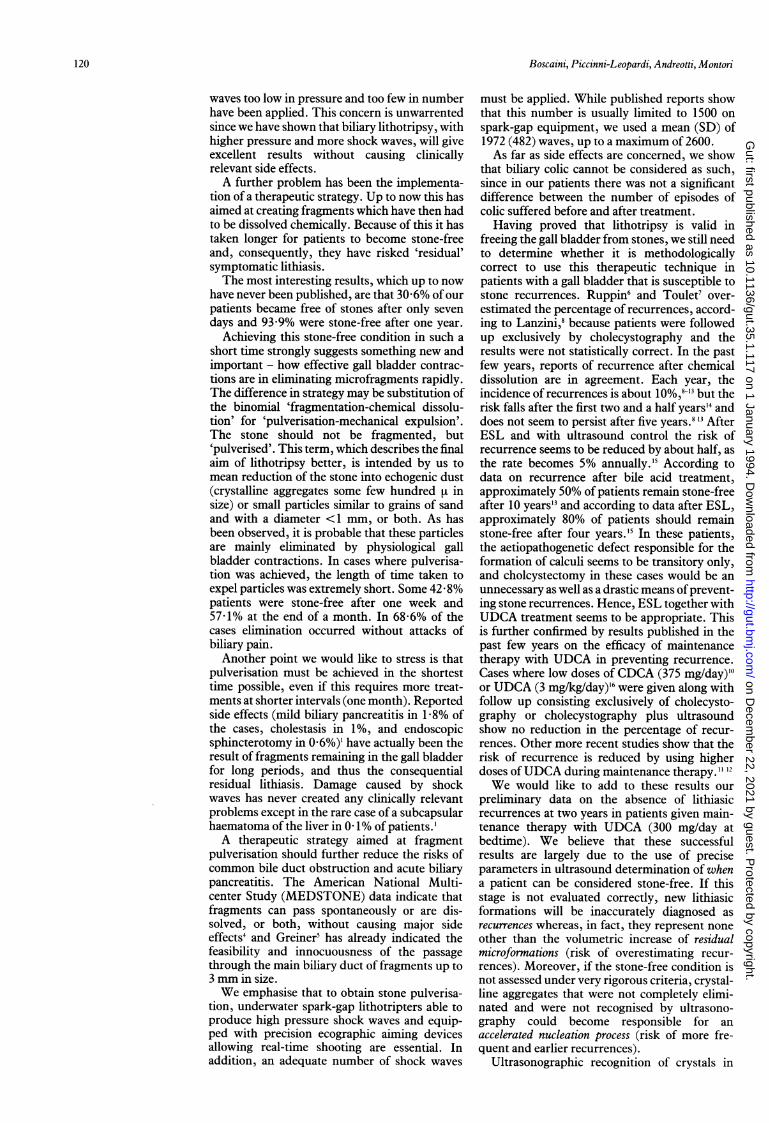
Figure 3: (A) Sagittal scaneight days afterextracorporeal lithotripsy.Two echogenic images(arrows) projecting a weakacoustic shadow are stillpresent in the gall bladder.Fragments or crystallineaggregates? (B) Sagittalscan after the 'shatteringmanoeuvre'. The twoechogenic images turned intoafine echogenic dust (arrows) -proving the presence ofcrystalline aggregates in thegall bladder.
-:-~~~~ ~ ~~~~~~~~~~~~~~~~~~~ ...... .
gall bladder bile is an extremely delicate diagnos-tic requirement with regards to preventingrecurrences after reaching the stone-free stage. Ifthe presence of crystals is not recognised earlyon, the process which we call 'ultrasonic nuclea-tion' and upon which stone formation is based,may not be detected. Ultrasonography, as wehave previously shown, allows great diagnosticcapabilities in visualising crystalline aggregatesin bile which may have multiple, and sometimesquite bizarre, morphological aspects.3 17 We havepreviously described an interesting aspect ofthese crystals - 'reversible aggregation' - bywhich they can simulate the presence of a solidparticle sometimes projecting a weak posterioracoustic shadow. We have suggested a 'shatter-ing manoeuvre'3 for the differential diagnosis ofthe echogenic particles contained in bile oradhering to the gall bladder wall, which consistsin repeated percussion of the patient's righthypochondrium with the ultrasound probe,without removing it from the skin. If a particleis made of crystalline aggregates, it will prob-ably dissolve into fine echogenic dust. Thismanoeuvre has proved useful even in follow upofpatients treated with ESL in that it has alloweddiscrimination between residual fragments andfalse ones made of reversible aggregations ofcrystalling particles, thus leading to a morecorrect treatment strategy (Fig 3A, B).
In conclusion, we maintain that the use ofequipment suitable for the treatment of biliarylithotripsy, when coupled with the use ofadequate power and optimal number of shockwaves, will allow the reduction of the stone intoechogenic dust consisting of crystalline aggre-gates or particles similar to grains of sand orboth. The fact that these microfragments arequickly eliminated strongly suggest that it iscaused by mechanical expulsion through physio-logical gall bladder contractions. This suggestioncan only be confirmed conclusively throughadditional motility studies without the use of bileacids. An adjuvant medical therapy with UDCAwill be necessary to help the elimination processthrough chemical dissolution of these microfrag-ments."8 Recurrences can probably be avoidedby giving patients - especially those at high risk -follow up maintenance treatment with UDCAand accurate ultrasonographic controls in orderto diagnose rapidly the presence of crystals inbile.
We are indebted to Ms Bonnie Bates, Ms Anna Maria Erikssonand Mr Alexander Guttieres, for assistance in preparing themanuscript.
1 Sackmann M, Pauletzki J, Sauerbruch T, Holl J, Schelling G,Paumgartner G. The Munich gallbladder lithotripsy study.Results of the first S years with 711 patients. Ann Intern Med1991; 114: 290-6.
2 Shapiro RS, Winsberg F. Comet-tail artifact from cholesterolcrystals: observations in the postlithotripsy gallbladder andan in vitro model. Radiology 1990;177: 153-6.
3 Boscaini M, Magnani G, Mandetta S, Montori A. Morpho-logical appearance of low-level echoes in the gallbladder.Interpretation with microscopic biliary analysis and clinicalcorrelation. Surg Endosc 1987; 1 (1): 41-9. Letter DornierUser 1989; 5: 30-7.
4 Burnett D, Ertan A, Jones R, O'Leary JP, Mackie R,Robinson JE, et al. Use of external shock-wave lithotripsyand adjuvant ursodiol for treatment of radiolucent gall-stones. A national multicenter study. Dig Dis Sci 1989; 7:1011-5.
5 Greiner L, Munks C, Heil W, Jakobeit C. Gallbladder stonefragments in feces after biliary extracorporeal shock-wavelithotripsy. Gastroenterology 1990; 98: 1620-4.
6 Ruppin DC, Dowling RH. Is recurrence inevitable aftergallstone dissolution by bile acid treatment? Lancet 1982; I(8265): 181-5.
7 Toulet J, Rousselet J, Viteau JM, Duchon Y, Pagniez R,Samain B, et al. Reidives et prevention des recidives apresdissolution de la lithiase vesiculaire par l'acide chenodeo-xycholique chez 22 patients. Gastroenterol Clin Biol 1983; 7:605-9.
8 Lanzini A, Jazrawi RP, Kupfer RM, Maudgal DP, JosephAEA, Northfield TC. Gallstone recurrence after medicaldissolution: an overestimated threat? J7 Hepatol 1986; 3:241-6.
9 Salen G. Gallstone dissolution therapy with ursodiol. Efficacyand safety. DigDisSci 1989; 34 (12): 39-43S.
10 Marks JW, Lan SP, the Steering Committee, the NationalCooperative Gallstone Study Group. Low dose chenodiol toprevent gallstone recurrence after dissolution therapy. AnnIntern Med 1984; 100: 376-81.
11 Tint GS, Salen G, Chazen D. Symptomatic gallstones arelikely to reoccur after dissolution with UDCA, but this maybe prevented by low-dose UDCA. Gastroenterology 1987; 92:A1787.
12 Villanova N, Bazzoli F, Taroni F, Frabboni R, Mazzella G,Festi D, et al. Gallstone recurrence after successful oral bileacid treatment. Gastroenterology 1989; 97: 726-31.
13 O'Donnell LDJ, Heaton KW. Recurrence and re-recurrenceof gallstones after medical dissolution: a long-term follow-up. Gut 1988; 29: 655-8.
14 Dowling RH, Gleeson DC, Hood KA, British Belgian Gall-stone Study Group. Gallstone recurrence in postdissolutionmanagement. In: Paumgartner G, Stiehl A, Gerok W, eds.Bile acids and the liver. Lancaster: MTP Press, 1987: 355-67.
15 Sackmann M, Niller H, Ippisch E, Klueppelberg U,Neubrand M, Pauletzki J, et al. Gallstone recurrence afterlithotripsy. Gastroenterology 1992; 4: A332.
16 Hood K, Gleeson D, Ruppin DC, Dowling RH, BBGSG. TheBritish Belgian Gallstone Study Group's (BBGSG) post-dissolution trial. Gut 1987; 28: A1359.
17 Boscaini M, Mandetta S, Magnani G. Aspects morphologiquesdes echos a faible intensite dans la vesicule biliare: interpre-tation echographique, signe de la troisieme moustache etcorrelations cliniques. Le Journal Franfais d'Echographie1983; I (2): 23-4.
18 Schoenfield LJ, Berci G, Carnovale RL, Casarella W,Caslowitz P, Chumley D, et al. The effect of ursodiol on theefficacy and safety of extracorporeal shock-wave lithotripsyof gallstones. The Dornier national biliary lithotripsy study.NEnglJMed 1990; 18: 1239-45.
on Decem
ber 22, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.35.1.117 on 1 January 1994. Dow
nloaded from